
Abstract
Objective
This study evaluates whether orthopaedic teleconsultations provide timelier access compared to in-person visits.
Methods
We prospectively analysed scheduling data (1 July 2022–1 January 2023) for the 15 busiest orthopaedic surgeons (by total teleconsultations) at a Midwest academic healthcare system. Three metrics were assessed using EHR data: (1) third next available clinic day (adjusted for physician visit modality frequency via standardization:
Results
Appointment data from seven orthopaedic surgeons were analysed for third next available/same day metrics; lead time included data from six surgeons. In-person appointments had a shorter median availability (2 vs. 3 clinic days, p < 0.001), which means at current in-person/teleconsultation frequencies a patient was able to schedule an in-person visit 1 clinic day faster than a teleconsultation. When adjusted for a lower frequency, teleconsultations had better access efficiency (3.53 vs. 46.88, p < 0.001, lower = better access)—they were easier to schedule relative to their availability. Same day availability was higher for teleconsultations (31.15% available vs. 16.2% available, p < 0.001). New teleconsultations had shorter lead times (median 5.0 days vs. 13.0 days, p < 0.01).
Conclusion
When visits were standardized, teleconsultations provide greater access compared to in-person visits relative to their frequency. Additionally, even with the current visit volume (in-person = 92%, teleconsultation = 8%), new patients were able to see providers sooner through teleconsultations. While in-person orthopaedic visits cannot be replaced by virtual visits, particularly in cases of acute pathology, increasing the availability of teleconsultation appointments can enhance access. Appropriate digital infrastructure, training, and workflow are necessary to ensure the appropriate selection of visit modalities.
Level of evidence
II (Prospective Cohort)
Introduction
According to the Agency for Healthcare Research and Quality, access is broadly defined as the ‘timely use of personal health services to achieve the best health outcomes’. 1 Access to healthcare is recognized as a pivotal concern by the US Department of Health and Human Services.2,3 Reduced patient access has been linked to adverse health outcomes resulting from delays in diagnosis and treatment, as well as heightened reliance on emergency departments for non-urgent medical concerns, whereas increased access to subspecialty appointment scheduling has been associated with increased patient satisfaction and continuity of care.4–9 Timely access to orthopaedic care is particularly critical, as delays in surgical treatment are linked to worse functional recovery, prolonged pain, and higher rates of complications.10–12 Moreover, in an increasingly competitive healthcare industry, convenience and access to specialized care are key drivers of patient loyalty and can subsequently increase hospital revenue.7,13 Healthcare systems have utilized strategies such as appointment scheduling optimizations to improve access to care, while telemedicine has been adopted worldwide to enhance healthcare delivery.14,15
The COVID-19 pandemic served as a pivotal catalyst for telehealth adoption across medical specialties, including orthopaedics. 16 During the pandemic's peak, teleconsultations surged as institutions prioritized remote care to reduce viral transmission. Although the direct operational impact of COVID-19 on the healthcare industry has diminished since the World Health Organization ended the Public Health Emergency of International Concern (PHEIC) on 5 May 2023, 17 the integration of telemedicine into the practices of various specialties continues to persist based on the benefits provided.18,19
Within the context of orthopaedics, virtual care has been reported to offer high-quality consultations for new and returning patients, 20 increase efficacy and efficiency of fracture clinics, provide cost savings for certain visit types,21,22 and provide patients with highly satisfactory care. 23 One study found patients with musculoskeletal diseases specifically preferred telemedicine visits to in-person. 24 Virtual care is also recognized for providing patients with equitable access to rehabilitation services 25 and enhancing the effectiveness of postoperative follow-up, allowing surgeons to track progress and address complications early. 26 Beyond eliminating the need for commuting to appointments and minimizing time off work for patients, 27 teleconsultations leverage structured protocols such as guided self-assessments to replicate critical aspects of in-person evaluations. For example, providers can remotely instruct patients to perform joint range-of-motion tests, localize symptoms through palpation, or demonstrate functional movements, although their success hinges largely on the physician's knowledge and comfort with said virtual procedures.28,29 However, some procedures, like joint injections, or certain imaging studies (X-ray, MRI), require in-person administration. Extensive work has been performed looking at the utility of telehealth in diagnoses of specific musculoskeletal disorders. One study found that, during the pandemic, most telehealth diagnoses of musculoskeletal complaints fell under chronic complaints, such as back pain, rather than acute injuries. 30 A second found that, while a virtual fracture clinic provided significant cost savings compared to an in-person clinic, certain diagnoses – for example distal radius fractures – were unable to be discharged virtually. 21 Within the realm of total joint replacement, across multiple studies teleconsultations have shown high patient satisfaction, comparable outcomes to in-person visits, and resource savings for institutions, however, have limitations, particularly in regard to post-surgical complications, as well as preoperative assessments for which in-person visits cannot be replaced by a virtual modality.31–35 On the whole, optimal digital workflows are essential to successful telehealth adoption, as an additional study found that a lack of streamlined workflows can lead to increased, rather than decreased wait times for patients the day of their appointment. 36 As shown, orthopaedic teleconsultations are not without challenges; lack of awareness, implementation and maintenance costs, billing challenges, difficulty with physical examinations, and regulatory barriers have additionally been cited as obstacles associated with teleconsultation implementation. 37 Regardless, a key benefit of virtual care is the potential for greater patient access to appointments. 38 While literature exists analysing patient satisfaction, quality of care, and appointment access from the patient financial perspective, citing reduced travel and cost of appointments,39,40 there is no current investigation of the ease and promptness of scheduling a teleconsultation compared to their in-person counterparts. Virtual care is proposed to offer patients a shorter time for appointment scheduling, thereby offering more convenient and higher quality care, but this has not yet been analysed for orthopaedic visits.41–43
The purpose of this study was to assess the availability and ease with which patients can access orthopaedic teleconsultations versus in-person appointments. To do so, we employed three established methods to measure in-person and teleconsultation access: the timeliness of scheduling prospective appointments, the availability of same day appointments, and the retrospective lead time for new appointments.44–46 We hypothesize that teleconsultations will exhibit significantly greater patient access across all three methods in comparison to in-person visits.
