
Abstract
Transplant patients represent a complex patient population for which telemedicine may allow enhanced access to the healthcare team and promote active engagement in health improvement. This retrospective study summarizes a multi-pronged approach that was instituted to implement a pharmacy telemedicine practice at our institution. Telemedicine visits included the provision of six key elements for our patients: (1) medication reconciliation, (2) vaccination history, (3) medication teaching, (4) pharmacotherapy review, (5) medication adherence, and (6) triage to other providers. From January through June 2017, 46 patients were registered for a visit (recipients n = 32 and living donors n = 14). Three-fourths of the patients who completed a visit connected using a mobile device. Time from discharge to the visit was 5.4 days. The average visit duration was 11.6 ± 8 minutes. Medication reconciliation was performed for 24 patients where 6 (25%) required medication list adjustments. An average of 1.2 ± 0.4 medication changes were updated in the medical record. During visits, patients were asked questions to assess adherence to their regimen, all patients responded favorably indicating that they were following instructions provided by the healthcare team. Telemedicine has the potential to improve the healthcare delivery model by providing increased patient-to-healthcare team interactions and access, which optimize engagement and outcomes.
Introduction
Solid organ transplantation is the treatment of choice for patients with end-stage organ failure. Patients eligible for an organ transplant represent a complex population, which require pre-transplant evaluation and preparation followed by post-transplant lifelong monitoring and interactions with a multidisciplinary medical team. Telemedicine allows health care professionals to interact with patients remotely using digital healthcare technology.1–3 This technology provides patients opportunities for enhanced access to their healthcare team from the comfort of their own home, and has potential to promote active engagement in health, which may translate to improved patient satisfaction and outcomes.4–6 Implementation of telemedicine in high-risk patient populations, such as transplant patients, provides opportunities for continuous interactions with patients, as Schmid et al. demonstrated a positive impact in practice. 7 In addition, this practice enables healthcare systems to overcome the physical barriers of space constraints in outpatient areas.8,9 The adoption of telemedicine in clinical practice has increased as the access to digital technology becomes more abundant. 8 Studies in transplantation have described use of telemedicine as part of waitlist management to improve quality of life and increase patient knowledge,10–12 living donor care to increase patient access and reduce travel costs during donor organ procurement to assess donor organs.11,13–15 In the post-transplant phase, telemedicine has been used for patient education to increase patients knowledge about skin cancer risk,16,17 and adherence with laboratory and medication regimens.18–20 Studies describing implementation and use of telemedicine for pharmacy services are limited.
The United Network for Organ Sharing (UNOS) and Centers for Medicare and Medicaid Services (CMS) specifically mention the clinical transplant pharmacist as a mandatory component of the multidisciplinary care team. 21 A telemedicine clinic can enhance the pharmacist’s ability to provide patients with medication education, monitor pharmacotherapy, and enhance medication adherence in a comfortable setting for the patient. Pharmacists can expand their outreach to patients, which ultimately improve quality, outcomes, and efficiency. Telemedicine can strengthen operational workflow for pharmacists, enabling them to have personalized face-to-face interactions with patients. Furthermore, it can enhance communication regarding pharmacotherapy and medication profiles with the multidisciplinary medical team to ensure adherence to program protocols and provision of up-to-date information. 22 As transplant pharmacists in a large academic medical center, we established and grew the use of telemedicine to reach our patients. Telemedicine was implemented in an effort to provide better access for patients to pharmacy services in their continuum of care. The purpose of this article is to outline the trials and tribulations we experienced in establishing our pharmacy telemedicine clinic in a kidney and pancreas transplant practice, which represents a high-risk patient population.
