
Abstract
Industry 5.0 is reshaping healthcare through human-centric design, sustainability, and advanced technologies. However, there is limited insight into how these innovations address the specific needs of people with disabilities. This review aims to examine the role of emerging and AI-driven technologies in enabling disability-inclusive digital healthcare solutions. A comprehensive scoping review was conducted, focusing on studies published in recent years on Industry 5.0 technologies applied to disability-inclusive digital healthcare pathways. Key technologies reviewed include collaborative robotics, virtual reality, telemedicine, and human-centered artificial intelligence. Relevant case studies and ethical considerations were also analysed. The analysis highlighted that Industry 5.0 technologies show promise in enhancing diagnostic accuracy, personalization, and accessibility for people with disabilities. Applications include remote assessments, assistive tools, and adaptive interfaces that improve diagnostic processes. Despite this progress, integration of these technologies remains fragmented, and challenges such as ethical concerns, regulatory barriers, and inclusive design persist. This review uniquely synthesizes these technologies within the framework of Industry 5.0, offering a broader perspective than prior single-technology reviews and proposing a roadmap for the successful implementation that incorporates training, regulatory alignment, interdisciplinary collaboration, social-economic barriers, real-world evidence, and inclusivity across disability types. As conclusion, Industry 5.0 holds significant promise for advancing disability-inclusive digital healthcare. Realizing this potential, however, requires coordinated efforts to address integration gaps, strengthen ethical and regulatory frameworks, and embed user-centered co-design principles. Future research should focus on more developing inclusive, and sustainable diagnostic solutions aligned with Industry 5.0 principles.
Keywords
Introduction
Industry 4.0 (IR 4.0) integrates technologies like the Internet of Things (IOT), big data, artificial intelligence (AI), and automation into industrial processes. 1 The main objectives of IR 4.0 adoption are to enhance efficiency, productivity, and automation by using data-driven insights and connected systems. Smart factory and Cyber Physical Production System (CPPS) are the core elements of IR 4.0 in an industrial setting. 2 IR 4.0 is not typically regarded as a human-focused initiative, and it is also known as a human out of the loop transformation. 2 A new paradigm for a manufacturing environment free from human intervention, driven by product intelligence, machine-to-machine communication, and networking, is promoted through IR 4.0 implementation. 3 IR 4.0 are often criticized for prioritizing efficiency over environmental and social impacts, where sustainability is not the core focus but occasionally considered to reduce cost, especially in terms of improving resource efficiency. 4
Meanwhile, Industry 5.0 (IR 5.0) emerged as an extension to IR 4.0, incorporating social and environmental dimensions. IR 5.0 emphasizes worker skills, knowledge, and their ability to collaborate with robots and machines while focusing on flexibility in the production process and minimizing environmental impact.5,6 IR 5.0 reinforces the co-existence of humans and machines, ensuring automation support for human creativity and customization. 7 Human positioned as partners to machine, focusing on personalization and problem-solving. The key technologies of IR 5.0 are collaborative robots, AI-driven personal assistance, customization-focused systems and techniques enabling sustainability and green technologies.8,9 It is represented by concepts such as sustainability, human-centric values, quality of life enhancement, and mass personalization. 10
Unlike IR 4.0, which emphasized automation and efficiency, IR 5.0 shifts toward human-centric innovation, making social inclusion, personalization, and the well-being of people at the peak of technological progress. This paradigm directly supports disability-inclusive healthcare, which integrates collaborative robotics, explainable AI, and assistive digital technologies, empowering patients and caregivers as active actors in the care process. Besides, ethical AI and human–machine co-evolution guarantee that healthcare solutions are designed around users’ needs, reducing, as a consequence, barriers in diagnosis, daily functioning, and rehabilitation globally. Therefore, the social-responsibility pillars of IR 5.0 encourage inclusive policy Frameworks, which can establish a good alignment between industrial innovation and the United Nations’ Sustainable Development Goals (SDGs 10 and 3) and reduce as a consequence inequalities. 11 In this context, IR 5.0 provides a transformative pathway for the development of healthcare ecosystems, not only technologically advanced, but also value driven-road, accessible, equitable, and responsive to the needs of people with disabilities. Although IR 4.0 supports certain aspects of sustainability at the micro-organizational level, it causes employment disruption, loss of workplace autonomy, the digital divide, social exclusion, overconsumption, and uneven regional development. 12 The European Commission, in a policy brief, stated that IR 4.0 is no longer an adequate framework for achieving sustainable industrial transformation or addressing modern socio-environmental challenges. IR 4.0 falls short in incorporating circulatory into value chains, fostering well-being, and preventing environmental degradation. 13 The key reasons for the transformation from IR 4.0 to IR 5.0 are shown in Figure 1. Despite the growing discourse around the transition from IR 4.0 to IR 5.0, a major conceptual and empirical gap concerning how this transition translates into disability-inclusive healthcare innovation has still not been deeply highlighted. Besides, a very limited number of researchers have synthesized how the human-centric, sustainable, and collaborative values of IR 5.0 can systematically advance health equity for disabled people despite the effort to review the individual technologies' contribution to this topic, such as telemedicine, AI, or robotics. Moreover, the interaction of these technologies with inclusive design principles, regulatory frameworks, and ethical challenges in real-world healthcare delivery is often overlooked by current research. Guided by these considerations, this review seeks to discuss the following issues: (i) How does the transition to IR 5.0 transform digital healthcare toward greater inclusion of disabled people? (ii) Which emergent and AI-driven technologies are currently enabling disability-inclusive diagnostics, treatment, and rehabilitation? (iii) What are the key challenges, ethical considerations, and policy implications involved in operationalizing IR 5.0 principles within healthcare systems?
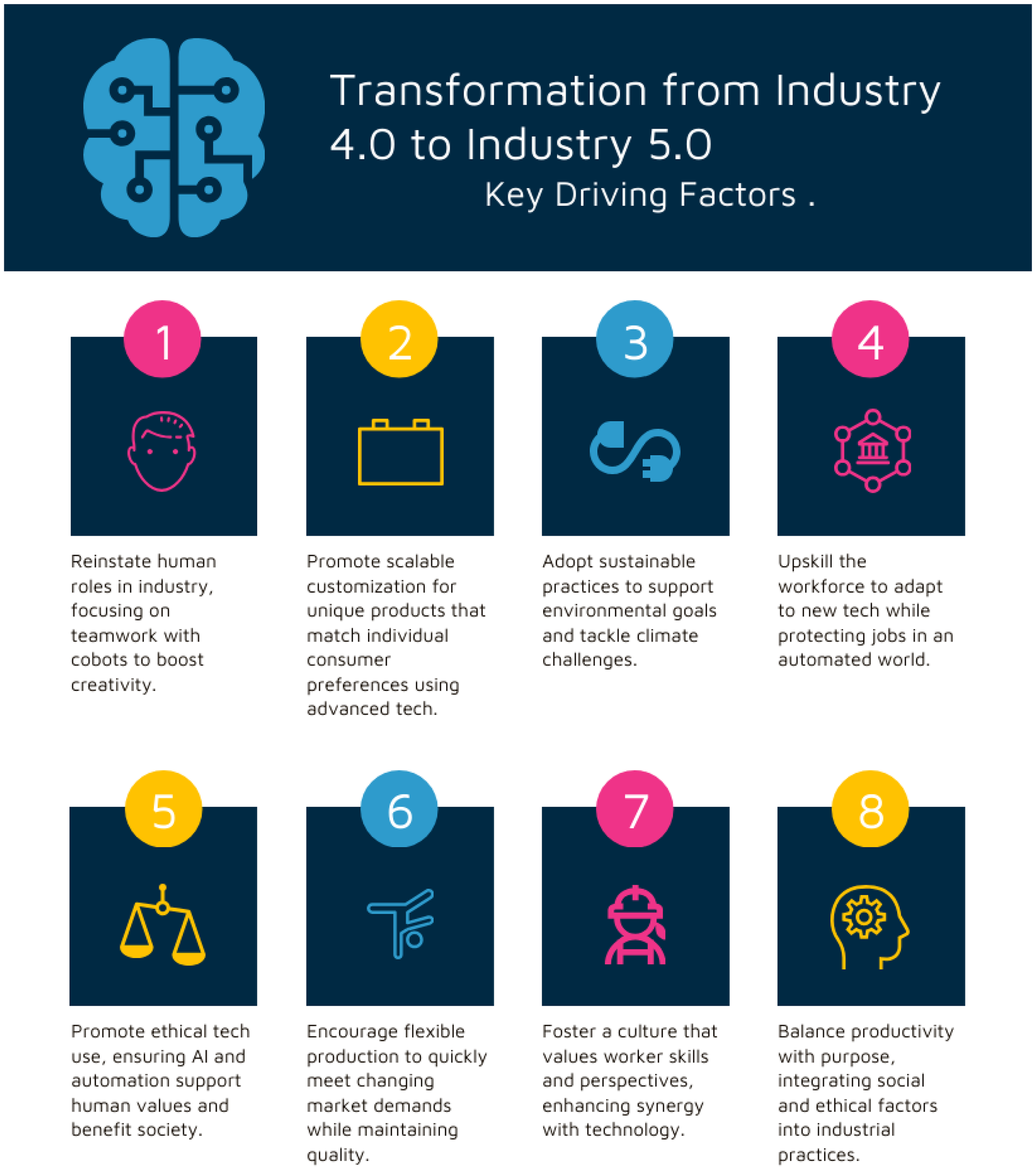
Transformation from IR 4.0 to IR 5.0.
Analytically, this review is guided by the IR 5.0 human-centric innovation framework, requiring reinforcement of social inclusion, sustainability, and resilience for its flow process. This theoretical lens provides the basis for interpreting the transformation of disability-inclusive healthcare systems by AI-driven and emergent technologies. Therefore, the main objective of this article is to systematically examine and integrate current knowledge on the use of emergent and AI technologies for disability-inclusive digital healthcare within the framework of IR 5.0. In doing so, this review seeks to bridge the gap between technological innovation, in field practices and social inclusions, offering a conceptual roadmap for designing equitable, human-centered, and sustainable healthcare ecosystems.
