
Abstract
Background
The Covid-19 pandemic has prompted healthcare professionals to adapt and implement new tools to ensure continuity of patient care. Teleconsultation became the only option for some practitioners who had never used it previously and boosted its use for others who already used it. Several studies have reviewed the use of teleconsultation in oncology during the epidemic, but few have addressed its continued use and how practitioners view it in a post-epidemic period. The aim of this survey was to conduct a qualitative exploration of how oncologists use teleconsultation in their daily practice in a post-COVID 19 period.
Materials and Methods
For this qualitative study, semi-structured interviews were conducted with oncologists in France who utilized teleconsultation in the field of oncology during the COVID-19 period. The interview guide included questions on the interests and limitations of using teleconsultation in oncology, on reluctance to use it among oncologists, and invited participants to formulate proposals for more optimal use.
Results
Fourteen oncologists participated in the survey. Currently, 12% of the consultations of the surveyed practitioners are conducted via teleconsultation. Seven themes were identified in the analysis of the interviews: (a) The oncologist and teleconsultation; (b) Clinical motivations for using teleconsultation; (c) Comparison between teleconsultation and in-person consultation; (d) Advantages and disadvantages of teleconsultation; (e) Technical modalities of teleconsultation; (f) Role of Covid and confinement in the use of teleconsultation; (h) Epistemic judgments about teleconsultation. Optimal teleconsultation occurs when seamlessly incorporated into patient care, offering reduced patient inconvenience, and providing economic and environmental benefits. Although there's a lack of unified agreement in research literature regarding time efficiency, teleconsultation facilitates more customized patient monitoring and addresses the challenge of “medical deserts” nationally. Considering patient preferences is crucial when contemplating the use of teleconsultation. Predominantly, technical issues stand as the principal barriers to teleconsultation implementation.
Conclusion
Even after the end of the health crisis, teleconsultation is still used in clinical practice. Recommendations for effective use are suggested.
Introduction
Teleconsultation is defined as “a form of remote medical practice supported by information and communication technologies. It brings one or more healthcare professionals into contact with one another or with a patient. It always involves a medical professional and, where applicable, other professionals providing care to the patient. Telemedicine makes it possible to establish a diagnosis, to ensure, for a patient at risk, preventive or post-therapeutic follow-up, to request a specialist opinion, to prepare a therapeutic decision, to prescribe medicine, to prescribe or perform services or procedures or monitor the condition of patients”. 1
Teleconsultation in oncology can be defined as the remote delivery of healthcare services to cancer patients through video or telephone calls. It can be viewed as a virtual appointment between a physician and a patient. This approach has become increasingly popular in recent years, as it provides patients with access to specialized medical care from the comfort of their homes. In France, Social Security began reimbursing teleconsultation procedures on 15 September 2018. 2 Nonetheless, data from Social Security suggests that only 60,000 teleconsultations were invoiced across the entire country during the initial year, up to September 2019. 3 With the COVID-19 pandemic, teleconsultation has gained more attention as a means to maintain social distancing and reduce the risk of infection for cancer patients who are often immunocompromised.4,5 Accordingly, the number of teleconsultations registered by Social Security has skyrocketed, with more than 4.5 million registered in April 2020 and more than 1 million in the summer of 2020. 4 Teleconsultation has the potential to improve access to care for cancer patients in remote areas or for those who face logistics or transportation challenges. 6 It can also increase convenience and reduce costs. 7 However, its effectiveness in comparison to traditional in-person consultations is still being evaluated.
