
Abstract
Current empirical evidence suggests that successful adoption of eHealth systems improves maternal health outcomes, yet there are still existing gaps in adopting such systems in Uganda. Service delivery in maternal health is operating in a spectrum of inadequacy, hence eHealth adoption cannot ensue. This study set out to explore the challenges that impede eHealth adoption in women's routine antenatal care practices in Uganda. A qualitative approach using semi-structured interviews was employed to document challenges. These challenges were classified based on a unified theory of acceptance and use of technology constructs. One hundred and fifteen expectant mothers, aged between 18 and 49 years, who spoke either English or Luganda were included in the study that took place between January to May 2019. Thematic analysis using template analysis was adopted to analyse qualitative responses. Challenges were categorised based on five principal unified theories of acceptance and use of technology constructs namely: performance expectancy, effort expectancy, social influence, facilitating conditions and behavioural intention. Facilitating conditions had more influence on technology acceptance and adoption than the other four constructs. Specifically, the lack of training prior to using the system, technical support, computers and smart phones had a downhill effect on adoption. Subsequently, the cost of data services, internet intermittency, and the lack of systems that bridge the gap between mothers and health providers further hindered technology uptake. In conclusion, strategies such as co-development, training end-users, garnering support at the national and hospital levels should be advocated to improve user acceptance of technology.
Keywords
Introduction
As of 2017, Uganda's maternal mortality rate stood at 375 deaths per 100,000 live births 1 with an estimated 16 women dying from giving birth every day. 2 It is highly premised that maternal mortality can be combatted if expectant mothers adhere to antenatal care and give birth with the help of a skilled birth attendant. 3 Antenatal care is one of the ‘four pillars’ of safe motherhood initiatives of promoting and establishing good health during pregnancy and the early postpartum period. 4 Recently, WHO recommended that pregnant women should have their first contact in the first 12 weeks’ gestation, with subsequent contacts taking place at 20, 26, 30, 34, 36, 38 and 40-weeks’ gestation. 5 Globally, during 2000-2010, about 53% of pregnant women attended the recommended minimum of four times antenatal care (ANC). 6 And in developing countries, the proportion of expectant mothers who attend at least one ANC has increased from 64% in 1990 to about 81% in 2009, but in Uganda, 47.6% had attended at least four times as of 2011. 7 The main objectives of ANC include satisfying any unmet nutritional, social, emotional and physical needs of expectant mothers; provision of patient education, including care and nutrition of the newborn; identification of high-risk pregnancy; and encouragement of (male) partner involvement in ANC. 8 In Uganda, ANC attendance predominantly takes place at the health facilities in the presence of a skilled birth attendant. However, there is very little literature citing the use of eHealth technologies in routine ANC practices, yet evidence shows that technology can accelerate service adoption. 9
World Health Organization defines eHealth as the cost-effective and secure use of Information and Communication Technology (ICT) in support of health and health-related fields, including health care services, health surveillance, health literature, health education, knowledge and research. 1 It involves the use of mobile wireless and fixed technologies such as mobile phones, computers, personal digital assistants, to transmit messages in form of text, audio, video, images among others. Technology has become an integrated part of the health care system, 10 for example medical treatment in patients with dermatological conditions, 11 wound management, 10 electronic health records 12 and maternity care. 9
Some of the eHealth initiatives in Uganda include mobile microscopy, mTrac which aims to address problems with the provision of maternal, neonatal and child health services in Uganda by gathering feedback from community members; U-Report – an anonymous toll-free SMS hotline for complaints about health services. 13 Similarly, familyConnect sends targeted life cycle-based messages via SMS to pregnant women, new mothers with information on what they can do to keep themselves and their babies in good health 14 ; Open Medical Record System (OpenMRS) – a generic medical record system that supports the care of patients and gathering data on maternal, neonatal and child health services in Uganda 15 ; District Health Information Software (DHIS2) – tracks mothers and children to improve the continuum of care through village health teams that submit data directly to the online portal.16,17 Currently, Uganda has 25 live mHealth initiatives deployed with partnerships from over 50 different organizations representing multiple stakeholder groups. 18 Nine of the 25 interventions implemented in Uganda focus on maternal and newborn child health interventions. Of the nine, seven focus on maternal health, and six address infant and young child health. To build a strong health information system reinforced by digital health, the Ministry of Health (MoH) of Uganda developed an eHealth strategy and framework, coupled with establishing a technical working group that meets regularly to guide this work. 19 It is quite evident that the Government of Uganda recognizes eHealth as a driver to better health service delivery.
Despite opportunities presented by eHealth, there is still slow adoption which is partly caused by primary users' limited computer skills and poor internet connectivity,12,20 poor existing infrastructure and network failure, 21 and excessive disease burden. 22 Additionally, lack of eHealth policy and strategy, 17 unavailabilities of local content in medical literature,17,23 lack of local ownership,16,17 lack of government support and funding24,25 have a downhill influence on eHealth adoption. Most eHealth initiatives remain proof of concept pilots, many originally funded by development partners through grants. 17 Within Uganda's eHealth strategy and framework, certain challenges impede rapid implementation of eHealth: fragmented data sources, numerous and uncoordinated digital health pilot projects, poor computer literacy skills, data security and privacy concerns, a shortage of health staff, and interoperability issues. 19 To implement eHealth innovation in daily practice, a phased approach tailored to specific groups and settings is most successful. 26 It should be noted that utilization of ANC in Uganda has largely been affected by the long distances to health facilities, the lack of transport especially in rural areas and congestion in health facilities, 27 yet once fully embraced, digital technologies can bridge this gap by decongesting health facilities and relieve the already overwhelmed health providers from unnecessary workload.
Whereas advancement in technology has influenced the use of health services, 28 the literature on ANC utilization and ICT's seems to have focused on issues related to the supply of health services rather than the users of these technologies (demand side). 29 Similarly, there is hardly any literature focusing on the role of eHealth initiatives in accelerating ANC utilization in Uganda from the demand perspective. 30 The rationale of focusing in this direction was two-fold; firstly, there is an exponential growth of ICT in the region and secondly, the influence ICT's have on the demand for health services through the information they make available to the users.9,31 In a study conducted by Namatovu and Oyana, 30 ICT uptake stood out as a key determinant of ANC utilization.
This study is aligned to the United Nations Sustainable Development Goals (SDGs) specifically Goal 3, which aims at ensuring healthy lives and promoting well-being for all of all ages. 32 The outcome of this goal is the reduction of maternal mortality, which, in part, can be achieved through strict adherence to ANC. Working closely with women to get insight into some of the challenges that hinder the successful adoption of eHealth, to a certain extent, also contributes to SDG 5, which aims at ensuring gender equality and empowering all women and girls. One of the outcomes of this goal is ensuring full participation of women in decision-making by promoting the empowerment of women through technology, which this research set out to understand. Exploring barriers of eHealth adoption is therefore very important for informing programs intended to improve antenatal care utilization in resource-constrained communities.
