
Abstract
Background
Breast cancer is one of the most common cancers among women globally, but there is a lack of public knowledge about breast health, and traditional health education methods are insufficiently interactive and difficult to sustain motivation for learning. Metaverse is a 3D immersive environment that allows real-time interaction through digital bodies. Integration of metaverse and gamification technologies provides new solutions to enhance learning.
Objective
The objective of this study is to evaluate the immediate and short-term effects of a gamified metaverse platform (Mammoverse) on breast health knowledge, and to explore how key design elements influence users’ learning motivation and behavioural intentions.
Methods
This explanatory sequential mixed-methods study was conducted between December 2024 and March 2025 with 36 women aged 20–30 years. Participants completed a single 20-minute experience with the Mammoverse platform and were assessed on breast health knowledge at baseline, immediately post-intervention, and 4 weeks later using Friedman and Wilcoxon signed-rank tests. Semi-structured interviews were conducted post-intervention and analysed thematically to explore user experience and motivation.
Results
Knowledge scores improved significantly post-intervention and at 4-week follow-up compared to baseline (17.44 ± 0.97 and 15.72 ± 1.83 vs 8.97 ± 2.57, P < 0.001). Qualitative data confirmed that immersive and gamified features – such as points, challenges, and achievements – enhanced user motivation and knowledge acquisition.
Conclusion
The Mammoverse platform excelled in enhancing immediate and short-term retention of women's breast health knowledge, reflecting the advantages and potential of gamified metaverse technology in the field of breast health education, which is worthy of further dissemination and research.
Introduction
Breast cancer is one of the most common malignant tumours in women worldwide, posing a serious threat to women's lives and health, and has become one of the major challenges in global public health. 1 According to the World Health Organisation, approximately 2.1 million women worldwide are diagnosed with breast cancer each year, accounting for nearly one-third of all female cancers, and the incidence continues to rise. 2 It has been shown that early breast cancer screening helps to detect the disease at a curable stage, thereby significantly reducing mortality and improving survival.3–5 However, due to insufficient awareness of screening and lack of breast health knowledge, many women fail to detect lesions in time and miss the best time for treatment. 6
Breast Self-Examination (BSE) is widely recommended as a simple, cost-effective, and non-invasive tool for the early detection of breast cancer. 7 Harvey et al. showed that more than 65% of breast lumps were detected by women during routine self-examinations, and Newcomb et al. found a significant reduction in the risk of breast cancer death in women skilled in BSE.8,9 However, the global implementation of BSE has not been favourable.10–12 Both developing and developed countries demonstrate a widespread lack of knowledge, inadequate practices, and low awareness of the importance of active participation in BSE.13,14 Many women remain unaware of the optimal methods and timing for conducting BSE and often avoid it due to anxiety and the psychological burden associated with discovering abnormalities.15,16 Traditional social and cultural factors, such as women's reluctance to undergo breast examinations and a lack of family and social support, also significantly hinder the promotion of breast self-examination. 17 In addition, traditional methods of breast health education, such as health talks, brochures and mass media campaigns, have revealed significant shortcomings in practice. It has been found that these types of educational methods have difficulty in maintaining the long-term attention and active participation of the audience, resulting in limited retention and application of the information. 18 Dhakal et al. (2023) further pointed out that although the traditional model improves knowledge in the short term, the effects of its interventions are difficult to sustain. 19 Therefore, how to effectively raise women's awareness of breast health and encourage them to develop the habit of regular breast self-examination has become an important issue that needs to be addressed in the field of breast health education. In response to this issue, there is an urgent need to develop educational tools that are more interactive, personalised, and effective in promoting long-term participation.
With the development of digital technology, the emerging technologies of Metaverse and Gamification provide new opportunities for the transformation of health education. Metaverse refers to a highly immersive 3D virtual environment in which users can interact with digital bodies in real time for a realistic and immersive learning experience.20–22 Gamification, on the other hand, is the introduction of mechanisms such as points, levels, feedback and rewards in non-game contexts, aiming to stimulate active participation and intrinsic motivation of users.23,24 Studies have confirmed the positive effects of these two techniques in enhancing health knowledge acquisition, engagement and behavioural motivation, respectively.25,26 However, most of the current studies still focus on the application of a single technology, and there are few systematic explorations on the integration path of metaverse and gamification, especially in the field of breast health education, where there is a lack of empirical studies.
Therefore, this study innovatively designed and developed the Mammoverse platform, a breast health education tool integrating metaverse and gamification elements, aiming to improve women's breast health knowledge and behavioural intentions. The metaverse plus gamification intervention is more in line with the theoretical mechanisms that motivate users than the traditional passive approach to health education. According to Self-Determination Theory (SDT), individuals show higher engagement when experiences satisfy autonomy, competence, and relatedness. 27 The immersive nature of the metaverse, coupled with the challenge mechanism in games, can work together to satisfy these psychological needs. At the same time, Flow theory suggests that this immersion and feedback mechanism contributes to increased focus and learning outcomes. 28 Therefore, Mammoverse may provide stronger behavioural engagement and knowledge retention through an immersive, task-oriented learning process than traditional one-way educational tools such as lectures and brochures. Therefore, this study takes Self-Determination Theory (SDT) and Flow Theory as the core theoretical foundation to explore in depth how the platform can stimulate learning motivation and enhance the learning experience by satisfying users’ psychological needs, thereby promoting behavioural transformation.
The objectives of this study include: (1) To evaluate the immediate and short-term effects of the Mammoverse platform on improving young women's breast health knowledge. (2) Explore how key design elements in the platform influence users’ motivation, behavioural intentions and potential behavioural change pathways.
This study will provide theoretical support and a practical basis for the design and promotion of digital health education tools in the future, and promote the continuous innovation of breast health education.
Methods
Study design
This study used Explanatory Sequential Mixed Methods (ESM) and followed the Reporting Specifications for Mixed Methods Studies (GRAMMS), combining experimental and semi-structured interviews, in order to comprehensively assess the metaverse-based gamified healthcare app ‘Mammoverse’ to improve breast health literacy and explore users’ motivations, behavioural intentions and potential behavioural change intentions. 29 While a single quantitative measure can assess changes in knowledge levels before and after an intervention, it is difficult to reveal deeper psychological and behavioural factors such as users’ subjective acceptance of the platform, their interaction experience and their motivation to behave. Therefore, this study was designed with a sequential design that centred on quantitative assessment first, followed by qualitative use to interpret and complement the quantitative results, and combined questionnaire assessment with semi-structured interviews to achieve complementary interpretation and a deeper understanding of the results.