Methods
Selection of physicians
For this study, the 15 physicians who had the greatest teleconsultation volume in 2022 from a Midwest tertiary-level academic healthcare system were considered from a pool of 85 total orthopaedic providers. ‘Top virtual providers’ were defined as those with the greatest absolute number of teleconsultations (not ratios), ensuring sufficient data for comparison. All 15 were orthopaedic providers: 14 surgeons (specializing in joints, hand, foot & ankle, trauma, sports, and general orthopaedics) and 1 non-operative orthopaedic physician. We focused on high-volume providers to standardize comparisons and minimize variability from low virtual utilization, as our data collection resources limited broader inclusion. Of note, all physicians outside the top 15 conducted less than 1% of their total visits virtually. In this study, ‘telemedicine’ or ‘virtual care’ refers broadly to the use of digital technologies to deliver remote healthcare. However, we specifically focus on ‘teleconsultations’; a subset of telemedicine defined as synchronous, real-time video consultations between patients and providers. Asynchronous methods (e.g. remote monitoring, e-consultations) were not included in this analysis.
Visit types and appointment scheduling
At our institution, teleconsultation types include new, return, and postoperative. For both in-person and teleconsultations, a new visit is defined as the initial consultation during which a patient establishes care with an orthopaedic physician, indicating that no prior patient–provider relationship exists with that specific physician. Return visits include patients who are established with a physician returning with a new concern and must be at least 90 days outside surgery. Postoperative visits include regularly scheduled appointments within 90 days of surgery. All visit types were scheduled following the Centers for Medicare & Medicaid Services Evaluation and Management Services Guide. 47 Both in-person and teleconsultations were scheduled for 15 min. Orthopaedic surgeons were permitted to employ guided self-assessments during teleconsultations at their discretion, consistent with institutional telehealth policies. While certain in-person activities cannot be replicated virtually, such as injections, the scheduling process for teleconsultations and in-person visits was similar. All patients scheduled appointments by contacting orthopaedic schedulers via phone or speaking with them in-person. For established patients requesting a specific physician, schedulers asked whether they preferred a teleconsultation or in-person visit. For new patients, schedulers triaged them to an appropriate physician based on their complaint and similarly offered both modalities. Patients were not restricted from choosing either option. Imaging studies (e.g. X-rays) were ordered identically for teleconsultation and in-person visits by the orthopaedic surgeon's ancillary staff. For example, a patient with chronic knee pain received an imaging order regardless of modality, with virtual patients completing imaging at their convenience and in-person patients during their visit. Schedulers did not review referral details or clinical notes when offering visit types. Physicians could convert teleconsultations to in-person follow-ups if procedures (e.g. injections) or exams were required, but this occurred post-consultation. All visits included in this study occurred in the outpatient clinic setting. Advanced Practice Providers (APPs)—encompassing nurse practitioners, physician assistants, and clinical nurse specialists—were excluded only if they conducted visits independently (i.e. without physician involvement). APPs may have participated in care (e.g. assisting with in-person exams), but APP-led visits were excluded because they represent a distinct pathway for accessing care, often with different scheduling protocols and patient populations. Our study focused on comparing access to physician-led appointments, which constitute the majority of subspecialty orthopaedic care in our system. Internationally, similar roles exist under titles like Advanced Clinical Practitioners (UK) or Advanced Practice Nurses (EU).