Materials and methods
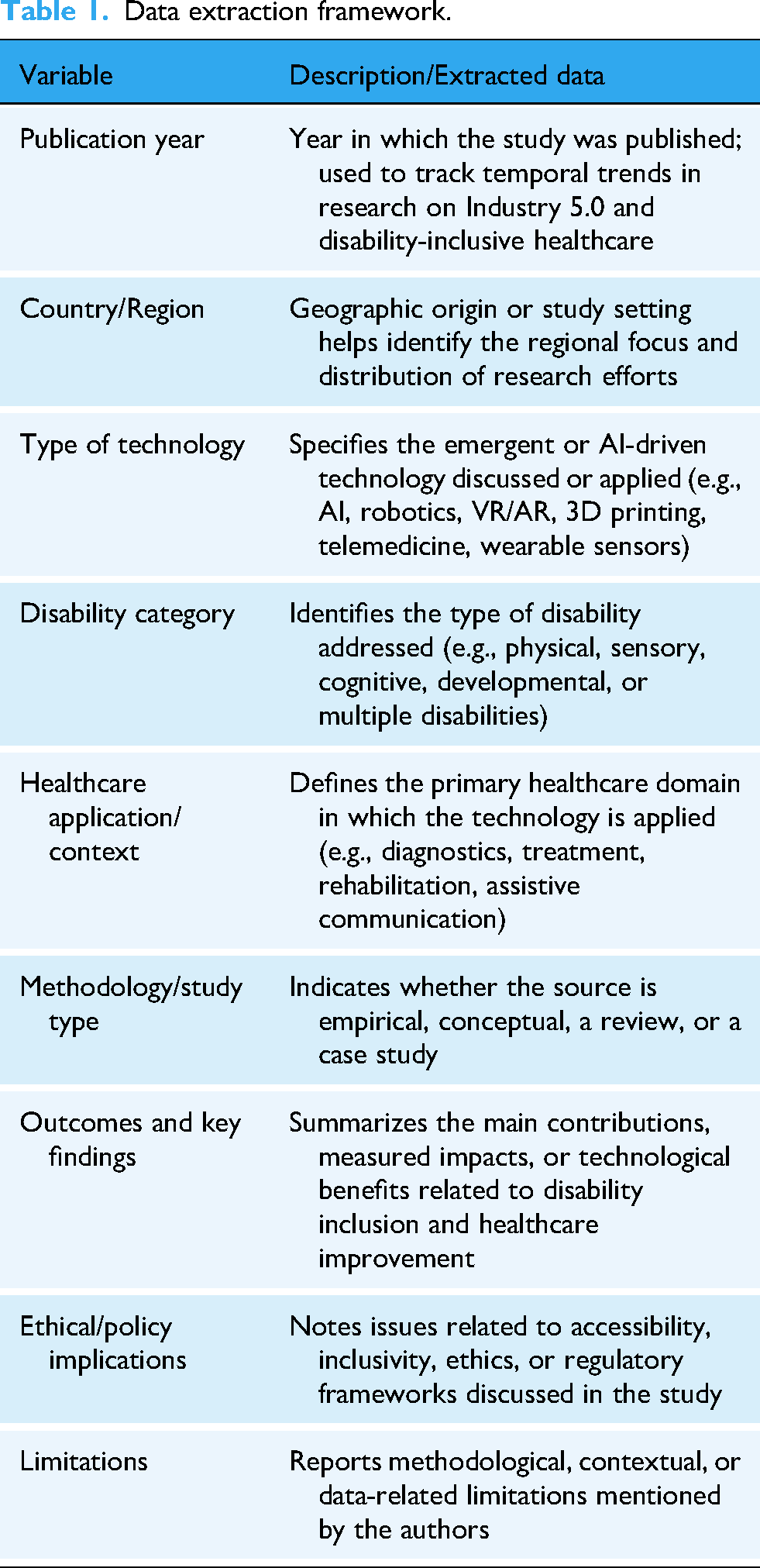
This study adopted a scoping review design, following the framework proposed by Arksey and O’Malley 14 and enhanced by the Joanna Briggs Institute (JBI) for scoping reviews. The scoping approach was selected as it allows the mapping of a broad, interdisciplinary entity that spans emerging technologies, disability inclusion, and healthcare transformation under the IR 5.0 paradigm, fields and topics that are conceptually diverse and complex, and methodologically heterogeneous and multiscale. The review was conducted in alignment with the PRISMA-ScR guidelines to ensure transparency and reproducibility. A formal protocol was developed internally by the research team and applied throughout the research work. However, given the exploratory nature of the topic, it was not registered in PROSPERO, which primarily indexes systematic reviews of clinical interventions. The flow process was conducted in PubMed, Scopus, Web of Science, and IEEE Xplore databases in December 2024. The search combined key terms and Boolean operators as follows: (Industry 5.0 or Human Centric Industry) and (Artificial Intelligence or AI) and (disability or Disability Inclusion or Assistive Technology) and (healthcare or Digital Health or Diagnostics or rehabilitation). Reference lists of key papers as well as relevant reviews were also screened to identify and confirm additional sources. The search was limited to English language publications, from 2015 to 2024, to concentrate on contemporary development in IR 5.0 and emergent digital health technologies. The studies were included when they covering the following criteria: (i) discussed or applied IR 5.0 related technologies (AI, robotics, VR, AR, etc.) in the context of disability-inclusive healthcare, (ii) presented case studies, reviews, empirical investigation, or conceptual frameworks related to the global topic (inclusion, accessibility, or human centric healthcare design), (iii) published in peer-reviewed journals or confirmed conference proceedings. When the studies were focused solely on IR 4.0 or general digital transformation without a healthcare or disability focus, or the source of the information was from non-peer-reviewed materials (opinion pieces, editorial, etc.), the references were excluded. The data extraction framework is detailed in Table 1, in which the different information discussed and evaluated by our teams and other benevolent experts are summarized, such as publication year, country, type of technology, disability category, healthcare application, outcomes, challenges, and limitations. Collected available data were then synthesized narratively and thematically to identify recurring patterns, conceptual gaps across studies, technological trends, and the degree of evolution and incorporation of the characteristics of IR 5.0 in the different healthcare ecosystems. The screening and selection process followed PRISMA-ScR guidelines and is reflected and summarized in the results narrative, indicating the total number of the identified, screened, excluded, and finally retained records for full analysis. Five analytics themes were addressed: (i) the importance of disability inclusion in healthcare, (ii) types and impact of disabilities, (iii) emergent technologies and diagnostics, (iv) role of AI in disability diagnostics and care approaches and strategies, and (v) illustrative case studies and success stories. In front of some limitations such as the heterogeneity of study designs and outcomes measures, and absence of standardized quality appraisal tools, several measures were adapted and well applied: (i) a multi-stage screening and review consensus process to enhance reliability in study selection, (ii) refinement of search terms in collaboration with subject experts in the related field and topic, (iii) inclusion of both conceptual and empirical evidence, recognizing the emergent nature of IR 5.0 and its applications to inclusive healthcare.
Data extraction framework.
Results and discussion
The results of the scoping review were organized into five thematic categories derived from the data extraction framework: Health inequalities and inclusion needs, (ii) disability typologies and their impact on healthcare access, (iii) emergent technologies enabling inclusive diagnostics and rehabilitation, (iv) AI and personalized care, (v) success stories and in-field case studies, illustrating IR 5.0 paradigm. A progressive synthesis- from conceptual needs and challenges to the technological and systemic innovations through the principles of IR 5.0 was structured in this section of results and discussion.