The study was divided into five phases: Pre-test, Intervention, Post-test, Interview, and final test after 4 weeks, as shown in Fig. 1.

Methodological design of the study (authors’ own drawing).
Mammoverse
This study developed a mobile metaverse medical education application called ‘Mammoverse’. The research team used Epicd and Unreal Engine version 5.4.4 professional tools to build a metaverse-based breast health education and health promotion platform. The platform is designed with 3D interactive games and is dedicated to providing users with breast health knowledge, guidance on breast self-examination methods and breast health education in order to enhance their knowledge of breast health and promote their self-health management ability. In order to facilitate more in-depth exploration and research in the future, the platform has specially adopted the bilingual mode.
Prior to the development of the platform, the researchers conducted a small-scale user preference survey to gain an initial understanding of the target users’ interest in the content, digital learning formats and interactive features of the breast health platform. While this survey was not included in the formal research analysis, the results informed the initial planning of the content structure and functional modules of the platform.
Figure 2 shows the specific interface and interaction scenarios of the Mammoverse breast health education platform developed in this study. (A) shows the main interface of the platform, where users can visualise the clinic environment and interaction options; (B) shows a 3D virtual character entering the platform clinic and receiving initial guidance from a virtual nurse; (C) shows the backstory of the platform and the introduction of the tasks to enhance the user's sense of immersion and engagement through narrative scenarios; and (D) displays virtual voice prompts from the future to give the user clear instructions about the tasks and operations; (E) Users discover hidden pieces of breast health knowledge through exploration to enhance interaction and knowledge internalisation; (F-H) are dialogue interactions between users and virtual patients, which enhance understanding of the patient's perspective through real-scene-style situational dialogues; (I) Users learn standardised breast self-examination techniques under the guidance of a virtual doctor; (J) Knowledge review sessions help users consolidate what they have learned; (K) is the final stage of the quiz challenge, which examines the user's knowledge mastery and provides immediate feedback. These modules are based on an immersive 3D environment and effectively reinforce users’ breast health knowledge and practical skills through task-oriented interactions.

Interface scenarios for the Mammoverse platform.
Users enter Mammoverse and embark on an interactive learning process in the form of an immersive virtual experience. The platform's scenario is set in the future, in the year 2074, where the participant will take on the role of an ordinary young person who receives a virtual phone call alerting him or her to an emergency situation of a high incidence of breast cancer in his or her environment. In order to change this future, the user returns to a 2025 medical virtual scenario to systematically learn breast health knowledge and skills. The learning process is centred around four core tasks: ① familiarise themselves with the virtual clinic environment; ② explore and learn hidden breast health knowledge points; ③ talk with virtual patients to gain a deeper understanding of health issues from the patient's perspective; and ④ interact with a virtual doctor to master standardised breast self-examination skills. Users control the character movement by keyboard (W, A, S, and D keys) and mouse, and use the E key for interaction and task operation. Upon completion of the task, the user is rewarded with points, the accumulation of which will determine the final virtual reward the user receives.
Through the combination of virtual character interaction, real scene simulation, and knowledge assessment, the platform encourages users to master breast health knowledge naturally in a strong sense of reality in the virtual experience. In the final quiz-based challenge, those who reach an accuracy rate of 80% or more will be awarded the title of ‘Self-examination Master’ to continuously motivate users to pay attention to and practice breast health behaviours in the long run.
Sampling
This study drew upon sample sizes established in recent mixed-methods health education research.30–32 Considering the exploratory nature of the study and resource constraints, the target sample size was ultimately set at 40 participants. Through a combination of snowball sampling and convenience sampling, 40 adult women were recruited. Among them, 36 successfully completed all study procedures and were included in the analysis. The remaining four participants were excluded due to personal schedule conflicts that prevented them from completing the post-test and interview. The qualitative and quantitative samples were identical, all 36 participants who completed T2 subsequently underwent semi-structured interviews.
All participants completed the study online via the social media platform ‘Xiaohongshu’. The research team posted recruitment posters and registration instructions on the platform, explaining the study objectives, participation criteria, and process arrangements. Volunteers who wished to participate in the study contacted the researchers via private message on WeChat and filled out a registration form, providing their contact information and available participation times. Researchers encouraged participants to share recruitment information with friends and family to expand the study population. The research process strictly followed the experimental design, with only those who completed the pre-test questionnaire receiving access to the platform experience link, post-test questionnaire, and Tencent Meeting interview invitation.
The study participants were adult women of Chinese nationality from various regions, with no geographical restrictions. Participants came from multiple provinces, possessed basic digital operation skills, and were interested in breast health education. They represented a broad general population rather than a specific community sample. Inclusion criteria include being at least 18 years old, having the ability to operate a smartphone or computer, and being able to complete the online and offline experimental processes smoothly. Exclusion criteria include device incompatibility, network latency, or discomfort with 3D virtual scenes, among other practical obstacles that may arise during the process. To enhance participation motivation, all participants who completed the entire research process received a subsidy of 20 Chinese yuan (approximately 2.8 USD).
Instrument
The quantitative questionnaire comprises two sections: sociodemographic statistics and a breast health knowledge questionnaire. Sociodemographic variables include age, educational attainment, family history of breast cancer, and prior breast health education or training – a total of four questions – described using frequency counts and percentages. The Breast Health Literacy Questionnaire was adapted from a survey instrument developed by McCance et al. to measure knowledge about breast cancer screening and detection. 33 The format and content of the questionnaire were modified by changing the questionnaire from judgmental and multiple-choice to multiple-choice, and by summarising the content of the questionnaire, the 18 items were adapted into three sections: 6 items on breast cancer risk factors and screening, 10 items on breast self-examination techniques, and 2 items on abnormal breast changes and symptoms. Each question was scored 1 point for correct answers and 0 points for errors, with a total score range of 0–18. The total number of correct questions was entered into SPSS as raw data for statistical analyses, which were used to compare changes in knowledge before and after the intervention.
To ensure content validity, one public health expert and one breast cancer expert were invited to review and revise the questions to ensure the relevance and professionalism of the questionnaire content. Additionally, a pre-test was conducted with five volunteers from the target population to assess the questionnaire's surface validity, clarity, and understandability. Since this questionnaire consists of objective knowledge test questions covering multiple independent knowledge points, Cronbach's α coefficient was not used to assess internal consistency.
The interview outline was designed to synthesise the Extended Technology Acceptance Model (UTAUT), the Health Belief Model (HBM), and Gamified Learning Theory (GBL).34–37 The interview questions focused on five main areas: basic user profile and breast health knowledge base, user feedback on the technical ease of use and overall experience of the platform, user experience and evaluation of specific gamification elements, specific user feedback on knowledge acquisition, motivation enhancement, and behavioural transformation, and specific user suggestions for optimisation of the platform.