Access measures
Numerous methods have been utilized for the purpose of measuring appointment access; however, due to the inherent strengths and limitations of each method, there is currently no widely accepted quantitative measure.41–44 For this study, third next available,44,48,49 same day availability, 46 and lead time14,45 were utilized to measure appointment access. Third next available is a prospective measure that determines the number of clinic days until the third next available appointment.44,48,49 The third next available is used rather than the first next available to help control for confounding variables such as last-minute cancellations or short-term openings, which can artificially inflate access estimates for the first next available slot. Additionally, the third appointment has been found to best represent actual wait times involved with patient appointment booking. 50 However, this method reflects clinic scheduling patterns rather than patient preferences, potentially overestimating delays for patients willing to accept last-minute openings. Same day availability prospectively examines the ease with which patients can promptly schedule an appointment on the same day they make the request by measuring the ratio of available to filled appointments immediately prior to the clinic day. 46 This was included to assess immediate access for urgent or time-sensitive concerns and provides a view of the relative availability of appointments based on how many total in-person and teleconsultations are offered. Same day access for teleconsultation and in-person appointments was compared as the ratio of available to filled return appointments. A greater ratio of available to filled appointments indicates greater access. Lead time is a retrospective view of access and is defined as the number of days between the date the patient called to set up the appointment to the date when the appointment was provided.14,45 Lead time captures the patient-facing delay, reflecting real-world wait times. However, this method is influenced by patient willingness to wait (e.g. elective vs. urgent cases), which our retrospective design could not assess.
Data collection
To collect third next available data, a prospective chart review was performed for the included physicians every Monday at 12:00 pm between 1 July 2022 and 1 January 2023. For same day, appointment data on the included providers was collected from the system's electronic medical record (EMR) the night before each clinic day between 1 July 2022 and 1 January 2023. However, because data were collected at a fixed time each day, real-time cancellations or last-minute openings closer to the appointment time may have been missed. For lead time, all in-person and teleconsultations designated as ‘new’ were pulled from the hospital's EMR system between 1 January 2022 and 1 January 2024. This collection period was utilized due to the overall low number of new teleconsultations. ‘New’ patient visit type was selected rather than ‘return’ or other appointment types to minimize confounding variables associated with lead time, such as provider suggested follow-up periods for return or postoperative patients. All appointment information was housed in the hospital's EMR system. Data collectors underwent training to familiarize them with the EMR interface, definitions of ‘available’ slots (unfilled appointments visible to schedulers), and criteria for distinguishing teleconsultation vs. in-person slots. All physician appointment data was collected from the same EMR system.
Standardization Calculation
Raw third next available days inherently favour modalities with higher visit frequency. For instance, in-person visits (92% of appointments) naturally have more frequent slots, reducing raw wait times. Standardization neutralizes this volume advantage, isolating how efficiently each modality utilizes its allocated appointments. To account for the difference in visit modality frequency, the following standardization calculation was employed for each physician:
Exclusion criteria
From an initial cohort of 15 orthopaedic providers (selected as the highest volume teleconsultation users in 2022), a stepwise exclusion process was applied to ensure methodological rigour. For the third next available and same day availability metrics, inclusion required providers to have dedicated appointment slots exclusively for teleconsultation or in-person visits (no overlapping/hybrid slots). Of the 15 providers, eight were excluded due to interchangeable slots, leaving seven for these prospective analyses. This was necessary because ambiguous slot types prevented calculation of modality specific access. For instance, third next available teleconsultations could only be determined if slots were explicitly reserved for teleconsultations. Eight of the original 15 providers were excluded due to hybrid slots reservable for either modality. For lead time, inclusion required providers to have a new teleconsultation during the study period. Among the original 15, six providers met this threshold. In total, nine unique providers contributed to at least one metric: seven to third next available/same day, six to lead time, with four providers overlapping across all methods.
Statistical analysis
For same day access, differences in the proportion of available to filled appointments for in-person and teleconsultation were analysed using χ2 analysis. For the third next available and lead time data, the Shapiro–Wilk test was employed to determine the normality of data distribution. Because the data was not normally distributed, the Wilcoxon signed-rank test was utilized for third next available (paired cohorts) and the Mann–Whitney U test was used for lead time (unpaired cohorts). Median values are displayed in the figures along with 25% and 75% interquartile ranges as error bars. Significance was set at p-value < 0.05. All statistics were performed on SPSS 29. This study was approved by the institutional review board at our institution (IRB#16153). No funding was received for this study.
Results
Using each method's specific selection criteria, nine total physicians were included in this study. Visits from seven providers were analysed for the same day and third next available methods (physicians 1, 2, 3, 4, 6, 7, and 9), while appointment data from six providers were used for lead time days (physicians 1, 2, 3, 4, 5, and 8). Of the physicians selected for this study, 3 specialize in joints, 1 in hand, 1 in foot & ankle, 1 in trauma, 1 in sports, 1 is non-operative, and 1 is a generalist. The percentage of visit types that were virtual for these providers ranged from 1.1% to 15.1% (Table 1). These percentages were not predetermined limits; rather, they emerged organically from their practice patterns. During the collection period (1 July 2022–1 January 2023), 9241 total in-person and 825 teleconsultations were observed.
