
Abstract
Background
Breast cancer is a common malignancy among women worldwide, frequently associated with cancer-related cognitive impairment, which significantly affects quality of life. Non-pharmacological therapies, especially digital health interventions (DHIs), show potential in mitigating cognitive impairment related to cancer through tailored and interactive cognitive training. Nonetheless, current research fails to systematically integrate intervention strategies, behavioral change techniques (BCTs), and their effectiveness.
Objective
This scoping review sought to delineate existing DHIs for cognitive impairment related to cancer in breast cancer patients, emphasizing intervention attributes, efficacy, and the use of behavior change techniques to guide future research and clinical practice.
Methods
Following Arksey and O’Malley's framework, nine databases were systematically searched (inception to February 2025). Inclusion criteria were defined using PICOS (Population, Intervention, Comparison, Outcomes, Study design). Data on intervention characteristics, BCTs, and outcomes were extracted and analyzed via Michie's BCT taxonomy.
Results
Nineteen studies were incorporated. DHIs predominantly employed computerized cognitive training (78.94%), virtual reality (VR) (15.78%), and robotics (5.26%). Prominent BCTs encompassed goal setting (100%), feedback/monitoring (89%), and social support (100%). Eighteen investigations indicated substantial cognitive enhancement, six saw better emotional well-being, and two evidenced an elevated quality of life. Gamification and VR therapies resulted in elevated patient adherence and satisfaction.
Conclusion
DHIs significantly enhance Cognitive Rehabilitation and Cognitive Impairment through cognitive training and multifaceted BCTs. Challenges encompass diverse study designs, insufficient long-term data, and technical obstacles. Future research must include standardized cognitive evaluations, longitudinal investigations, and initiatives to address the digital divide.
Keywords
Introduction
Breast cancer is a malignant neoplasm arising from the epithelial cells of breast tissue. The development is impacted by various elements, including genetics, hormones, and environmental exposures. 1 As per the most recent data from the International Agency for Research on Cancer of the World Health Organization, breast cancer ranks among the most prevalent malignancies worldwide, with around 2.31 million new cases reported in 2022, representing 11.7% of all cancer diagnoses. 2 In China, breast cancer is the predominant malignancy among women, with around 420,000 new cases documented each year, and there is a tendency towards a younger age of diagnosis.3,4 Due to advancements in early identification and treatment, the 5-year survival rate for breast cancer patients in China has increased to 82.0%. 5 Nonetheless, these interventions, especially surgery and radiotherapy, have significant repercussions for patients. Issues like inadequate body image and sexual dysfunction indirectly influence overall quality of life.6,7 Furthermore, numerous patients encounter the difficulty of enduring sequelae, such as postoperative lymphedema, radiation dermatitis, chemotherapy-induced peripheral neuropathy, cardiovascular toxicity, and osteoporosis.8,9
Recent research indicates that 17% to 75% of breast cancer patients experience cognitive impairment following therapy, highlighting a substantial concern over their quality of life. 10 Cancer-related cognitive impairment (CRCI) denotes the multifaceted deterioration of cognitive abilities, including attention, memory, and executive function, attributable to either the cancer or its treatments. 11 A review 12 indicated that cognitive impairment was observed in 75% of patients during therapy and in 35% of patients 1-year post-treatment completion. CRCI not only impedes daily activities but also diminishes work productivity, with certain patients unable to resume employment. 13 Furthermore, cognitive impairment can affect social interactions, leading to less participation in social activities and a reduced quality of life. 14
Current methods for cognitive rehabilitation in breast cancer patients encompass pharmaceutical therapies, traditional Chinese medicine rehabilitation, psychological support, physical exercise, and cognitive training. 15 The National Comprehensive Cancer Network advises non-pharmacological approaches as the primary strategy due to the unclear efficacy and possible negative effects of pharmacological treatments, which should be considered only when alternative methods fail.16,17 Several systematic reviews have shown that,18–20 Non-pharmacological therapies, including psychological interventions, cognitive training, physical exercise, and lifestyle modifications, are effective in mitigating CRCI.
In recent years, digital health interventions (DHIs), a novel category of non-pharmacological treatment, have surfaced as effective instruments for addressing cognitive impairment in breast cancer patients. DHIs utilize digital technology such as mobile applications, internet platforms, and wearable devices to provide health management and intervention services. 21 These technologies provide benefits including personalization, flexibility, interactivity, data monitoring, and feedback, thereby augmenting the efficacy of conventional non-pharmacological therapies through intelligent and customized approaches. 22 The incorporation of Artificial Intelligence in healthcare is progressively revolutionizing DHIs, facilitating enhanced personalization, real-time data analysis, and adaptive intervention tactics. AI-driven algorithms can evaluate extensive patient data to discern distinct cognitive profiles and customize interventions, advancing from static programs to dynamic and adaptive health care. 23 DHIs have shown considerable promise and efficacy in addressing cognitive impairment related to cancer in breast cancer patients. A study by Anne et al. 24 showed that video game cognitive training can improve cognitive functioning, especially subjective cognitive functioning, in breast cancer patients. A systematic evaluation by Wang et al. 25 demonstrated that online cognitive interventions have a positive impact on Subjective Cognitive Impairment in cancer survivors, especially breast cancer patients. Nonetheless, the existing research on the utilization of Digital Health treatments (DHIs) in this domain is fragmented and lacks comprehensive summarization and compilation, with all aforementioned studies deficient in additional analysis to discern the successful components of the treatments.