Importance of disability inclusion in healthcare
Access to healthcare is essential for achieving good health and is recognized as a fundamental human right. An inclusive healthcare system for people with disabilities is essential to ensure equitable access to medical services, improve health outcomes, and promote dignity and social justice. It is estimated by the World Health Organization (WHO) that around one billion people globally live with a disability, with approximately 80% residing in low and middle-income countries. 15 Studies have shown that people with disabilities, whether in high-income countries or low- and middle-income countries, are more likely to have poorer health outcomes compared to those without disabilities. 16 Disabilities can be physical, sensory, intellectual, or mental health related. The World Health Survey estimates that the prevalence of disability is 60% higher among women compared to men. 17 Poor access to healthcare for people with disabilities has a far-reaching impact on their health, well-being, and social participation. The key consequences of poor access to healthcare are presented in Figure 2. The United Nations International Children Emergency Fund (UNICET) reported that children with disabilities account for approximately 150 million. These children have less access to the healthcare system due to few reasons, such as personal and community beliefs, lack of awareness of disability, unavailability of health services, complicated clinical pathways, and absence of qualified health professionals.18–20
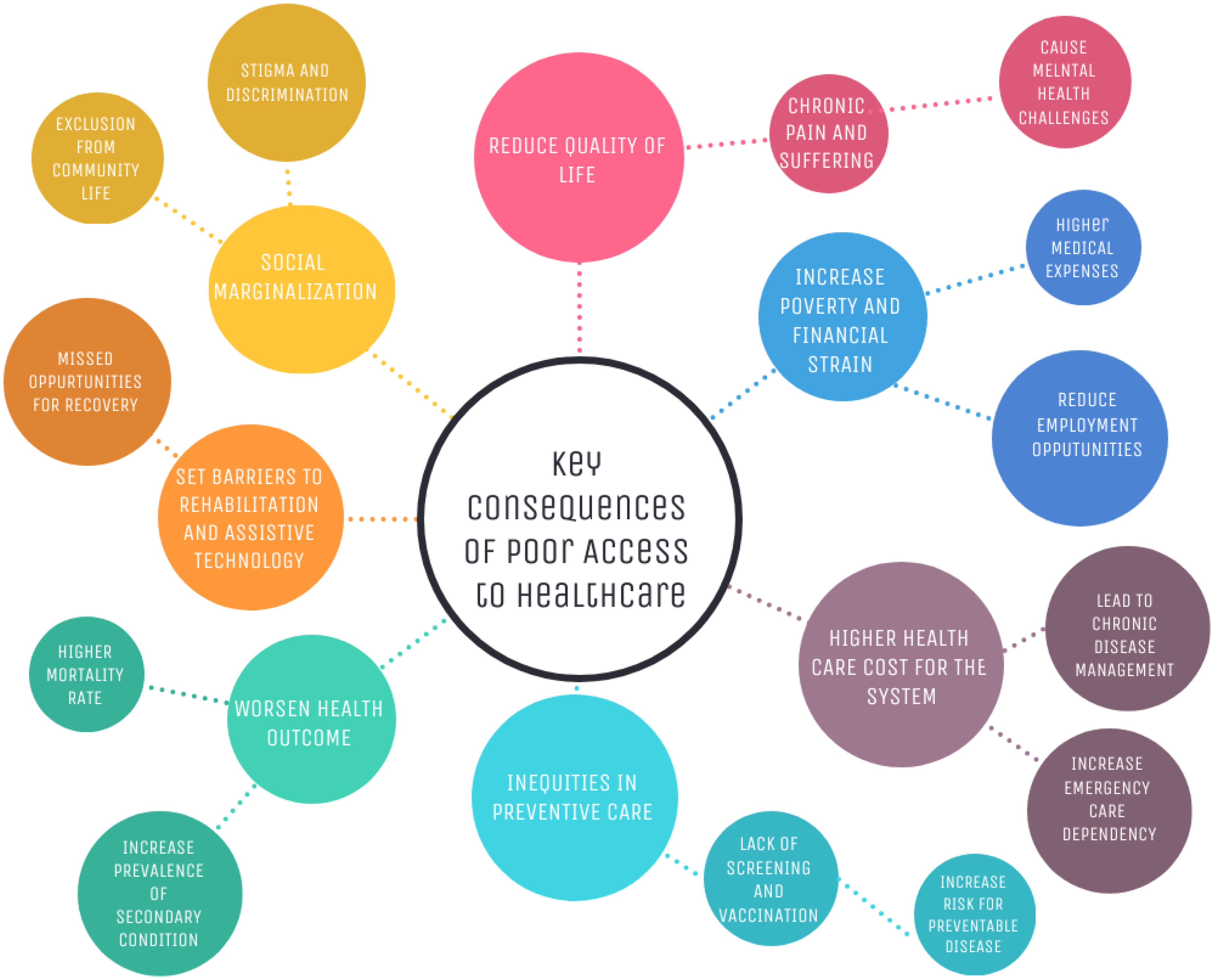
Key consequences of poor access to healthcare.
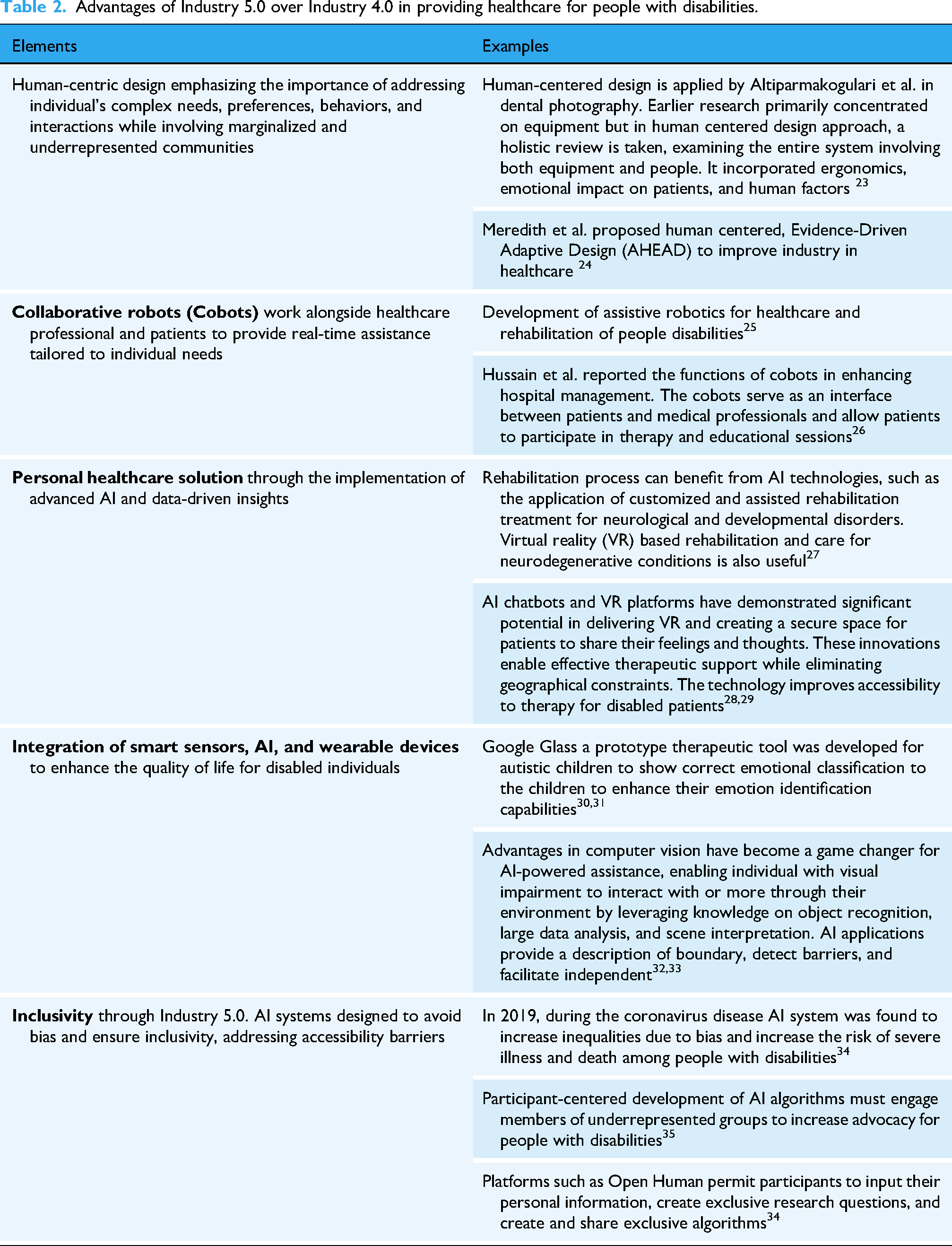
IR 4.0 technologies have significantly enhanced the inclusiveness of the healthcare system for people with disabilities by addressing barriers, improving accessibility, and enabling personal care. Advanced data analysis for personalized care can analyze health records and behavior patterns to design personalized treatment plans for individuals with disabilities. However, existing personalized healthcare is tailored to a specific environment, focusing on technological customization through devices and gadgets. They often overlook the complexity of interconnected health conditions, leading to misdiagnosis and compromising both sustainability and long-term health and quality of life for patients. 21 One of the major elements of IR 5.0 is human-centered artificial intelligence (HCAI). Facilitation of human–machine interaction is crucial, and it focuses on designing AI systems that are user-friendly, comprehensible, and accessible, bridging the gap and enhancing the way humans engage with technology. 22 While IR 4.0 relies much on autonomous robotics and efficiency, it often sidelines human aspects. Patients and healthcare workers are treated more as elements of components than as individuals with unique needs. Advantages of Industry 5.0 over Industry 4.0 in providing healthcare for people with disabilities are listed in Table 2.
Advantages of Industry 5.0 over Industry 4.0 in providing healthcare for people with disabilities.
Disabilities and impact on healthcare
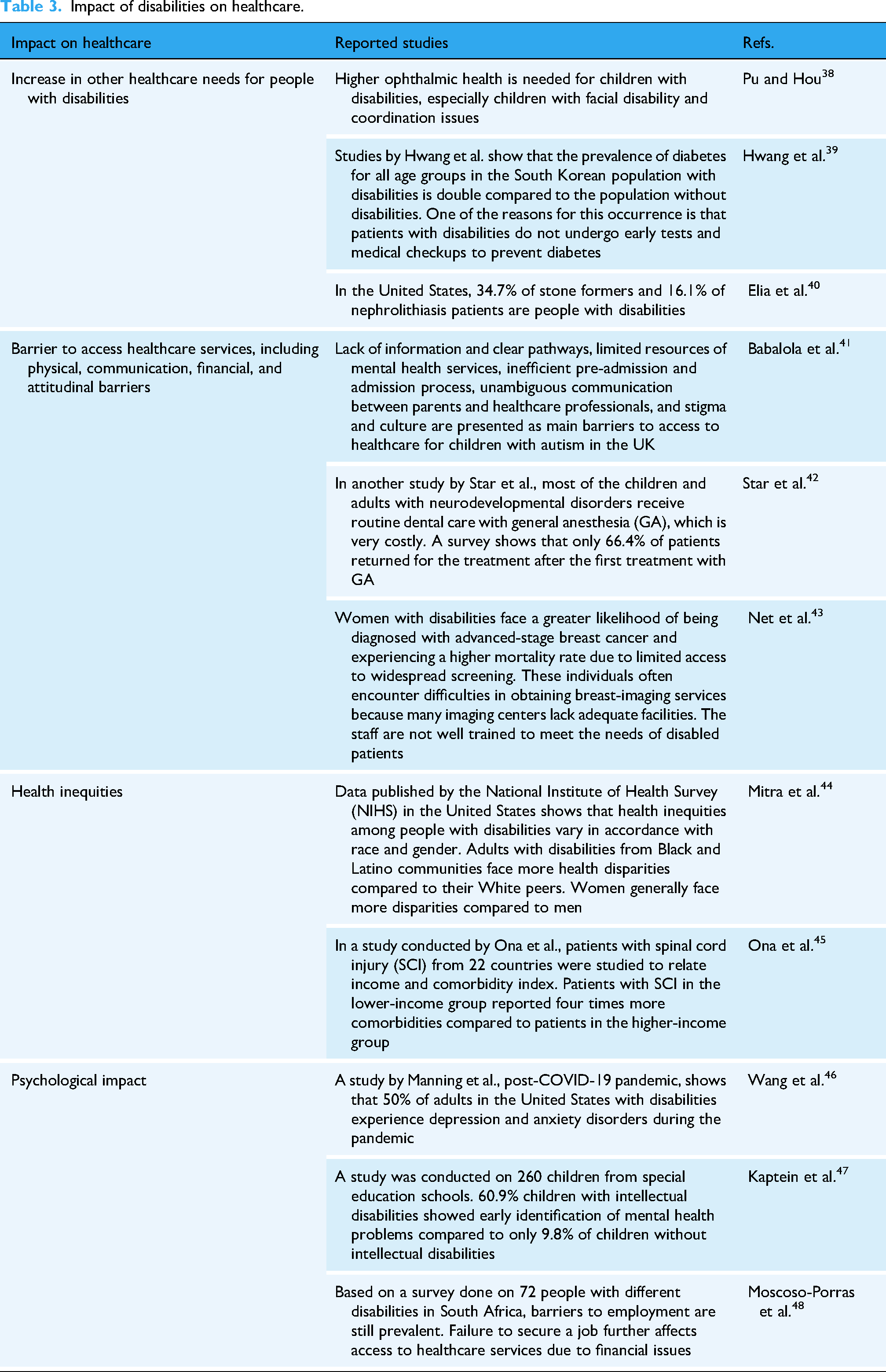
Disabilities are defined as physical, mental, intellectual, or sensory issues that constrain human ability to carry out activities of daily living, participate as a part of the community with meaningful societal roles, or grab opportunities in terms of academic and career. 36 In recent years, patients, especially children with intellectual or sensory disorders, have increased dramatically, which will cause a greater impact on the healthcare system. 37 The categories of disabilities are shown in Figure 3. The impact of disabilities on healthcare, as reported in some previous literature, is listed in Table 3. Individuals with disabilities face numerous barriers when accessing healthcare, as summarized in Figure 4. The impact of the barriers on the disabled patients is shown in Figure 5.

