
Abstract
Background
In China, clinical doctors bear heavy medical responsibilities and perform large volumes of diagnostic and therapeutic tasks. As the Artificial Intelligence-based Clinical Decision Support System (AI-CDSS) can assist in diagnosis, treatment, and decision-making to improve healthcare quality, it is especially important for improving healthcare quality. However, a crucial question remains: Are clinical doctors willing to adopt the AI-CDSS?
Methods
Based on the Unified Theory of Acceptance and Use of Technology (UTAUT) and related theoretical models, this study constructed an influence factor model for the willingness of clinical doctors to adopt the AI-CDSS. This model includes seven dimensions: performance expectancy, perceived risk, facilitating conditions, social influence, technology anxiety, personal innovativeness, and adoption willingness. Following the outline, a survey questionnaire was designed and distributed to 450 clinical doctors across 27 Chinese provinces. A structural equation model was used to analyse the factors influencing AI-CDSS adoption willingness, and semi-structured interviews were conducted to supplement and explain the data results.
Results
A significant positive association was found between AI-CDSS adoption willingness and performance expectancy (β=0.149, P < 0.001), social influence (β=0.156, P < 0.001), and personal innovativeness (β=0.649, P < 0.001). Conversely, technology anxiety demonstrated a significant negative association (β=-0.142, P < 0.001), while perceived risk showed no significant association (P = 0.115). This study also evaluated the moderating effects of the institutional level and AI-CDSS usage experience. Increased social influence was found to slightly weaken doctors’ willingness to adopt the AI-CDSS in tertiary hospitals.
Conclusions
This study constructed a theoretical influence factor model of AI-CDSS adoption willingness that is applicable to the context of China. Simultaneously, the study uncovers the double-edged sword mechanism of social influence in driving the willingness to adopt an AI-CDSS. This provides significant insights for clinical doctors, policymakers, medical institution managers, and AI-CDSS developers and aids in promoting the adoption of AI-CDSS in China.
Keywords
Background
The Artificial Intelligence-based Clinical Decision Support System (AI-CDSS) is a cutting-edge system based on Artificial Intelligence (AI) technology. 1 It interprets and analyses substantial volumes of medical data using advanced algorithms such as machine learning and data mining. The AI-CDSS aims to provide technical support to clinical doctors and assist them in making accurate and effective decisions throughout the diagnostic process, thereby enhancing the quality and efficiency of medical services. Numerous medical institutions and technology companies have committed substantial resources to the development of AI-CDSS, which now has wide applications in diverse areas such as radiology, pathology, dermatology, ophthalmology, oncology, cardiology, and the prevention of Venous Thromboembolism (VTE).2–6 For example, in the field of oncology, Watson for Oncology (WFO, IBM Corporation) is one of the most widely used Clinical Decision Support Systems (CDSSs) and is commonly applied in the diagnosis of various cancers, including lung, colon, rectal, breast, gastric, and gynaecological cancers. 7 In the VTE sphere, a retrospective study evaluated the effect of AI-CDSS on reducing hospital-related VTE incidence and showed a decrease from 5.89/1000 to 4.75/1000 patients during hospital stays in the intervention group. 8 In cardiac disease management, the AI-CDSS demonstrated its effectiveness by reducing the incidence of new vascular events by 26% through various quality improvement measures within three months. 9 The AI-CDSS plays a pivotal role in risk assessment, diagnosis, treatment optimisation, monitoring, and early warning of Cardiovascular Diseases (CVDs) by providing clinicians with more accurate and personalised information. 10 One of the core advantages of AI-CDSS lies in its intelligence and user-friendliness. It is designed from the outset to serve as a “smart assistant” for physicians, rather than a new burden that requires significant time and effort to learn.4,6
In recent years, more research has begun to explore the willingness of clinical doctors to adopt AI-CDSS. Castellanos and Goehler, among others, found that doctors showed a high willingness to adopt the AI-CDSS, believing that it contributes many conveniences to their clinical work, significantly improves medical work efficiency, reduces tedious repetitive work, and allows doctors to focus more on their work.11,12 Tolley et al.(2018) believed that the application of the AI-CDSS could help doctors decrease error rates and provide more accurate auxiliary diagnoses and treatment plans, thereby improving medical quality and minimising unnecessary medical errors. 13 However, Van et al.(2022) reported that physicians have certain reservations and concerns about AI-CDSS. They were apprehensive that AI-CDSS could eventually replace their roles, diminish their professional significance, and undermine the standing of human doctors. 14 Sun et al.(2020) expressed skepticism regarding the accuracy and reliability of AI technology, noting that unchecked input data in AI algorithms might introduce bias, potentially resulting in skewed diagnostic and treatment decisions. 15 Boers et al.(2019), evaluating the issue from an ethical standpoint, highlighted that beyond risks such as data breaches and information security threats, AI systems can influence disease diagnosis and contribute to prejudice and discrimination. 16 Given these viewpoints, what are doctors’ attitudes toward AI-CDSS? This study sought to evaluate whether clinical physicians are open to adopting AI-CDSS and to identify the factors influencing their willingness to do so.
In China, the integration of AI technology in the healthcare sector is steadily progressing, and AI technology is increasingly utilised in areas such as medical imaging and health management. Given China's vast population and relatively limited number of doctors, each doctor must provide diagnostic and therapeutic services to a high volume of patients daily, resulting in a substantial workload. In October 2023, the Chinese government released the “Statistics Bulletin on the Development of Health and Health Care in China in 2022.” The data revealed that in 2022, the total number of outpatient visits in medical and healthcare institutions across the country reached 8.42 billion, with a total of 3.72 million practicing physicians nationwide. This equates to 2.6 practicing physicians per thousand population with hospital physicians handling an average of 6.2 treatment visits per day. The issues of alleviating doctors’ workloads and enhancing medical efficiency and quality are challenges that need to be addressed. China's health supervisory department has specifically formulated the “Management Specifications for the Application of Clinical Decision Support Systems in Medical Institutions,” covering the information management, application management, and security management of CDSSs. This publication aimed to enhance medical safety and quality, particularly the diagnostic and therapeutic capabilities of primary healthcare facilities, through the effective implementation of policies. These measures also reflect the Chinese government's support for AI and its commitment to promoting the application and development of AI technology in the clinical healthcare sector.
Although attitudes and perceptions towards AI-CDSS differ among doctors, the adoption of the AI-CDSS remains a prevailing trend in the future development of medicine. With the initial perspective of China's national conditions, this study explored the willingness of clinical doctors in China to adopt the AI-CDSS, with the aim of offering recommendations to encourage the implementation and advancement of the AI-CDSS in clinical environments.
Methods
Theoretical analysis and assumptions of the model
This study utilised the Unified Theory of Acceptance and Use of Technology (UTAUT) as the basis for analysing doctors’ willingness to adopt the AI-CDSS. In 2003, Venkatesh et al. (2003) proposed the UTAUT based on eight major theoretical models, including the theory of reasoned action (TRA) and the technology acceptance model (TAM).17,18 The UTAUT model includes four core dimensions: performance expectancy, effort expectancy, social influence, and facilitating conditions. The UTAUT also considers the moderating effects of sex, age, experience, and willingness to use. Because of the humanoid characteristics of the AI-CDSS, which differ from non-intelligent technology and do not require user training, this study excludes effort expectancy. It incorporates performance expectancy, facilitating conditions, and social influence from the UTAUT as variables, while also introducing perceived risk, technology anxiety, and individual innovativeness to propose a comprehensive model of the factors influencing the willingness of doctors to adopt the AI-CDSS.