Behavioral change techniques (BCTs) are discernible, reproducible, and integral components of an intervention aimed at modifying or directing behavior. 26 These strategies serve as the essential components of an intervention that can directly affect an individual's behavioral patterns to get enhanced health results. Examining the function of BCTs in interventions is essential as it elucidates the active components of an intervention, hence enhancing the design and efficacy of the intervention. 27 BCTs are extensively utilized in the domain of DHIs. DHIs employ digital technology, including mobile applications and wearable devices, to facilitate health management and promote behavioral change in individuals.28,29 Self-monitoring functionalities offered by mobile applications enable users to document and monitor their health metrics, including blood pressure, blood glucose, and physical activity, in real time.30,31 This self-monitoring device enables users to comprehend their behavioral patterns more effectively, facilitating more precise behavioral modifications. Moreover, DHIs can deliver prompt incentive and assistance via push notifications, reminders, and tailored feedback to improve user engagement and adherence. 32
Despite numerous studies rigorously assessing non-pharmacological therapies for cognitive rehabilitation in breast cancer patients, there is an absence of thorough explanations regarding the characteristics, efficacy, and behavior change techniques employed in these programs. Systematic reviews and meta-analyses generally aggregate previous research but do not furnish direct, first-hand information regarding the specific BCTs utilized. A scoping review is a methodical approach of summarizing and mapping the available literature on a certain issue, providing a comprehensive overview of the field. 33 This scoping review aimed to systematically explore the landscape of DHIs for CRCI in breast cancer patients. Specifically, guided by Arksey and O'Malley's framework, the research aimed to address the following three structured research questions: (1) To explore the characteristics and general intervention strategies of DHIs for CRCI in breast cancer patients. (2) To analyze the specific techniques, procedures, and content elements utilized in these DHIs, as well as BCTs incorporated within them. (3) To evaluate outcome indicators and the effectiveness of intervention strategies. This review is not registered as PROSPERO does not accept scoping reviews.
Methods
This study followed the methodological framework for scoping reviews proposed by Arksey and O'Malley, 34 which includes the following steps: (1) identifying the research question, (2) conducting a comprehensive search for relevant studies, (3) selecting the studies, (4) extracting the data, and (5) organizing, summarizing, and reporting the results.
Review question
The specific research questions addressed in this review are: (1) What are the intervention strategies for CRCI in breast cancer patients, and what are their general characteristics? (2) What techniques, procedures, and content elements are used in DHIs? Which BCTs are incorporated? (3) What outcome indicators are used, and what is the effectiveness of these intervention strategies?
Eligibility criteria
The study utilized inclusion and exclusion criteria based on the Population, Intervention, Comparison, Outcomes, and Study Design (PICOS) framework. 35 Inclusion criteria: (1) Population: Research focused on patients aged 18 or older diagnosed with breast cancer, who had received chemotherapy, radiation, hormone therapy, and/or surgery, and who were evaluated for chemotherapy-related cognitive impairments or shown signs of cognitive deterioration. (2) Intervention: DHIs designed to enhance cognitive impairments in breast cancer patients. This includes, but is not restricted to, cognitive training software, online psychoeducational courses, telemedicine consultations, mobile health applications, and similar resources. (3) Comparison: The control group may consist of standard treatments and care, or alternative non-DHIs such as classic psychoeducation or in-person cognitive training. (4) Outcome: Research must use at least one metric pertaining to overall cognitive functioning, specific cognitive domains (e.g. memory, attention, executive functioning, language ability), or objective neuropsychological evaluations, as primary or secondary outcome measures. (5) Study Design: The included study types comprise randomized controlled trials, experimental studies, feasibility studies, and mixed-method studies. Exclusion criteria: (1) Literature not accessible in full text; (2) Literature published multiple times; (3) Studies that offer merely a cursory overview of the intervention, precluding the identification and coding of behavior change techniques in later phases.
Data sources and search strategy
The system searched nine databases, including PubMed, CINAHL, Web of Science, ProQuest, Cochrane Library, Embase, PsycINFO, China National Knowledge Infrastructure, Wan fang Data. The search utilized a combination of subject phrases, keywords, and Boolean operators, together with citation analysis, undertaken from the library's inception until 9 February 2025. To augment the thoroughness of our research, gray literature was systematically searched via specialized databases and platforms. ProQuest, as an extensive database, was employed to obtain pertinent doctoral and master's theses. In a similar manner, Chinese doctorate and master's theses were retrieved from the China National Knowledge Infrastructure database, a principal repository for academic dissertations in China. The searches for gray literature utilized analogous keywords and Boolean operators as those applied to peer-reviewed journal articles, concentrating on terms associated with “Breast Neoplasm,” “Cognitive Dysfunctions,” “chemotherapy-related cognitive impairment,” and “digital health intervention” (as outlined in Table 1).
Search strategies and search terms.