Patients report positive views on teleconsultation,8,9 but the opinion of health professionals remains unclear. 10 Several studies evaluating physician satisfaction have shown that teleconsultation can be integrated into the daily management of cancer patients.11–15 These studies confirm that teleconsultation ensures continuity of care (hence its rise during the COVID-19 pandemic) and that it does not affect the doctor–patient relationship, or the quality of care offered. However, recurring technical problems, difficulties associated with certain patient profiles and perhaps entrenched habits mean that a majority of physicians who responded to our questionnaire still prefer a face-to-face physical consultation to teleconsultation.10,11 Some authors report that such virtual interactions between oncologists and patients may actually reduce understanding between patients and families, leading to an increased number of subsequent requests thereafter. 11 Additionally, others are concerned about the development of “medical nomadism”: teleconsultation can facilitate the request for multiple advice from various physicians, with repercussions on the effective initiation of a treatment, in particular if the opinions of specialists diverge. 16
Thus, it appears necessary to improve the use of teleconsultation for daily clinical practice, to establish clinical practices guidelines based on scientific evidence, but also to consider training physicians in digital tools. 17 Several medical French university deans recently agreed that training in telehealth in insufficient and should be developed as soon as possible. 18 This is important because a physician's telehealth experience can have a significant effect on patients’ telehealth experiences, which could lead to a disparity in care. 19
Thus, it seems important to ascertain the feelings of oncologists on their practice of teleconsultation in routine clinical care: hence the interest of a qualitative evaluation resulting from semi-structured interviews.
Materials and methods
Objective
The present study aims to explore the experience of oncologists regarding teleconsultation practice through semi-structured interviews. It follows and complements a quantitative survey that was conducted by means of a questionnaire from April to October 2021. 15 This study was approved by the Center Léon Bérard institutional review board and by the Auvergne Rhône-Alpes Regional Health Authority. The survey was conducted from October 2021 to April 2022. Participants were eligible if they were oncologists in the region covered by the survey and if they resorted to teleconsultation. No exclusion criteria were retained. All participants agreed to participate freely and gave written informed consent.
Sample
During the online survey, 15 28 oncologists out of 64 participants agreed to be contacted by email for semi-structured interviews. The participants were therefore a sample of oncologists practicing in the French Auvergne-Rhône-Alpes region.
Procedure
All interviews were conducted by a single interviewer using videoconference between October 2021 and April 2022.
The Interviewer is a woman who holds a Doctorate in Health Psychology and is Associate Researcher at the LIP/PC2S Laboratory of Grenoble Alpes University. Her research interests include understanding the psychological issues, needs, resources, and strategies of adjustment in people confronted with cancer (patients, entourage, professionals). No relationship had been established between the interviewer and the interviewees prior to the interviews. Interviewees were asked to participate in the second phase of the study on the use of teleconsultation in oncology. The interviews commenced with the collection of participants’ sociodemographic data through closed-ended questions, followed by open-ended questions, guided by an interview framework that enabled participants to expand on their responses (Table 1). The interview guide, first reviewed, and verified by the study's co-author, utilizing a semi-structured approach, outlined the primary themes to be discussed and questions to be posed to participants if themes weren’t organically addressed. The guide was not used systematically and themes were not consecutively addressed, but it served to steer discussions or facilitate their progression when necessary. To facilitate exchanges, all interviews were recorded with the participants’ agreement. The interviews aimed to gather information on the interests and limitations of teleconsultation practice in oncology, on reluctance levels among oncologists to use it, and on possible proposals for optimal use.
Semi-directive guide for interviews

Data analysis
Statistical analysis of sociodemographic date was carried out with the Statistical Package for the Social Sciences (SPSS.22) software. Each interview was transcribed electronically. The transcripts were not sent to participants for possible comments or editing. Transcripts were subjected to a thematic content analysis. 20 This method consists in identifying recurring themes in verbal or textual material, based on key words, key expressions, or salient phraseology. 21 In other words, thematic analysis consists in systematic identification and classification of key themes present in a corpus, combined with discursive analysis. 22 Accordingly, main themes and sub-themes were identified in our corpus of interviews and associated with relevant quotations, using excerpts from the oncologists’ discourse. Thematic analysis was performed by another researcher trained in corpus linguistics. The outcomes of this analysis were not sent to participants for possible comments (please see the COREQ checklist in the appendix).
Results
Participant description
Among the 28 oncologists who agreed to participate in the second phase of the survey, 14 participated in the interviews, among whom six men and eight women, with a mean age of 47 years (SD = 10). The reasons why 14 oncologists declined to participate are unknown. They did not respond to additional emails inviting them to participate in the second phase of the survey. Table 2 presents the characteristics of the study population sample.
Participants demographics.

Mean duration of the interviews was 23 min (SD = 11). At the time of the study, 12% of the consultations were conducted by the surveyed oncologists via teleconsultation. One out of 14 doctors (7%) reported being completely averse to teleconsultation. Nine participants (64%) reported discussing the use of teleconsultation in oncology with their colleagues, and two (14%) reported that they read literature on the subject.
