
Abstract
Background
Routine health information systems (RHISs) are essential for evidence-based planning and decision-making in the health sector. However, their utilization in Ethiopia's private health sector remains under-examined. The limited quality and quantity of RHIS data further restrict their usefulness, particularly in private health facilities. This study aimed to assess the extent of RHIS data utilization and identify determinant factors among healthcare providers in private health facilities in Gondar, Amhara Region, Northwest Ethiopia.
Objective
To evaluate the utilization of routine health information and its associated factors among healthcare providers in private health facilities within the Gondar City Administration.
Methods
A cross-sectional study was conducted from 8 July to 24 August 2022, involving 400 healthcare providers selected from 20 private health facilities. The data were collected using structured questionnaires administered to managers, health workers, and health informatics professionals. The data were analyzed using SPSS version 26, and binary logistic regression was employed to identify significant determinants. Variables with a p-value <0.05 were considered statistically significant.
Results
Routine health information utilization was reported by 53% of respondents. Educational status, professional category, and departmental assignment were significant determinants (p < 0.05). The mean age of respondents was 28 years. The majority were male (68%) and held BSc degrees; approximately 188 (47%) worked in outpatient departments. Educational status, profession, and working units were found to be positively associated with utilization of health information, while having no performance standard was found to be negatively associated.
Conclusion
The moderate level of RHIS utilization underscores the need for targeted capacity building, on-the-job training, and stronger integration of private health facilities into the national RHIS framework.
Keywords
Contributions to the literature
There is limited evidence in assessing the private health sector's routine health information delivery system from the relevant authorities.
The routine health information is primarily owned by the government; the routine health information delivery system, particularly to the private health facilities, is very crucial as they contribute more to public health. The routine health information delivery system is an important method to deliver quality healthcare to the public, both by private and public health facilities.
Background
Health information is the foundation of the overall building blocks of health systems, to strengthen the knowledge and skills of healthcare providers. The availability of information will enable healthcare providers to utilize the same information for planning, implementation, monitoring, and evaluation, and to amend the making of health programs. 1 The utilization of routine health information systems (RHISs) has the potential to facilitate the development of private healthcare facilities’ indication and evaluation systems. 2 Routine health information is likely to allow private healthcare facility managers and service providers to document, analyze, and use information to improve coverage, continuity, and quality of healthcare services at all levels by better planning, monitoring, and evaluation of private health facility services. 3
Health information managers are charged with the protection of patient privacy and are responsible for training their employees in the proper handling and usage of the confidential information entrusted to them. 4 With the rise of technology's importance in healthcare, health information managers must remain competent with the use of information databases that generate crucial reports for administrators and physicians. 5
The Declaration of Alma-Ata in 1978 led most developing countries to implement health sector reforms, among which the utilization of routine health information became very important for reference and evidence. 6 The underpinning primary level of health management units in the delivery of health services was taken as the core providers of health services to the people, especially in rural areas, which meant that they also carried the responsibility of managing health-related information. 6
Globally, all countries have implemented a Health Information System, which initially enabled the production of high-quality, timely data. These data build the foundation for the functionality of the health systems and are used for decision-making across the other building blocks of the healthcare system, influencing the quality of health service delivery modalities and overall health outcomes. 1
The Ethiopian Health Management Information System has been implemented since 2008 to improve the provision of health services and ultimately, to improve the health status of the population. Currently, the information revolution is collected in the health facilities, summarized at the district, zonal, and regional levels, and later forwarded to the Ministry of Health Ethiopia at the central level, where data analysis would be done, but the private health facilities are not routinely involved in the process. 7
Routine data can also be collected from the community. The factors for routine utilization of health information are divided into technical, organizational, and behavioral characteristics, 8 and this will be a basis for the formulation of the objectives of the study that will guide the whole research process. In this study, these categories of determinants are reported to have an influence on the proper utilization of routine healthcare for better private health facility management. 9
It is important to understand whether the continuously recorded data are regarded by these private health facilities to inform decision-making for quality service delivery and contribute to national policy formulation. The major intention of this study is to document whether private health facilities in Gondar district, based on the routine collected information, make their organizational decision-making process. 9 This study, therefore, aimed to assess the level of routine health information utilization and identify its determinant factors among healthcare providers in Gondar's private health facilities. By shedding light on existing gaps and opportunities, the research sought to contribute actionable knowledge to strengthen health data usage for health information use across Ethiopia's mixed health delivery landscape.