CRCI: cancer-related cognitive impairment.
Study selection
The acquired material was loaded into EndNote reference management software. Two researchers, both proficient in evidence-based nursing, independently evaluated the studies according to the established inclusion and exclusion criteria. This procedure entailed examining the titles and abstracts, thereafter acquiring and further evaluating the complete texts of pertinent papers. Disputes were settled through collaborative dialogue or adjudicated by an impartial third researcher.
The data extraction for the included studies was conducted independently by two researchers, with any differences addressed and resolved through the participation of a third researcher. A self-created form was utilized to gather general study information, encompassing: authors, country of origin, study design, sample size, components of the DHI (including techniques, procedures, and content elements), control group interventions, intervention duration, cognitive functioning assessment tools, and intervention outcomes. The cognitive function assessment tools are summarized in Table 2. A detailed description of the cognitive assessment tool is included as a separate comprehensive table in Supplementary File 1. The extracted data are summarized in Table 3.
Tools for measuring cognitive function.

Overview of included studies.

VR: virtual reality; RCT: randomized controlled trial.
BCTs were classified utilizing the approach established by Michie et al. (version 1), which organizes 93 unique BCTs into 16 categories, so offering a consistent framework for the identification of BCTs in behavior change interventions. The coding was conducted independently by two reviewers (YXC and YZ), with any discrepancies addressed through deliberation with a third reviewer (WYH) until a consensus was achieved. Table 4 delineates the specific BCTs incorporated in the DHI techniques.
BCTs involved in intervention strategies.
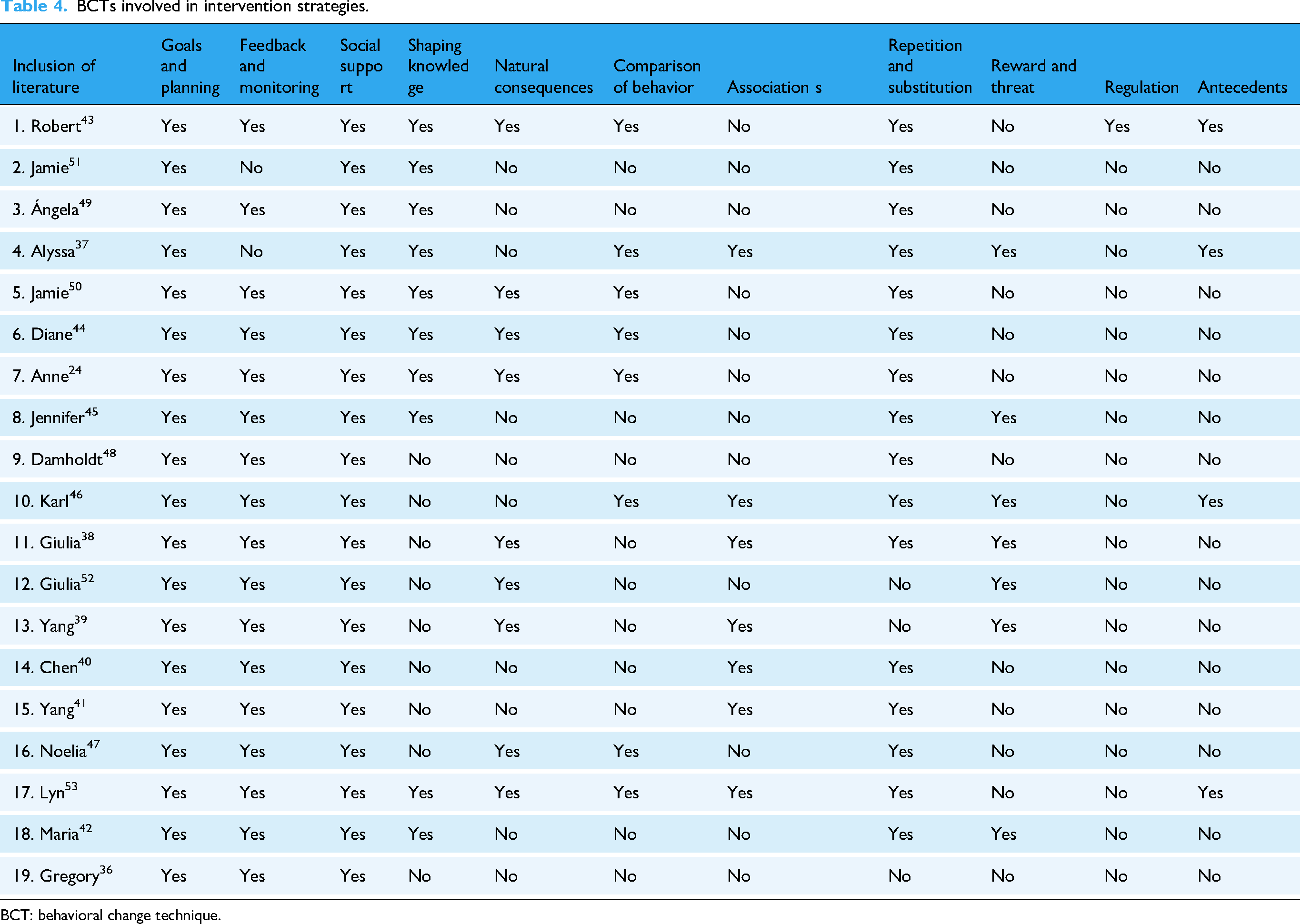
BCT: behavioral change technique.