Across different disciplines of health, transport, banking and education, several theoretical frameworks have been used to try and understand the user's acceptance of technology and the factors that influence adoption. These frameworks include, but are not limited to the Theory of Reasoned Action (TRA), 33 Diffusion of Innovation Theory (DIT), 34 the Motivational Model (MM), 35 Unified Theory of Acceptance and Use of Technology, 36 the Theory of Planned Behaviour (TPB) 37 and the most widely used Technology Acceptance Model (TAM). 38 These theories aim to explain usage behaviour considering a variety of independent variables in different environment settings. 39 The uniqueness with unified theories of acceptance and use of technology (UTAUT) is that each of the constructs in the TRA, DIT, TPB, TAM, MM, Social Cognitive Theory (SCT), 40 pertains to one of the UTAUT's main constructs and measurement items. 41
UTAUT has been adopted in several studies such as: assessing students' needs for English eLearning websites 41 ; evaluating older adults’ perspective on social communication technologies 42 ; ascertaining preservice acceptance of ICT integration in the classroon 43 ; market assessment acceptance 44 ; and evaluating ICT adoption among medical doctors. 45 Specifically in ANC, UTAUT has been used to explore midwives’ need and intention to adopt electronic integrated ANC, 46 assessing nurses’ adoption of hospital electronic information management systems, 47 determining intention to use a mobile nursing application 48 and clinician adoption of health information system. 49 Very few studies have explored challenges impeding the uptake of eHealth technologies in routine ANC practices among expectant mothers using UTAUT, which was the purpose of this study.
The UTAUT model
Recent research indicates that UTAUT is the most predominantly used model to predict and evaluate technology acceptance.50,51 UTAUT model was developed by Venkatesh et al. 36 bringing together eight different models of technology acceptance, diffusion and use, including TRA, 33 TPB, 37 TAM, 38 MM, 35 combined theory of planned behaviour/technology acceptance model (C-TPB-TAM), 52 the DIT 34 , Social Cognitive Theory 40 and the Model of Personal Computer Utilization (MPCU). 53 The UTAUT model explains ∼70% of the variance in behavioural intention ranking better than the eight existing models. 36 Several qualitative studies have used UTAUT to assess technology acceptance42, 54, 55giving credence to adopt it in this study.
The UTAUT model in Figure 1 contains three independent constructs, that is, the performance expectancy (PE), effort expectancy (EE) and social influence (SI) directly influencing behavioural intention (BI) while the construct of facilitating conditions (FC) is asserted to impact usage behaviour. 36 Within the model, there is age, gender, experience and voluntariness to use considered as variables meant to moderate the influence of the four independent constructs on BI and use behaviour. 36

The unified theories of acceptance and use of technology (UTAUT) model. 36
According to Venkatesh et al., 36 the performance expectancy is ‘the degree to which an individual believes that using the system will help him or her to attain gains in job performance’; effort expectancy is ‘the degree of ease associated with the use of the system’; social influence is ‘the degree to which an individual perceives that important others believe he or she should use the new system’; and facilitating conditions refers to ‘the degree to which an individual believes that an organization and technical infrastructure exists to support the use of the system’. Behavioural intention is the willingness of the respondents to use the system and use behaviour is often operationalised by a self-report of respondents of their degree of current system usage.
Materials and methods
Study design
This study employed a qualitative design based on UTAUT to collect data on the barriers of eHealth adoption in routine antenatal care. Specific data on expectant mothers was collected using face-to-face semi-structured interviews. The guiding philosophy for conducting this research was interpretive epistemology using inductive reasoning influenced by the ontological underpinning of critical realism. An interpretive approach was used because it identifies the presence of the participant's perspectives as primary sources of information analysed against cultural and contextual circumstances. 56 Critical realism is a belief that we have a limited understanding of the real world out there, hence knowing the complex reality demands use of multiple perspectives. 57 The purpose of this study was to explore challenges that impede the use of eHealth technologies in routine antenatal care practices among expectant mothers in Uganda. To achieve this, the following questions in Table 1 were used based on the five constructs of the UTAUT. The perceptions of expectant mothers were structured along with the UTAUT constructs of performance expectancy, effort expectancy, social influence, facilitating conditions and behavioural intention.
Interview questions following the five constructs of the UTAUT model.

The use of the qualitative approach was suitable because this study revolved around getting the participant's perception and sentiments on the challenges of eHealth adoption, hence there was a general feeling that these thoughts would have been missed if another research design was adopted.
Study setting
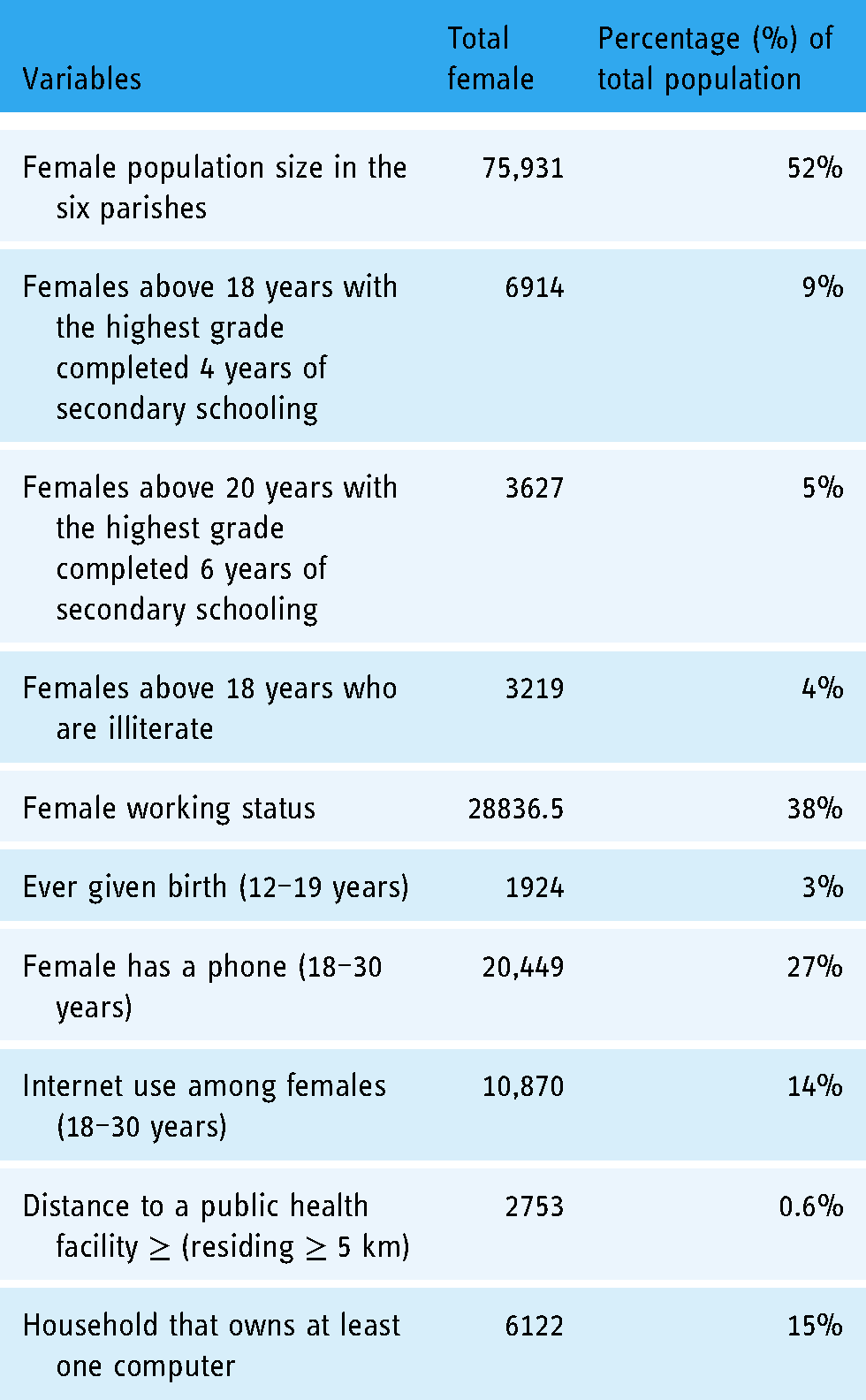