Type of disabilities.

Individuals with disabilities face numerous barriers when accessing healthcare.

The impact of the barriers on disabled patients.
Impact of disabilities on healthcare.
Emergent technologies and disability diagnostics
Emergent technologies in healthcare are shaping the future of medical treatments, patient care, diagnostics, and health management. These innovations are driven by advancements in fields such as AI, biotechnologyrobotics and data analytics. Although technologies such as telemedicine, augmented reality, and virtual reality originated under IR 4.0, their integration within the IR5.0 framework marks a paradigm shift from automation and care efficiency to human-centered co-creation and application. In this context, these technologies are considered not merely as tools but also collaborative enablers, permitting enhanced accessibility, personalization, and sustainability in disability inclusive healthcare.
Telemedicine and remote patient monitoring
Remote patient monitoring (RPM) utilizes digital technologies to track and monitor patients’ health conditions in real time, enabling healthcare professionals to collect vital health data from patients while they remain outside a conventional clinical environment.49,50 Telemedicine enables remote healthcare services, including diagnosis, consultation, and treatment, through the use of communication technologies. 51 Combined with tools like wearables monitoring devices, it offers a pathway to more tailored, effective, and real-time medical care. The integration of big data significantly enhances both telemedicine and RPM by facilitating the gathering, analysis, and interpretation of extensive health-related information.
For instance, web-based monitoring of patients with inflammatory bowel disease (IBD) has been shown to enhance patients’ quality of life, improve adherence to prescribed medicine, and reduce healthcare expenses. The patients could also report symptoms and notify the medical team of their condition in real time. These digital tools enable timely treatment for patients without requiring them to visit health facilities. 52 Atilgan et al. had conducted RPM from 2017 to 2020 on 2340 patients who had undergone cardiac surgery. Medical devices, namely Minotr DakiApp and Holter EG, were used to register crucial parameters such as pulse rate, blood pressure, body temperature, electrocardiography, and blood glucose. These data were kept in web-based software and mobile applications, which then enable Remote Medical Evaluation (RME). According to the statistics, the Telemedicine team had handled 79,560 RMEs between 2017 and 2020. 144 patients were hospitalized and underwent appropriate treatments due to mild and potentially life-threatening complications detected by RME. 53 Telemedicare and RPM had become very crucial for screening, diagnosis, and monitoring COVID-19 pandemic patients. 54 Continuous monitoring of COVID-19 patients with continuous pulse oximetry has resulted in a mortality rate of 6 per 1000 patients compared to 26 per 1000 patients without RPM. Pulse oximeters, traditionally used in hospitals and at home. It transmits the data to smartphones, secure cloud platforms, and web dashboards. This enables physicians and healthcare providers to monitor patients’ conditions in real time. 55 The success of RPM and telemedicine depends largely on the continuous and frequent engagement of patients with the technology. A case study on 1354 diabetes type two patients between 2015 and 2017 showed that patients who uploaded an average one upload of data per day had lower hemoglobin Alc (HbAlc) compared to patients who registered but did not frequently upload their data. 56 The success of RPM and telemedicine also depends on effective and user-friendly telemedicine tools. Application of nanotechnology enabled telemedicine sensor development for COVID-19 diagnosis, including a wearable sensor to monitor vital signs and metabolic sensors. Web-based platforms and smartphone apps were proven to be effective in the management of COVID-19 patients as reported by Lukas et al. 56 Even though, in principle, telemedicine could be very beneficial for patients in remote area but the implementation and its success depend largely on factors such as internet connectivity problems. 57 From this global analysis, it can be concluded that in the context of IR 5.0, telemedicine involves beyond digital efficiency to embody human-centered continuity of care, ensuring that intelligent monitoring systems not only automate diagnostics, but also extend accessibility, empathy, and inclusion for persons with disabilities, across geographic and socio-economic barriers.
Wearable health technology
The early stages of wearable health device development were noted between the 1960s and 1990s, with the development of basic heart rate monitors and portable ECGs. The technology bloomed around 2014 with the introduction of fitness trackers and smartwatches. 58 In 2020, 19% of Americans utilized wearable fitness trackers.59,60 At the same time, between 2005 and 2010, smart inhalers and other connected devices for asthma monitoring gained popularity in terms of usage among consumers. In 2012, Propeller Health introduced a smart inhaler device, which uses a sensor to monitor the frequency of inhaler use and record the data in mobile apps. 61 The development of wearable device technology in healthcare is shown in Figure 6.
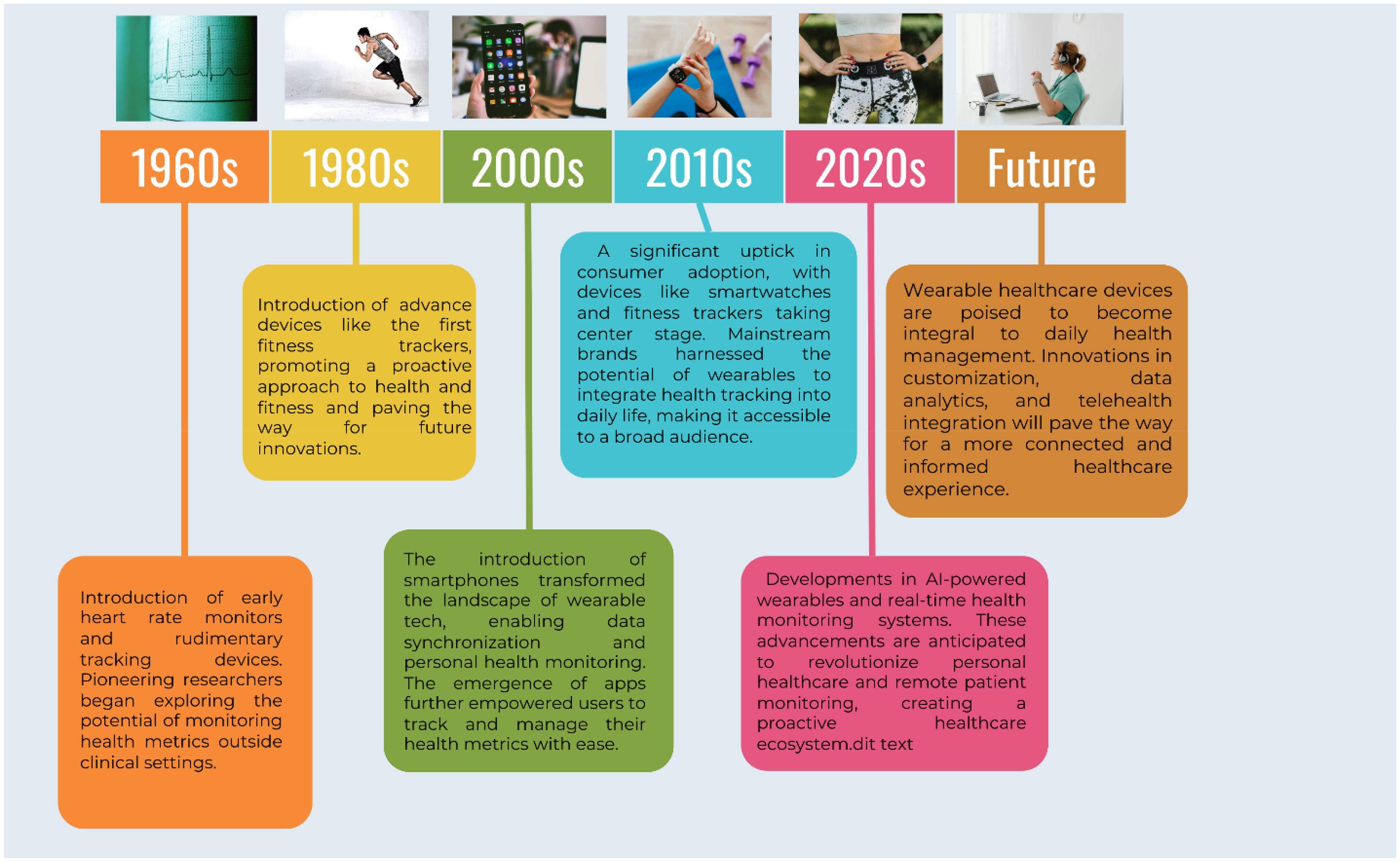
Timeline of wearable health technology development.