Performance expectancy hypothesis
Performance expectancy is defined as “the extent to which an individual believes that utilising the system will enhance their job performance”. 18 Individuals’ performance expectancies of technological systems significantly affect their intentions to use these systems. 19 Performance expectancy captures the relative advantage 20 and perceived usefulness 21 of a target technology. Previous studies have demonstrated that CDSSs can mitigate the occurrence of medical errors by providing alerts and recommendations in emergency situations.22–24 Therefore, we propose the following hypothesis:
H1: Performance expectancy positively influences doctors’ willingness to adopt the AI-CDSS.
Perceived risk hypothesis
Perceived risk was initially derived from the field of psychology by Bauer at Harvard University. 25 It encompasses the degree to which users perceive uncertainty and potential adverse outcomes related to their behaviour while using the system. Liu et al. (2016) mentioned in their study that data privacy and security are key concerns surrounding CDSSs. 26 Therefore, doctors may perceive the existence of risk while using the AI-CDSS for reasons such as data privacy and security, which may affect their willingness to adopt the AI-CDSS. Therefore, we propose the following hypothesis:
H2: Perceived risk negatively influences doctors’ willingness to adopt the AI-CDSS.
Facilitating conditions hypothesis
Facilitating conditions refer to the degree to which an individual believes that certain technical and organizational conditions exist that facilitates the use of a system. Venkatesh et al.(2003) proposed a direct relationship between facilitating conditions and usage behaviour rather than a direct relationship between facilitating conditions and adoption willingness. 18 However, several studies have focused on measuring willingness to adopt rather than actual usage. Foon, Zaremohzzabieh, and other scholars revealed an important connection between facilitating conditions and intention to adopt.27–29 Therefore, we propose the following hypothesis:
H3: Facilitating conditions positively influence doctors’ willingness to adopt the AI-CDSS.
Social influence hypothesis
Social influence is defined as the degree to which an individual perceives that those who they deem important (e.g., family and friends) should use a specific technology. 30 In a mandatory environment, individuals may use technology due to the need to comply with regulations rather than personal preference. 18 Aljarboa et al.(2021) demonstrated that doctors’ willingness to adopt CDSSs was influenced by the opinions of superiors and colleagues, and patient satisfaction with AI systems positively affected their acceptance. 31 Therefore, we propose the following hypothesis:
H4: Social influence positively influences doctors’ willingness to adopt the AI-CDSS.
Technology anxiety hypothesis
Technology anxiety refers to the feelings of fear and discomfort experienced when using a new technology or when faced with the prospect of using a new technology. 32 This includes job replacement anxiety, which is related to concerns that AI may replace humans in various occupations.33,34 Learning anxiety refers to a lack of confidence in learning to use AI, believing that the learning process is difficult. Previous studies have shown that poor computer skills can trigger technology anxiety.35,36 Huang et al.(2020) proposed that when individuals perceive that technology might risk their own existence, technology anxiety is generated, thereby reducing their willingness to adopt the technology. 37 Hence, technology anxiety is integrated into this model.
H5: Technology anxiety negatively influences doctors’ willingness to adopt the AI-CDSS.
Personal innovativeness hypothesis
Personal innovativeness refers to the degree to which an individual is willing to try innovative products or technology. 38 Each person's willingness to accept new products and technologies is different, and groups with high innovativeness are usually keener to contact and use new products. 39 Chen et al.(2020) introduced personal innovativeness into the UTAUT model and verified that it significantly affects the public's acceptance of driverless buses. 40 In addition, Wu et al.(2011) demonstrated that personal innovativeness has a positive impact on doctors’ willingness to adopt mobile medical care. 41 Therefore, doctors characterised by high levels of innovativeness may be more amenable to adopting and implementing the AI-CDSS as a new technology. In this model, by adding a personal innovativeness variable, we make the following assumption:
H6: Personal innovativeness positively influences doctors’ willingness to adopt the AI-CDSS.
Moderating effects
Our study attempts to test the moderating effects of the institution level and AI-CDSS usage experience on performance expectation, perceived risk, facilitating conditions, social influence, technology anxiety, personal innovativeness, and willingness to adopt the AI-CDSS.
Based on the above theoretical assumptions, we propose a hypothetical model of factors influencing the willingness to adopt the AI-CDSS (Figure 1).
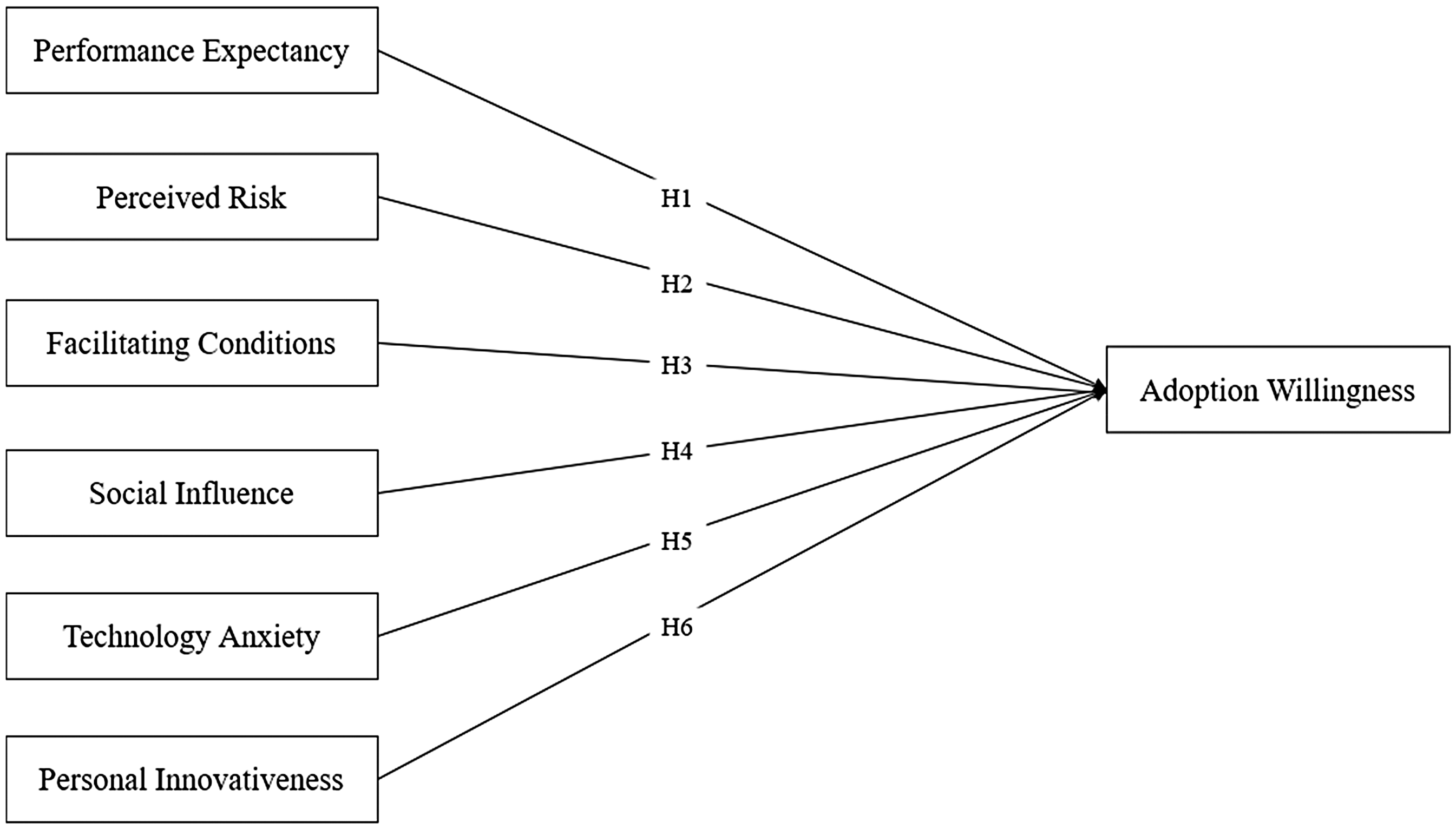
Hypothesis Model of Factors Influencing Willingness to Adopt the AI-CDSS.