Kampala has a total of 1458 health facilities, of these 26 are government-owned, 1371 are private-for-profit and 61 are private-not-for-profit. 58 Of the 26 government-owned facilities, 11 offer antenatal care services to the public. The study focused on six of the 11 health facilities located in Mengo Kisenyi, Kasubi Kawaala, Komamboga, Kitebi, Kiswa and Kisugu, which partly make up the low-income suburbs of Kampala. This area has a total population of 145,020. That is about 1% of Kampala City's residents who are served by these health facilities. Of these, the composition of the female population is 52.5%. Census data was used to describe the socio-economic profiles of the study participants (Table 2). Nine percent of the females completed ordinary level education, 5% advanced level education and 4% above 18 years are illiterate. Similarly, 3% between 12 and 29 years had given birth, 38% were working, 27% possess mobile phones, 14% used the internet and 15% of the households owned a computer. On average, 0.6% of the participants stayed 5 km or more from a health facility. The data was used as the basis for selecting the study population.
Overall profile, statistics, and demographic characteristics by Kampala City’s underserved Parishes, Uganda. 59
Health facilities that provide free basic and comprehensive obstetric antenatal care services to expectant mothers were chosen. Kampala, a heavily populated city was of particular interest because (i) it is a primate city with a wide range of agglomeration of economic and socioeconomic activities; (ii) it is the largest population centre with wide mobile coverage and digital healthcare services, (iii) 30% of its population have access to internet unlike their counterparts that score at 9% and (iv) Kampala is the only town with 4G/LTE. 60 A higher proportion of female individuals in Kampala owned smartphones (18%) compared to male individuals (13%). 61 Kampala is Uganda's national and commercial capital bordering Lake Victoria with an estimated population of 1,680,800 people covering an area of 3263.3 square miles. It is reported to be among the fastest-growing cities in Africa, with an annual growth rate of 4.03%.
Health facilities were purposively selected while study participants were selected based on three broad classifications; (i) proximity to the health facility (within a radius of 15 km), (ii) health measures (gestation, gravida and parity) and (iii) socio-economic status. We used education and literacy as a proxy for socio-economic status.
Participants Selection
A total of 305 expectant mothers were drawn from Mengo Kisenyi health centre (HC) IV, Kasubi Kawaala HC III, Komamboga HC III, Kitebi HC III, Kiswa HC III and Kisugu HC III during antenatal care clinic days. In all these facilities, ANC services are offered between 9:00 am and 1:00 pm. At the facilities, the research team randomly selected the expectant mothers who were either at the pharmacy, entering or exiting through the main gate, or those exiting the examination room or laboratory. At that point, verbal consent was sought and phone numbers were exchanged, which were later used to schedule interviews, typically within 48 h. Upon receiving verbal consent at the health facility, the research team collected some information on demographics, gravida, gestation, and parity to ascertain the eligibility of the study participants, whilst collecting data to determine their level of eHealth adoption, ranked using a scale of 1 to 5 (1 represented those that had never used eHealth before and 5 represented frequent users).
Eligible respondents were telephoned and a meeting was set up to obtain written approval prior to the commencement of the formal interviews. All participants who assented were first asked their language of preference, then presented with a consent form for signing and their rights to participate clearly spelled out. After thorough scrutiny of the inclusion criteria coupled with those who declined to participate after being telephoned (citing reasons like privacy, busy schedules, lack of spousal consent), the number dropped from 305 to 115 participants. Selection bias cannot be completely avoided, however, the rigor in the selection process we employed aimed at minimizing this possibility. This whole study took five months between January and May 2019.
Inclusion criteria: Expectant mothers aged 18–49 years residing in Kampala and its outskirts who could speak English or Luganda were eligible for the study.
Data collection
Face-to-face semi-structured interviews were conducted with 115 expectant mothers because they gave researchers the flexibility to navigate and probe participants’ viewpoints on the challenges of eHealth adoption. Four research assistants (RA) and the lead researcher (HKN) conducted the in-depth interviews at the homes of the participants. Using research assistants during the exercise was to a certain degree minimize bias issues. The research assistants who were university graduates were trained in qualitative data collection methods, objectives of the research, dialogue management, and how to respond to participants of a different disposition. Similarly, basic training in transcription, coding and analysis was done.
The interview guide was in English, but the research team used both English and Luganda (a local dialect that is widely spoken in the central region of Uganda) during discourse to allow those who could not comprehend English to participate with ease. The research team took notes during the interviews; however, all sessions were audio-recorded. The interview guide was composed of questions that explored the challenges that hinder the use of eHealth technologies during ANC and recommendations to improve eHealth adoption among expectant mothers. Each interview took an average of 45 minutes to complete. The majority of the participants preferred having the interviews during mid-morning hours because they had to first finish their house chores. A pretest was done with the expectant mothers of Wakaliga, Rubaga division to determine that the respondents will understand the questions as well as ascertain the validity of these questions. One repeat interview was conducted with seven mothers to help demystify some responses that were not clear in the first interviews. Interviews were conducted at the homes of the respondents to allow participants to freely express themselves without feeling pressured.
Interviews followed topical trajectories however, the conversation slightly pivoted away from the main questions to gain deeper insights into the participants’ views.