For the design of inclusive wearable devices, it must consider diverse disability types. In fact, for individuals with mobility impairment, lightweight and flexible materials facilitate ease of wearing and removal. Whereas haptic or auditory cues can replace visual displays for users with visual impairments, while AI-enabled adaptive feedback allows cognitive or neurological disability users to receive simplified, context-aware notifications. As a consequence, such technology transforms wearable devices from mere monitoring tools into truly inclusive healthcare companions. In terms of size and ergonomic characteristics, wearable devices are small electronic gadgets or computers equipped with wireless communication capabilities. These devices are integrated into items such as accessories, clothing, or even more invasive forms of technology as microchips or smart tattoos that can be worn on the body. Unlike conventional smartphones and tablets, wearable offers the added benefits of continuous monitoring and data saving features such as biofeedback and physiological functions released by biometrics. Despite their battery limitations, wearables are compact, portable, convenient, and provide hands-free interaction with electronic systems. 62 The market growth rate for wearables is expected to increase by 20% annually and will reach more than 150 billion euros by 2028. 63 The COVID-19 pandemic has accelerated the spread of wearable technology. 14 However, the development of wearable health device technology is quite slow compared to other hardware technologies like smartphones and tablets due to low acceptance among consumers. 64 The development of a useful and generally accepted wearable health technology requires collaborations between researchers, software developers, clinicians, statisticians, and information technologists. 65 Therefore, it can be concluded that, in IR 5.0, wearable technologies transform from passive monitoring devices into interactive companions that can adapt to users’ physical, sensory, and cognitive abilities, supporting personalization, empathy, and well-being of disabled people through continuous human–machine collaboration. Examples of wearable health technology devices are summarized in Table 4.
Examples of wearable health technology devices.

Virtual reality (VR) and augmented reality (AR)
Virtual reality (VR) and augmented reality (AR) are considered immersive technologies that have evolved from visualization and training tools of IR 4.0 into human-in-the-loop therapeutic systems characteristics of IR 5.0.72–74 With this paradigm, VR generates a fully computer-created environment where users interact through head-mounted displays and motion sensors,75–77 while AR overlays digital information on the physical world through smart glasses or mobile devices.58,78,79 In fact, within IR 5.0, these technologies transcend their original efficiency-driven purpose to foster personalization, inclusive, and cognitive-emotional engagement in the healthcare of disabled people. These technologies were initially deployed to improve surgical precision and professional training. 59 From the feedback of use and application, their integration with AI and adaptive interface design was considered a real and concrete evolution that enables co-creation between humans and intelligent systems applied for disability assistive technology.60–62 Mohapatra and Singh 63 reported that these systems dynamically adapt to patient performance, comfort, and therapeutic progress, rather than replacing clinical expertise where it was applied in the field of motor disability. Liang et al. 66 affirmed this idea when they concluded that these technologies can embody the human-centric ethos of IR 5.0 by embedding AI-driven feedback, special audio, and gesture recognition: it was highlighted some cases in which AR/VR applications were interpreted as individual motor, cognitive, and sensory capabilities, ensuring that therapy sessions involve responsiveness with the user's needs.67,68 As examples, Leap Motion-based rehabilitation games, which employ motion tracking to assist upper-limb motor recovery, were evaluated as an innovative solution, providing real-time feedback that adjusts exercise difficulty and visual cues based on patient progress.69,70 Similarly, hologram-driven balance physiotherapy systems, which integrate head-mounted holographic interfaces and AI algorithm, were used as assistive healthcare systems to guide patients through customized balance exercises.71,80 It was noticed by several experts that these immersive environments transform repetitive rehabilitation tasks into engaging, gamified experiences that enhance motivation and adherence to treatment. In other words, it was highlighted that a possible contribution to these technologies to multisensory inclusivity.81,82 The incorporation of special audio cues aids disabled users with visual impairments, while haptic feedback mechanisms assist individuals with limited motor control. As a consequence, perception and special awareness can be improved. Such designs illustrate, as a consequence, the shift from technology-centric optimization to human-adaptive co-design, where accessibility, empathy, and comfort drive the innovative rehabilitation process. 83 Based on this framework, VR and AR are considered a collaborative environment where patients, clinicians, and AI systems engage interactively to achieve shared rehabilitation goals, well designed for people with disabilities. Creed et al. 84 considered that VR and AR can successfully embody IR 5.0's vision of co-creation, personalization, and sustainable well-being for disabled people when they couple immersive experiences with human oversight and ethical AI design.
Collaborative robots in rehabilitation and daily care
Collaborative robots (cobots) represent a key pillar of IR 5.0, which can enable safe, adaptive, and human-centered physical interaction between humans and robots in a healthcare ecosystem.25,26,85 They are designed to work alongside patients and clinicians when they are equipped with force and proximity sensors that ensure safety and responsiveness to human movement.86,87 In the field of disability rehabilitation, it was reported several applications: the support of cobots to motor recovery and upper-limb training for patients with stroke, cerebral palsy, and spinal cord injury. 88 Practically, robotic arms can provide assist-as-needed therapy, which adjusts resistance and trajectory based on patient effort and progress. 27 When they are combined with AI-driven feedback and biomedical sensing, these robots can personalize therapy intensity and encourage patient motivation through real-time feedback and gamification. It was reported by Tung et al. 89 that cobots showed successful results in daily care when they were used to assist individuals with limited mobility in performing activities of daily living such as feeding, dressing, or transferring from bed to wheelchair. Studies highlighted that integrating cobots with computer vision and natural language interfaces allows users with physical or speech impairments to command assistive robots.90,91 This can be achieved through gestures or voice, enhancing autonomy and safety at home or clinical settings. In other contexts and situations, collaborative robots were used to alleviate caregiver burden by performing repetitive tasks like lifting, reducing musculoskeletal strain among healthcare workers. 92 Therefore, it can be concluded that cobots epitomize IR 5.0 by merging precision with compassion-supporting human caregivers rather than replacing them, which can enable safe physical interaction. And promote dignity, autonomy, and shared intelligence in disability-inclusive healthcare.
Role of artificial intelligence in disability diagnostics
AI in diagnostics and treatment
Artificial intelligence (AI) is increasingly transforming diagnostics and therapeutic interventions for individuals with disabilities by enabling earlier detection, more precise classification of complex conditions, and data-driven treatment optimization. AI systems, especially those based on machine learning and deep neural networks, excel at processing large-scale, heterogeneous datasets such as medical imaging, electronic health records, genetic profiles, and real-time biosensor inputs.93,94 For example, AI-based image analysis tools can detect subtle anomalies in MRI or CT scans for conditions such as neurodevelopmental disorders, cerebral palsy, or visual impairments that might escape human observation.95,96 AI-powered diagnostic tools like Canvas Dx significantly reduce the time to autism spectrum disorder (ASD) diagnoses from months to days, facilitating timely intervention and improving developmental outcomes.97,98 Moreover, predictive models leveraging AI can stratify risk and guide clinical decisions for coexisting conditions often prevalent among people with disabilities, such as cardiovascular disease in patients with Down syndrome. 99 AI-driven decision support tools are increasingly integrated into clinical workflows, enhancing diagnostic consistency, minimizing human error, and improving therapeutic planning.100,101 Moreover, human-centered AI frameworks emphasize transparency, interpretability, and inclusive interface design, ensuring that AI-driven diagnostics remain accessible to disabled users across sensory and cognitive disability groups. However, challenges remain, including algorithmic bias, insufficient data from underrepresented disability groups, and the necessity for explainable AI to ensure trust and clinical adoption.102,103 Nonetheless, evidence suggests that AI has the capacity to mitigate disparities in healthcare access for people with disabilities, offering transformative tools for both clinicians and patients in the diagnostic and treatment journey.104,105
Personalization of care
AI's potential to deliver personalized care solutions marks a paradigm shift toward disability-inclusive healthcare, aligning closely with the human-centric vision of Industry 5.0. Personalization, powered by AI, leverages patient-specific data—ranging from genomics to daily behavioral patterns—to tailor interventions precisely to individual needs and preferences.106,107 For individuals with disabilities who frequently experience overlapping conditions and unique functional challenges, AI enables dynamic customization of treatment plans, therapies, and assistive technologies. For instance, AI-driven rehabilitation platforms, like XRHealth, adjust exercise difficulty and feedback in real-time, boosting patient engagement and optimizing therapeutic outcomes.108,109 In the context of communication disabilities, AI-fueled augmentative and alternative communication (AAC) apps such as Avaz offer predictive text and adaptive interfaces, empowering non-verbal users to communicate effectively in their native languages and cultural contexts.71,80,110,111 AI-powered wearable devices continuously monitor physiological signals and environmental cues, allowing proactive adjustments in care, crucial for individuals with chronic disabilities prone to sudden health events.81,112 Human-centered AI (HCAI) frameworks further emphasize transparency and usability, ensuring technologies remain accessible, ethical, and trustworthy.82,113 However, achieving effective personalization demands inclusive co-design with people with disabilities, to avoid one-size-fits-all solutions and ensure cultural and contextual relevance.114,115 As AI technologies continue evolving, their integration into personalized care holds the promise of enhancing autonomy, quality of life, and health equity for diverse disability communities, fundamentally reshaping disability-inclusive healthcare landscapes.116,117
Case studies and success stories
The following section highlights real-world applications of Industry 5.0 principles, focusing on human-centeredness, personalization, and intelligent technology, to develop inclusive healthcare systems for people with disabilities. These cases demonstrate how emergent and AI technologies significantly enhance healthcare accessibility and quality for diverse groups with disabilities.