Methods
This single-center, retrospective study summarizes a multi-pronged approach that was instituted to implement a pharmacy telemedicine practice at our institution. This study was approved by the Institutional Review Board. During the initial development stages, a population assessment was performed to examine our patient’s access and perceptions with using technology. An internally developed questionnaire was used to ascertain availability of electronic resources (e.g., smart phones, computer, tablet, etc.) and perceived benefits of technology in healthcare. This questionnaire was distributed by our clinical team to transplant patients admitted to the hospital or coming to clinic for post-transplant follow up visits. Secondly, a team of clinical pharmacists developed a standard operating procedure that represents important intervention areas for our transplant patients and donors was created: medication reconciliation, vaccination history, medication teaching, pharmacotherapy and protocol review, medication adherence, and answering medication-related questions. Each element is described in detail below:
Medication reconciliation: Maintenance of an accurate medication list in the medical record and for the patient is critical to ensure patient safety and optimal outcomes. Transplant patients are at an increased risk of medication errors due to the frequent transitions of care in the pre- and post-transplant environment, the number of medications required (typical regimens contain up to 12 medications), and the frequent changes needed in their medication regimens following transplantation. Vaccination history: Transplant candidates and recipients are at increased risk of infectious complications. The response to vaccines is diminished in organ failure; hence, it is important for transplant candidates to be immunized early in the course of their disease. Maintaining current vaccination histories can potentially decrease unnecessary healthcare costs for both the patient and our institution. Medication teaching: Pre-transplant: Educating transplant candidates and their families about the safe use of transplant medications is an important proactive step to ensure an understanding of the complex nature of transplant pharmacotherapy and share expectations with the patient before they embark on the transplant journey. Post-transplant: Kidney transplant recipients have a short hospital stay with a limited amount of time to learn and retain information about their discharge regimen. Patients with lower levels of health literacy are particularly vulnerable to adverse drug events. Close follow-up after discharge presents an opportunity to optimize patient understanding about their medications. Pharmacotherapy review and transplant program protocol compliance: Most transplant patients will receive therapy based on the hospital medication management protocol, which coincides with the treatments recommended by respective guidelines and clinical practices. In order to ensure compliance to protocol, patient’s course of therapy must be monitored from the start of admission and followed in the outpatient setting to ensure medication use safety. Medication adherence: Adherence to immunosuppressive medications after transplantation is vital in maximizing positive clinical outcomes, yet nonadherence occurs in 30% of transplant recipients.
23
Telemedicine visits enable pharmacists to promote adherence and monitor patient progress. Triage to other providers: Interactions that pharmacists have during telemedicine visits may identify opportunities for referral to other disciplines to provide comprehensive services.
Finally, in partnership with the Information Technology Department’s Innovation Team, the transplant team created a patient-centered telemedicine workflow while taking into consideration the pharmacist’s daily routine (Figure 1). Patients were identified for a virtual visit during their index hospitalization for transplant or living donation. During standard medication teaching sessions, required as part of practice, the pharmacy team assessed which patients had access to technology with webcam capabilities (smartphone, laptop, or tablet) and registered patients for a post-transplant virtual pharmacy visit with the outpatient transplant pharmacist after hospital discharge. A member of our pharmacy team created an account and downloaded