The thematic analysis of the interviews revealed seven main themes (Table 3).
Thematic category and theme.

The practitioner and teleconsultation. A majority of surveyed practitioners started using teleconsultation during the COVID-19 pandemic. For all but one oncologist, its use continues, but with a significant decrease. Teleconsultations are “offered to the patient, who may refuse.” The use and scheduling of teleconsultation depend on practices and specialties. Some practitioners include teleconsultations every month between their 3-month follow-up consultation to “readjust” therapy if necessary. In their schedule, teleconsultations are usually scheduled “early in the morning, but on any day.”
Clinical motivations for the use of teleconsultation. Oncologists report the usefulness of teleconsultation, as it allows to cover multiple subjects with patients in a comprehensive fashion. Another advantage is rapid transmission of medical results. Practitioners would recommend it for “non-crucial” encounters and “ordinary patient follow-up.” The hybrid mode of care (alternating in-person consultations and teleconsultation) has an interest in follow-up treatment. However, for certain cancer types requiring physical consultation, teleconsultation is not feasible. The patient's individual profile affects the use of teleconsultation. Teleconsultations for patients with pain or metastases seem difficult. Teleconsultations are useful for patients living in medical deserts.
Patients must have been seen in-person before teleconsultation is proposed. This makes it more productive, more relevant, justifying its use, because some of the work has already been done beforehand. This condition seems essential for a majority of respondents. However, teleconsultation remains interesting for unforeseen appointment requests, to discuss chemotherapy-related side effects, for example.
In conclusion, respondents reported that they mainly resorted to teleconsultation for post-treatment monitoring consultations, for follow-up consultation in the context of oral anticancer treatment, as well as for unforeseen requests for consultation related to treatment side effects without a life-threatening emergency. Teleconsultation is consistently avoided in several scenarios: initial consultations with new patients, consultations to disclose initial illness, disease recurrence or progression, consultations to commence an oral anticancer treatment, and follow-up consultations under a strictly palliative care context.
Comparison between teleconsultation and in-person consultation. In-person consultation remains preferred by most practitioners. It opens up more discussion with the patient; its added value lies notably in the ability to better assess non-verbal communication. The main limitation of teleconsultation is the inability to physically examine the patient. Practitioners report that there is a personal preference of patients for in-person consultation.
Teleconsultation changes the relationship with the patient. On the one hand, practitioners state that listening is different and that the link with the patient is not the same. On the other hand, a “video effect” allows some patients to feel more at ease.
In certain instances, such as reviewing biological tests or interpreting medical imaging, a physical consultation is not requisite. Teleconsultation is employed for patient monitoring but is never utilized in situations necessitating a diagnosis. It is applied when a trustful relationship with the patient has previously been established.
Advantages and disadvantages of teleconsultation
The main advantages highlighted by oncologists are economic. They also underline its environmental interest. Teleconsultation is also perceived as comfortable for patients, involving less fatigue and stress. It is time-saving for patients who can “request a consultation more quickly” but also for practitioners: “shorter consultation.” However, opinions remain mixed on this point. For some practitioners, teleconsultation has allowed them to gain in “quality of life at work” with less “pressure from the waiting room.” Conversely, others for whom teleconsultation is not integrated in their schedule report that it is not a time saver.
Some practitioners report an increased workload related to teleconsultation for their secretariat as well as organizational difficulties: “explaining to the patient.” There is a lower quality in the consultation. Some practitioners raise concerns that teleconsultation could become an additional source of social exclusion or discrimination.
Finally, teleconsultation seems conducive to a different “presence” of the caregiver.
Technical modalities of teleconsultation. The technical problems encountered remain numerous and are mitigated by another modality, the telephone. Some patients may be barred from teleconsultation due to the lack of appropriate digital devices: “elderly people,” “20% of cancer patients do not have an email address.”
Practitioners agree that the use of teleconsultation can be facilitated, provided that adequate digital means are available.
The role of Covid and confinement in relation to the use of teleconsultation. Practitioners report that teleconsultation is recommended in times of crisis. The Covid period was the trigger that actually prompted many practitioners to develop teleconsultation in their practice.