Results
Selection of sources of evidence
A total of 636 articles were obtained during the initial screening, 21 articles were incorporated from retrospective references, and 545 articles persisted following the removal of duplicates. Following the review of titles and abstracts, 278 articles were excluded; an additional 13 articles were dismissed; 254 articles were eliminated upon full-text evaluation (comprising 51 articles that did not align with the study population, 149 articles lacking cognitive function assessment in the outcome measures, and 35 articles that did not incorporate BCTs in the intervention descriptions); ultimately, 19 articles were selected for inclusion in the final literature review. The process of study selection is illustrated in Figure 1, the study selection diagram.
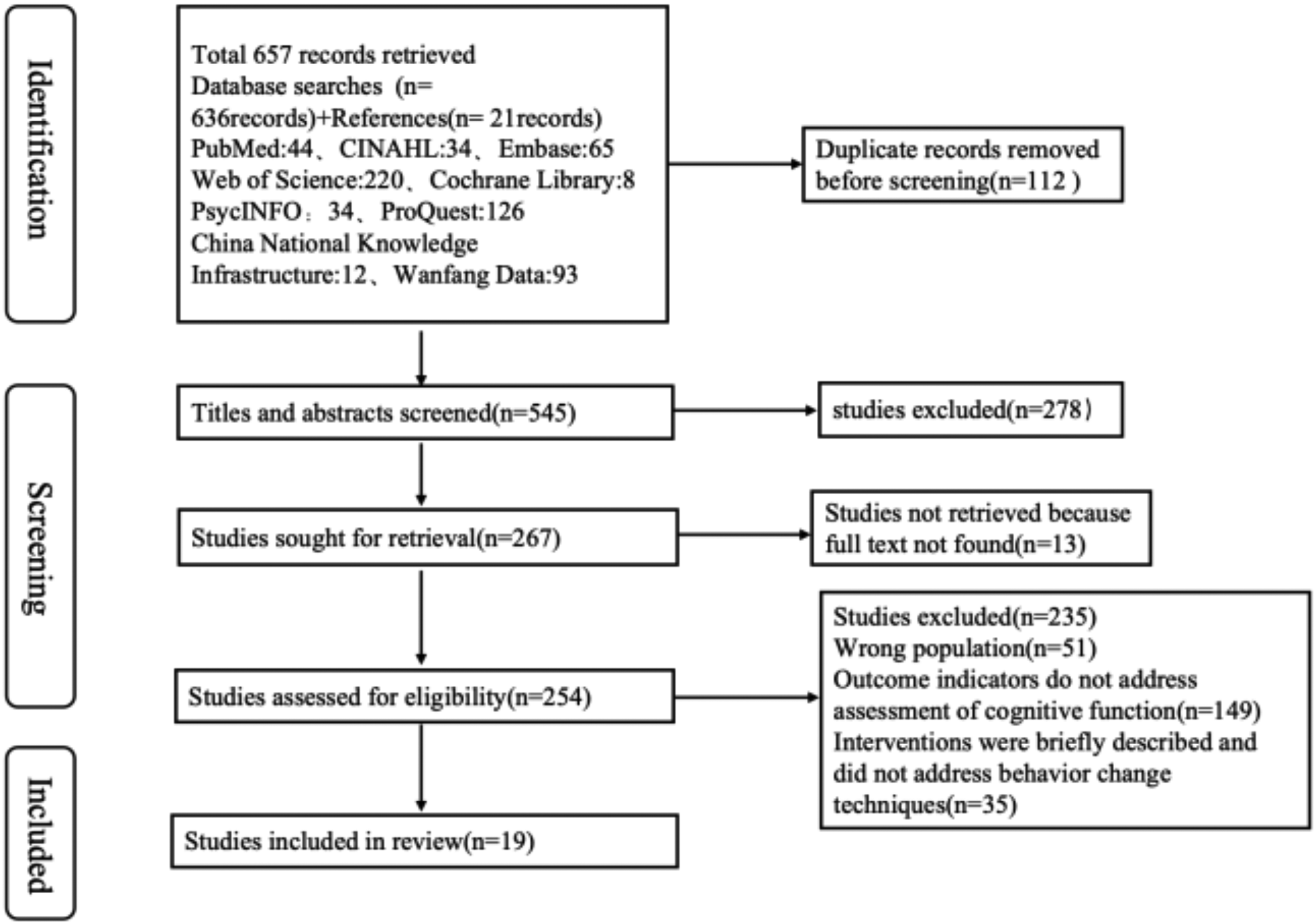
Study selection diagram.
Characteristics and results of sources of evidence
A total of 19 papers were included in this study, published between 2015 and 2024. The geographic distribution of the included literature was broad, with seven from the United States,36,43–45,50,51,53 three from China,39–41 three from Spain,42,47,49 two from France,38,52 one from Germany, 46 one from Denmark, 48 one from Belgium, 24 and one from Canada. 37 Study types included randomized controlled studies (n = 12),24,39–44,46–49,53 feasibility studies (n = 6)36,38,45,50–52 and mixed studies (n = 1). 37 Study sample sizes ranged from 6 to 176. The study subjects were all breast cancer patients with an age range of 18 years and above.