Data collection
Participant recruitment for the data collection phase was completed in December 2024. The formal data collection process for the study was divided into two stages. The first stage, which included a knowledge assessment, platform experience evaluation, and semi-structured interviews on the day of the intervention, was completed by the end of February 2025. The second stage, which involved a delayed knowledge assessment four weeks after the intervention, was fully completed by the end of March 2025.
The collection of quantitative data comprised three phases. During Phase T1, all participants completed a breast health knowledge questionnaire to assess their baseline knowledge prior to the intervention. Subsequently, participants used their personal laptops to experience the Mammoverse platform in a quiet indoor environment of their choice, as illustrated in Figure 3. The platform access link was single-use only, permitting a single experience to prevent repeated exposure from influencing intervention outcomes. Prior to intervention implementation, all participants received platform operation instructions, including brief verbal guidance from researchers and written explanations when necessary, to ensure consistent operational starting points. The intervention duration was limited to under 20 minutes, based on pre-intervention testing time estimates. Most participants reported this duration as reasonable, allowing task completion without undue burden. Immediately after the intervention, participants completed the same knowledge questionnaire as the pre-test (T2) to assess immediate knowledge enhancement. Finally, four weeks after the intervention concluded (T3), all participants completed the same questionnaire online to evaluate knowledge retention. The entire intervention process was supervised by researchers, with technical support provided only when necessary to ensure consistency. Three technical assistance incidents occurred during the study, such as login anomalies and slow scene loading, all were attributable to individual network instability. These were promptly addressed and did not impact data quality or the research process.

Participants take the test.
Qualitative data were collected through semi-structured interviews conducted by the first author via Tencent Meeting with all participants after they had completed the T2 knowledge questionnaire. Each interview lasted approximately 15–20 minutes. The interviews centred on three core topics: (1) experiences using gamified elements within the platform. (2) feedback on knowledge acquisition and comprehension. (3) perceptions regarding willingness to adopt breast health-related behavioural changes. With consent obtained, all interviews were audio-recorded for subsequent analysis.
Data analysis
This study employed SPSS 28.0 (IBM Corporation) for quantitative data analysis. Sociodemographic variables were described using frequencies and percentages. For the knowledge measurement section, the Shapiro-Wilk test was first conducted to assess data normality and determine the appropriate statistical test method. If the data satisfies normal distribution, it was analysed by repeated measures ANOVA; if the data deviates from normal distribution, the differences in knowledge assessment results at different time points were analysed by nonparametric Friedman's test, and the Wilcoxon signed rank test with Bonferroni correction will be used for multiple comparisons. Multiple comparisons were performed. The statistical significance level was set at P < 0.05. This study is exploratory in nature and does not quantitatively control for potential confounding factors. However, these factors are discussed in the discussion section as limitations of the study, and it is recommended that future studies further incorporate relevant variables to enhance the rigour of causal inference.
Qualitative data analysis employed the six-step thematic analysis method proposed by Braun and Clarke (2006). 38 The analysis phase utilised a deductive thematic analysis strategy, employing theoretical concepts such as the UTAUT, HBM, and GBL as the initial coding framework. NVivo software was utilised for coding and thematic induction. All interview recordings were transcribed verbatim by researchers. Qualitative coding was performed by one researcher and conducted in two rounds of independent coding at different times. Consistency was verified, and the coding framework was optimised by comparing the results of the two rounds. No new concepts or themes emerged during the analysis of interviews with participants 23 and 24, indicating that the study had reached theoretical saturation, and the sample size was sufficient within the scope of the current research objectives. Qualitative analysis aimed to gain a deeper understanding of users’ authentic experiences and feedback regarding learning motivation, knowledge acquisition, and behavioural transformation.
After completing both quantitative and qualitative analyses, this study integrated the two types of data through parallel presentation and cross-interpretation during the results interpretation phase, conducted by the first author. The trends in knowledge assessment scores across three evaluations were compared and cross-validated against themes extracted from the interviews, thereby establishing a connection between the objective measurement of knowledge changes and users’ subjective experiences.
Results
Quantitative results
Table 1 details the demographic characteristics of the participants. A total of 40 adult females were recruited for this study, of which 36 completed all measurements and were included in the final analysis. The age of the participants was concentrated between 20 and 30 years old (80.56%); the educational background was predominantly undergraduate (61.11%) and graduate (33.33%). The vast majority of participants had no family history of breast cancer (86.11%), and 77.78% had no prior training or education related to breast health.
Demographic characteristics of the participants.

In order to determine the statistical analysis of the data, the data from the three measurement phases were first tested for normality. The results of the Shapiro–Wilk test showed that the data from the pre-measurement were normally distributed (P = 0.259), whereas the data from the post-measurement (P < 0.001) and the data from the 4-week post-intervention period (P = 0.010) deviated significantly from a normal distribution, and therefore, subsequent non-parametric tests were used.
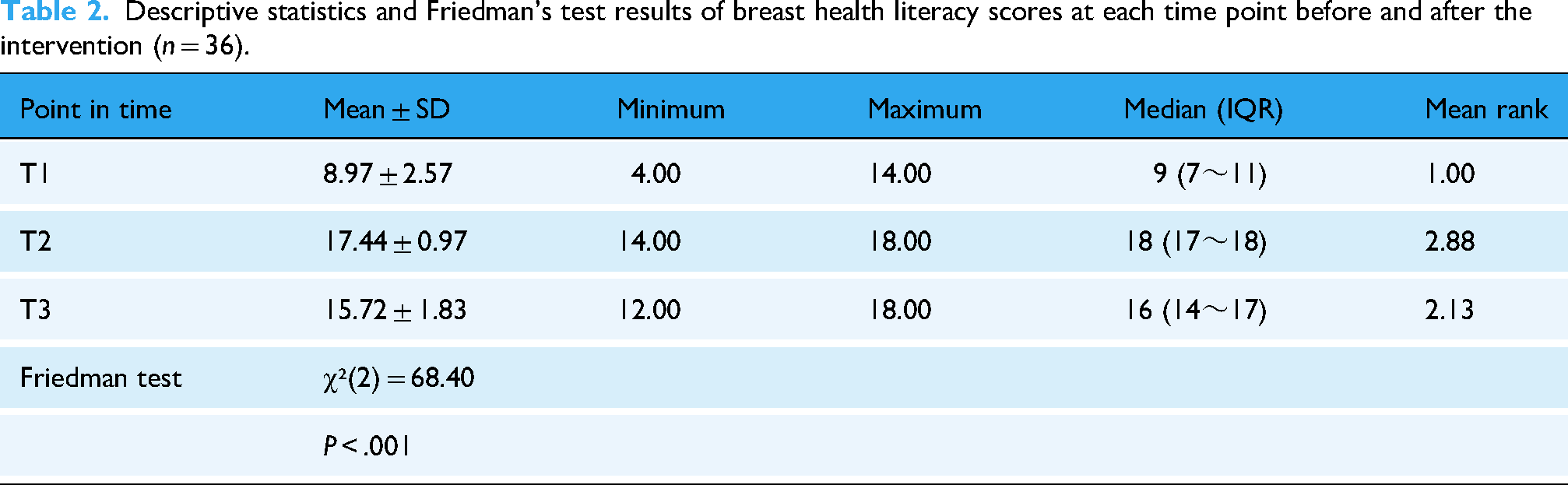
Table 2 demonstrates the results of descriptive statistical analysis of participants’ breast health knowledge scores at three stages: pre-intervention (T1), immediate post-intervention (T2), and 4 weeks post-intervention (T3). Friedman's test showed that the difference between the three measurement time points was statistically significant (χ²(2) = 68.40, P < 0.001). In terms of mean rank values, the immediate post-intervention measure (T2) had the highest score (mean rank = 2.88), the measure 4 weeks later (T3) had the second highest (mean rank = 2.13), and the pre-intervention score was the lowest (T1, mean rank = 1.00).