Research design
Questionnaire design
Prior to the questionnaire, participants were required to review an electronic informed consent form that included the study purpose, data confidentiality, and voluntary participation terms. The survey could be accessed after participants confirmed their agreement to these terms. To ensure the effectiveness of the questionnaire, all scale designs in this study referred to existing literature and scales, with minor modifications to adapt to the subject of this study. The questionnaire was structured using a 5-point Likert scale, where respondents could express their agreement or disagreement on a scale from 1 to 5, defined as follows: 1, “strongly disagree”; 2, “disagree”; 3, “neither agree nor disagree”; 4, “agree”; and 5, “strongly agree.” The scales of performance expectancy, facilitating conditions, social influence, and adoption willingness were adapted from Venkatesh et al.(2003). 18 The perceived risk scale was adapted from Zhu et al.(2006)42,43 and technology anxiety was adapted from Meuter et al.(2003).18,44 The Personal Innovation Scale was adapted from the work of Wu et al.(2011) 41 According to the model hypothesis, the descriptive statistical variables at the institution level and AI-CDSS usage experience were treated as moderating variables. The questionnaire was mainly composed of two parts. The first part was demographic information, including age, sex, education level, and the level of the medical institution, and the second part was the main questionnaire scale items, including performance expectancy, perceived risk, facilitating conditions, social influences, technology anxiety, personal innovativeness, and adoption willingness. The survey questions used to measure the variables are presented in Appendix 1: Measurement items examined in the model.
Data collection
To ensure the quality of the acquired questionnaire and the reliability of the sample data, the selected survey areas included 27 provinces, cities, and autonomous regions, such as Beijing, Shandong, Henan, Heilongjiang, and Guangdong. Considering that the AI-CDSS is still in its initial stage, the survey subjects in this study were clinical doctors (e.g., respiratory, dermatology, radiology, and other specialties). Before the survey, the concept of the AI-CDSS was clarified to the respondents, and the doctors were relatively familiar with the AI-CDSS. Moreover, the group of doctors was very likely to follow and research the AI-CDSS.
Statistical analysis tools
This study used SPSS version 27 software to organize data and Cronbach's α to measure reliability. The structural validity of the model was examined through confirmatory factor analysis using Amos 28 software. The study employed structural equation modelling to investigate the following aspects: (1) whether the hypothesis model holds and the influencing factors and pathways of clinicians’ willingness to adopt the AI-CDSS; and (2) the moderating effects of the institution level and AI-CDSS usage experience on the relationship between influencing factors and adoption willingness.
Results
Demographic information
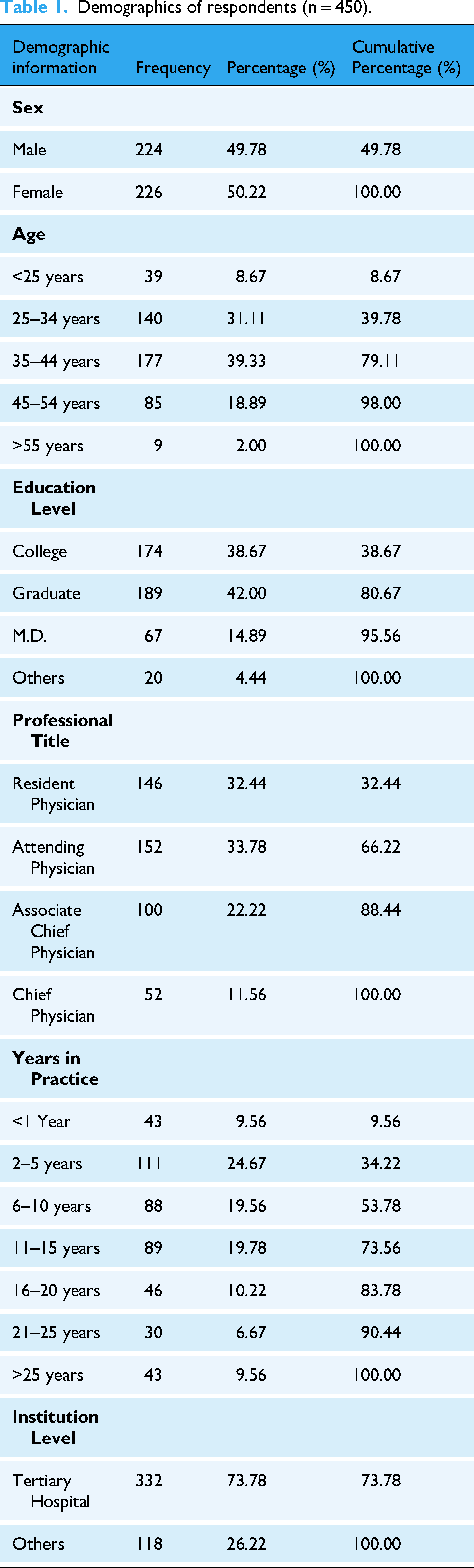
Using SPSS version 27 software for descriptive analysis of the survey participants, among the 450 doctors surveyed, 226 were female, and 224 were male. The predominant age group was 25–44 years. Additionally, 332 clinicians were from tertiary hospitals, and 118 were from other healthcare facilities. The basic experimental conditions are listed in Table 1.
Demographics of respondents (n = 450).
Homogeneity of variance test and reliability-validity analysis.
Homogeneity of Variance Test
Because all items in the questionnaire used in this study were completed by a single respondent, a possibility of common method variance was present. Therefore, this study applied Harman's single-factor test to verify common method variance and check for any common method bias that might have affected the research results. Exploratory factor analysis was performed on all items using principal component analysis (PCA). The verification results showed that the first principal component explained 34.39% of the variance and did not exceed the threshold of 40.00%. Thus, no significant common method bias that might have affected the results was observed.
Internal Reliability and Validity Analysis
Cronbach's α is commonly used to test for the internal consistency of variables. As illustrated in Table 2, all estimated indices were >0.80, above the recommended thresholds. Structural validity includes convergent validity and discriminant validity. The former reflects the correlation among different measurement items under the same variable (higher value is better); the latter refers to the correlation among different variables (lower value is better). Convergent validity is generally analysed based on three indicators: factor loadings, average variance extracted (AVE), and composite reliability (CR).The factor loadings were >0.60, the AVE values were all >0.50, and the CR values were all >0.80, indicating good convergent validity among the measurement items.
Internal reliability and convergent validity of the measurements.

Note: PE, Performance Expectancy; PR, Perceived Risk; FC, Facilitating Conditions; SI, Social Influence; TA, Technology Anxiety; PI, Personal Innovativeness; AW, Adoption Willingness.
A common method of evaluating discriminant validity involves comparing the square root of the AVE with the correlation coefficients between variables; when the correlation coefficient between variables is less than the square root of the AVE, discriminant validity is considered good. The results of the discriminant validity test, as shown in Table 3, reveal that the correlation coefficient between “Social Influence” and “Facilitating Conditions” is higher than the square root of the AVE, indicating low discriminant validity between these two dimensions and potential multicollinearity. The square root of the AVE of each remaining variable was larger than that of the other variables.
Inter-Construct correlations and square roots of AVE.