Epistemic judgments on teleconsultation. In grammar, epistemic modality relates to everything concerning knowledge of the world, which can be found in the expression of a subjective judgment, belief, or opinion.
The majority of oncologists report that the implementation of teleconsultation remains a successful approach, generating positive impacts on service organization and the way of working. However, success depends on being able to conduct a teleconsultation with an “ideal patient profile,” that is, “one who is familiar with computer tools, has a network, is young, autonomous in decision-making, and in disease management,” or has “a stable illness.” If these conditions are not met, the assistance of a close relative is necessary. Oncologists agree not to give any announcement by video or phone.
For only one of the participants, teleconsultation is “a failure.”
Discussion
The advantages of teleconsultations, motivations, and criteria for using this practice in oncology
Teleconsultation "was born" in the practice of some practitioners during the Covid period. The majority of oncologists in the survey report that they will continue to use it in their practice, in line with the literature.23,24
The main advantage reported by practitioners is that teleconsultation ensures continuity of care: for example, it is easier for a patient to request a teleconsultation to ask about side effects related to their treatment than to request and wait for a physical consultation. Practitioners did not report any fear of dehumanization of the doctor–patient relationship. Teleconsultation is appreciated because it is integrated into the care pathway as Bibault et al. 25 have demonstrated. Some physicians in our survey stated that they refrained from utilizing teleconsultation in the palliative care setting for their cancer patients, aligning with the reservations voiced by certain authors regarding the utility of teleconsultation when conducted directly between members of a palliative care team and the patient. 26 However, Buckmann et al. 27 have reported its potential value in this context, aiming to enhance and streamline collaboration among various medical disciplines in palliative care.
Many practitioners from our survey employ teleconsultation, such as on the day preceding chemotherapy sessions, facilitating discussions about any ongoing issues with patients and enabling in-person meetings on the subsequent day—the scheduled chemotherapy day—should an issue necessitating a physical examination arise. When teleconsultation is not incorporated into a patient's care pathway, challenges may emerge related to managing the influx of patient requests for additional teleconsultations between appointments. Teams might contemplate ways to optimize the scheduling of teleconsultation appointments. 28 Seeking second opinions is prevalent in oncology (6.5% to 36% of cancer patients) as a means of obtaining reassurance or contemplating various treatment options.29,30 While teleconsultations seem to ease access to second opinions for patients, they may concurrently pose higher risks of delaying the management of complex or rare cancers. 10 This concern is particularly pointed when there is discordance in treatment plans, stemming from multiple care providers offering conflicting advice, potentially escalating anxiety and confusion for the patient. 31
Other advantages are energy savings, a reduction in stress and pain for patients, as well as economic and environmental benefits related to travel, consistent with previous studies.32–34 Oncologists remain divided on time savings. On the one hand, in the absence of a clinical examination, teleconsultation seems to take place more quickly than a physical consultation, and it allows for certain discussions (such as about transport vouchers) to be avoided. On the other hand, it requires additional work time for the secretariat. Teleconsultation allows for a more comprehensive view of the patient and capitalizes on the fact that they remain in their private sphere. Access to the environment where patients live seems to ensure more personalized follow-up. Moreover, the literature suggests that this patient-centered approach promotes disease self-management.34–37 Also, practitioners who responded to our survey feel that patients seem more comfortable at home discussing certain topics. Interaction on a computer screen does not seem to be an obstacle; it even seems to facilitate the transmission of information. However, Powell et al. 37 indicated in their study that patients reported difficulties in finding a sufficiently “private” place at home to conduct the teleconsultation and feel comfortable sharing sensitive information. Practitioners reported a different involvement of caregivers. They are present in teleconsultation but not known during in-person consultations. However, during physical consultations, more attention seems to be paid to them, unlike in teleconsultations. Finally, teleconsultation appears to be a promising solution to “relieve” medical deserts as Snoswell et al. 7 previously showed.