Descriptive statistics and Friedman's test results of breast health literacy scores at each time point before and after the intervention (n = 36).
As shown in Fig.4, there was a significant trend in knowledge levels at the three measurement stages.T1 represents the pre-intervention measurement, T2 represents the immediate post-intervention measurement, and T3 represents the 4-week post-intervention measurement. The line graph visualises the trend of participants’ mean and median breast health knowledge scores before and after using the Mammoverse platform, with a significant increase in knowledge scores in the immediate post-intervention period (T2) and a slight but still high level of knowledge scores in the 4-week post-intervention period (T3).

Line graph of trends in mean and median breast health knowledge scores by measurement stage.
To further clarify the specific differences in performance at each measurement stage, the study used the Wilcoxon signed rank test for two-by-two comparisons with Bonferroni correction for significance level (α = 0.0167). As shown in Table 3, the two-by-two comparisons between the measurement phases reached the level of significance (all P < 0.001), as shown in the following: scores were significantly higher in the immediate post-intervention period (T2) than in the pre-intervention period (T1) and 4 weeks after the intervention (T3), and scores were significantly higher in the 4-week post-intervention period (T1) than in the pre-intervention period (T1).
Wilcoxon signed rank test two-by-two comparison results for breast health knowledge scores (n = 36).

Significance values have been adjusted by the Bonferroni correction for positive pairwise multinomial tests.
Quanlitative results
Overview of themes
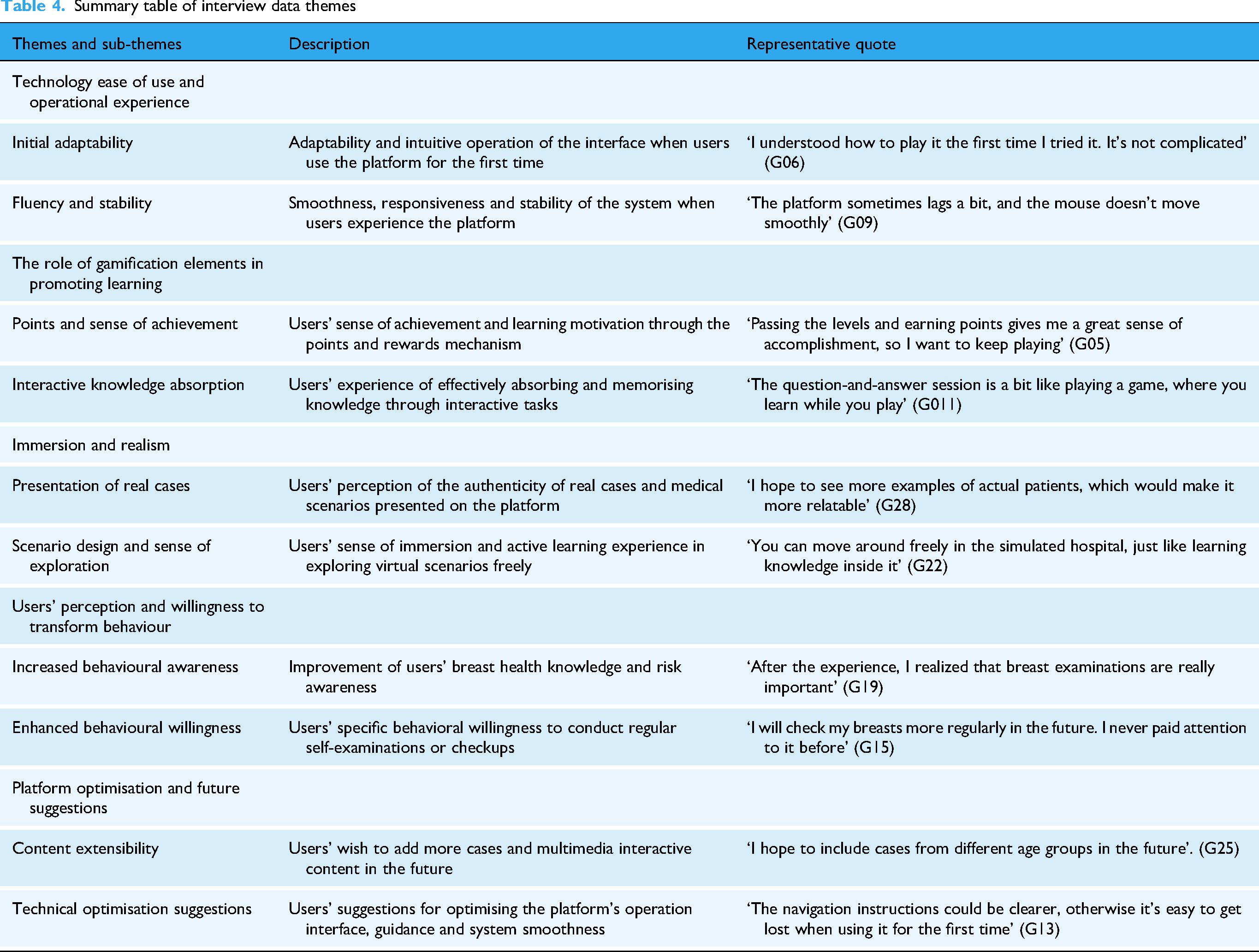
Analysis of the interview data revealed five core themes, each of which contained several sub-themes, as shown in Table 4. Theme 1, ‘Technology Ease of Use and Operational Experience’, contains two sub-themes: ‘Initial Adaptability’ and ‘Fluency and Stability’. Users generally agreed that the platform was easy to use and the interface was friendly, but they also suggested that some functions were difficult to operate when they first encountered them. Theme 2 was ‘The role of gamification elements in promoting learning’, with two sub-themes: ‘Points and sense of achievement’ and ‘Interactive knowledge absorption’. Participants believed that points and rewards significantly increased motivation to learn, while interactive tasks designed by the platform further deepened users’ understanding and memorisation of knowledge. Theme 3 is about ‘Immersion and realism’, which includes two sub-themes: ‘presentation of real cases’ and ‘scenario design and sense of exploration’. Users pointed out that the design of real-life scenarios in the platform effectively enhanced the sense of immersion and interest in participation, and improved the overall learning experience. Theme 4, ‘Users’ Perception and Willingness to Transform Behaviour’, explored the aspects of ‘Increased Behavioural Awareness’ and ‘Enhanced Behavioural Willingness’. Most of the users showed a high awareness of breast health and a clear willingness to conduct self-examination or regular checkups after the experience. Theme 5 is ‘Platform Optimisation and Future Suggestions’, which consists of two sub-themes: ‘Content Extensibility’ and ‘Technical Optimisation Suggestions’. Respondents suggested that more real-life cases and multimedia interactive elements could be added to the platform in the future and that clearer and more detailed guidance should be provided on the operation of the technology in order to optimise the overall user experience.