Types of technologies, applications for digital health interventions
In this study, there were various types of DHI technologies, mainly including computer technology, virtual reality (VR) technology, and robotics, with computer technology being the most common. The length of the intervention ranged from 60 min to 12 months, with most studies ranging from 8 weeks to 12 weeks. ① Fifteen studies24,37,38,42–53 (78.94%) used computerized technology for cognitive interventions, with commonly used tools including the Tandberg centric 1700 MXP (2),43,51 NeuroNation© (3),37,46,49 HappyNeuron series (3 items),38,48,52 Zoom (2 items),37,53 BrainHQ program (1 item), 44 Aquasnap (MyCQ™) (1 item), 24 e-CUIDATE system (1 item), 47 and ICOnnecta't program (1 item). 42 Computerized cognitive training uses computer programs and software to enhance cognitive functioning and usually involves a series of organized, interactive computer tasks designed to improve cognitive domains such as attention, memory, and executive functioning. 54 The computer technology interventions in this study covered cognitive behavioral therapy, cognitive training, adaptive training, and homework. ② Three studies39–41 (15.78%) used VR technology for cognitive interventions, and all of them used homemade VR game programs combined with virtual scenarios and somatosensory interactive devices to implement cognitive rehabilitation training. VR technology is a technology that generates a three-dimensional virtual environment that can be interacted with through computer simulation, allowing users to feel like they are in the realm of the real world, 55 The application of VR in cognitive rehabilitation is to improve and rehabilitate cognitive functions by creating immersive virtual environments that allow users to perform various cognitive training tasks in a virtual scene. The VR technology interventions in this study included a virtual cognitive rehabilitation training system, virtual scenes, and game tasks. ③ One study 36 (5.26%) conducted an innovative attempt to combine robotics and VR, using the BrightArm Duo rehabilitation system, which integrates robotic assistance with virtual rehabilitation games for motor and cognitive training. The robot improves user engagement and cognitive recovery through personalized training programs, real-time feedback, and gamified design.
Content elements of digital health interventions
The content elements of the DHI focused on six cognitive training domains, as follows: ① 15 studies24,37–41,43–45,48,49,51–53 involved attention training: using self-directed training, 43 positive thinking meditation,37,51 task-switching, 37 spatial matching, 44 and temporal order judgment. 44 This was done in a variety of ways. Common tasks include “concentration” exercises,49,51 breath control exercises, 37 distraction tasks such as “Pay Attention!”,38,52 “Private Eye!”,38,52 virtual mazes,39–41 vehicle lane changing, 39 and complex puzzles. 42 ② Seventeen studies24,36–46,48–52 involved memory training, covering short-term memory, long-term memory, and different types of memory tasks, such as verbal repetition, 43 visualization strategies, 43 mnemonics, 51 imagery, 51 memorization of words, numbers, or images,36,42,49 and memorization of repetitions of specific yoga poses and sequences. 37 ③ Three studies37,38,52 dealt with language skills training: understanding and following instructions, 37 vocabulary tests, vocabulary and language comprehension tasks such as “Split words,”38,52 “Embroidery,”38,52 and other communication tasks. ④ Eleven studies24,36,38,39,43–45,50–53 dealt with executive skills training: making an organized schedule, 43 simple arithmetic, 50 time-limited crossword puzzles, 44 and problem-solving and decision-making tasks such as “Towers of Hanoi,”38,52 “Basketball in New-York,”38,52 tasks such as rowing a boat, playing ping-pong, and cutting a cake with an avatar, 39 interactive exercises, 53 and task training such as Breakout 3D 36 : training executive functions by bouncing a virtual ball. ⑤ Three studies38,42,52 involved training in visuospatial orientation skills: including training in spatial perception and visual processing tasks such as maze games, 42 3D object rotation and puzzle games. 42 ⑥ One study 52 involved logic and numeracy training: it included logical reasoning tasks, such as “The Right Count” training task. ⑦ One study 49 involved daily living skills training: helping patients to manage daily activities more effectively through energy management and time management skills.
Behavioral change techniques used in intervention strategies
The 19 studies included in this scoping review addressed a total of 11 categories of BCTs, as detailed in Table 3. All 19 studies used at least one category of behavior change technique. Seventeen studies24,36–50,52,53 used greater than five categories of BCTs. Intervention components used in intervention strategies included goals and plans24,36–53 (setting specific cognitive training goals) (n = 19), feedback and monitoring24,38–41,43–50,52,55 (workbooks, telephone assessments, logs, online platforms to record) (n = 17), social support24,36–53 (emotional support, informational support) (n = 19), Knowledge Shaping24,37,42–45,49–51,53 (instruction on how to conduct cognitive training, problem-solving training) (n = 10), Natural Consequences24,39,43,44,47,50,53 (Participants were able to directly perceive an improvement in cognitive functioning through self-reported assessments of cognitive functioning) (n = 9), Behavioral Comparison24,37,43,44,46,47,50,53 (role modeling by others) (n = 8), Connection37–41,46,53 (linking healthy behaviors to positive emotions and outcomes) (n = 7), Repetition and Substitution24,37,38,40,41,43–51,53,55 (diversified activities such as cognitive stimulation combined with physical activity to replace a single activities) (n = 16), Reward37–42,45,46,52 (social or material rewards for completing cognitive training tasks) (n = 7), Conditioning 43 (relaxation training, stress management, emotion regulation) (n = 1), and Antecedents37,43,46,53 (environmental changes e.g. community-centered group activities, videoconference interactions) (n = 4).