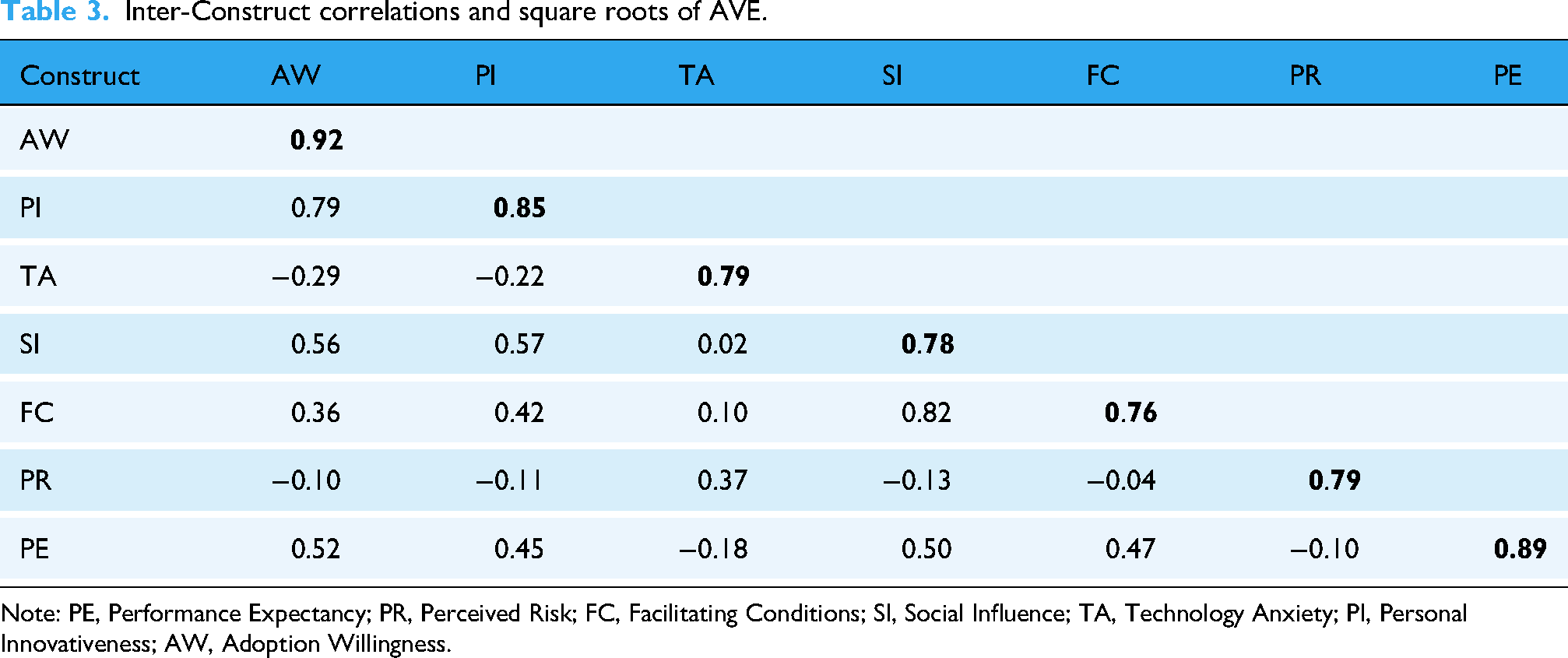
Note: PE, Performance Expectancy; PR, Perceived Risk; FC, Facilitating Conditions; SI, Social Influence; TA, Technology Anxiety; PI, Personal Innovativeness; AW, Adoption Willingness.
To address the issue of multicollinearity between “Facilitating Conditions” and “Social Influence,” this study incorporated semi-structured interviews to delve deeper into the root cause of the problem. Based on the analysis of the questionnaire survey results, an interview content framework and outline were developed. The questions were as follows: ① “Can you distinguish between the items for ‘Facilitating Conditions’ and ‘Social Influence’” and ② “How would you interpret the impact of ‘Social Influence’ and ‘Facilitating Conditions’ on the willingness to adopt AI-CDSS?”
Eleven clinical doctors were randomly selected from the survey respondents for the interviews. The inclusion criteria for clinical doctors in the interviews were as follows: ① completion of the survey questionnaire for this study; ② possession of over three years of clinical work experience; and ③ agreement to participate in the study. Information on the experts interviewed is shown in Table 4.
Demographics of the respondents.

The interview results showed that most doctors believed that “Social Influence” and “Facilitating Conditions” are two different concepts, and both can impact adoption willingness. However, since the clinical doctor group generally lacked systematic training in the humanities and social sciences, they faced challenges in understanding and clearly distinguishing between these two concepts. Interviewee A3 said, “This questionnaire is filled out subjectively. There is strong randomness when I filled out the questionnaire without prior understanding.” Interviewee A10 said, “There will be help when encountering difficulties, I don't understand what this means.” Some interviewees also confused the items between the two dimensions. Interviewee A4 said, “Actually, ‘Social Influence’ has become ‘Facilitating Conditions.'” Interviewee A5 said, “The items are a bit confusing.” Lastly, Interviewee A10 said, “'The hospital will provide financial and manpower support for the implementation of CDSS technology’ in the ‘Social Influence’ dimension may overlap with ‘Facilitating Conditions.'” The average response time for the questionnaire was 221 s, with 36 questions covering basic information and the survey theme, resulting in an average of approximately 6 s per question. The constrained time allotted to complete the questionnaire may have led respondents to read the questions hastily, potentially contributing to the observed low discriminant validity between the two dimensions.
In the UTAUT model, no direct influence path exists between “Facilitating Conditions” and “Adoption Willingness.” This directly affects the behavioural intention to use the system. 45 In this model, we treated “Adoption Willingness” as a dependent variable, with no investigation into actual usage behaviour. Recognising this consideration and aiming to reduce the bias stemming from multicollinearity, we opted to remove the dimension of “Facilitating Conditions.” After deletion, the results of the reliability and validity analyses met the required criteria, and the discriminant validity was significantly improved.
Structural Model Analysis.
Model Fit Test
A fit analysis was conducted on the hypothesised model, primarily evaluating the Chi-square/df, root mean square error of approximation (RMSEA), incremental fit index (IFI), Tucker-Lewis index (TLI), and comparative fit index (CFI). The criteria and actual values are listed in Table 5. The values of Chi-square/df, RMSEA, normed fit index (NFI), IFI, TLI, CFI were 3.32, 0.07, 0.91, 0.94, 0.92, and 0.93, respectively, all within acceptable ranges, suggesting that the hypothesised model demonstrated a good fit.
(ii) Regression Results of Hypothesis Path Coefficients
Model fit.

Note: Chi-square/df, Chi-Square/Degree of Freedom; RMSEA, Root Mean Square Error of Approximation; NFI, Normed Fit Index ; IFI, Incremental Fit Indices; TLI, Tucker-Lewis Index, TLI; CFI, Comparative Fit Index.
Table 6 presents the results of the model testing, which aimed to examine the significance of each hypothesis path. A positive standardised path coefficient indicates a positive influence between variables, whereas a negative coefficient signifies a negative influence, measuring the strength of the causal relationship between variables. The standardised path coefficient typically falls within the range of 0–1. A coefficient closer to 1 indicates a stronger causal relationship, whereas a coefficient closer to 0 suggests a weaker relationship.
Hypotheses testing results.

* P < 0.05, *** P < 0.001.
Note: SE, Standard Error; CR, Composite Reliability; PE, Performance Expectancy; PR, Perceived Risk; SI, Social Influence; TA, Technology Anxiety; PI, Personal Innovativeness; AW, Adoption Willingness.
The results showed that hypotheses H1, H4, H5, and H6 had absolute CR values of >1.96 and P values of <0.001, indicating that they passed the significance test. Therefore, the four hypotheses were supported. H2 did not pass the significance level test and thus was not supported.