Summary table of interview data themes
Theme 1:Technology ease of use and operating experience
This theme has two sub-themes: ‘Initial Adaptation’ and ‘Fluency and Stability’. The majority of participants reported that they were able to adapt quickly when using the Mammoverse platform for the first time and that the interface design was intuitive and user-friendly. However, some users pointed out that there were operational difficulties during their first experience, for example: ‘I was not familiar with the way of moving the viewpoint for the first time and it took me some time to get used to it’ (G07), ‘I was not very good at operating the interface in the beginning, and it was not clear to me that the mouse was for controlling the viewpoint, and the keyboard keys were for controlling the walking. Keys are to control walking, these are not prompted, which made me confused initially’ (G02); some users also said, ‘When my mouse points inside that screen, the perspective will follow the mouse to rotate, and it rotates very fast, the mouse sensitivity is too high, and it's not very convenient to operate the character’ (G05).
In addition, in terms of smoothness and stability, users also gave feedback on some specific issues, such as ‘the overall use is quite smooth, but occasionally in the interactive process of the interface response delay or lag, I hope that the platform in the stability of further optimisation’ (G11), ‘the platform experience occasionally lags, sometimes the network connection is not stable, and the operation experience is not very smooth’ (G10). Participants also pointed out that ‘the font size of some operation prompts is too small, such as the prompt to press E or F to interact, which are not eye-catching enough and not easy to be noticed’ (G02).
In summary, although most participants were able to master the basic operation of the platform relatively quickly, there is still room for further optimisation of the platform in terms of operation guidance for first-time use, interface response sensitivity, and smoothness to enhance the overall user experience.
Theme 2:The role of gamification elements in promoting learning
Sub-themes under this theme include: ‘Points and fulfilment’ and ‘Interactive knowledge absorption’. Many users reported that the points and rewards system significantly increased motivation and engagement. For example, one user noted, ‘Getting points and honours makes me feel like I am constantly accomplishing something and willing to continue to learn more’ (G14), while another user elaborated, ‘I was particularly impressed by the point system at the end, and seeing my score increase little by little from 0 to close to 100 gave me a sense of accomplishment and motivated me to seriously participate in the learning process. I felt a sense of accomplishment, which motivated me to seriously participate in the learning process’ (G01). At the same time, some users also emphasised that the sense of achievement brought by the points helped to focus their attention: ‘When answering the questions, knowing that you can get points after answering correctly, you want to participate as seriously as possible and don’t want to make mistakes’ (G02).
In addition, the platform's interactive task design received positive feedback from participants. One user noted, ‘I remembered a lot of key knowledge points by interacting with the virtual characters, which is more vivid and interesting than the traditional learning method’ (G21); another user specifically mentioned, ‘In the interactive quiz session, since I knew there would be a test later on, I was more conscious of remembering every knowledge point’ (G02). Another user stated, ‘Interactive conversations with patients or doctors make me feel like I am listening to a real story, and this format is more likely to stimulate interest and make it easier to remember knowledge points’ (G14). These user feedbacks show that the interactive design of gamification significantly promotes knowledge absorption and memorisation effects.
In summary, the gamification element not only enhances users’ motivation and intrinsic motivation to participate but also effectively enhances users’ understanding and memorisation effect of breast health knowledge through the interactive learning format.
Theme 3:Immersion and realism
This theme includes two sub-themes: ‘Presentation of real cases’ and ‘Scenario design and sense of exploration’. Users generally commented that the real-life scenarios and cases designed by the platform made them feel closer to real medical situations and enhanced the effect of knowledge absorption. One user said, ‘The cases displayed in the platform are very real as if I am talking to the patients, which is very impressive’ (G09); another user further described, ‘What attracts me the most is the patient finder session, where I can learn about my cases from the patients, and I have the feeling of listening to a story, which is more appealing to me’ (G09). ‘It attracted me more’ (G14). Another user stated, ‘The doctor–patient interaction made me feel closer to reality and left a deep impression on me, it felt like I was consulting a doctor’ (G16).
In addition, the exploratory learning approach was also recognised by users, for example, ‘The free exploration function in the platform makes me feel more active and interested in exploring and learning’ (G17); another user mentioned, ‘Exploring the hidden knowledge fragments is particularly interesting, like playing a real puzzle solving game, it is easy to stimulate curiosity and motivation to learn’ (G06). Some users also emphasised the authenticity and sense of immersion in the context during the exploration process: ‘The whole scene design makes me feel novel, like learning in a real medical environment, with a particularly strong sense of immersion’ (G08); and another user pointed out that, ‘The design of the scenes and wards is very realistic, making me feel that I am really in a hospital situation, and this design is particularly effective in increasing my interest in learning’ (G11).
In summary, the platform's highly realistic case presentation and exploratory interactive learning mode not only effectively enhanced users’ sense of immersion and realism, but also significantly enhanced their understanding and memorisation of breast health knowledge.