The specialty of each physician and the composition of their visits during the collection period.

For the third next available method, 179 scheduling events (clinic days until next available appointment) were collected for both in-person and teleconsultations (358 total) across the seven physicians. Demographic data for patients seen by physicians during the third next available collection period is displayed (Table 2 and Figure 1). Demographic disparities between in-person and teleconsultation patients were statistically significant. Teleconsultations had a higher proportion of white patients (72.4% vs. 59.5%) and lower representation of Black patients (22.1% vs. 28.8%, p < 0.01). Patients seen in-person were also a median age of 2 years older (in-person: 66 years, teleconsultation: 64 years, p < 0.01). When analysing third next available appointment access, the median in-person third next available appointment was 2 clinic days away (IQR 1, 4) compared to 3 clinic days away (IQR 2, 5) for teleconsultations (p < 0.001, Figure 2). However, upon standardizing the data by visit proportion, the in-person median standardized access efficiency score was 46.88 (IQR 35.1, 90.9) whereas the teleconsultation median access efficiency score was 3.53 (IQR 2.1, 5.3), indicating that teleconsultations operate more efficiently relative to their volume (lower value = greater access, p < 0.001). The median first next available appointment was 1 clinic day (IQR 1, 3) for in-person and 2 clinic days (IQR 1, 4) for teleconsultations (p < 0.01), aligning with the third next available trends. In a post-hoc sensitivity analysis of the third next available standardized access efficiency score, we adjusted each physician's visit distribution by increasing teleconsultation frequency by 20% and reducing in-person visit frequency by 20%. This adjustment continued to favour teleconsultations, with in-person visits yielding an access efficiency score of 5.7 (IQR 2.9, 11.4) and teleconsultations scoring 4.6 (IQR 3.1, 7.7; p < 0.001).

Demographic information for in-person and teleconsultation return patients seen by physicians included in the ‘third next available’ and ‘same day’ methods during the collection period. The top graph depicts age distribution by visit type. The bottom graph depicts race and ethnicity distribution among return patients. Error bars represent the interquartile range, and ** signifies a p-value of <0.01.

The clinic days until the third next available slots for both in-person and teleconsultations are presented. Error bars represent the interquartile range, and *** signifies a p-value of <0.001.
Demographic information for in-person and teleconsultation return patients seen by physicians included in the ‘third next available’ and ‘same day’ methods during the collection period.