XRHealth: Virtual reality for remote disability rehabilitation
XRHealth, a US-based company, exemplifies the integration of VR and AI into remote rehabilitation services, particularly for individuals with cognitive, neurological, and physical disabilities. Originating in 2016 and approved by the US FDA, the platform provides immersive, interactive therapy experiences that are monitored in real-time by clinicians. 118 The technology combines VR headsets with motion tracking and biometric sensors to create customized therapeutic environments. 119 Patients undergo gamified exercises designed to enhance motor and cognitive functions. At the same time, clinicians track performance through AI-driven dashboards that adapt treatment plans based on real-time feedback, as shown in Figure 7.
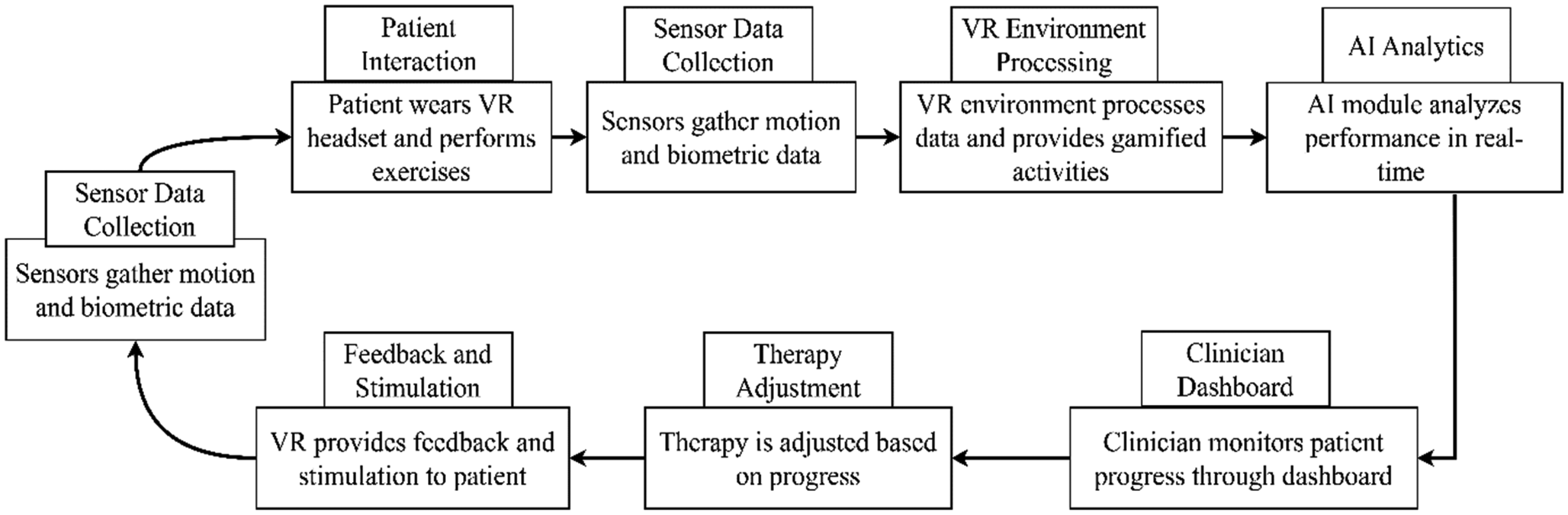
Workflow of XRHealth’s VR-based closed-loop rehabilitation system integrating AI and clinician feedback.
The implementation of XRHealth gained momentum during the COVID-19 pandemic, offering a safe and accessible alternative to in-clinic rehabilitation. It has proven especially valuable for patients with limited mobility or those living in remote areas. The platform demonstrated positive outcomes, including increased therapy engagement, better functional recovery, and reduced care costs. Lessons learned from XRHealth emphasize the importance of human–AI collaboration, simplicity in user interface design, and data privacy safeguards. Potential pitfalls include the need for continuous user training, sufficient internet infrastructure, and ensuring emotional engagement without a physical therapist's presence. Nevertheless, XRHealth stands as a scalable model for future disability-inclusive, remote healthcare delivery systems, aligning with Industry 5.0 values. These insights are further illustrated in Table 5, which compares traditional rehabilitation outcomes with those achieved using the XRHealth platform.
Comparison of traditional vs. XRHealth rehabilitation outcomes.

Seha Virtual Hospital (Saudi Arabia): AI-enhanced telehealth for inclusive healthcare
Seha Virtual Hospital, launched in 2022 by Saudi Arabia's Ministry of Health, is recognized as the world's most extensive integrated telehealth system and a transformative model for disability-inclusive healthcare in the Middle East. The platform was developed to connect over 200 hospitals across the Kingdom, offering specialized healthcare services to patients, including those with disabilities, regardless of their geographic location. 120 The technology infrastructure underpinning Seha Virtual Hospital includes AI-powered diagnostics, digital twins for clinical simulations, remote patient monitoring systems, and real-time AR consultations. These technologies allow patients with physical, cognitive, or chronic conditions to receive personalized healthcare while remaining in their homes or local clinics. The AI components aid in triage, risk prediction, and decision support for clinicians, thereby enhancing diagnostic accuracy and reducing service bottlenecks. 121 The implementation of Seha has been particularly impactful in expanding access for people in rural and underserved areas, many of whom face mobility limitations or transportation barriers. Figure 8 illustrates how Seha's telehealth services map to various disability types and contribute to inclusive healthcare outcomes. The platform facilitates virtual consultations, follow-up care, chronic disease management, and remote therapy, improving care continuity and reducing travel-related burdens for patients with disabilities. It also contributed to the resilience of the healthcare system during the COVID-19 pandemic by supporting remote triage and treatment. Key lessons from Seha underscore the importance of a strong governmental commitment, the integration of multi-speciality services, and user-centric design in telemedicine platforms. Challenges include ensuring digital literacy among patients, maintaining cybersecurity, and coordinating cross-institutional data sharing. Despite these challenges, Seha represents a scalable and sustainable model for leveraging emergent and AI technologies to build a more equitable and accessible healthcare system aligned with Industry 5.0 goals.
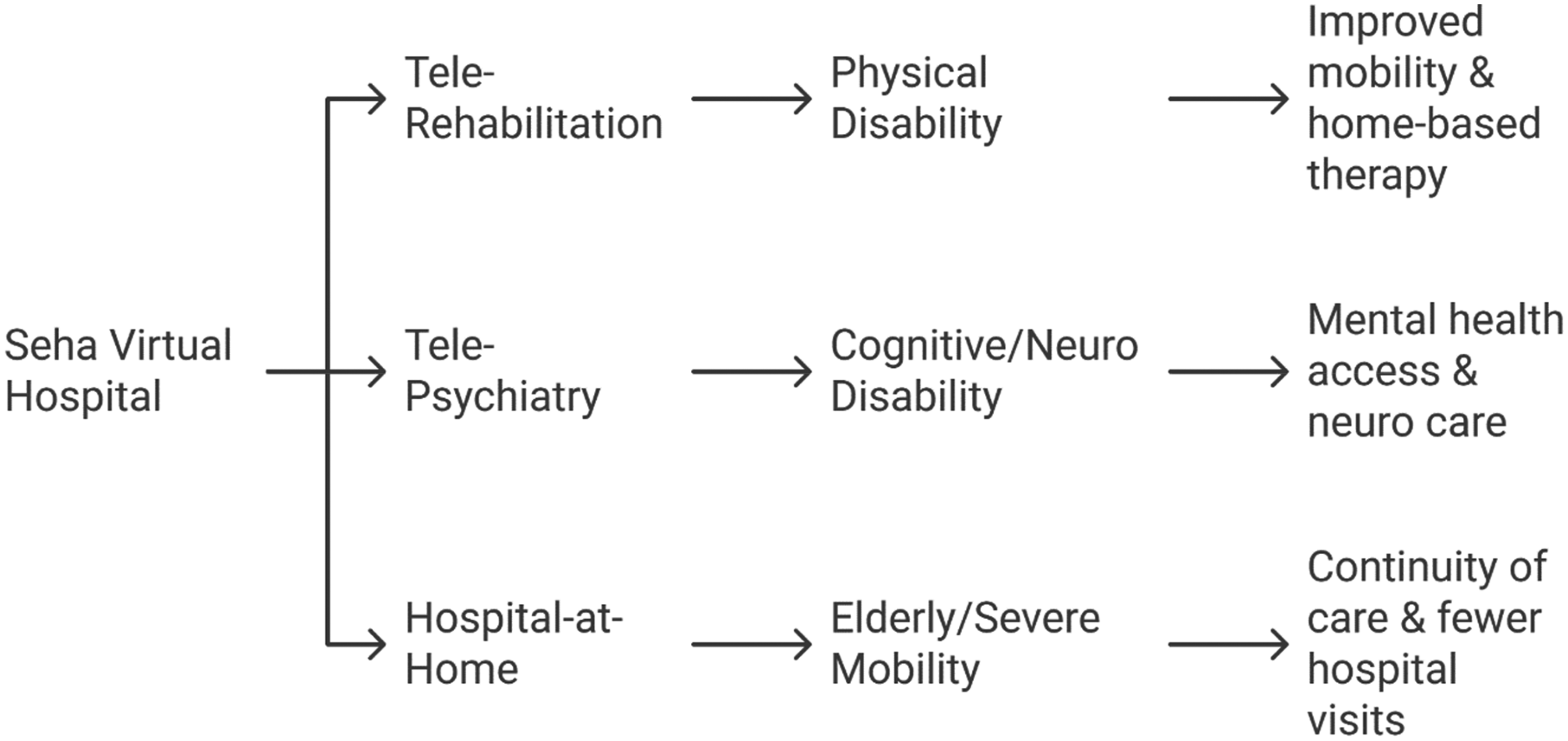
Mapping Seha Virtual Hospital's telehealth services to specific disability types and inclusive outcomes.