the in-house developed app to the patient’s device. The app utilizes American Well’s software development kit, which allows video visits to occur through the American Well platform. The app provides the interface for the video visit, which is encrypted and Health Insurance Portability and Accountability Act (HIPPA) compliant. During this process the pharmacy team member explained the visit structure and expectations to the patient and asked if a test visit was desired. Members of the IT Innovation Team conducted test visits with the patient 24 h prior to the scheduled virtual visit to troubleshoot any potential issues beforehand, saving the pharmacist time during the virtual visit.
Transplant pharmacy virtual visit follow-up workflow.
Results
Technology assessment survey.

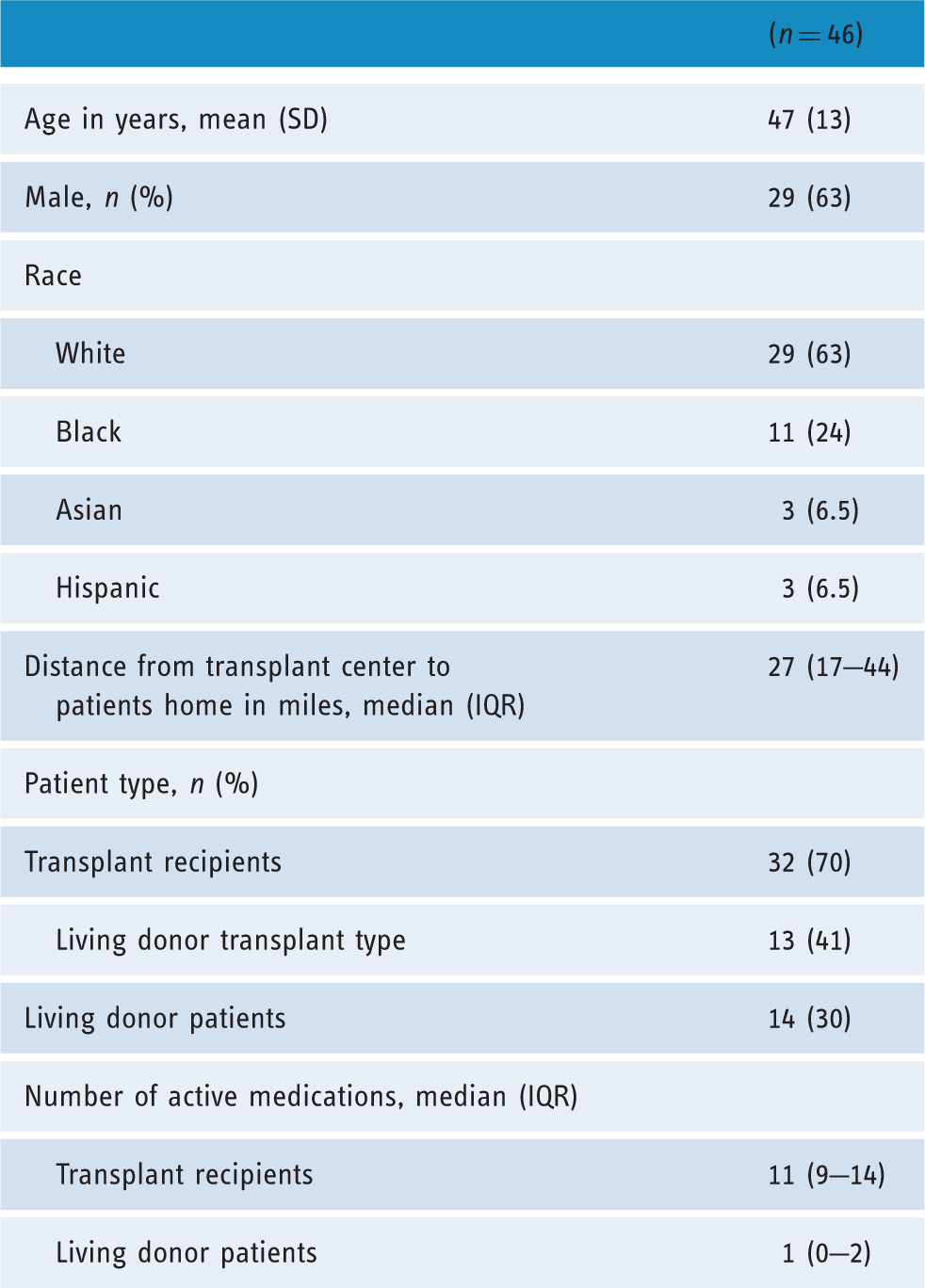
Baseline demographic characteristics.
Discussion
Integrating a novel approach to healthcare delivery in a high-risk patient population of transplant recipients has revolutionized our practice model. Our study contributes to the existing literature by describing a telemedicine implementation for transplant pharmacy services, which are currently limited. Prior to implementing telemedicine, transplant pharmacists at our center were limited to practice as inpatient clinicians. This technology and practice model enhancement has enabled us to provide pharmacy services in the continuum of care as patient’s transition from the hospital and clinic to home setting. This practice has been important to ensure the safe and effective use of medications for our patients; for example, we have had an opportunity to identify and quickly resolve a patient care issues related to pain management, which may have gone unnoticed or led to an emergency department visit had we not seen the patient. The described pharmacy telemedicine practice model can be generalized to other institutions and patient populations with complex medication regimens and multiple comorbidities who may benefit from a pharmacy consultation. The essential key to success is involving key stakeholders early in the development process to ensure adequate support and collaboration. Our telemedicine practice has continued and expanded in scope to the pre-transplant phase of care with an emphasis on medication reconciliation and education. All patients are offered a 1-month follow up check-in after the initial visit, which has allowed the pharmacy team to establish a relationship with patient in advance of their transplant surgery.
This is a newly developed practice model and long-term follow up is not yet available. Currently, the patients in this cohort have only had one post-transplant telemedicine visit and adherence assessments were only conducted at a single time point (early post-transplant) at the first telemedicine encounter. As our population grows and follow-up time progresses, we will have opportunities to further engage with patients through additional telemedicine visits to reassess our six key elements approach. Strategies to minimize no-show rate continue to be explored; in addition to the standard app, email and calendar reminders, patients are encouraged to set an alarm that will remind them about the upcoming appointment. Patients who are not seen by a pharmacist because they did not show to a visit are contacted by telephone on three occasions to reschedule their appointment. Transplant centers care for unique high-risk patients that must be seen and cared for locally in a routine, life-long fashion. Telemedicine allows expansion of services without requiring physical real estate. In addition, telemedicine visits increase access to the transplant pharmacist and allow patients to benefit from clinical services and learn in a non-overwhelming, comfortable, and familiar setting.
Footnotes
Contributorship
NJ, BW and DT designed the research/study and collected data. All authors analyzed data, co-wrote the paper, and contributed to the development of this manuscript.
Conflict of interest
The authors declare that there is no conflict of interest
Ethical approval
The Columbia University Institutional Review Board approved this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Guarantor
DT
Peer review
This manuscript was reviewed by Elizabeth A. Krupinski, Emory University, Atlanta, Georgia, USA and two other individuals who have chosen to remain anonymous.