For the measure of same day availability, 5372 in-person return and 825 teleconsultation return appointments were observed. Demographic data for patients seen by the physicians included in this methodology was the same as the third next available methodology (Table 2 and Figure 1). When investigating the same day availability, we found same day in-person visits were 16.2% available (n = 868 available, 4504 filled) while same day teleconsultations were 31.15% available (n = 257 available, 568 filled) (p < 0.001, Figure 3), demonstrating approximately a 3.5-fold difference.
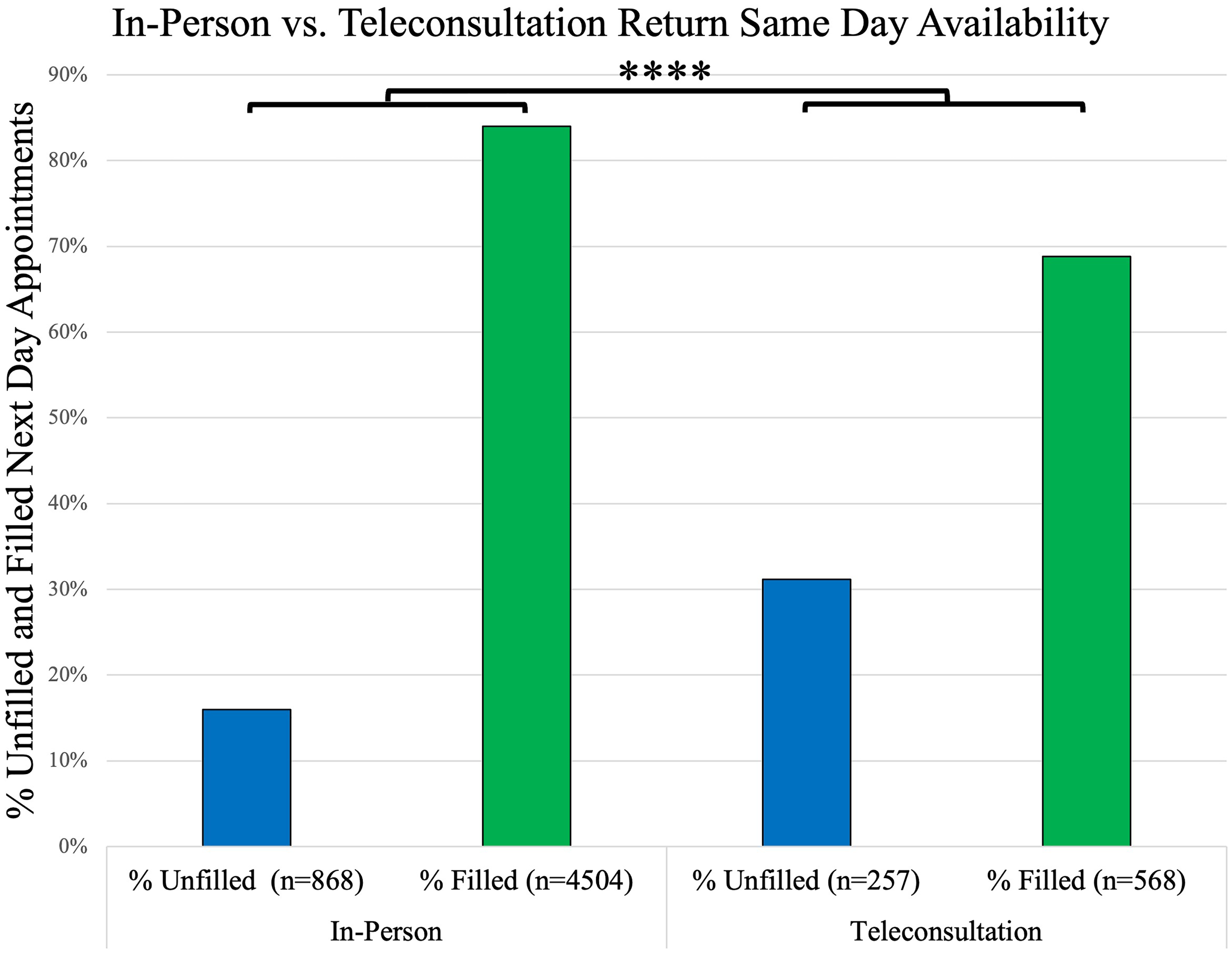
The comparison of available versus filled return appointment slots for both in-person and teleconsultations is illustrated. Each bar represents the total number of visits for its specific section. The interquartile range is represented by error bars, and **** signifies a p-value of <0.0001.
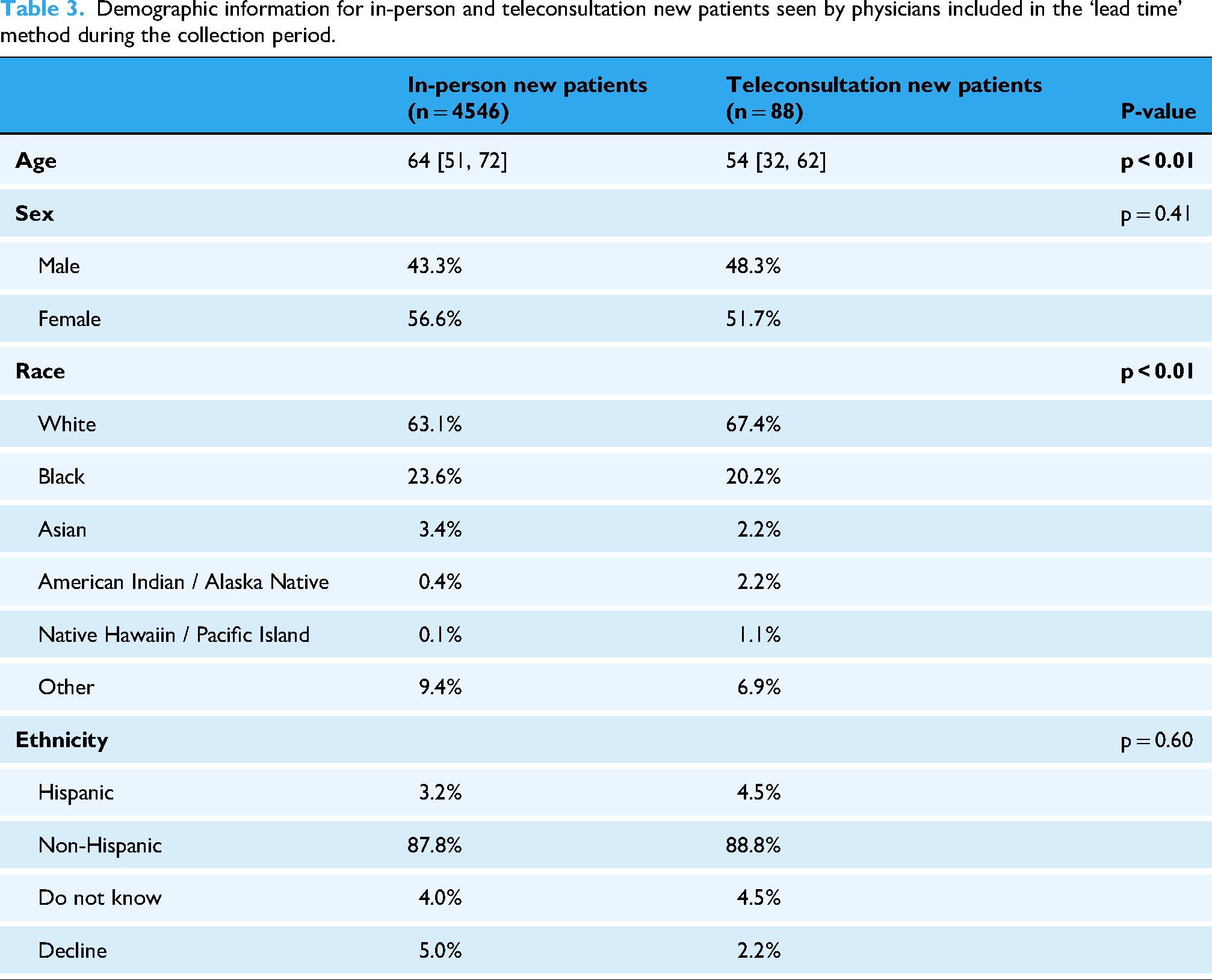
Lead time retrospective analysis yielded 4546 in-person new visits and 88 new teleconsultations. Demographic data for patients seen by the physicians included in this methodology during the collection period (1 January 2022–1 January 2024) is displayed (Table 3 and Figure 4). Demographic disparities showed a similar pattern to the third next available and same day access cohorts, with teleconsultation patients being more likely to be white (in-person: 63.1%, teleconsultation: 67.4%, p < 0.01) and younger (median age: in-person 64, virtual 54, p < 0.01). When comparing the lead time between the two groups, in-person visits had a median lead time of 13.0 days (IQR 5, 28) while teleconsultations had a median lead time of 5.0 days (IQR 2, 7) (p < 0.01, Figure 5).

Demographic information for in-person and teleconsultation return patients seen by physicians included in the ‘lead time’ method during the collection period. The top graph depicts age distribution by visit type. The bottom graph depicts race and ethnicity distribution among return patients. Error bars represent the interquartile range, and ** signifies a p-value of <0.01.

The lead days for new patients, both for in-person and teleconsultations, are depicted. Error bars represent the interquartile range, and **** signifies a p-value of <0.0001.
Demographic information for in-person and teleconsultation new patients seen by physicians included in the ‘lead time’ method during the collection period.
Discussion