Data analysis
Responses from the qualitative survey were analysed within 2 months. Thematic analysis using template analysis was adopted using preconceived themes based on the UTAUT constructs. Transcripts and researchers’ notes were compiled to identify common patterns, which were later coded and validated by the four RA's, the lead researcher (HKN), and the second author (TJO). AQUAD 7 software was used for transcription; however, minor improvements were made to make the transcription 100% accurate particularly in cases where participant utterances were in the local dialect. The lead researcher, TJO and the four research assistants participated in the transcription process. For each researchers’ transcriptions, the frequency of responses to a particular question was documented and compared across other researchers’ transcriptions; hence, analysis for each group of respondents was developed. This was done to identify common patterns, similarities, and differences in responses. The lead researcher employed inductive reasoning which begins with a detailed observation of the world followed by empirical generalizations and identification of preliminary relationships. 62
The data was analysed to help explain the current challenges that impede expectant mothers from using eHealth initiatives during their ANC routine practices. Also, it provided an insight into the possible recommendations that could drive adoption. Uploaded transcripts were carefully studied to get insight into the data collected; coded to provide an overview of the disparate data, 63 and clustered to identify patterns and generate themes. A deductive approach to theme identification was employed since we had preconceived themes.
Coding was done in two phases; the RA's, who essentially used descriptive codes to summarize detailed data, did the first level coding and, the second level coding was done by HKN which was interpretive, focusing majorly on pattern codes aimed at giving more inference to data by clustering data into a smaller number of more meaningful units. In the first level coding, the RA's generated 56 codes, and after thorough scrutiny, overlaps, ambiguous, irrelevant and redundant codes were integrated or discarded leaving 21 codes in the second level coding (pattern codes), which were further collapsed into five preconceived themes.
To understand the distribution of the demographic characteristics of mothers and test the independence of the variables, coded data was processed using IBM SPSS statistics. This was further analysed using descriptive statistics and Pearson's chi-square illustrated in Table 3.
Demographics of the respondents.

To eliminate researcher bias and prejudice, the second author (TJO) with a good research trajectory coded part of the data (pattern codes), henceforth, discussions of the similarities and differences in coding were held. To ascertain the validity of the findings, the analysis and all coding instances (first level codes and pattern codes) were first given to the study participants and later to two independent researchers (with doctorates in community psychology and ethical sociology) to further audit the findings. Researchers unanimously agreed on the coded data which was later compared against those of the study participants and independent researchers for purpose of building consensus. This rigorous process can ascertain largely the level of authenticity of the analysis process.
After transcription, a subset of five interviews were gradually examined until all were added to the template. Using a clustered analysis of five interviews offered a good cross-section of the insights and views covered in the entire dataset. For each interview examined, if it offered new insight, it was compared against the already defined themes in the template, and if it did not fit, then a new theme was created. This iterative process involved defining new themes, modifying existing ones, and to a certain extent, especially where redundancy was registered, some themes were discarded which left the five preconceived themes (PE, EE, SI, FC and BI). The themes were a result of the pattern codes created in the second-level coding. To avoid misrepresentations, data errors and collecting feedback for theme enhancement, the generated data was validated with the seven respondents, and the feedback collected was used to strengthen the themes. The resultant template is shown in Figure 2.

Final version template.
Results
Table 3 shows the demographic information of the respondents, uptake of eHealth systems in ANC and the digital technologies used to access ANC.
Results in Table 3 indicate that 44% of the respondents had completed primary school education while 29% were not educated at all. At the time of the study, majority (57%) were between 18 and 30 years of age, 54% had 1–3 children, 33% were married and 66% were unemployed. More than three quarters (89%) had never used eHealth for ANC and the remaining 11% predominantly used handheld devices such as mobile phones to access ANC services. Whereas only 13% of the participants had used eHealth during their ANC routine practices, 18% had used it to access other medical services. This may summarily indicate how unpopular eHealth is in ANC service.
Figure 3 shows the number of times a sub-theme was mentioned in the interviews. This helped in providing insight into the challenges that were perceived to be greatly influencing the uptake of eHealth technologies among expectant mothers in Uganda.

Expectant mother's opinions on the challenges that bar eHealth adoption in routine antenatal care practices.
Results in Figure 3 reveal that facilitating conditions had the greatest contribution to the low uptake of digital health technologies. Specifically, illiteracy 74 (64%), lack of prior training before deployment 60 (52%), lack of user involvement during development 62 (54%) and high data costs 63 (55%) scored highly in this theme. Spousal support 5 (4%) and unreliable eHealth systems 9 (8%) received the least number of mentions, whereas limited knowledge of the benefits of eHealth systems 93 (81%) scored the highest, thus alluding to the most significant influence on eHealth adoption.
Responses from expectant mothers
Our findings came from the objective analysis of the data and to the best of our knowledge, no research has explored the challenges that encumber expectant mothers from using eHealth initiatives during ANC in Uganda, this is the first of its kind. The analysis concluded with five major themes: performance expectancy, effort expectancy, social influence, facilitating conditions and behavioural intentions. Using template analysis, we adopted a bottom-up approach, which started with low-level pattern codes, incrementally building into high-level themes. Figure 3 demonstrates the number of times a challenge was mentioned by a given respondent during the interviews. [Note: Quotations are anecdotal narratives from the respondents to give the reader what exactly transpired.]
Performance expectancy
Under PE, the perceived utility of the eHealth systems was the only sub-theme that was identified.
Perceived utility of the eHealth systems
Participants perceived existing eHealth systems to lack the ability to address critical maternal health issues like basic and emergency obstetric issues. ‘The available health systems are not meant for maternal health’, said one mother whose opinion did not differ from those of other mothers. A mother who shares her frustration about these health systems stated that; These systems have got nothing unique about them. I have not come across one that predominantly addresses maternal issues, hence I don't see value in investing time to explore others.
Respondents who had tried to use some eHealth systems revealed that they lacked depth with many having limited functionalities, thus their successful adoption in antenatal care is a dream far from being achieved. ‘… If you wanted to measure blood pressure, monitor fetal and maternal heart rate, you are required to have a minimum of three applications. These are too many to be on the phone …’ said one mother. Another mother also expressed her frustration with many eHealth systems that seem to have few services, which sometimes are not related to ANC. ‘I have not seen any eHealth system with assorted services’, revealed one mother whose sentiments coincided with the opinions of many other participants. Respondents advised tech-innovators to develop systems that can offer a range of services if systems are to be widely adopted. They further advised Ministry of Health to steer the development of systems that predominantly address maternal health issues.
Effort expectancy
Usability challenges associated with some applications were identified under effort expectancy.
Usability issues of some applications
Some mothers found some applications with navigability issues, hardly understandable and with less user-friendly interfaces. ‘Since I am not tech-savvy, when I log into a system that I hardly can teach myself, I never use it again’, narrated one mother. Other mothers who were in agreement with this statement, further expressed their discontent with some systems whose registration process is lengthy with many irrelevant sections, while other systems had many graphical misalignments. Participants advocated for simple systems that would be easy to understand even in circumstances where training is not done.