Be My Eyes: AI-powered visual assistance for the visually impaired
Be My Eyes is a globally recognized mobile application that supports individuals with visual impairments by combining crowdsourced volunteer assistance and AI. Founded in Denmark in 2015, it began as a peer-to-peer service connecting blind or low-vision users with sighted volunteers via live video calls to assist with real-time visual tasks such as reading labels, navigating unfamiliar environments, or checking expiration dates. 122 In 2023, the platform expanded its capabilities by integrating OpenAI's GPT-4 Vision model through the “Be My AI” feature. This enables users to take photos and receive detailed, AI-generated descriptions, read text, interpret documents, and ask follow-up questions—all without requiring human intervention. Figure 9 illustrates a timeline of key milestones in the app's development. This advancement marks one of the earliest real-world applications of multimodal AI for accessibility. 123 Be My Eyes has achieved a truly global impact, serving over half a million visually impaired users and supported by more than six million volunteers across 150 countries. Its hybrid model—blending AI with human assistance—ensures that users can access both fast automated support and personalized help when needed. Strategic partnerships with companies like Microsoft and Google have also enabled access to trained accessibility support directly within the app. The platform has significantly improved independence and confidence among users, reducing reliance on caregivers and enhancing day-to-day autonomy. The integration of AI has enabled more private and immediate assistance in sensitive contexts. By centering on empathy, inclusivity, and technological empowerment, Be My Eyes exemplifies the human-centric ethos of Industry 5.0 and demonstrates how AI can complement, rather than replace, human connection in delivering inclusive healthcare solutions.

Timeline of key milestones and innovations in the development of Be My Eyes and its AI-powered expansion.
Avaz: Assistive communication for non-verbal disabilities
Avaz is a pioneering augmentative and alternative communication (AAC) app developed in India to support individuals with speech and communication impairments, particularly children with autism, cerebral palsy, Down syndrome, and other non-verbal disabilities. Launched in 2009 by Invention Labs, it stands out as one of the first major assistive tech innovations from the Global South, embodying Industry 5.0's human-centric and inclusive ideals. 124 The app enables users to communicate through picture symbols, text-to-speech synthesis, and customizable vocabulary boards. Designed with motor and cognitive challenges in mind, Avaz also incorporates AI-powered word prediction and is available in multiple regional languages, enhancing accessibility across linguistically diverse and underserved communities. 125 Avaz blends intelligent technology with practical, localized design. Features like dynamic vocabulary suggestions, offline support, and caregiver dashboards make it suitable for low-resource settings. The platform also includes training tools for parents and educators, promoting inclusive communication and learning. Lessons learned from Avaz's journey highlight the importance of cultural and linguistic adaptation in global assistive technology. While many AAC apps originated in the West, Avaz's localized development approach made it more relatable and practical in the Indian and Global South context. Another key insight is the value of ongoing feedback from end users, families, therapists, and educators, which helped refine the app into a scalable, user-friendly solution. Avaz demonstrates how intelligent assistive communication platforms can empower non-verbal individuals by restoring their voice, literally and metaphorically. By integrating AI into inclusive and culturally sensitive design, Avaz makes a meaningful contribution to the development of equitable, disability-friendly healthcare and educational systems that align with Industry 5.0 principles. The usage of the Avaz AAC App is summarized in Table 6.
Use cases of the Avaz AAC app across different disability types.

Cognoa's Canvas DX: AI-powered autism diagnosis for inclusive early healthcare
Canvas Dx, developed by the US-based health tech company Cognoa, is the first FDA-authorized AI diagnostic tool for early autism detection in children aged 18–72 months, Fig. 10. It integrates machine learning with inputs from caregiver questionnaires, home-recorded videos, and clinician assessments to generate accurate ASD diagnoses through a secure platform. 126 By processing this multimodal data with clinically validated algorithms, Canvas Dx significantly reduces diagnosis time from months to days, facilitating earlier access to therapy. Designed for use in primary care settings by non-specialists, the tool helps bridge diagnostic gaps in underserved communities. 127 Several lessons have emerged from the Canvas Dx journey. First, it underlines the feasibility of deploying AI-based diagnostic tools in early childhood, a particularly delicate and high-impact developmental window. Second, it demonstrates the value of human–AI collaboration, where the AI supports but does not replace the clinical judgment of trained professionals. Third, it emphasizes the need for robust and diverse training datasets to ensure the tool performs reliably across different demographic groups, thereby avoiding algorithmic bias. Lastly, it highlights that regulatory approval, particularly by agencies like the FDA, is key to building public and institutional trust in AI healthcare solutions. Canvas Dx aligns seamlessly with Industry 5.0's vision by promoting personalized, accessible, and ethically aligned healthcare systems. Through intelligent diagnostics that empower caregivers, streamline clinical workflows, and reach underserved populations, it serves as a blueprint for integrating AI into inclusive pediatric and neurodevelopmental care.
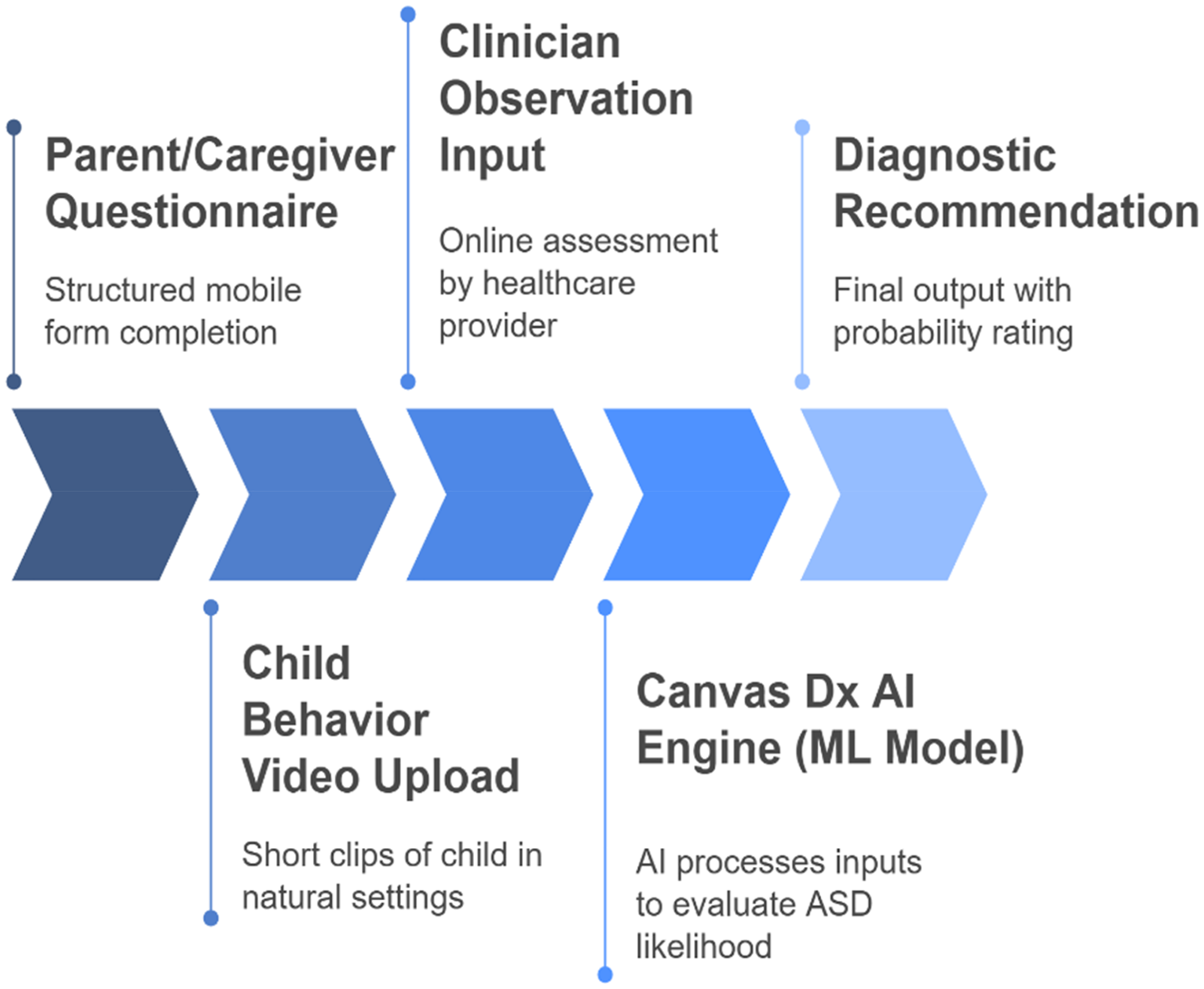
Diagnostic process flow of Canvas Dx for early autism detection using AI, clinician input, and behavioral data.
Cross-case summary and lessons learned
To draw broader insights from the preceding case studies, Table 7 summarizes the key elements of each initiative, including the type of technology, implementation scale, focus on disability, and notable outcomes. These case studies collectively underscore the multifaceted role of emergent and AI-driven technologies in shaping inclusive healthcare. From real-time diagnostics and assistive communication to immersive therapy and hybrid visual support, the projects demonstrate the core principles of Industry 5.0—personalization, ethical AI integration, and human–machine collaboration. A recurring theme across successful implementations is the centrality of accessibility, whether achieved through cultural localization (Avaz), regulatory validation (Canvas Dx), or platform scalability (Be My Eyes). However, these initiatives also highlight challenges such as digital literacy, infrastructural readiness, and the ongoing need for human oversight in sensitive health interactions. Across the reviewed studies, it was concluded that technologies originally conceived within the automation logic of IR 4.0 are being reimagined through the human-centric, co-adaptive, and ethical principles of IR 5.0. Techniques such as telemedicine and wearables extend inclusion by enhancing remote accessibility and personalization, while VR and AR, as well as collaborative robots, embody the human-in-the-loop paradigm by placing empathy, comfort, and user agency at the center of technological interaction. As a consequence, these developments signal a transition from efficiency-driven digitalization to value-driven human empowerment.