This study found that, at current teleconsultation volume, there is earlier availability of prospective appointment scheduling for in-person visits (2 clinic days) compared to teleconsultations (3 clinic days). However, when accounting for the discrepancy in visit frequency (with teleconsultations comprising 8.2% of total), teleconsultations are available at a 3.5 greater rate (available / filled) on the day of request compared to in-person and display a greater level of standardized prospective access. This disparity in score (teleconsultation: 3.53, in-person 46.88) suggests that teleconsultations are less prone to overbooking or underuse, contributing to more efficient scheduling and shorter wait times. Thus, scaling virtual capacity could alleviate systemic scheduling bottlenecks for those appointment types amendable to a virtual visit, even if raw wait times initially favour in-person care. This study also discovered that new patients experienced a shorter time between appointment scheduling and service date by 8 days for teleconsultations compared to in-person visits. Thus, even at current volume, teleconsultations offer new orthopaedic patients more timely appointments.
It is important to consider that the availability of teleconsultation and in-person appointments likely reflects institutional constraints (e.g. slot allocation, resource distribution) and patient preferences. In our findings, we observed that 16% of in-person visits and 31% of teleconsultations were available on the day of clinic. While patients freely choose their preferred modality, this disparity likely reflects a combination of factors: patients may prioritize in-person visits due to familiarity or perceived urgency, while institutional practices and limited awareness/understanding of telehealth offerings could steer choices. Teleconsultations accounted for only 8% of total appointments, and faster raw scheduling times for in-person visits (median 2 vs. 3 days) may incentivize patients to select them. Thus, we cannot disentangle whether the difference in availability represents true patient preference or whether patients are selecting in-person because they are available sooner. Convenience, clinical need, unequal access to telehealth resources (e.g. digital literacy, broadband access), and systemic influences may also shape decisions.
Regardless, our findings should be interpreted within the constraints of a system prioritizing patient choice over clinical triage. Institutions with structured telehealth guidelines (e.g. restricting teleconsultations to specific indications) may observe different access patterns.
Additionally, our findings align with studies showing reduced telehealth uptake among Black, Hispanic, and other people of colour as well as older patients.51,52 These patients may face additional barriers such as mistrust in healthcare systems, lower comfort with technology, or socioeconomic challenges that limit access to devices or reliable internet. To address this, healthcare systems could implement digital literacy programs tailored to these populations or multilingual teleconsultation support. Such initiatives could help bridge the gap in telemedicine utilization.