Theme 4:Users’ perception and willingness to transform behaviour
This theme explored both ‘increased behavioural awareness’ and ‘increased behavioural willingness’. The vast majority of participants indicated that their awareness of breast health and the importance they attached to it had increased significantly after experiencing the platform. For example, one participant said, ‘After the experience, I deeply realised the importance of self-examination and will pay more attention to breast health in the future’ (G19). Another user specifically mentioned, ‘After learning through the platform, I now clearly know that I should self-examine once a month, and I also know how to self-examine correctly, such as using the pads of my fingers instead of the tips, which I had not noticed at all before’ (G26). Participants also expressed a significant increase in alertness to the potential risk of breast cancer: ‘Now I will pay a lot of attention to information about breast health before I thought I didn’t need to pay attention to it because of my age, but now I realise that it is necessary for young people as well’ (G22).
At the same time, many users showed a clear shift in behavioural intention. One participant mentioned, ‘Now I have a clear plan to check myself every month’ (G22). Another participant emphasised, ‘The learning experience of the platform directly contributed to my decision to perform regular breast self-examinations every month in the future because knowing this knowledge, I felt that self-examinations were not complicated and I could easily do them myself’ (G02). Another user noted, ‘After using this platform, I am not only willing to perform regular self-examinations but also intend to go to the hospital for professional breast screening afterwards because the experience made me realise the importance of early screening’ (G05).
In summary, participant feedback indicates that the gamified metaverse education platform not only effectively enhanced breast health knowledge but also directly increased users’ attention to breast health issues and prompted a clear willingness for behavioural transformation.
Theme 5:Platform optimisation and future suggestions
Under this theme, users suggested improvements in two aspects: ‘content scalability’ and ‘technical optimisation suggestions’. First, in terms of content scalability, respondents hoped that the platform could provide more real cases and multimedia interactive content in the future to meet the learning needs of different users. For example, the user suggested, ‘It is recommended to add more breast health cases of different age groups and more interactive videos to better meet the needs of different users’ (G25); another user said, ‘It is possible to design a few more cases with more patients, such as women in their twenties, thirties, and forties. Women over the age of 40, and the design of cases for different age groups can better target different groups of people’ (G15). Another user pointed out, ‘In addition to the current case content, more actual clinical pictures or video cases can be added so that I can more clearly understand the difference between normal and abnormal breasts’ (G01).
Second, in terms of technical optimisation, users made some specific suggestions to improve the ease of use and smoothness of the platform. One user suggested, ‘The platform interaction prompts can be more detailed, such as adding obvious navigation arrows to improve the initial experience of new users’ (G05); another user reflected, ‘Sometimes the platform response is slightly slow, and occasional lagging occurs, so I hope that further optimisation can be done technically, especially for the view angle It is hoped that further technical optimisation can be made, especially in terms of the sensitivity of movement’ (G10). In addition, some users suggested improving the intuitiveness and simplicity of the interactive interface: ‘The operation interface can be designed to be more simple and intuitive, and reduce complex operations, which is especially important for first-time users’ (G09).
In summary, user feedback clearly points the way forward for the platform's future optimisation, particularly highlighting the need for further improvements in operational guidance and system stability at the technical level. It is worth noting that these opinions are primarily based on participants’ one-time usage experiences, meaning their feedback is to some extent limited by the nature of a ‘single-session experience’. Nevertheless, it still provides valuable reference for the platform's future development and application.
Integration of findings
By integrating quantitative and qualitative findings, this study further elucidates the underlying mechanisms of learning motivation, user experience, and behavioural change intentions based on knowledge change trajectories. Figure 5 illustrates the trends in knowledge assessments across T1, T2, and T3, corresponding to five core themes extracted from user interviews to comprehensively demonstrate intervention effects.
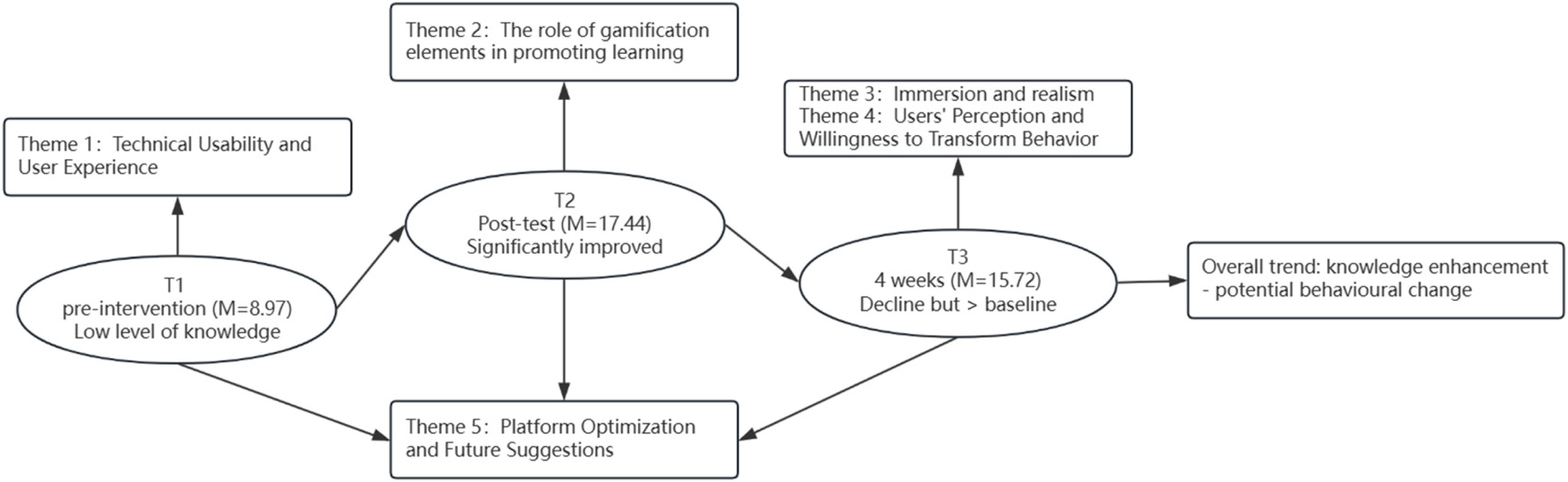
Integrated framework of quantitative results and qualitative themes.
At T1, participants exhibited generally low breast health knowledge levels (M = 8.97). Qualitative findings indicated that users frequently encountered issues such as insufficient operational guidance and difficulties adapting to perspective control during initial use (Theme 1), which contributed to heightened learning barriers at baseline.
By T2, knowledge levels significantly improved (M = 17.44, P < 0.001), with T2 scores significantly higher than both T1 and T3 in pairwise comparisons. This immediate gain was closely linked to the sense of accomplishment from the points-based reward system and the heightened focus stimulated by interactive tasks, as mentioned in user feedback (Theme 2).