Summary of AI-driven applications for disability-inclusive healthcare.

While these reviewed technologies illustrate significant progress toward disability-inclusive healthcare, their tangible results demand more than technical advancement alone. In fact, effective implementation within the IR 5.0 framework requires comprehensive training and capacity-building programs for both disabled people and healthcare man-power. Equally, robust regulatory and ethical frameworks are critical factors that must evolve to govern data protection, algorithmic accountability, and patient consent in AI-driven systems. In parallel, ensuring data privacy and cybersecurity is paramount, as the sensitive nature of disability-related health data demands strict compliance with global data-protection standards. Moreover, the type of interaction between a large panel of disability types, different technical resources, and various domains of experts and trainers challenges the interdisciplinary collaborative participation, which is crucial to transform laboratory innovation into practical, inclusive, and sustainable solutions. Besides, the improvement of these emergent technologies for more successful real-world application without taking into account the feedback from people with disabilities at every design stage is considered a great challenge both for developers and users with disabilities. Thinking about all these elements needs the proposition of a roadmap with systemic transformation toward inclusive, resilient, and ethically aligned healthcare ecosystems.
Future directions
The future of disability-inclusive healthcare is being shaped by a new wave of technological innovations rooted in the human-centric values of Industry 5.0. A key trend is the rise of multimodal AI assistants that combine vision, speech, and contextual awareness to support users with complex disabilities, interpreting not just text and voice but also gestures and environmental cues. Another significant advancement is brain-computer interfaces (BCIs), which enable individuals with severe physical or speech impairments to control devices using neural signals, offering new possibilities for communication and mobility. Hyper-personalised rehabilitation is also emerging, using biometric sensors, emotional AI, and real-time analytics to adapt therapy protocols dynamically to each user's cognitive and emotional state. Additionally, augmented reality (AR) is being explored as a cognitive aid, helping users’ complete daily tasks independently through smart glasses or mobile devices. Collectively, these innovations mark a shift toward intelligent, personalized, and empowering healthcare systems for a more inclusive future.
Despite significant progress in AI and emergent technologies for disability-inclusive healthcare, several critical challenges persist. Accessibility and digital equity remain major concerns, especially in rural or low-resource settings lacking adequate infrastructure and connectivity. The high cost of advanced tools, such as brain–computer interfaces and VR systems, also limits their widespread adoption. Data privacy and the ethical use of AI pose further barriers, particularly when handling sensitive health information. A lack of inclusive design, often excluding direct input from people with disabilities, results in solutions that are technologically advanced but practically inaccessible. Lastly, limited training for both users and healthcare providers hinders effective implementation, underscoring the need for ongoing education and capacity building.
Finally, to operationalize the transition from conceptual innovation to practical application, a structured roadmap is proposed, encompassing six key pillars, Figure 11: (i) training and capacity building, (ii) regulatory and ethical governance, (iii) interdisciplinary collaboration, (iv) socio-economic enablement, (v) real-world validation, and (vi) inclusive co-design. These interconnected domains collectively define the enabling environment for the sustainable deployment of IR 5.0 technologies in disability-inclusive healthcare. Their integration ensures that technological advances are matched with human readiness, ethical assurance, and social equity, paving the way toward resilient, human-centered digital health ecosystems. Table 8 illustrates the structural overview of this proposed roadmap framework for implementation.
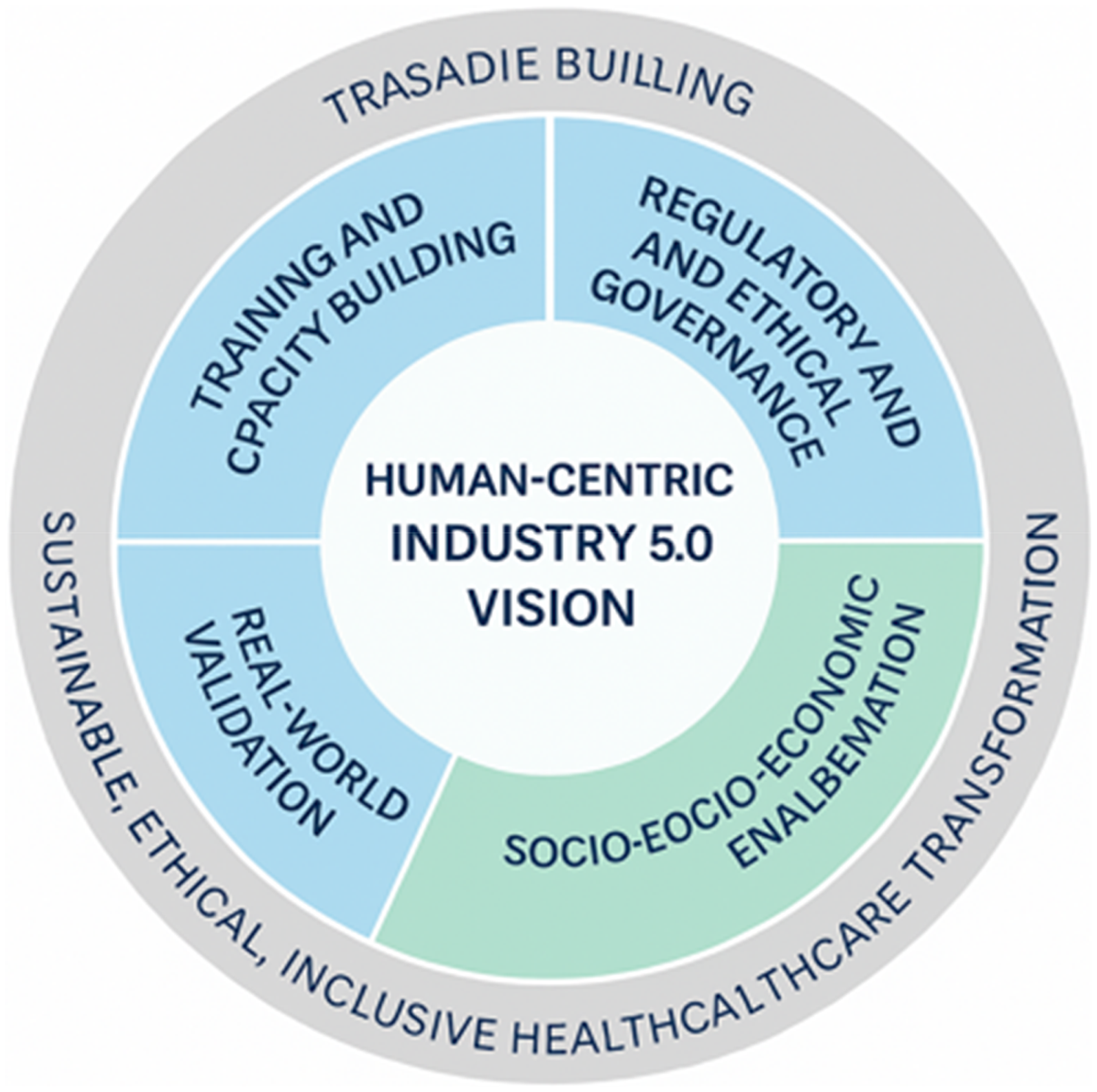
Pillars of IR 5.0 roadmap for disability-inclusive healthcare.
Structural overview of the proposed roadmap framework.

Conclusion
This review has critically examined the intersection between emergent technologies, artificial intelligence, and disability-inclusive healthcare within the evolving framework of Industry 5.0. By emphasizing human-centricity, personalization, and the ethical integration of technology, the study underscores how Industry 5.0 offers a paradigm shift from automation-centered care to collaborative and empathetic systems. Through the analysis of current literature, global strategies, and pioneering case studies, it is evident that these technologies can transform healthcare experiences for people with disabilities by improving access, autonomy, and tailored interventions.
Moreover, the study identified promising trends such as brain–computer interfaces, multimodal AI assistants, and context-aware smart systems that will further enhance inclusivity and responsiveness in future healthcare models. However, several challenges remain, including digital infrastructure gaps, ethical concerns, affordability, and the need for inclusive co-design. To truly realize the potential of these technologies, stakeholders must prioritize accessibility, cross-sector collaboration, and user-centered innovation. Ultimately, this review contributes a forward-looking foundation for researchers, policymakers, and healthcare innovators aiming to design equitable, resilient, and inclusive healthcare systems that empower people with disabilities in the era of Industry 5.0.
To fully realize the potential of emergent and AI technologies in disability-inclusive healthcare, coordinated collaboration among governments, healthcare providers, and tech companies is essential. Policymakers must support inclusive innovation through regulation and infrastructure, while healthcare institutions adopt user-centered technologies. Tech developers should engage people with disabilities in co-design to ensure accessibility and cultural relevance. Such multi-stakeholder efforts are key to building equitable, resilient healthcare systems aligned with Industry 5.0's human-centric vision.
Footnotes
Acknowledgments
The authors extend their appreciation to the King Salman Center for Disability Research for funding this work through Research Group No. KSRG-2024-465.
Contributorship
Conceptualization, M.K., A.F.A.; methodology, M.K.; software, Y.M.; validation, M.K. and K.A.A.; formal analysis, K.A.A.; investigation, M.K., A.F.A.; resources, Y.M.; data curation, K.A.A.; writing—original draft preparation, M.K. and Y.M.; writing—review and editing, K.A.A.; visualization, M.K. and K.A.A.; supervision, M.K.; project administration, M.K. and K.A.A.; funding acquisition, K.A.A. and M.K. All authors have read and agreed to the published version of the manuscript.
Institutional review board statement
Not applicable.
Institutional review board statement
Not applicable.
Informed consent statement
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the King Salman Center for Disability Research (grant number KSRG-2024-465).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.