Measurement tools for cognitive functioning
This scoping review categorizes techniques for assessing cognitive function into two primary groups: objective assessments (neuropsychological tests) and subjective assessments (patient-reported outcomes (PROs)).
Neuropsychological examinations offer standardized and quantitative evaluations of cognitive functioning. These instruments are employed to assess general cognitive functioning and particular cognitive domains. A variety of neuropsychological assessments have been employed to evaluate overall cognitive functioning. The Montreal Cognitive Assessment was employed in four research.38–41 Other tools for assessing overall cognitive function include the NIH Toolbox Cognitive Battery (n = 1), 37 CNS Vital Signs® (n = 1), 38 and Neuropsychological Assessment Battery 36 (n = 1).
In addition to the overall assessment, studies have targeted specific cognitive domains. In the area of memory functioning, assessment tools for verbal learning and memory include the Hopkins Verbal Learning Test, 36 Rey Auditory Verbal Learning Test, 42 California Verbal Learning Test 43 (each in one study), Selective Reminding Task,44,45 and Verbal Learning Memory Test36,46 (both in two studies). The Auditory Consonant Trigrams Test 47 (n = 1) was also used in this domain. For the assessment of visuospatial memory, Rey-Osterrieth Complex Figure, 46 the Corsi Block-Tapping Test, 42 and the Brief Visuospatial Memory Test, Revised 43 (each in one study) were used. Executive power was assessed by the Trail Making Test42,45,47,49,50 (n = 5), and attention instruments included the Digit Span Task,42,44–46 the Paced Auditory Serial Addition Test 48 (n = 1), the Brief Test of Attention44,45 (n = 2), and the Stroop Colour Word Test 42 (n = 1). Processing speed was assessed with instruments such as the Digit Symbol Substitution Test 42 (n = 1) and the Symbol Digit Modalities Test 43 (n = 1). In addition, Verbal Fluency Test 42 (n = 1) and Rey-Osterrieth Complex Figure 46 (n = 1) were used to assess verbal function and visuospatial function.
Subjective assessments, known as PROs, assess patients’ self- perceived cognitive changes and complaints. In terms of overall cognitive functioning, the most frequently used PRO is the Functional Assessment of Cancer Therapy-Cognitive Function (FACT-Cog),37,38,42–46,49–53 which was used in 12 studies. Other PROs include the PROMIS Applied Cognition 51 (n = 1) and the Cognitive Failures Questionnaire24,48 (n = 2).
Effectiveness of digital health interventions
In 18 studies,24,37,39–42,44–47,49–52,55 the results showed that DHIs had a significant improvement in the cognitive functioning of breast cancer patients. Among them, six studies36,37,42,43,51,53 also found that DHIs were effective in improving patients’ mood states, and the improvement in mood in turn facilitated the recovery of cognitive functioning, creating a virtuous cycle. In addition, two studies42,53 showed that breast cancer patients’ quality of life was significantly improved after receiving DHIs. Meanwhile, five studies39–42,52 found that patients’ satisfaction and compliance with DHIs were high, further demonstrating the feasibility and effectiveness of this intervention program.
Discussion study summary
This study comprehensively analyzes the existing status of DHIs for CRCI among individuals with breast cancer via a scoping review. The findings reveal that DHI techniques include a diverse array of technological methods and content components, integrating modalities such as computer technology, VR, and robotics. These interventions incorporate many BCTs, such as goal setting, feedback monitoring, and social support. The therapies significantly enhanced cognitive impairment in breast cancer patients, especially in the areas of attention, memory, and executive function. Technological Approaches in Digital Health Interventions.
The predominant technologies utilized in DHIs for CRCI in breast cancer patients are computer-based technologies, VR, and robots, with computerized technology representing 78.94% of all interventions. Computerized cognitive training delivers individualized rehabilitation programs using software and interactive challenges, ensuring significant flexibility, repeatability, and real-time progress assessment. 54 Widely used software systems like HappyNeuron and BrainHQ facilitate the training of attention, memory, and executive functions, employing gamification to enhance patient engagement and therapeutic results. 52 Moreover, computerized technologies can be incorporated into multi-module, stratified care frameworks. The ICOnnecta't program integrates advanced digital interventions with cognitive modules, resulting in notable cognitive enhancements and decreased healthcare expenditures. 42 Future research ought to concentrate on investigating the synergistic effects of multidimensional interventions, such as the integration of cognitive training with psychological support or physical rehabilitation, and formulating standardized, tiered intervention protocols customized for patients at various stages of disease.