This study has several limitations. First, we did not include factors such as patient travel and time off work when assessing access, which are known benefits of teleconsultations.38,53 However, the goal of this study was to provide a quantitative measure of access using three previously utilized methods, which did not include patient travel or work restrictions in their methodologies. Regardless, this concept may explain the discrepancy between our third next available and lead time findings. The third next available prospective data suggested there is more timely availability for in-person appointments, but our retrospective lead time data found that new patients were seen faster virtually compared to in-person. This may result from travel and work restrictions leading to further out appointment scheduling for in-person visits compared to virtual. Second, at our institution, in-person visits are offered with greater frequency than teleconsultations, which can make them difficult to compare and may decrease the generalizability of our findings. However, this ratio aligns with prevailing orthopaedic practice patterns, where most surgeons continue to prioritize in-person visits over teleconsultations. Our findings reflect the operational realities of hybrid care models during the study period, where in-person visits dominated scheduling systems. While this limits direct comparison, we utilized standardization based on visit frequency for the third next available method, which revealed untapped efficiency in virtual care that could inform resource reallocation. Third, our study did not assess technological barriers such as digital literacy, internet access, or device availability, which disproportionately affect rural, elderly, and low-income populations. 54 These barriers may explain the underrepresentation of certain demographic groups in teleconsultations (Table 2 and Figure 1, Table 3 and Figure 4) and limit telehealth adoption. Fourth, our findings should be interpreted within the context of post-pandemic telehealth normalization. Our study period (July 2022–January 2023) reflects a unique transitional phase where pandemic-driven telehealth familiarity coexisted with a return to routine care. While this provides insights into early post-pandemic telehealth adoption, it limits direct comparability to pre-COVID-19 or later post-PHEIC periods. 17 Fifth, our scheduling system relied on patient preference rather than structured criteria to determine visit modality, which may have led to mismatches between clinical needs and visit type (e.g. patients opting for teleconsultations when in-person care was more appropriate). Physicians could recommend in-person follow-up after teleconsultations if interventions (e.g. injections) or physical exams were required. However, this reflects real-world practice in many institutions lacking standardized telehealth triage protocols. Future work should develop evidence-based guidelines for visit modality selection. Despite this limitation, our findings remain valid for assessing access when patients freely choose their preferred modality, a common scenario in hybrid care models. The observed access advantages for teleconsultations (e.g. shorter lead times) suggest systemic inefficiencies in in-person scheduling, even when self-selection occurs. An additional limitation is that by focusing on high-volume virtual providers, our findings may not generalize to orthopaedic practices with lower telehealth adoption. However, this reflects a pragmatic compromise between data feasibility and clinical relevance. High-volume users are often early adopters of telehealth, making them ideal for studying systemic access patterns in hybrid models. Another limitation is the exclusion of APPs from our analysis. APP-led visits were omitted because they often follow distinct scheduling protocols and serve different patient populations compared to physician-led appointments, which were the focus of this study. However, given the growing role of APPs in orthopaedics, their exclusion may limit the applicability of our findings to real-world practice. Since certain musculoskeletal pathologies are more amenable to consultation via a virtual visit, having a list of top diagnoses would provide more actionable evidence. Lastly, surgeon workload indicators utilizing clinical volume metrics, time-based metrics, and surgeon scheduling impact, as well as benchmarking metrics such as productivity benchmarks, quality metrics (e.g. Press Ganey scores), and efficiency and cost metrics would yield insightful information between in-person and telehealth appointments. Surgeon workload indicators and granular diagnostic information are beyond the scope of this current study.
Current literature comparing orthopaedic appointment access between in-person and virtual settings is limited. A study taking place in London from 2014 investigated appointment efficiency of a newly implemented virtual orthopaedic fracture clinic compared to their previous all in-person model. 55 Post-implementation, 71% of all new fracture patients were seen in the virtual clinic. Prior to the virtual clinic, patient lead time between referral and first orthopaedic review was 10.9 days on average, which decreased to 5.1 days on average when utilizing the virtual clinic. 55 Additionally, prior to the virtual fracture clinic, 5.1% of new patients had an appointment within 72 h, which increased to 46.4% of patients following virtual clinic implementation. 55 Thus, the virtual fracture clinic increased patient access to orthopaedic care. In our study, we found faster prospective scheduling for in-person visits and a greater number of available same day return visits compared to virtual. We believe this is largely due to the smaller teleconsultation volume of 8% of total visits, as our standardized same day and third next available calculations suggest between 3.5- and 12-fold greater access for teleconsultations. In the London study, 71% of patients were seen virtually, which may have allowed for quicker access to appointments.