Moderation effect
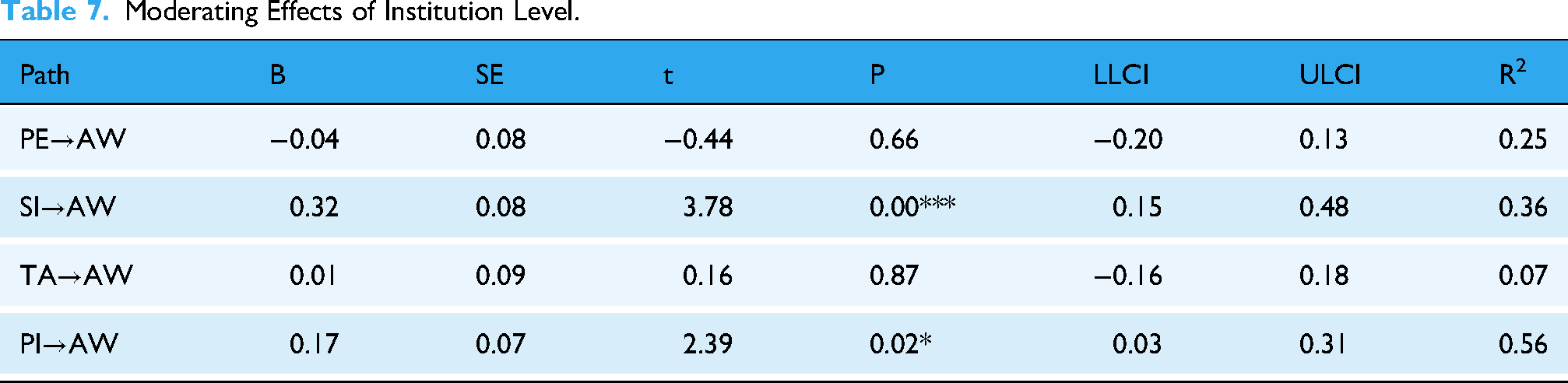
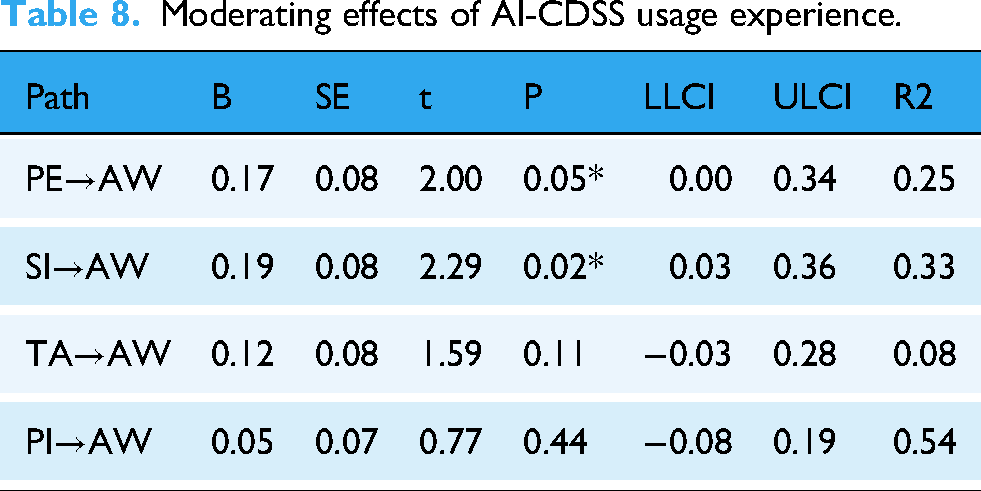
We ran bootstrapping calculations with 5000 samples to test the moderating effects of the institution level and AI-CDSS usage experience. The confidence interval of the PROCESS plugin was set to 95%, and the model sequence number was chosen as MODEL 1. The results are presented in Tables 7 and 8. Institution level is a significant moderator on two paths: social influence→adoption willingness and personal innovativeness→adoption willingness. AI-CDSS usage experience is a significant moderator on two paths: performance expectancy→adoption willingness and social influence→adoption willingness.
Moderating Effects of Institution Level.
Moderating effects of AI-CDSS usage experience.
Institution Level
A simple slope plot was drawn to provide a clear comparison of the moderating impact of the institution level. As depicted in Figure 2, the slope for hospitals at other levels was steeper than that of tertiary hospitals, suggesting that institution level plays a role in moderating the relationship between social influence and adoption readiness. Physicians from other hospitals exhibited a stronger positive impact of social influence on their willingness to adopt the AI-CDSS. Conversely, for physicians from tertiary hospitals, social influence slightly dampened adoption readiness.

Simple slope graph of institution level moderating effect (SI-AW).
As shown in Figure 3, the slope of hospitals at other levels was greater than that of tertiary hospitals, indicating that the institution level has a moderating effect on the relationship between personal innovativeness and adoption willingness. At primary and secondary hospitals, personal innovativeness has a more pronounced impact on willingness to adopt the AI-CDSS, and even a slight enhancement in personal innovativeness can lead to substantial increases in adoption willingness. Conversely, for doctors from tertiary hospitals, the impact of personal innovativeness on the willingness to adopt is comparatively less significant.
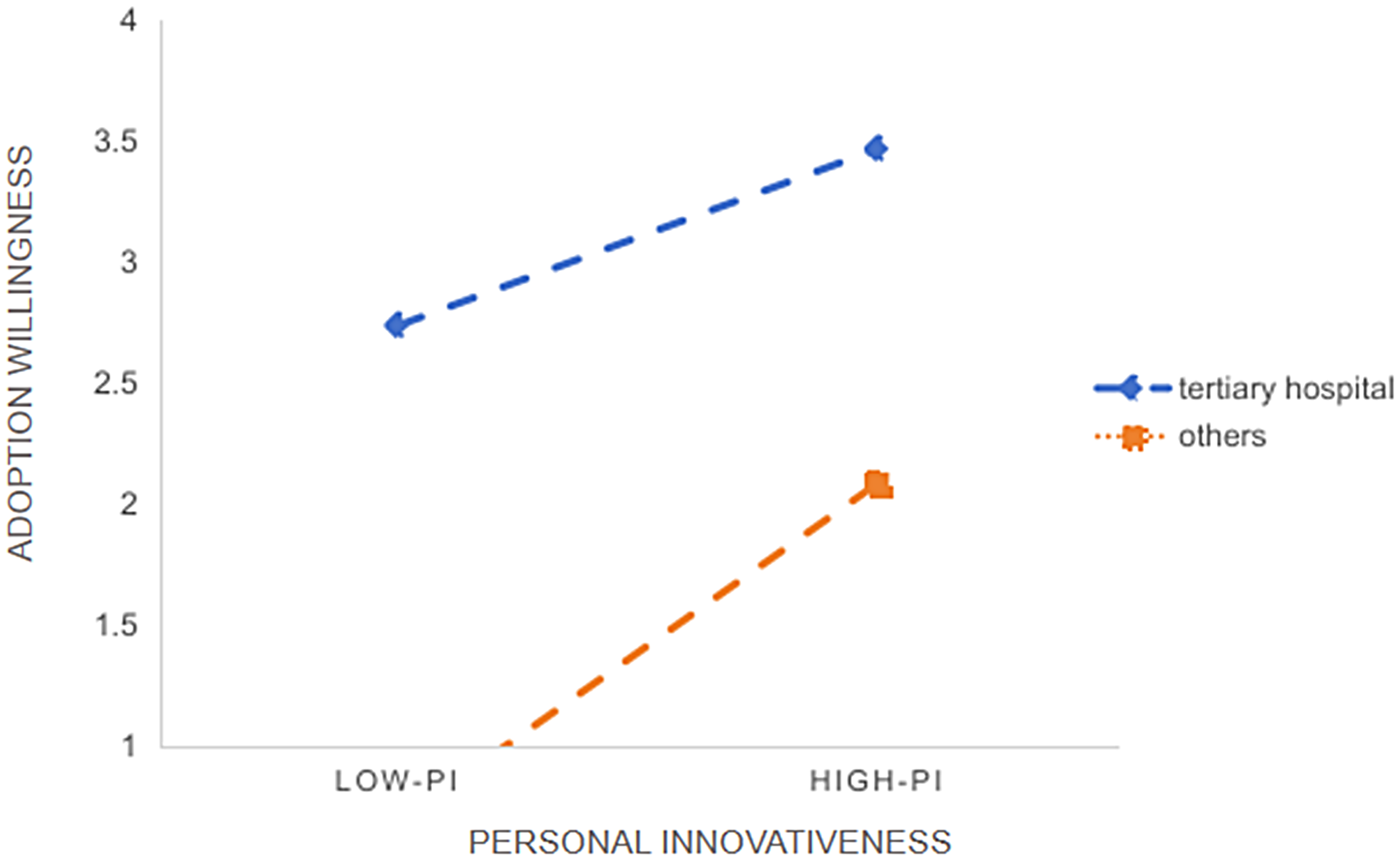
Simple slope graph of institution level moderating effect (PI-AW).