During T3, knowledge levels declined slightly from T2 (M = 15.72) but remained significantly higher than baseline. Interview findings indicate that immersive scenarios and real-world case studies partially delayed forgetting (Theme 3). More importantly, users demonstrated markedly enhanced health awareness and positive behavioural intent (Theme 4), such as recognising the importance of regular self-examination and expressing willingness to seek further medical checkups. This indicates that short-term fluctuations in knowledge retention did not diminish the intervention's core value, but rather facilitated positive behavioural transformation.
Notably, some individuals achieved suboptimal learning outcomes. Interview findings suggest this may relate to insufficient operational prompts, suboptimal interaction fluidity (Theme 1), and relatively limited case content (Theme 5). This feedback not only explains individual variations but also provides concrete pathways for platform improvement.
Discussion
Summary of key findings
This study is the first to evaluate the actual effectiveness of a breast health education platform (Mammoverse) that integrates metaverse and gamification technologies in improving women's breast health knowledge and motivation. The study found that after participating in the platform intervention, participants’ breast health knowledge levels significantly improved both immediately and in the short term, which is consistent with existing research showing that digital interactive educational methods can effectively improve health knowledge.39,40
Qualitative interview results further indicate that users generally hold positive attitudes toward the platform's interactive experience and gamification mechanisms, particularly in terms of immersion, interactivity, and learning motivation. This aligns closely with existing research emphasising the critical influence of immersion and interaction on digital health education.41–43 The Mammoverse platform significantly enhances users’ intrinsic motivation through gamified elements such as points rewards, task-driven activities, and immediate feedback, aligning with the three psychological needs of autonomy, competence, and relatedness outlined in Self-Determination Theory (SDT). 44 Additionally, its clear objectives and timely feedback help users enter a state of deep focus known as the ‘flow state’, which aligns with Flow Theory. Flow theory also emphasises that when a learning environment features clear goals, immediate feedback, and appropriate challenges, it can facilitate individuals entering a state of deep focus known as ‘flow’, thereby enhancing learning efficiency and knowledge retention. 45 Compared to traditional one-way educational methods such as lectures or promotional brochures, Mammoverse enhances engagement and experiential learning by guiding users to actively explore and interact. This gamified learning model not only facilitates knowledge understanding and retention but may also encourage users to develop positive, healthy behavioural intentions.
From a behavioural change perspective, the interview results showed that the platform not only significantly improved users’ knowledge levels but also increased their willingness to perform regular breast self-examinations. This finding contrasts with some digital education studies that remain at the knowledge level, emphasising the need to consider the ‘knowledge-motivation-behaviour’ pathway as a comprehensive intervention strategy.46,47 This further underscores the importance of focusing on long-term behavioural change rather than merely short-term knowledge enhancement in breast health education.
Previous studies have independently validated the effects of the metaverse and gamification technology in health education. The findings of this study are consistent with previous research on the metaverse and gamification in health education. In terms of immersive educational technology, Wei and Yuan (2023) noted that in the field of health education, immersive virtual reality (IVR) can effectively enhance focus and knowledge retention. 44 Luai et al. (2024) further confirmed that VR and AR not only help improve knowledge levels and behavioural performance but also effectively reduce learning anxiety. 48 The ‘Dr Meta’ metaverse cancer care platform developed by S. Kim et al. enhanced patient engagement and telemedicine experiences, 49 while Gouveia et al. validated the promotional effect of augmented reality (AR) technology on spatial understanding in breast surgery education. 50
In the field of gamified education, multiple empirical studies have supported its effectiveness in enhancing learning interest and motivation. Haruna (2024) significantly improved adolescents’ knowledge and attitudes toward healthy sexual behaviour through the ‘My Future Begins Today’ platform. 51 Yusoff et al. developed ‘CytoUniverse’, which uses real-time feedback mechanisms to enhance students’ knowledge absorption and engagement in cytology, 40 while Tzioutzios et al. (2024) demonstrated the effectiveness of immersive teaching in improving the public's understanding and response capabilities regarding natural disaster risks through the ‘EGNARIA’ project. 52
Further research has also explored the integration of gamification with virtual reality technology in various health education settings, yielding positive outcomes. Joy et al. (2024) developed a desktop-based gamified module titled ‘Kidney Treasure’, which, although it did not significantly improve test scores, significantly enhanced students’ satisfaction with the learning content, indicating that interactive educational formats possess high perceived value. 53 Kim et al. (2024) constructed a clinical simulation course integrating VR technology, effectively enhancing nursing students’ clinical reasoning abilities and engagement. 54 Han et al. (2023) developed a biomedical laboratory platform using Unity 3D, improving students’ learning efficiency and knowledge retention. 55 Tran et al. (2025) designed the neuroanatomy serious game ‘BrainSpace’, which significantly enhanced students’ spatial understanding and self-efficacy. 56 Demircan and Kaya (2025) found that gamified instruction significantly improved students’ learning confidence and satisfaction in nursing skill training. 57 These studies collectively validate the broad applicability of gamified metaverse environments in health education and support the theoretical model and empirical findings of this study from various perspectives, providing a solid empirical foundation and research direction for future studies.
It is worth emphasising that the mixed-methods design of this study not only validated the effectiveness of the Mammoverse platform in enhancing knowledge and motivation but also revealed additional findings that would be difficult to capture using a single approach. Quantitative data objectively reflects improvements and trends in knowledge levels, while qualitative data delves into underlying mechanisms (how gamification elements and immersive experiences stimulate learning motivation), challenges in long-term retention (partial knowledge decline after four weeks), and the process of translating cognitive gains into behavioural intent (increased willingness for regular self-examination). By integrating both data types, this study further unravels the complete ‘knowledge-motivation-potential behaviour’ chain. This integrated analysis not only deepens our understanding of intervention effectiveness but also provides a more robust theoretical foundation and practical insights for designing and optimising future breast health education interventions. It further points to directions worthy of further validation in subsequent research.
Limitations and future work
Although this study has achieved some positive results, there are still several limitations that require further discussion and reflection. First, the sample size is relatively small, and the participants are mainly young, highly educated women, which may affect the representativeness and external generalisability of the study results. To improve the universality and adaptability of the intervention, future studies should expand the sample scope to include a wider range of age groups and educational backgrounds. Additionally, the platform currently supports both Chinese and English interfaces to enhance accessibility for users with different language backgrounds. Future versions could explore more language adaptation mechanisms to enhance its scalability in multicultural contexts.