Method and materials
Study area and periods
The study was conducted in Gondar City, Ethiopia, in private health facilities from July to August 2022. There are two private hospitals and 42 clinics in the city. Gondar City is located in the central Gondar Administrative Zone, Amhara National Regional State. It is about 738 km northwest of Addis Ababa, the capital city of Ethiopia. They are serving 344,635 inhabitants of the city. 10 Gondar is one of the ancient and heavily populated cities in Ethiopia.
Those private clinics have different rooms and beds for service. Each clinic has at least six rooms: examination, laboratory, triage, pharmacy, testing, counseling, and X-ray or ultrasound rooms. On average, each private clinic has 15 health professionals, one head, and one data manager.
Study design
An institution-based cross-sectional quantitative study was conducted at private health facilities in Gondar city, Ethiopia.
Population
Source population
All healthcare providers who are working in private health facilities and managers in the Gondar city administration were the source population.
Study population
All healthcare providers who were working in private health facilities during the data collection period were the study population.
Eligibility criteria
Inclusion
Healthcare providers who were randomly selected were included in the study.
Documents from the past three years were used
Exclusion
Healthcare providers who were not available during data collection, sick, or on leave were excluded. Documented for less than three years, and healthcare providers who have worked in that facility for less than six months were excluded from the study.
Sample size determination
The sample size was determined using the single proportion formula with a 95% confidence interval (CI) and a 5% margin of error, and p = 50%.
The sample in this study will be calculated as follows:

Sampling technique
Among 44 private health facilities found in Gondar city, 20 of them were chosen through a lottery method. Then, 400 randomly selected respondents (healthcare providers) participated in this study. One hundred healthcare providers from each selected health facility were selected using the lottery method.
Data collection tools and procedures
The data collection tool, questionnaire, and checklist were adopted from different literature. 8 Pre-determined structured interview-based questionnaires and an observational checklist were used. Document review using a pre-determined checklist was used to ascertain reporting and health information utilization at the health facilities. Responses from healthcare providers were obtained by the use of both closed and open-ended self-administered questionnaires, and the data were collected by three trained data collectors and supervised by a supervisor.
Study variables
Dependent variables
• Effective utilization of routine health information
Independent variables
• Socio-demographic factors
✓ Age ✓ Sex ✓ Educational status ✓ Religion ✓ Marital status ✓ Profession
• Technical factors
✓ Skilled staff skills ✓ Computer software ✓ IT complexity ✓ Complexity of data management ✓ Standard indicators ✓ Information processing ✓ Data collection tools
• Organizational factors
✓ Culture of information ✓ Information distribution ✓ Supervision ✓ Governance ✓ Planning • Resource availability
• Behavioral factors
✓ Beliefs ✓ Customs ✓ Values ✓ Attitude and values ✓ HIS tasks
Operational definitions
The mean scores were used to label healthcare providers as having good or bad utilization of information and health information utilization. “Has good routine health information utilization” when they scored above the mean value, or “has poor routine health information utilization” when they recorded equal to or below the mean value.
Data processing and analysis
The collected data were entered, checked for completeness, and accuracy. Based on the objectives of the study, the data were analyzed using the Statistical Package for Social Sciences (SPSS) Version 26 computer program, through which percentage and frequency were used to determine routine utilization of health information in private health facilities. Frequency tables, pie charts, and text narrations were used for descriptive results.
Data quality management
Three days of training were given for data collectors and a supervisor. The supervisor was checking data completeness and consistency daily during data collection. Descriptive statistics were used to describe the variables. We did pre-testing of the questionnaire with a few (10%) respondents, other than the target respondents, at a private health facility found in the Bahir Dar city administration.
Ethical consideration
Ethical approval was obtained from the ethics review committee at the University of Gondar. In addition, verbal permission from the managers was obtained from each private health facility to conduct the data collection. Verbal consent was obtained from each participant, and strict confidentiality was maintained. Special codes were used for study participants recorded on questionnaires. The filled questionnaires were kept under lock, and only the researcher had access to the keys.