AI-CDSS Usage Experience
The moderating effect of AI-CDSS usage experience is shown in Figures 4 and 5. In the relationship between performance expectancy and willingness to adopt, the slope for individuals with AI-CDSS usage experience exceeded that of those without such experience. Doctors with AI-CDSS usage experience exhibited a more significant positive effect on adoption willingness, with increasing performance expectancy, than those without such experience.

Simple slope graph of AI-CDSS usage experience moderating effect (PE-AW).
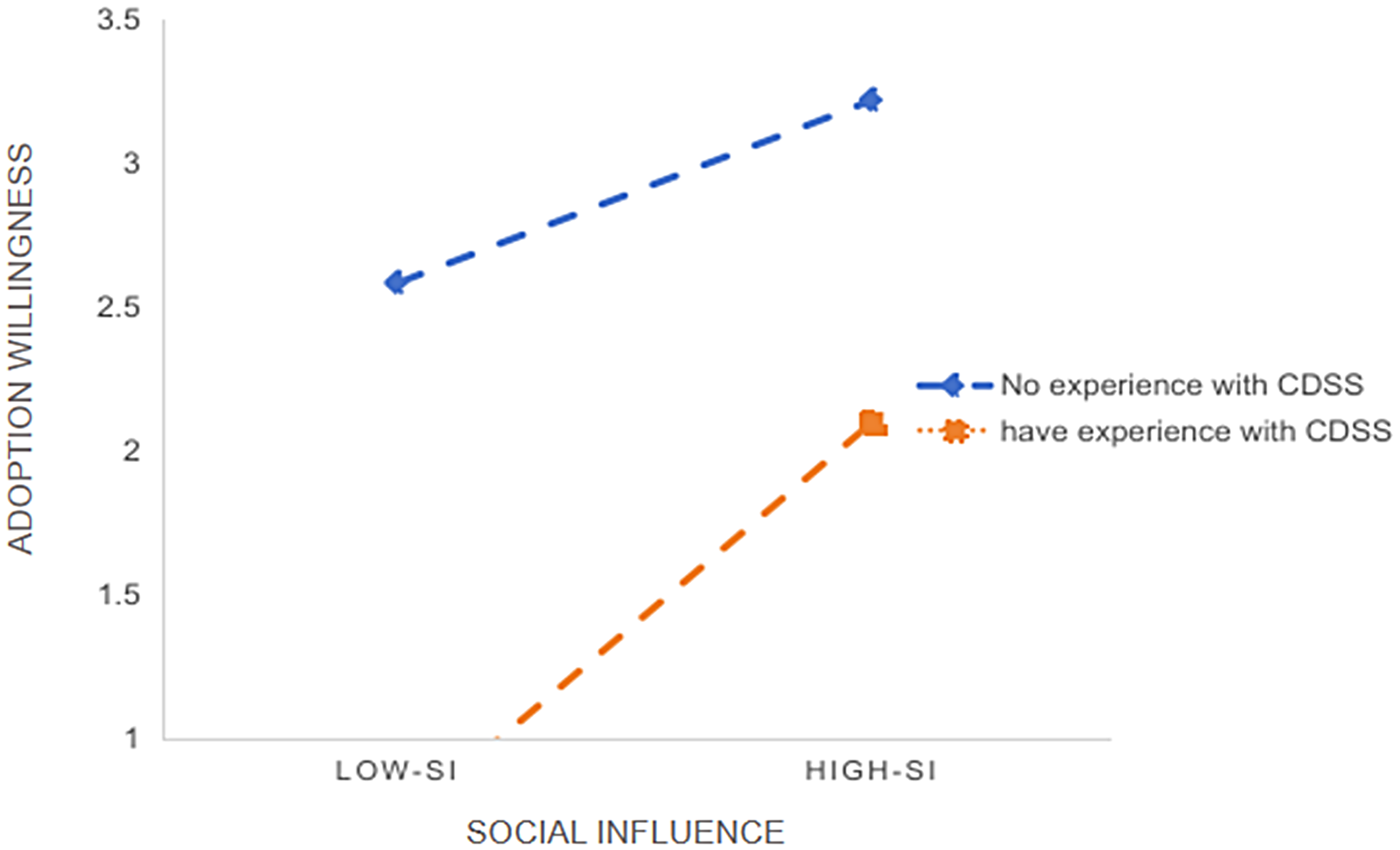
Simple slope graph of AI-CDSS usage experience moderating effect (SI-AW).
In the relationship between social influence and willingness to adopt, the slope for individuals with AI-CDSS usage experience was greater than that for those without such experience. This indicates a moderating effect, implying that social influence has a stronger positive impact on doctors’ willingness to adopt with prior usage experience.
Based on our results, a model diagram of the factors influencing willingness to adopt the AI-CDSS was drawn (Figure 6). Performance expectancy, social influence, and personal innovativeness had a positive impact on willingness to adopt, whereas technological anxiety had a negative impact. A moderating effect was observed between the institutional level and AI-CDSS usage experience.
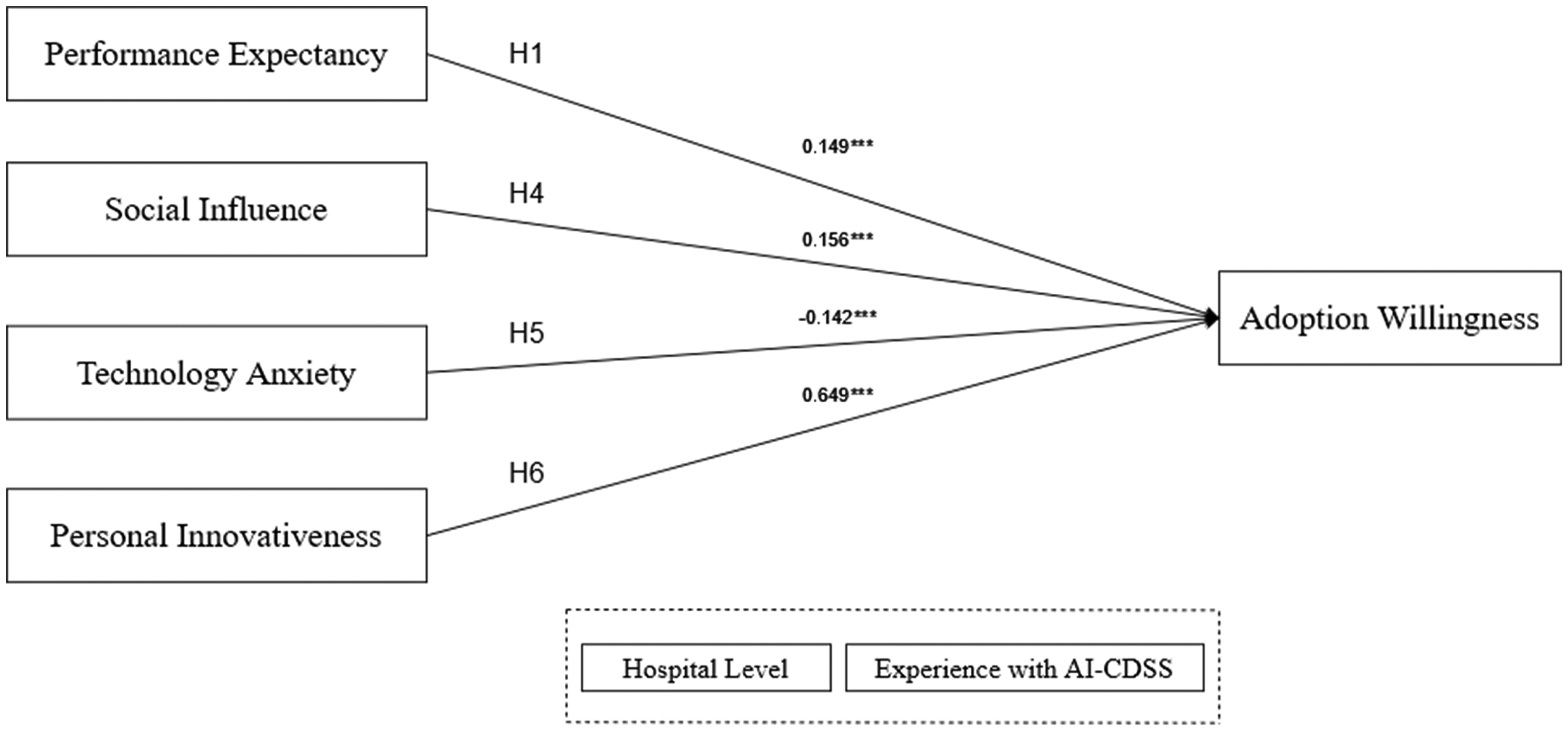
Research model.