Another study from Ontario in 2018 investigated the effectiveness of a primary care practitioner (PCP) video referral system to orthopaedic specialists (eConsult). 56 PCPs connected with orthopaedic surgeons in an average of 3.7 days using the video referral system; the traditional referral system had an average time of 102.2 days between PCP referral and the patient appointment with an orthopaedic specialist. 57 For 36% of video referral patients, in-person orthopaedic consultation was deemed necessary. Therefore, unnecessary referral after eConsult was avoided in 64% of cases originally planned for in-person referral. Thus, the authors concluded the video referral system offered increased patient access to orthopaedic advice and decreased unnecessary consultation to orthopaedic surgeons. 56 Our findings are similar for new patients, but we found quicker access overall to in-person appointments at current volume. However, methodological differences exist, as this study measured teleconsultation vs. in-person patient access indirectly by investigating the time for PCPs to connect with orthopaedic surgeons via video referral and comparing it to the national in-person average for patient connection with a surgeon; thus, they did not consider any discrepancy in visit type frequency (teleconsultation vs. in-person). Our study specifically compared in-person vs. teleconsultation access at the same hospital system and in the same timeframe.
A non-orthopaedic study on this topic based in California investigated lead time for patients after scheduling in-person or virtual PCP visits with new medical concerns between 2016 and 2018. 45 They found teleconsultations were associated with a 35% reduction in days between scheduling date and appointment time (3.52 days for in-person, 2.29 days for video visits). When investigating same day appointments, they found teleconsultation patients were 10% more likely to choose a same day appointment than in-person patients. 45 These results are also similar to our lead time data for new orthopaedic patients, which suggests that teleconsultations offer decreased time between scheduling and appointment date. Previous literature has shown that shorter teleconsultation lead times may improve patient satisfaction by addressing time-sensitive concerns more rapidly.58,59
Future studies should pair access metrics with patient preference surveys to disentangle the interplay of availability, institutional capacity, and patient choice. For instance, a discrete choice experiment could quantify how patients weigh factors like lead time, travel burden, and visit type when selecting appointments. Such work would build on our framework to optimize telehealth adoption in orthopaedics. Future studies could also pair access metrics with longitudinal outcome tracking (e.g. reoperation rates, patient-reported pain/function) while differentiating ‘virtual care’ and ‘teleconsultations’ to holistically evaluate telehealth's value in orthopaedics. Additional studies could also investigate the role of APPs in hybrid care models to better understand their impact on patient access and scheduling efficiency or examine whether teleconsultations lead to different follow-up visit frequencies compared to in-person visits. Additionally, the optimal balance between virtual and in-person visits has yet to be determined. Based on the sensitivity analysis, a 20–30% increase in teleconsultations may be reasonable to maintain equitable access aligned with patient preferences. However, predicting the impact of increased teleconsultation volume on access is challenging, as patient preference and availability are interconnected.
Conclusion
Teleconsultations present a promising opportunity to enhance patients’ access to orthopaedic appointments for pathologies amendable to such visits. While in-person appointments currently offer shorter raw wait times, our findings reveal that teleconsultations exhibit greater standardized scheduling access and significantly shorter lead times for new patients, underscoring their potential to alleviate systemic bottlenecks. To implement an increase in teleconsultation capacity, institutions can adopt several practical strategies. First, appointment slots can be reallocated by dedicating specific days or times for teleconsultations, such as reserving 20–30% of daily slots for teleconsultations. Second, staff can be trained to manage hybrid workflows, including educating schedulers on offering virtual options and clinicians on remote consultation best practices. Third, robust technical infrastructure with reliable video platforms and patient support for digital access must be ensured. A phased approach, beginning with non-procedural visits like follow-ups or imaging reviews, can ease the transition. Finally, patient satisfaction and access metrics should be monitored to adjust allocations as needed, balancing improved access with operational feasibility. Clinics should also monitor outcomes (e.g. conversion rates to in-person follow-ups, patient satisfaction) to continue to refine hybrid workflows. These strategies could reduce delays exacerbated by external barriers like transportation and time off work. While in-person visits are integral to patient care in the orthopaedic clinic and virtual visits cannot be claimed to be equivalent to in-person visits, institutions that expand their teleconsultation capacity are poised to significantly improve patient access to physicians for appointments conducive to the virtual environment. This has the potential to improve health outcomes, satisfaction, and affordability while preserving in-person resources for hands-on care.
Footnotes
Ethical considerations
This study was approved by the institutional review board at our institution (IRB#16153).
Consent to participate
Informed consent to participate has been waived by the IRB.
Author contributions
NL contributed to conceptualization, data curation, formal analysis, investigation, methodology, writing – original draft, and writing – review & editing. NK contributed to formal analysis, investigation, writing – original draft, and writing – review & editing. AC contributed to formal analysis, investigation, methodology, writing – original draft, and writing – review & editing. JMC contributed to formal analysis, investigation, methodology, writing – original draft, and writing – review & editing. AL contributed conceptualization and writing – review & editing. KL contributed to formal analysis and writing – review & editing. CD contributed to conceptualization, methodology, writing – original draft, and writing – review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved by the institutional review board at our institution (IRB# 16153)
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
COI statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members.