Virtual reality and robotics in cognitive rehabilitation
VR provides an immersive training environment that markedly enhances cognitive function and daily life skills in breast cancer patients. Research indicates that VR therapies significantly enhance visuospatial abilities, attention, and memory, hence increasing cognitive functions and self-management skills.39,40 Additionally, the use of robotics, such as the BrightArm Duo system, has expanded intervention dimensions by incorporating real-time feedback and personalized training. 36 The BrightArm Duo system aims to rehabilitate upper limb motor function while concurrently providing cognitive training and emotional support via gamified tasks and VR environments. 56 Future research should investigate the amalgamation of cognitive and affective therapies in rehabilitation to improve patient experiences and outcomes.
Content elements of digital health interventions
DHIs focus on six essential cognitive domains: attention, memory, executive functions, language, logic and numeracy, and visuospatial orientation. These domains are trained in a variety of ways, such as attention training through visual tracking tasks to improve concentration, 49 and memory training through memory games and repetitive exercises to enhance memory capacity and efficiency.24,48 In executive training, the combination of gamified design (e.g. “Towers of Hanoi”) and social interaction (Zoom group tasks)38,52 significantly improves long-term adherence and treatment outcomes. This design methodology not only augmented the enjoyment of the tasks but also elevated the patients’ sense of belonging and participation through social interactions, so enhancing the overall therapy experience. The DHI significantly enhanced attention, memory, and executive function, offering patients an effective and sustainable treatment plan via Internet-based cognitive behavioral therapy, gamified design, and real-time feedback mechanisms. Future study should investigate the customization of personalized DHIs to align with the distinct needs and contexts of patients. For instance, creating more specialized training modules and task designs for patients of varying age demographics or disease classifications.
Behavior change techniques in digital health interventions
This analysis thoroughly analyzed the BCTs employed in DHIs for cognitive rehabilitation in breast cancer patients. The findings suggest that intervention strategies employ a diverse array of multidimensional methodologies to enhance cognitive function. “Goal setting and planning” evolved as a fundamental method, assisting patients in elucidating intervention aims and augmenting adherence through the establishment of specific cognitive goals (e.g. enhancing attention or memory). This corresponds with prior research indicating that goal-oriented interventions can significantly enhance self-efficacy. 42 Furthermore, “feedback and monitoring” facilitates real-time data tracking via workbooks and online platform records, enabling patients to dynamically modify training intensity. Research has also demonstrated that these strategies can improve behavioral maintenance through instant feedback.38,52 Social support, as a prevalent method, alleviates patients’ psychological stress via emotional and informational assistance (e.g. group interactions, therapist guidance), potentially enhancing cognitive symptoms and underscoring the significance of psychosocial factors in CRCI interventions. 42 Significantly, procedures like “knowledge shaping” (n = 10) and “behavioral comparison” (n = 8) may assist patients in developing adaptive strategies through cognitive training instruction and role modeling. 57 Conversely, “Repetition and Substitution” amalgamates many therapies, including cognitive stimulation and physical activity, or amplifies the efficacy of interventions via neuroplasticity mechanisms.58,59 In contrast, the low utilization of “conditioning” and “antecedent” techniques suggests the need to further explore the mechanisms and scenarios of relaxation training and environmental adjustment in CRCI. 60 Despite the fact that most of the existing studies used comprehensive BCTs, extrinsic motivators such as “rewards” (n = 7) were less frequently used, which may limit long-term behavioral maintenance.21,61 Future research should investigate methods to enhance long-term patient engagement and adherence via extrinsic motivators (e.g. incentives), while employing digital platforms to deliver real-time feedback and facilitate dynamic adjustments in training intensity may significantly improve intervention efficacy. Augmented emotional and informational support (e.g. group engagement, therapist advice) can mitigate patients’ psychological stress and indirectly enhance cognitive symptoms.
Challenges and future directions
While current research has shown the substantial impact of DHIs on enhancing cognitive impairment in breast cancer patients, numerous problems and limits persist. Cognitive functioning is frequently neglected, mostly due to the absence of defined protocols, inadequate awareness of cognitive effects among healthcare providers, limitations in resources and time, and the unavailability of suitable assessment instruments. 42 Secondly, while research indicates that older breast cancer patients exhibit greater acceptance and compliance with digital cognitive stimuli, variations among distinct patient demographics may influence the acceptance rate. 52 In the future, it is essential to create more intuitive interfaces (e.g. streamlined operating procedures) and assess the efficacy of long-term incentives. Simultaneously, technical obstacles (e.g. device compatibility, financial constraints) must be resolved to mitigate the digital divide. 62 Moreover, despite the convenience and cost-effectiveness of DHIs, patients may encounter issues with device and network access or a lack of familiarity with digital tools, thereby constraining the generalizability of the intervention. The constraints of assessment instruments and the intricate influence of several factors (e.g. chemotherapy, endocrine therapy, psychological condition, etc.) on cognitive performance pose problems for intervention development.63–65 While short-term impacts have been evidenced, long-term effects require further validation, and the majority of existing studies have concentrated on short-term observations, missing longitudinal research extending five years or beyond. Moreover, extensive investigations of DHIs remain constrained by resources and financing, thus restricting the scope and depth of the studies, thereby impacting the comprehensiveness and trustworthiness of the findings. Future research must address these challenges by enhancing intervention programs, increasing sample numbers, and investigating long-term impacts to improve the efficacy and generalizability of therapies.