Discussion
From a theoretical perspective, this study extended the empirical assessment of doctors’ willingness to adopt the AI-CDSS by building upon existing research. By utilising UTAUT as the theoretical framework, this study identified the influencing factors that promote or hinder doctors’ willingness to adopt the AI-CDSS and provides a theoretical foundation for the factors affecting doctors’ willingness to adopt the AI-CDSS.
Establishing a model of AI-CDSS adoption willingness applicable to conditions in China
Performance expectancy positively influences adoption willingness
Doctors’ willingness to adopt the AI-CDSS was positively correlated with their perceptions of the AI-CDSS's ability to enhance work efficiency and improve the quality of diagnosis and treatment. This is consistent with social cognitive theory, which suggests that individuals are more inclined to engage in a particular behaviour if they anticipate favourable outcomes. 46 As a system assisting doctors in clinical decision making, the AI-CDSS can help doctors make decisions more quickly and accurately by providing patient data, disease diagnosis recommendations, and treatment plans. When doctors recognise that these functionalities of the AI-CDSS can alleviate their workload, improve efficiency, and improve the quality of diagnosis, their willingness to adopt this system will be strengthened. 47
As a system integrating AI and medical decision-making knowledge, the completeness of the AI-CDSS's functions directly determines its performance in practical applications. The efficacy of the system hinges on continuous innovation to bolster its capacity to manage intricate data, execute intelligent analyses, and facilitate decision making. Achieving superior performance requires sustained investment in research and development, a proficient team, and continuous market feedback. For example, at the system level, a feedback loop must be established to ensure that the dynamic system can be continuously tested and upgraded as required. At the data level, we must continually improve the usability of electronic medical record data across systems and databases to promote machine learning capabilities.48,49 At the application level, optimising user experience should be a main focus, as systems that are user-friendly and adaptable are more likely to be embraced by users. 50
Social influence positively affects adoption willingness
Social influence correlates positively with doctors’ willingness to adopt the AI-CDSS, indicating that their adoption decisions are influenced by their social environment and interactions. Given that doctors form a closely knit professional community characterised by communication and collaboration, the endorsement and adoption of the AI-CDSS by colleagues or peers can offer valuable insights and information to doctors who lack prior experience with the technology, which can alleviate uncertainty and anxiety, thereby enhancing their willingness to adopt the AI-CDSS. 51
Therefore, hospital managers should take proactive measures to promote the AI-CDSS and facilitate its integration through initiatives such as publicity, training, and incentives. Medical staff can also share their experiences and lessons learned from using the AI-CDSS to jointly solve problems and mitigate confusion encountered during utilisation.
Technological anxiety negatively affects adoption willingness
Technological anxiety is a negative emotion that leads to technology avoidance. 52 The results of this study show that technological anxiety is negatively correlated with doctors’ willingness to adopt the AI-CDSS. Lack of familiarity with the AI-CDSS, self-doubt, and lack of confidence in learning to use the system, as well as perceiving it as a potential rival or threat, can all contribute to doctors’ hesitation to adopt the AI-CDSS. This hesitation may lead to a reluctance to learn and actively use the system, ultimately fostering resistance to its implementation.
To thrive, medical institutions must incorporate the AI-CDSS into their long-term development strategies and prioritise organising training sessions for all medical staff. The necessity of pre-use training for the adoption of new technology has been discussed by Vassilios, Rania, and others.53–55 Even a short training session can significantly enhance medical professionals’ willingness to use decision-support tools for medical diagnoses. 56 Therefore, medical institutions should consider inviting experts to conduct onsite demonstrations and address queries related to system operations, data interpretation, decision support, and other pertinent aspects. Providing doctors with comprehensive product descriptions and operation manuals can facilitate a deeper understanding of the system's functionalities and features, enabling them to effectively master their utilisation.
Personal innovativeness positively influences adoption willingness
Personal innovativeness and willingness to adopt are positively correlated. With higher personal innovativeness traits, doctors have higher willingness to adopt the AI-CDSS. Personal innovativeness in the field of information technology affects individuals’ adoption of new information technology. 57 Healthcare professionals with elevated levels of personal innovativeness tend to be more open to novel ideas and technologies and actively explore and experiment with new tools or products pertinent to their profession. When facing emerging technologies such as the AI-CDSS, doctors high in innovativeness are more likely to explore, learn, and adopt new technologies. To encourage and support this attitude, medical institutions should implement measures to nurture an innovative culture. These include establishing innovative awards, organizing innovative seminars, reforming hospital management models, and establishing innovative management departments. Additionally, doctors must stay informed about advanced research and developments within their respective professional fields, continually analysing and incorporating the latest research findings and technological advancements.
Perceived risk does not directly influence adoption willingness
The hypothesis regarding the relationship between perceived risk and willingness to adopt was not supported; doctors’ concerns about potential risks or uncertainties associated with the AI-CDSS did not directly impact their willingness to adopt the system. Zhu et al.(2006) believed that data security issues hindered the application of electronic information technology 42 ; however, our research conclusions indicate that no significant correlation exists between perceived risk and adoption willingness. This may be attributed to the fact that doctors, as seasoned medical professionals, generally exhibit a higher tolerance for risk and possess strong assessment capabilities. They tend to prioritise potential benefits and practical outcomes when encountering new medical technologies, rather than excessively dwelling on potential risks. Even if a system provides an incorrect or redundant diagnosis, doctors can make the correct judgment based on their own expertise and experience. Notably, the AI-CDSS serves as a supplemental tool during the diagnostic process, offering guidance rather than definitive conclusions. 58 Therefore, even if doctors perceive a certain risk of the AI-CDSS, their willingness to adopt it does not necessarily lessen.
An exploratory study of the double-edged sword effect in AI-CDSS adoption willingness
During the moderation effect analysis at the institutional level, we observed that in the group of tertiary hospitals, the enhancement of social influence slightly weakened doctors’ willingness to adopt the AI-CDSS. We investigated the underlying causes accordingly.
Our research team conducted follow-up interviews with the aforementioned 11 clinical doctors, posing the following question: Our research findings indicate that the social influence of doctors in tertiary hospitals has a negative impact on their willingness to adopt AI-CDSS. In your opinion, what are the possible reasons for this phenomenon?