The limitations and barriers to the use of teleconsultation
The main limitation to the use of teleconsultation in oncology is the inability to perform a physical examination. This finding is consistent with the literature review conducted by Thiyagarajan et al. 38 The absence of a physical examination is associated with the difficulty of assessing the patient comprehensively. Teleconsultation requires the practitioner to adapt in order to understand the patients’ symptoms. These authors also reported that patients with chronic diseases are more likely to prefer a face-to-face consultation. Teleconsultation should be considered as an adjunct and best used to supplement in-person visits. Consistent with this, practitioners in our survey stated that the physical examination allows for intimacy with the patient, creating a connection that goes beyond the medical aspect. In teleconsultation, the “official” context of the medical consultation seems to be lost: it is less perceived as a formal appointment or a consultation that will move the case forward. Non-verbal communication remains limited: according to oncologists, there is a loss of information (for example, not seeing how the patient moves to the doctor's office).
The other barriers mainly reside in technical difficulties (connection, network, sound problems). This is in line with the literature: the easier the technology, the more it is used. 39 The importance of equipment, as well as network efficiency, is fundamental, as without them, there is no teleconsultation. A number of teleconsultations end up being conducted over the phone. The systematic review by Rush et al. 36 found that visual consultations have significant advantages over consultations by phone. These advantages are reflected in fewer medication errors, greater diagnostic accuracy, and better decision-making accuracy.
Other barriers are more specifically related to oncologists’ work organization and the additional burden on medical secretaries in implementing teleconsultation. This point was raised in the study by Jess et al. 40 The concerns of healthcare professionals were particularly related to the workload that video consultations can entail. If video consultations are not part of the practitioner's usual way of working, and if they are only conducted with a few patients, professionals may see this as a disruption to their usual work routine, and the lack of routine becomes a barrier. It is necessary to integrate teleconsultation into standard consultation schedules. Additionally, access to technical support for patients and ongoing training for practitioners are necessary to help them use these new technologies to their full potential.
Finally, some practitioners reported a fear of exacerbating inequalities in access to healthcare and social discrimination through the widespread use of teleconsultation. The French government, recognizing its potential benefits and challenges, has taken steps to ensure that telemedicine services are both accessible and maintain a high standard of care. Keeping a balance between promoting innovation and ensuring patient safety (initially with a limited number of teleconsultations per year per patient) is essential. Political discourse and regulatory guidance will continue to evolve depending on the evolution of teleconsultation and its use.