Social influence
Lack of spousal support was the only social factor that was cited as a challenge impeding mothers to use eHealth technologies.
Lack of spousal support
Some mothers did not use technology simply because their spouses were not strong advocates of these ‘alien systems’. This worked against them especially those without smartphones, money for data, and were illiterate. One mother narrated and quoted the husband's words verbatim, ‘… you want to be a wiseacre, technology is for the white people …’. This demonstrates the challenges mothers face especially where spousal support and consent are paramount. Mothers advocated for an inclusive technology-based system that has spouses actively involved in their ANC practices.
Facilitating conditions
Facilitating conditions that inhibited the adoption of eHealth systems were: not involving users during the system's development, lack of eHealth systems that link mothers to doctors, not training users prior to piloting the system and lack of technical support. Furthermore, the cost of data services, irresponsive healthcare providers, intermittent internet connectivity, power issues, lack of computers and smart phones, illiteracy and unreliable eHealth systems were facilitating conditions impeding eHealth adoption.
No user involvement during the development of eHealth systems
The development of most eHealth systems does not involve prior engagement with the beneficiaries which makes many shun the systems. Mothers cited this as a hindrance to eHealth uptake viewing them as alien systems while others felt no obligation of using something that they were not part of from inception. One mother stated; The people who develop these systems do not know what we want, that is why we find these systems with many irrelevant features yet the most essential ones are not implemented. If the developers do not feel my participation is important at the initial phase of development, then why should I be involved at deployment?
Dumping the system on them, as some mothers purported, made them feel like a testing ground because many are oblivious of the existence of these systems. They, however, advocated for inclusion during the development of these systems.
The lack of eHealth systems that link mothers to healthcare providers
Many mothers cited the lack of systems that connect directly to healthcare providers. ‘Most systems do not connect us to the doctors’, said one mother. Other mothers equally had interacted with different systems like ‘baby center’ but it has no link to a doctor in case of further inquiry. One mother whose sentiments coincided with those of other mothers narrated, I always want to know the development of my baby in the womb, so I use a pregnancy application called ‘baby center’ that gives a week by week fetal development. Sometimes I wish to ask a few questions but this application does not have online doctors.
When asked if they have ever used any application whether web or mobile to interact with the healthcare providers, they affirmatively declined citing the lack of such systems in Uganda. They expressed the need for such systems to help in decongesting hospitals and also be an avenue of quick access to information and services.
No prior training conducted before piloting these systems
There is no formal user training conducted before the piloting of these eHealth systems which is aggravated by the non-involvement of users during development. This increases usability issues and low uptake. Many respondents found it hard to use systems that they were not acquainted with. ‘How do you use something you do not know about?’ asked one mother. ‘Some systems are very hard to navigate’, another mother emphasized. One respondent stressed that; I am not technically proficient in software and hardware usage. This is exacerbated by my low level of education and my inability to comprehend English. With all these factors, it becomes hard to use sophisticated technology. I wish innovators take time to educate us about these systems rather than assuming that we know.
It was evident that training users was a key aspect in system adoption as some respondents demonstrated willingness to use these systems if they have the know-how.
Lack of technical support in case of system failure
A few of the participants who had interacted with some of the systems cited the lack of technical support when the systems failed. ‘Where or who do you contact when the system fails?’ asked one mother. ‘Why use a system that will not provide me technical support when it fails?’ posited another mother whose frustrations concurred with those of other respondents. This feeling of frustration was a clear demonstration of the deflated morale to use technology in ANC. Mothers advised having a dedicated call centre (like utility companies) or a strong technical support team to help with system problems.
Irresponsive healthcare providers with little technical knowledge of eHealth systems
The majority of the mothers felt that healthcare providers were irresponsive to their needs, citing many as being over-worked, poorly motivated and remunerated. With this perception, systems that required direct interaction with healthcare providers would practically not work even if the systems were fully functional. One respondent stated, There's no single time I go to a health facility and I don't find the midwife moody. Some do not even respond when you greet them which could be attributed to fatigue as a result of the long working hours. It would be worse when subjected to a system, which is viewed by many health providers as additional work.
Other mothers also felt like the healthcare providers were only responsive to mothers of a certain socio-economic class, hence economically marginalised respondents were convinced that using eHealth platforms would be futile. Another respondent whose viewpoint quite surprisingly coincided with many participants narrated that; It is very frustrating to go to the hospital and you do not find a doctor or you find them very busy. How about a platform whose functioning predominantly relies on the availability of a doctor?
Similarly, some women argued that some healthcare providers were not digitally savvy, so even if the will is there, the know-how impedes use. Participants recommended training healthcare providers in both technical and interpersonal skills to improve technology adoption and interpersonal relationships.
The cost of data services
The majority of the mothers stressed their inability to pay for the internet services because they were exorbitantly priced. They felt there was no value for money, especially where the least data package or bundle (15 MB) is charged at 300 Uganda Shillings which is equivalent to $0.06. One mother stated that ‘… sometimes I fail to get money for my ANC visit, food and water, how then can I buy data bundles?’ other participants stressed that their husbands only give them money for necessities. One mother in particular postulated, I am a housewife with virtually no income, it is not possible to buy internet neither is it logical to ask my husband to buy it because he has a lot of responsibilities at home.
To a greater extent, this challenge largely contributes to the slow adoption of eHealth because over ninety percent of eHealth systems are internet-based. Many mothers are not income earners, yet those who are, earn meagrely. Many respondents urged the government to reduce the tax levied on some telecom services because the internet is becoming a necessity in people's lives.
Intermittent internet connectivity
Those who could afford to subscribe to the internet were disappointed with poor internet connectivity due to the remoteness of some places, poor infrastructure, and network coverage. One mother, in particular, posited that, Internet in this area is not good at all. I cannot sustain a Whatsapp call for even 3 minutes, calls keep dropping. How then can I use a system that requires constant internet connectivity? Sometimes even the voice calls drop at a considerably high rate.
Some mothers were particularly stressed about the slow internet speeds resorting to using the service during off-peak hours between 8 pm and 7 am. Participants were urging for the improvement of network infrastructure to enhance internet connectivity.
Unreliable eHealth systems
Respondents were concerned with the reliability of the system and health workers. Many intimated the general lack of empathy by the doctors during the physical visits and were highly convinced that with the system, it could be worse. First, there was a general concern about the system's inability to function as needed and the lack of doctors to offer the services, this affects the reliability of the system. One mother posited; I do not have trust in these Ugandan systems as they are susceptible to being off than on. Nothing in Uganda is sustainable so it is a waste of time to even imagine that a system can work for even a week.
Many respondents shared the same concerns and indicated that it would be sheer luck to have a fully functional system without any glitches.