In contemplating the future advancement of DHIs for breast cancer patients, several critical directions warrant attention. Initially, the design of tailored interventions is crucial for enhancing outcomes. Patients with breast cancer exhibit varying forms of cognitive impairment, making it essential to tailor interventions according to their cognitive function and specific requirements. Employing artificial intelligence and big data analytics to monitor patients’ cognitive alterations in real time and adapt intervention tactics accordingly can enhance the precision and efficacy of therapies. The creation and execution of DHIs necessitate interdisciplinary cooperation. Interdisciplinary collaboration among medicine, nursing, psychology, and computer science, particularly in data collecting, analysis, and privacy protection, will establish a more robust foundation for future interventions. Consequently, interdisciplinary collaboration will be essential for the effective implementation of DHIs. Third, while current research has offered initial indications that DHIs can enhance cognitive function, the precise pathways are not fully elucidated. Future research should concentrate on boosting cognitive ability through the stimulation of neuroplasticity and the optimization of brain network coordination, thereby elucidating its biological foundations and offering theoretical support for intervention strategies. The long-term consequences of DHIs and patient satisfaction are critical factors that must not be overlooked. Notwithstanding the substantial immediate results of the intervention, the patients’ acceptance and happiness, along with the sustainability of the long-term impacts, remain critical inquiries that require urgent exploration in forthcoming investigations. Consequently, longitudinal follow-up studies and patient feedback will be essential to refine the intervention program and augment its practical applicability.
Strengths and limitations
This study, unlike other systematic studies, further demonstrates the capacity of DHIs to include various BCTs. Conventional non-pharmacological interventions (e.g. psychoeducation, fitness programs), while demonstrated to be successful, do not possess the personalized and data-informed attributes of DHIs. This paper is the inaugural systematic summary of the application model of BCTs, addressing the research gap in CRCI management. The review indicated that DHIs markedly enhanced cognitive functioning, especially in the areas of attention, memory, and executive functioning. Moreover, research has highlighted the beneficial effects of DHIs on emotional well-being and overall quality of life, with numerous studies indicating elevated patient satisfaction and adherence to DHIs. Nonetheless, limits in research persist. The significant heterogeneity among the included studies, characterized by substantial variations in sample size and intervention duration, may compromise the generalizability of the findings. Additionally, the absence of long-term follow-up data, particularly regarding the validation of effects beyond 1 year, constrains the evaluation of the enduring impacts of DHIs. Moreover, technological obstacles (e.g. device compatibility, financial constraints) and variations among patient demographics (e.g. age, digital literacy) may have resulted in disparate rates of intervention adoption, while insufficient descriptions of BCTs in certain trials exacerbated the challenges of coding and analysis. The variety of cognitive function testing techniques and the intricate influence of confounding variables (e.g. chemotherapy, psychological condition) may undermine the trustworthiness of the results.
Conclusion
DHIs present a viable strategy for addressing Cognitive Impairment related to Cancer in breast cancer patients. This scoping study indicates that DHIs, utilizing technologies such computerized cognitive training, VR, and robots, can markedly enhance cognitive performance, emotional well-being, and overall quality of life. By incorporating diverse BCTs, these therapies foster patient involvement and adherence, hence augmenting their overall efficacy. Nonetheless, obstacles including the absence of standardized evaluation instruments, study variability, and insufficient long-term data persist. Future study ought to concentrate on creating standardized cognitive evaluation instruments, examining long-term impacts, and tackling the digital divide to enhance accessibility. It is essential to investigate personalized, interdisciplinary strategies that integrate cognitive training, psychological support, and physical rehabilitation to enhance the efficacy of DHIs for breast cancer patients.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251358297 - Supplemental material for Digital health interventions for cancer-related cognitive impairment in breast cancer patients: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076251358297 for Digital health interventions for cancer-related cognitive impairment in breast cancer patients: A scoping review by Ying-Xiang Chen, You Zhou, Xiao-Lan Zhang, Wen-yan He, Qin Ye and Min Xu in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251358297 - Supplemental material for Digital health interventions for cancer-related cognitive impairment in breast cancer patients: A scoping review
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251358297 for Digital health interventions for cancer-related cognitive impairment in breast cancer patients: A scoping review by Ying-Xiang Chen, You Zhou, Xiao-Lan Zhang, Wen-yan He, Qin Ye and Min Xu in DIGITAL HEALTH
Footnotes
Acknowledgment
The author thanked all.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Zhejiang Province Science and Technology Plan Project (Grant Number: 2023C03165).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Credit author statement
All authors were involved in the conceptualization and design of the study. YXC was responsible for the study design, developing the literature search strategy, literature search, data extraction and writing the first draft. YZ was responsible for the literature search, data extraction and writing part of the first draft.MX, XLZ, WYH, and QY were responsible for providing their expertise, making suggestions and critically revising the first draft.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.