Recommendations for good teleconsultation practice in oncology
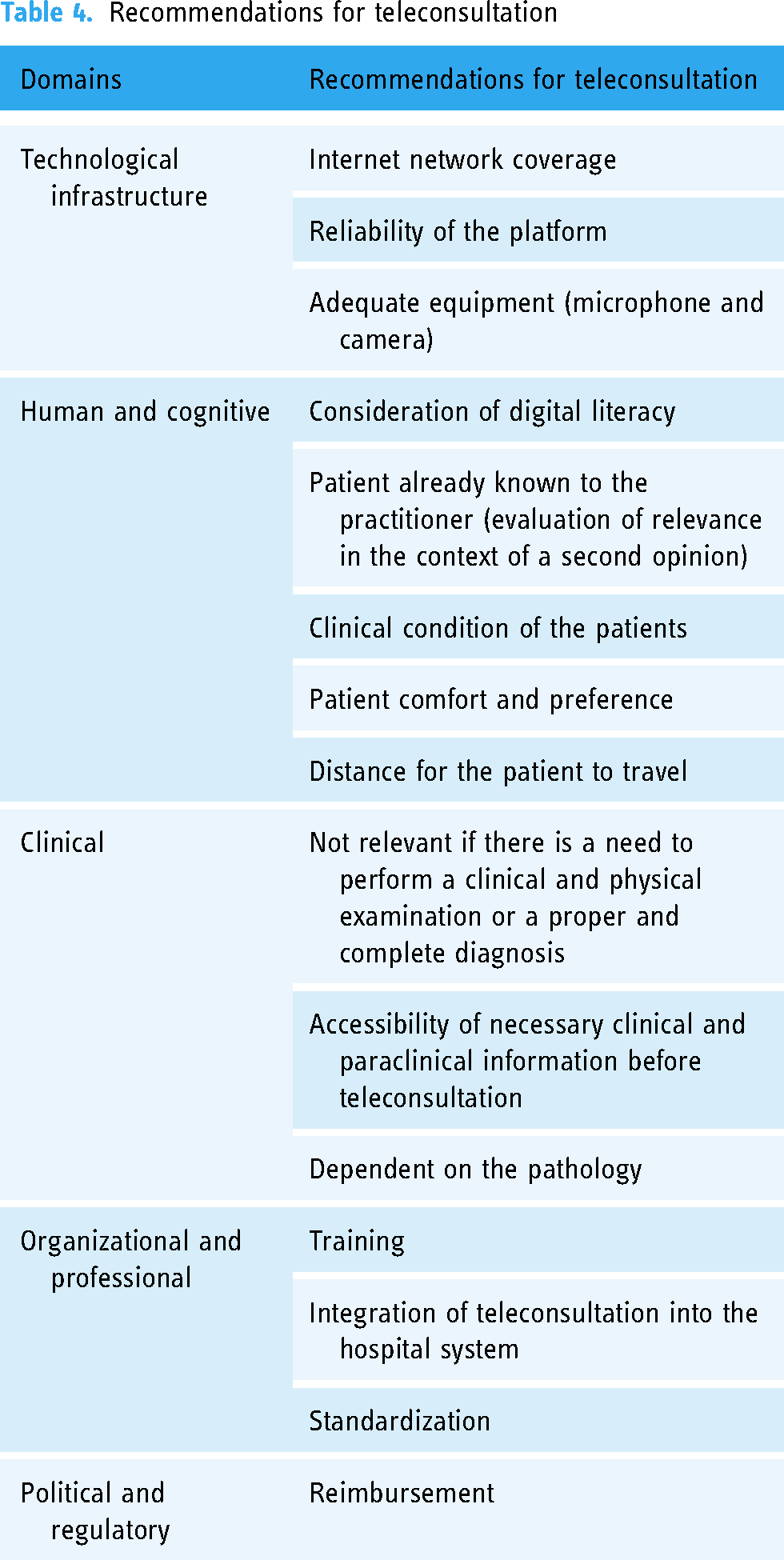
The results of this survey provide “lessons learned” for the use of teleconsultation in oncology. 41 Table 4 provides some recommendations for good practice in four main areas, supplementing the article by Boudjema et al. 42 on best practices in telemedicine. Several facilitators for the use of teleconsultation in oncology are reported: internal factors that mainly refer to the behavior and motivation of users, but also external factors that refer to the environment surrounding its use.
Recommendations for teleconsultation
Limitations
A principal limitation of this survey resides in the modest participant number, despite achieving a 50% participation rate. Additionally, the predominance of respondents specializing in two areas (senology and digestive cancers) might impact the representativeness of our survey. Obtaining concurrent feedback from patients about their teleconsultation experiences in the surveyed centers would have also been insightful. Lastly, given that this was a retrospective study, a before/after evaluation of oncologists’ sentiments regarding their care would have enhanced the investigation's potency.
Conclusion
Teleconsultation serves as a valuable tool in clinical practice, offering numerous advantages in oncology across various scenarios. Our survey respondents identified several key criteria for recommending teleconsultation: patients must have a reliable internet connection, reside at a significant distance from the healthcare center, possess the capability to make autonomous decisions, and manage their illness. Additional factors include having a stable or stabilized disease, assessing patients’ cognitive abilities, considering their age, and, if necessary, ensuring the presence of a caregiver. Furthermore, accommodating the patient's preferred consultation format is essential. The use of teleconsultation prompts inquiries into the role of caregivers, the work-life quality of oncologists, and the needs of both practitioners and patients, functioning as a means of sustaining connectivity. Its optimal utilization is observed when seamlessly integrated into the daily practices of oncologists and the patient's care journey.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231215906 - Supplemental material for A qualitative study of teleconsultation practices among French oncologists in a post-COVID-19 period
Supplemental material, sj-docx-1-dhj-10.1177_20552076231215906 for A qualitative study of teleconsultation practices among French oncologists in a post-COVID-19 period by Sophie Lantheaume, Louis Doublet, Jean-Eudes Mory, Thierry Durand, William Lebosse and Pierre-Etienne Heudel in DIGITAL HEALTH
Footnotes
Contributorship
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Sophie Lantheaume. The first draft of the manuscript was written by Pierre-Etienne Heudel and Sophie Lantheaume and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Center Léon Bérard institutional review board and by the Auvergne Rhône-Alpes Regional Health Authority.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.