Electricity/power issues
Participants described power as a big challenge in some areas especially due to the advent of load-shedding. Even those with stable power supply had issues with power tariffs which render many to voluntarily stay in a blackout. One mother stated that ‘It was cheaper to use a kerosene lamp …’ while some resorted to solar bulbs which are used at night for lighting purposes. Many could not pay for power because they were financially handicapped thus using electric gadgets like computers were not possible. One mother stated: When I want to charge my phone, I take it to the mobile phone charging kiosk and I pay UGX500 only.
A reduction in power tariffs is something that many advocated for, not for charging purposes only, but for other things like lighting and cooking.
Lack of computers and smartphones
The majority of the mothers lacked handheld devices and computers, that is, laptops or desktops. The most predominantly used handheld devices were ordinary phones that were not smart. They claimed to be having not-so-good quality smartphones with many of such phones having graphical display issues, overheating when using the internet, and having short battery life. One mother described her phone as ‘too cheap to browse any page’ while other mothers did not have smartphones at all. One mother whose sentiments represent the opinions of other mothers narrated that: I do not have a smartphone although I need it. I depend on my husband‘s phone if I want to check for something on the internet. Most times, I cannot use his phone because he works upcountry.
This was not an isolated case where mothers did not have access to smartphones, hence even where the motivation was undeniably there, the lack of a computer or a decent smartphone made the use of eHealth systems practically impossible. Many respondents advocated for tax cuts on technological equipment because this is believed to lower the prices of such devices.
Illiteracy
It was undoubtedly obvious that some of the participants were illiterate, attaching no significance to technology and antenatal care at large. Some mothers could hardly communicate with the care providers because of illiteracy and the language barrier. A mother, whose assertions corroborated with the opinions of other mothers stated that, I cannot read anything on my antenatal care card neither can I write. I always ask doctors to translate the lab results so that I understand and be in a position to explain to my husband who is also illiterate.
Relatedly, another mother alluded to her infrequent utilization of ANC to the fear of being ridiculed by nurses because of her inability to expressively describe her health condition which is largely due to the low self-esteem as a result of illiteracy. Other mothers alike shared similar concerns and a mother whose sentiments coincided with those of many mothers stated, My educational background is not that good and my ability to read English text is so bad that I cannot even use mobile money services on my phone, it's my son who always helps me. That technology is for the educated who can navigate the system with ease.
Many mothers were digitally illiterate, downplaying the relative importance of eHealth systems, while others simply did not believe that service can be offered digitally to the satisfaction of the user. They lacked knowledge of navigating computers and using the internet. Illiteracy impedes access to information, limits ANC visits to hospitals, and subsequently works against technology adoption. When asked how best they can be helped, many recommended having these systems in multiple local languages.
Behavioural intention
Limited knowledge of the potential benefit of eHealth systems
It was evident during this discourse that many respondents did not appreciate the potential of eHealth systems in easing access to ANC services, hence no relevance to use. One respondent described eHealth technologies ‘as platforms for people in urban areas’ while another mother, ‘thought that they are for the rich and educated class of people’. One mother whose opinion represents the sentiments of other mothers narrated: I do not see the difference between being physically in the doctor's clinic and using the system. How can a doctor do a physical examination using a system? Also, how do I know that I am not talking to a robot? I do not think I can use those systems because it is even hard to operate them.
Other mothers alike thought that using eHealth systems will only widen the gap between them and doctors yet ‘… at the time of delivery, you want to go to the hospital when the doctor has seen you before …’ Similarly, some mothers thought that using eHealth initiatives to exchange pertinent information like multimedia information such as ultrasound scan images, lab tests etc. was intricate and a waste of time. Other mothers thought that using a mobile phone to measure the foetal heart was not effective, like one mother who stated that, Using a mobile phone to listen to the heart of the baby cannot be the same as a midwife using pinard stethoscope because the latter is globally recognised and the former is an imitation that can‘t give accurate results.
Misconception about the existing systems
There was a general misconception among women that since many systems die at the piloting stage, it is equally not important to use any at all. This greatly affects the willingness to use new technology even if its utility has been tested and surpasses the usefulness of other systems. Many participants felt no urge to use eHealth systems because they are not sustainable in the long run.
Lack of trust in the eHealth systems
Many respondents largely perceived some systems to be intrusive asking a lot of information yet the safety of this information is sometimes not guaranteed. One mother vehemently detested the use of systems because she thought the information would leak, in her words, she postulated ‘… I have heard that information can be used to blackmail people …’ another mother also expressed her worries stated, ‘I have my medical information that I wouldn't want to get in the eyes of the public, so I cannot use systems’. Many mothers did not trust having their personal information stored in these systems for fear of being mishandled.
Discussion
Adopting eHealth in the routine ANC practices in Uganda is complex. This study set out to explore the barriers that hinder the successful adoption of eHealth among expectant mothers. To the best of our knowledge, no research has explored eHealth adoption among expectant mothers in Uganda, making it the first of its kind. The study revealed that the lack of trust in eHealth systems, usability issues, lack of spousal support, perceived usefulness of the system and irresponsive healthcare providers were barriers to adoption. Equally important was the lack of computers, systems that link mothers to doctors and misconceptions about existing systems. Reliability issues, lack of technical support, intermittent internet connectivity and electricity issues were also pointed out as technical barriers to adoption.
Performance expectancy
Perceived utility of the eHealth systems
There was a common belief among mothers that the existing eHealth systems do not address pertinent issues in maternal health specifically antenatal care. Several scholars have emphasized the importance of system usefulness as perceived by the users36–38 and have underscored its role in accelerating technology acceptance among users. As reported by Namatovu and Devex Partnerships,30,64 use of digital health systems can substantially improve pregnancy outcomes, although a study conducted by Heuvel et al. 65 stressed the need for evidence for health outcomes as a result of eHealth interventions in perinatal care. This study revealed that mothers were very skeptical to use existing systems for their perinatal needs which, in the end, hampers their willingness to use digital health systems. In a study conducted by Namatovu, 9 mothers were not ready to use systems that were perceived not useful. To a certain extent, some systems have been perceived as not useful partly because, users have limited knowledge to navigate the system, the lack of digital skills and the failure of many systems at infancy, which in the long run affects the willingness of many potential adopters to embrace new technology.
Effort expectancy
Usability issues
The study revealed usability as one of the challenges that bar the adoption of eHealth technologies in routine antenatal care practices among perinatal mothers in Uganda. A usable product should be easy to learn, use and perform its functions in the proper environmental context. 66 However, many mothers reported that some applications were hard to navigate with unfriendly user interfaces, a fact that can be corroborated with other similar studies.23,67 The correlation that exists between usability and actual system usage cannot be disregarded, with several scholars36,38 positively reporting about it. Many mothers reported not being tech-savvy which strongly works against the acceptability of the system should it be found with usability issues. In the Ugandan context, the lack of a usable system coupled with digital illiteracy, poor internet services and the poor attitude of many mothers substantially affects the uptake of many eHealth systems.