During the platform design phase, the study preliminarily considered variations in users’ health literacy and digital literacy, enhancing the platform's comprehensibility and usability through simplified terminology, visual guidance, and scenario-based tasks. Furthermore, although this study included a knowledge retention assessment 4 weeks post-intervention, it did not incorporate quantitative evaluations of participants’ actual completion of breast self-examination or medical consultations. Consequently, it falls short in presenting a complete ‘knowledge-motivation-behaviour’ conversion pathway. Simultaneously, due to the sequential mixed-methods design, recruitment for qualitative interviews relied entirely on participants who completed quantitative assessments, limiting both sample size and diversity. While the quantitative component reflected trends in knowledge levels, it did not directly capture behavioural indicators like breast self-examination. Consequently, interpreting the knowledge-to-behaviour conversion pathway required supplementation from qualitative interview findings. Future research should consider incorporating more direct behavioural implementation indicators in the quantitative phase and expanding the sample scope. Simultaneously, adopting more flexible sampling methods in the qualitative phase could enhance the generalizability of results while maintaining interpretive depth.
Regarding user experience, while most respondents provided positive feedback on the platform's immersive experience and content design, some users reported issues such as insufficient guidance and unintuitive interaction logic during initial use. In certain scenarios, minor lag or delay phenomena also occurred, which aligns with the technical challenges commonly reported in existing literature on VR-based health education platforms.46,51,52,58–61 It should be noted that the current version's mouse movement sensitivity is a platform default setting and does not currently support user-defined adjustments. This issue has been included in the subsequent optimisation plan. Therefore, future technical iterations should further optimise interface guidance, interaction fluidity, and system stability to enhance user-friendliness during initial use and increase the likelihood of long-term continued use. Additionally, user interview feedback indicated that the current platform's limitation to single-session experiences is restrictive. Some participants expressed a desire to be able to re-enter the platform as needed or independently select modules for review. Future versions may consider introducing modular design and multiple access mechanisms to support personalised learning paths and long-term behaviour maintenance.
From a promotional perspective, although the platform is built on an open-source engine, which offers some cost control and platform compatibility, issues such as hardware configuration differences, unstable network quality, and insufficient digital skills among users may still pose practical challenges to the widespread implementation of the intervention. Therefore, during future technical expansion, it is necessary to further optimise the platform's accessibility threshold based on user group characteristics, while conducting usability testing and multi-device compatibility design, such as mobile WeChat mini-programs, tablets, Switch, and VR, to enhance the fairness and accessibility of the intervention tool. Looking ahead, it is recommended to further explore the integration of the platform with artificial intelligence technology and social interaction elements to enhance personalised educational outcomes and user engagement. Additionally, intervention evaluations should incorporate multi-dimensional long-term behavioural tracking and mechanism analysis to deeply reveal the effectiveness and feasibility of the integration of the metaverse and gamification in various health education scenarios.
In summary, this study not only preliminarily validated the feasibility and effectiveness of gamified metaverse platforms in the field of breast health education but also provided a theoretical foundation and practical reference for the design optimisation and empirical pathways of future digital health intervention tools. Future research should continue to deepen in areas such as expanding audience coverage, optimising technical support, and improving evaluation systems to drive innovative practices in breast health education and the sustained transformation of behavioural change.
Conclusion
This study employed an ESM approach to systematically evaluate the effectiveness of the gamified metaverse platform (Mammoverse) in enhancing women's breast health knowledge and stimulating learning motivation. Results indicate that immersive interactive experiences combined with gamified design significantly boost learning motivation and knowledge acquisition while fostering positive behavioural intentions, demonstrating superiority over traditional health education methods.
The innovation lies in the pioneering integration of the metaverse and gamification for breast health education, empirically validating their synergistic effects across the ‘knowledge-motivation-potential behaviour’ chain. By presenting objective knowledge measurements alongside subjective user experiences through parallel presentation and cross-explanation, the study elucidates at the mechanism level how immersion and incentives drive learning and behavioural intentions. It also proposes concrete optimisation directions from a practical perspective, such as interface guidance, interaction fluidity, and content expansion, providing actionable design and iteration guidelines for digital health education tools in breast health and other scenarios.
However, this study has certain limitations, such as a small sample size, a short follow-up period, and the absence of objective behavioural metrics in the quantitative analysis. Future research is recommended in three areas: First, consider expanding the sample size and conducting cross-cultural comparisons. Second, implementing longer-term follow-ups incorporating objective behavioural data could assess the platform's sustained impact on knowledge retention and health behaviours over time. Third, exploring the integration of gamified metaverse platforms with advanced technologies like artificial intelligence and social networks represents a significant and promising research direction. Overall, Mammoverse offers a replicable and scalable pathway for the digital transformation of breast health education, demonstrating potential for broader adoption across diverse populations and settings.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251390466 - Supplemental material for A gamified metaverse platform (Mammoverse) for breast health education: A mixed-methods study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251390466 for A gamified metaverse platform (Mammoverse) for breast health education: A mixed-methods study by Rui Li, Seng Yue Wong, Bingyu Duan and Sabzali Musa Kahn in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251390466 - Supplemental material for A gamified metaverse platform (Mammoverse) for breast health education: A mixed-methods study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251390466 for A gamified metaverse platform (Mammoverse) for breast health education: A mixed-methods study by Rui Li, Seng Yue Wong, Bingyu Duan and Sabzali Musa Kahn in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251390466 - Supplemental material for A gamified metaverse platform (Mammoverse) for breast health education: A mixed-methods study
Supplemental material, sj-docx-3-dhj-10.1177_20552076251390466 for A gamified metaverse platform (Mammoverse) for breast health education: A mixed-methods study by Rui Li, Seng Yue Wong, Bingyu Duan and Sabzali Musa Kahn in DIGITAL HEALTH
Footnotes
Ethics approval and consent to participate
This study was approved by the Ethics Committee of UM University (Approval No.: UM.TNC2/UMREC_3967) and was registered at ClinicalTrials.gov (Identifier: NCT06930898) on 15 April 2025. Retrospectively registered. This article reports findings from a sub-phase of the registered trial. Written informed consent was obtained from all participants prior to their participation.
Consent for publication
Contributorship
The first author, Li Rui, is the developer and owner of the Mammoverse platform evaluated in this study. Li Rui is a postgraduate student at the University of Malaya and developed the Mammoverse platform as part of her academic research. No external funding, commercial interests, or third-party sponsors were involved. The authors declare no other conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Written informed consent was obtained from all participants for publication of this paper, including consent for publication from the individuals depicted in ![]() .
.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request. The Mammoverse platform described in this study is currently not publicly available; however, requests for platform access can be made directly to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.