We analyzed the interview results using thematic coding, with two researchers independently coding the data, then comparing the results and resolving discrepancies through iterative discussions. The results revealed that doctors in tertiary hospitals exhibited strong individual independence, rebellious tendencies, confidence in their professional abilities, scepticism about AI technology, and disappointment in AI systems that failed to meet their needs. These factors collectively led them to prioritise decision-making based on professional judgment, rather than external social pressures. The following are specific quotes from the interviews:
Strong individual independence: “I think it's about independence, because doctors in tertiary hospitals are more independent and we are more willing to trust ourselves.” (A10) Rebellious tendencies: “If the hospital or leader imposes the use of AI technology, I may display some rebellious behaviour and even feel resistant, as I am concerned about potential interference with my work.” (A1) Confidence: “After all, I believe that the current diagnostic capabilities of AI are not as precise as my own expertise.” (A3) Distrust of AI technology: “The underlying issue lies in a lack of trust in AI technology: the more you enforce its use on doctors, the potential outcome could be counterproductive.” (A4) Disappointment in AI systems failing to meet their needs: “If AI-CDSS is a truly helpful auxiliary tool for clinical practice, I would gladly use it. However, if the function cannot meet my needs, I might choose not to utilise it.” (A6)
In contrast, social influence exerted a positive effect in secondary and lower-level hospitals. This favourable influence may arise from instilling doctors with confidence and providing support, leading them to believe that embracing new technology can improve service quality, efficiency, and patient satisfaction. Integrating the findings above, this study suggests that social influence may act as a complex “double-edged sword” mechanism in moderating doctors’ willingness to adopt the AI-CDSS. In tertiary hospitals, excessive social influence may hinder technology adoption. However, in secondary and lower-level hospitals, social influence has become an important force in promoting technological innovation. It should be noted, however, that these interpretations remain exploratory due to the limited sample size (n = 11) of the interview data.
This exploratory study offers valuable insights for policymakers, hospital administrators, and AI-CDSS developers. To effectively leverage social influence, we recommend developing tailored implementation strategies based on hospital tier:
For tertiary hospitals, we recommend shifting from top-down mandates to promoting voluntary adoption through peer-led demonstration projects and the establishment of clinical-AI collaboration frameworks. This approach positions physicians as co-designers and evaluators in the process.
For secondary and primary care hospitals, social influence can be leveraged through structured support systems. This includes developing clear implementation guidelines, establishing incentive mechanisms for successful adopters, and formally integrating AI-CDSS training into continuing medical education programs.
Conclusion
This study further refines the UTAUT model by incorporating perceived risk theory, technology anxiety theory, and individual innovativeness theory to construct a conceptual model outlining the factors influencing doctors’ willingness to adopt the AI-CDSS. The model was verified using the data collected through a questionnaire. The main research conclusions are as follows: Performance expectancy, social influence, and personal innovativeness positively influence doctors’ willingness to adopt the AI-CDSS, whereas technology anxiety has a negative impact. Perceived risk did not show a significant correlation with willingness to adopt. Furthermore, moderation effects were observed at the institution level and AI-CDSS usage experience.
Analysis of the institutional-level moderation effects revealed a divergent pattern: while enhanced social influence slightly diminished adoption willingness in tertiary hospitals, it exerted a positive effect in secondary and lower-level hospitals. This pattern suggests the possibility that social influence functions as a “double-edged sword” in shaping physicians’ adoption of AI-CDSS. These nuanced findings highlight the need for future research, particularly longitudinal studies to track the evolution of these influences as AI-CDSS becomes more embedded in practice, and comparative studies to examine how institutional factors modulate social influence across different hospital tiers.
Research limitations and future studies
First, the survey questionnaire used in this study contained unclear statements regarding facilitating conditions and social influence. This directly led to a significant reduction in the differentiation between the two dimensions during data analysis, introducing multicollinearity. We believe the reason may lie in the implementation of the president responsibility system under the leadership of the Party Committee. Within this framework, the will of hospital management constitutes the most fundamental source of social influence. The signal that “hospital administrators encourage us” (Social Influence) directly translates into concrete actions such as “the hospital will provide financial and human support for implementation…” (Facilitating Conditions). Conversely, when hospitals provide sufficient facilitating conditions, including robust IT infrastructure, timely expert support, and systematic training, the underlying message conveyed to physicians becomes: “The hospital is fully committed, this technology is reliable.” This significantly reinforces physicians’ perception that “using AI-CDSS represents correct and institutionally supported behavior” (Social Influence). To a certain extent, this affected the accuracy and interpretability of the research results. Following detailed follow-up interviews, the “Facilitating Conditions” dimension was excluded to effectively address the bias stemming from multicollinearity. This underscores the essential role of optimising questionnaire design. Therefore, future research could develop an adoption willingness survey tool targeting doctor groups to ensure clear and distinct responses, thereby augmenting the overall quality and value of the research.
Second, the study's sample presents several limitations. Among the 450 participants, 286 people had not used the AI-CDSS, accounting for 63.5% of the sample. Although they formed psychological expectations of the AI-CDSS based on their cognitive preferences and knowledge, these expectations may differ from actual usage experience, potentially skewing the results. Furthermore, the reliance on self-reported measures of adoption willingness introduces the risk of social desirability bias, where respondents may have over-reported their positive attitudes to align with perceived institutional or professional expectations. Geographically, while the sample covered 27 regions, it was likely skewed toward urban and tertiary hospitals, as the distribution via WeChat and Questionnaire Star may have primarily reached physicians who are tech-savvy, frequent internet users, or based in better-resourced medical centers. This may limits the generalizability of the findings to the broader physician population. In future research, a larger number of participants with actual AI-CDSS usage experience should be recruited, and sampling strategies should be designed to mitigate geographic and institutional-level biases to improve the representativeness of the sample.
Finally, this study employed a Structural Equation Model (SEM). Although the SEM is effective in confirming linear relationships between variables, it may not adequately demonstrate complex multi-factor simultaneous causal relationships. For future research, methods such as the fuzzy set/Qualitative Comparative Analysis (fsQCA) can be used to examine aggregate relationships and analyse complex conditional combination effects for further validation. 59
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251396984 - Supplemental material for Analysis of clinical doctors’ adoption willingness pathway for the artificial intelligence-based clinical decision support system (AI-CDSS)–A survey study from China
Supplemental material, sj-docx-1-dhj-10.1177_20552076251396984 for Analysis of clinical doctors’ adoption willingness pathway for the artificial intelligence-based clinical decision support system (AI-CDSS)–A survey study from China by Qiuyi Zhao, Xiang Hu, Ning Hu, Chunshan Xu and Zhongguang Yu in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgements
Ethics approval and consent to participate
This study was approved by the Clinical Research Ethics Committee of China-Japan Friendship Hospital (No. 2024-KY-254). All participants provided informed consent before the investigation began. Furthermore, the information of the research participants was kept confidential, and personal private information was not disclosed.
Consent for publication
Not applicable.
Authors’ contributions
ZQY performed the analysis and wrote the original draft; YZG collected the data, edited, and critically reviewed the manuscript; HX participated in the data analysis and designed the study; HN participated in the statistical analysis and data entry; XCS edited and critically reviewed the manuscript. All the authors have read and approved the final version of the manuscript.
Funding
We thank the interviewees who participated in the study. This work was supported by the National Natural Science Fund for Young Scholars of China (72104255), the Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences (CIFMS; 2021-I2M-1–046), and the China-Japan Friendship Hospital High-Level Project (2024-NHLHCRF-GL-12).
Chinese Academy of Medical Sciences Initiative for Innovative Medicine, China National Funds for Distinguished Young Scientists, China-Japan Friendship Hospital Youth Science and Technology Excellence Project, (grant number CIFMS; 2021-I2M-1-046, 72104255, 2024-NHLHCRF-GL-12).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and/or analysed in the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Clinical trial number
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.