Social influence
Lack of spousal support
Mothers reported the general lack of spousal support during pregnancy a fact that is reported in many similar studies.68,69 Pregnancy involves a lot of psychological changes which requires a woman to get support not only from a husband but from within her social network. Many studies have reported husbands detaching themselves from their wives’ antenatal care journey,70–72 which in part, can explain why, even when their wives need to embrace digital technology, their motivation is suppressed.
Although some scholars report no positive effect of social factors on behavioural intentions to use, 73 the role of social support has been reported by Venkatesh et al. 36 as key in advancing technology acceptance.
Facilitating conditions
The cost of data services
The cost of data was cited to be one of the impediments of eHealth adoption, especially since most of these digital platforms are internet-based solutions, a fact that can be corroborated by other similar studies.16,24,30,67,74–77 Apart from the general perception of feeling exorbitantly charged for internet/data, mothers generally lacked money for hospital bills, were dependent on their husbands for necessities and quite a number of them were stay-home mothers. On average, only 38% of the entire female population in this region is working, and because of the social-economic challenges, as revealed in the study, internet subscription was viewed as a luxury.
Intermittent internet connectivity
Similarly, even when all odds are in their favour, the poor network characterised by slow, intermittent and unreliable internet connections especially during peak hours increases the user's vehemence towards technology adoption. This, to a greater extent limits technology uptake, as reported in similar other studies.12,78 From the discourse, it was evident that some mothers were living in areas with poor telecom infrastructure which not only affected the internet but voice services too. Many resorted to utilizing these services during off-peak hours, which makes it less feasible to use digital systems.
The lack of user involvement during the development of the eHealth technologies
Not involving users especially during systems development made mothers feel alien to these eHealth systems. As primary users of technology, active involvement right from inception is paramount for successful adoption. Co-development has been emphasised as a pedestal to technology acceptance and creates an avenue for users to tailor systems to suit their needs. It was revealed that the current systems are predominantly messaging platforms yet ANC is a broad domain consisting of basic and emergency obstetric care. Because prior consultations are not made with users, these vital obstetric services are unknowingly disregarded in many eHealth systems. It should also be emphasized that currently, there is no system in Uganda that comprehensively deals with antenatal care issues, save for data capture or text messaging. Those that try to mirror this, are limited in breadth as reported in other previous studies.9,17,79 When users are involved, these pertinent obstetric services can be integrated into the systems, which can potentially increase uptake.
The lack of training prior to piloting of the systems
The lack of basic training on how to use the systems increases the mother's complacency to use eHealth systems. It was evident that mothers were tech-illiterate which made it hard to navigate the system since many were not trained and lacked good formal education. Most users are not given prior skills in ICT use which creates a state of technophobia, aggravated by the lack of technical support during turbulent times of system glitches. A combination of all those factors leaves no room for system acceptability. The studies conducted by11,20,80 cited the lack of training as a major impediment to the adoption of eHealth systems and information systems at large. Some applications are hard to use particularly for people who are first-time digital users or novices. Systems with sophisticated user interfaces that are not intuitive to traverse make them even more complex to use. In a study that was conducted by Schreiweis et al. 79 in Germany and Spain, experts highlighted usability as one of the major challenges impeding adoption, which can be alleviated through training users.77,81,82 Other studies 9 have also delineated the relative importance of technical know-how in the successful adoption of the same.
Illiteracy
A considerable number of mothers were either illiterate or suffered language barrier problems. Many could not use eHealth systems because of linguistic issues yet most of these technologies are predominantly in English. The study revealed that some mothers could not read nor comprehend the content on their ANC cards which makes them rely on other people for translation. This is evidence that mothers cannot use digital technologies as may be reported in other studies.79,80,83 There is a strong correlation between digital literacy and technology use, 84 hence, for one to competently use digital technologies, they must have attained a certain level of education and ICT skills. In relation to this study, illiteracy was in two-folds, (i) mothers who could not read or write and (ii) digital illiteracy which technically is the lack of ICT skill to operate a digital gadget. For both categories, mothers were not adequately competent. This, coupled with the limited focus of eHealth content in local languages, reduces the uptake of eHealth technologies.
The lack of systems that link mothers to healthcare providers
Systems are as important as the value they give to the users, thus, this linear relationship implies that users need to appreciate the value of the system in order to embrace it. This value in the antenatal care domain, partly involves, a mother having a direct link with the healthcare providers. The study revealed that, currently, there are no such systems apart from an antenatal care studio 9 which also requires scaling to include other actors like doctors. Other available systems are unilateral and SMS based which limits collaboration and value accrued from synchronous systems. This can explain why mothers are reluctant to embrace such digital health technologies.
Irresponsive healthcare providers with inadequate digital skills
Mothers felt like the healthcare providers did not have their interests at heart especially when they visit hospitals for antenatal care. Healthcare providers ignore mothers, are impolite and sometimes delay to offer them services, which, as reported by mothers, are attributed to the overwhelmingly busy schedules of health providers. This can be corroborated by many other studies.85–88 This kind of treatment from the service providers widens the access gap yet digital technologies, which are known to bridge this gap, have not been widely utilized. Some health providers were reported not to be digitally literate, a finding reported in other studies,23,89,90 whilst many deliberately shunned systems because they were considered time consuming. The health provider's temperament coupled with their poor ICT skills discouraged many mothers from using technology.
Unreliable eHealth systems
Mothers were wary about the reliability of the eHealth systems in Uganda as many, who had used them before, did not have a pleasant experience. This, to a certain extent, can be related to other studies16,67,75,91 where systems could be off because of software, hardware, telecommunication or power issues. A reliable system should be able to support and perform the tasks for which it was intended, and since some eHealth systems are synchronous, this equally requires the users to be available in real-time. For mothers, this was unattainable relating it to the bad attitude exhibited by the healthcare providers. Whereas this subtheme received very low mentions, some studies30,82 have emphasized the relative importance of reliable eHealth systems in influencing uptake.
Electricity issues
Electricity is still a very big challenge in many developing economies yet a reliable and functional system depends on the constant supply of power. Many mothers intimated the lack of stable power supply because of load shedding while others felt that the power tariffs were too high, thus could not afford them. The issue of power supply has been reported in many studies16,76,92,93 as being one of the hindrances of digital penetration in most under-served communities of Uganda. In a country where the majority of the population are still using kerosene lamps, digitization is improbable. With such challenges, eHealth uptake in certain communities may not be achievable since these infrastructural issues are beyond the user’s control.
Lack of computers and smartphones
Whereas many mothers had demonstrated the willingness to be part of the digital spectrum, the lack of technology devices that are a medium of access, barred many from using health systems. Although these seem to be minimal problems in the developed world, many studies74,89,94–97 in Uganda are reporting this as one of the biggest challenges in technology access for both the service provider and service users. In a study that was conducted in the rural post-war conflict of Northern Uganda, researchers 95 noted that five out of the eleven health facilities visited did not have computers. This goes to show that healthcare providers and service seekers are technologically challenged.
Lack of technical support in case of system glitches
The majority of the women admitted not being tech-savvy and several others were illiterate. This means two things (i) providing users with usability training prior to system use and (ii) being able to offer technical support should the system malfunction. As posited by mothers, none of these are available which leaves many wondering whether those advocating for technology uptake have are realistic. This finding is consistent with other studies.24,74,75,96 With the lack of this support, coupled with the language barrier and limited digital knowledge, it is highly unlikely that adoption of eHealth can ensue.
Behavioural intention
Limited knowledge of the potential benefits of eHealth systems
The survey revealed that the majority of the expectant mothers had little knowledge of the benefits of eHealth systems. This potentially makes it hard to appreciate the value of digital technologies in bridging the access gap. With many perceiving these technologies as not useful, it is not surprising that eHealth adoption still remains in balance. Although some studies have underscored the importance of digital technologies in maternal health,29,98 some mothers instead felt that these systems are intrusive and would widen the patient-doctor gap, yet many could not envisage service delivery without physical contact with the doctor. The limited knowledge as revealed in other studies,29,30 impedes the mother's ability to use digital technologies not just as avenues of improved interaction and efficiency but also as platforms for improved access, especially in rural areas. The general feeling that these systems were for people of a particular socio-economic status further alludes to the fact that these mothers were not cognizant of the potential of eHealth in enhancing ANC, hence barring their intention to use.
Misconception about existing systems
There was a misconception about eHealth systems and their inability to move beyond the pilot phase and as such, mothers felt no obligation of embracing systems with no full implementation plan. Once potential users become skeptical about the system's continuity plan, uptake becomes substantially low, a fact that many scholars79,99 assent to.
Lack of trust in the eHealth systems
Throughout the survey, several respondents expressed fear of having their information shared and stored in systems they hardly know, a fact that is congruent to other similar studies.16,24,92 Although not directly linked to antenatal care, a study that was conducted by Meyer et al. 24 to investigate the challenges that were encountered in the implementation of a mHealth intervention to enhance tuberculosis contact revealed that community health workers lost trust in the system and a substantial decline in its use was registered. When users mistrust the system, certainly its use will go downhill. The lack of trust can be exacerbated by the lack of digital literacy and usability training which could potentially improve the user's knowledge of the system.
Mothers however recommended factors that would facilitate adoption and eHealth acceptance. These included; having systems developed in multiple local languages; adopting co-development especially at inception, requirements collection and testing of the system; conducting user training to (i) sensitise mothers on the importance of eHealth technology in ANC, (ii) build trust in the systems, (iii) improve digital literacy and (iv) change the attitude and perceptions of mothers. Relatedly, they advised the Ministry of Health and other innovators to have systems that specifically address antenatal care issues and train health care workers in digital literacy and being responsive to the needs of the patients. Important to note was their plea to have the government cut tax on technology devices (computers, phones, tabs) and data services to accelerate adoption and information access. Mothers advocated for competent technical support teams that would extend technical assistance when deemed fit. This creates an avenue to source for solutions in times of system breakdown in the end, build confidence among users to ensure continuity. Many urged the government to cut power tariffs because it was becoming extremely expensive to use electricity.
Conclusions
The facilitating conditions such as illiteracy, lack of training, the cost of internet/data services, the lack of computers and smart phones and the lack of user involvement during the development of the eHealth systems stood out as some of the challenges affecting the uptake of digital health technologies. Furthermore, electricity challenges, the lack of technical support, unreliable eHealth systems, irresponsive healthcare providers and lack of systems that link mothers to health providers were facilitating conditions that hampered adoption. Whereas there is a need for a structural change in health service delivery, effort to change the attitude of mothers and healthcare providers should equally be emphasized, whilst advocating for co-development.
Digital literacy among users in the healthcare ecosystem is paramount to changing attitude and shaping perception. This can be achieved through massive sensitization, 98 training end-users, garnering support at the national and hospital levels. There is need to empower women to appreciate their role in the health service delivery not just as service consumers but also as service advisors. Subsequently, the study revealed the non-existence of functional end-to-end eHealth technologies connecting mothers to health workers. Henceforth, systems that emphasize and promote synergy between care providers and expectant mothers should be of great focus to bridge this access gap. Similarly, further research should look into the development of inclusive eHealth initiatives tailored to specifically address pertinent ANC issues but most importantly, encourage men’s participation to enhance a holistic adoption. This is because of the salient role of men in ANC utilization and thus their involvement is likely to boost women's participation in ANC. Research should also explore challenges that impede eHealth adoption among health providers. Our findings, therefore, conclude that facilitating conditions had much more influence on usage behaviour than the other four constructs.
Strength and limitations of this study
Firstly, the major strength of this paper is that, unlike the previous studies that generalize barriers and facilitators of eHealth adoption, this study was context-specific to the needs of expectant mothers, something that has not been explored before. Secondly, since Uganda is moving towards achieving sustainable development goal 3, which partly aims at reducing maternal mortality through improving ANC utilization, we strongly believe that this research is a key ingredient to the perennial problem of non-utilization of ANC services. Thirdly, this research was inclusive, by having women of different socio-economic statuses to help minimize bias. Limitations of this study were; (i) many women had originally, through verbal consent, accepted to be part of this study, however, they later declined, (ii) barriers at the supply-side specifically healthcare providers were not explored and (iii) the questions particularly revolved around barriers with little flexibility of discussing the facilitators of eHealth adoption.
Footnotes
Sincere gratitude goes out to the management of Kampala City Council Authority for the support extended by staff in the respective health centres especially the sisters-in-charge. Similarly, appreciation goes out to the research assistants and the expectant mothers whose participation in this study was very pivotal. Lastly, we appreciate the support that was extended by Makerere University.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/ or publication of this article.
Contributorship
The authors’ contribution towards this study were as follows; ‘Conceptualization, HKN and HGS; Data collection, HKN. Methodology, HKN, TJO and HGS; validation, HKN, TJO and HGS; Thematic analysis, HKN, TJO; data curation, HKN, TJO. Writing – original draft preparation, HKN; writing – review and editing, HKN, TJO, HGS; supervision, HGS; funding acquisition, HKN, TJO. All authors have read and agreed to the published version of the manuscript’.
Ethical approval
Before the study, consent was sought from Kampala City Council Authority ‘REF: DPHE/KCCA/201/17’. Introductory letters to grant access to the health facilities were obtained from City Hall, the headquarters of Kampala City Council Authority. Also, consent was sought from the District Health Officer of Kampala District. At the village level, consent was sought from the local council leaders. For the women written consent was sought. Respondents were informed of their rights to withdraw at any point of the study.
Funding
This research received internal funding from Makerere University Directorate of Research and Graduate Training and College of Computing and Information Sciences, Makerere University.
Guarantor
HKN.