Results
Sociology: Demographic characteristics of respondents
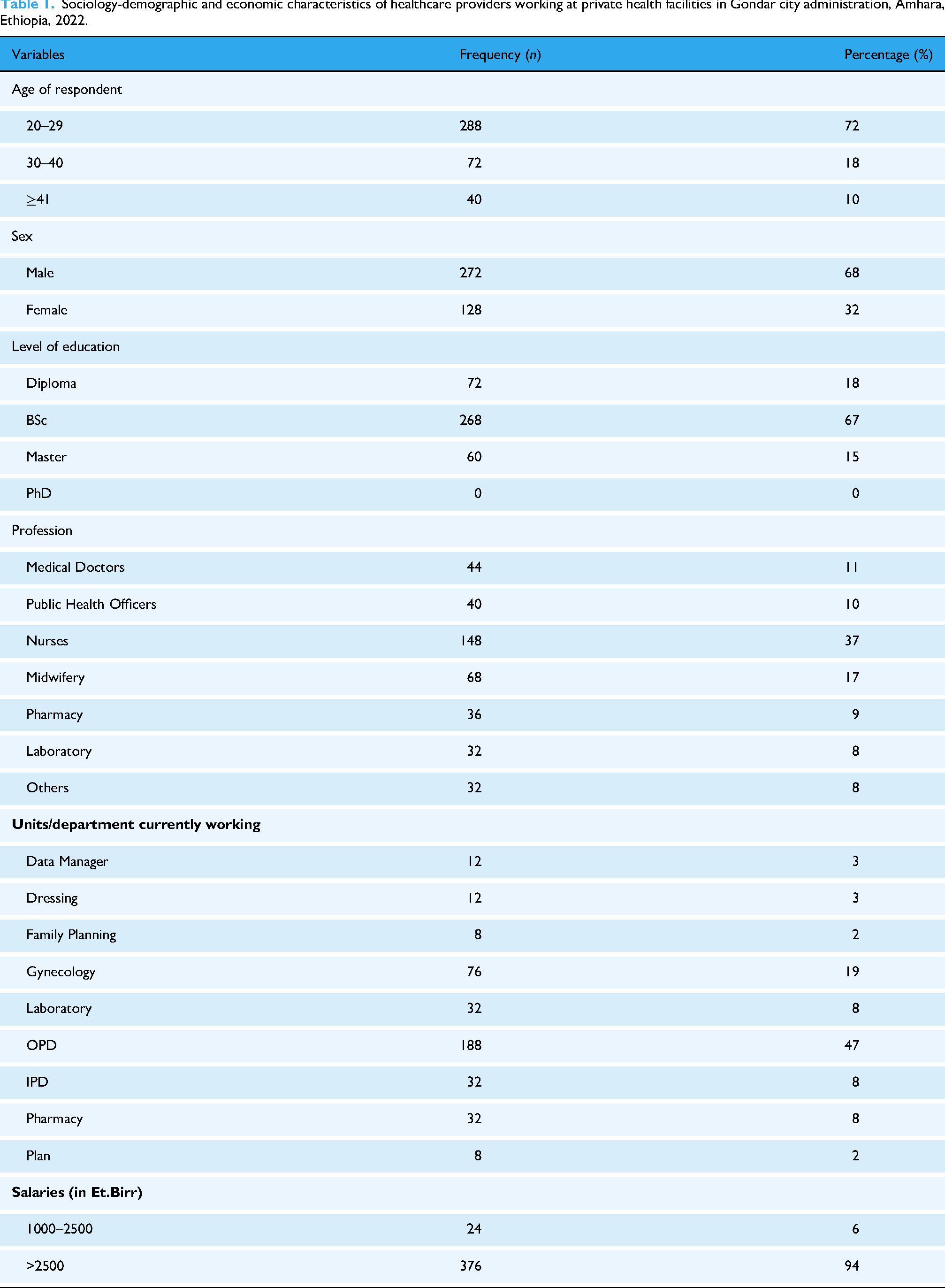
From the total of 423 study subjects, 400 (94.5%) were involved in the study, yielding a response rate of 94.5%. The mean age of the participants was 28 years. Of the total respondents, the majority (67%) were males, and the majority of the respondents were BSc holders. From the total of working departments or units, 47% were working in the outpatient departments (Table 1).
Sociology-demographic and economic characteristics of healthcare providers working at private health facilities in Gondar city administration, Amhara, Ethiopia, 2022.
Activities used for the utilization of routine health information
According to our findings, the magnitude of routine health information utilization of healthcare providers was found to be 53% [at 95% CI: (58%, 48%)]. In the study, the majority of the respondents, 373 (93%), used information to treat patients. Most facilities, 349 (87%), were collecting data using standard tools, and very few facilities did not use standard tools for collecting data. A majority of the respondents, 283 (71%), said there were no department performance evaluations (Table 2).
Activities used for utilization of information at private health facilities in Gondar city administration, Amhara, Ethiopia, 2022 (n = 400).

Technical factors for the utilization of health information
More than half of the study participants, 237 (59%), had received training in the previous 12 months. The majority of the respondents, 210 (53%), took training over the last 12 months on health information collection. Of the total respondents, only six participants took training on health information analysis (1.5%) (Table 3).
Technical factors for the utilization of health information at private health facilities in Gondar city administration, Amhara, Ethiopia, 2022.

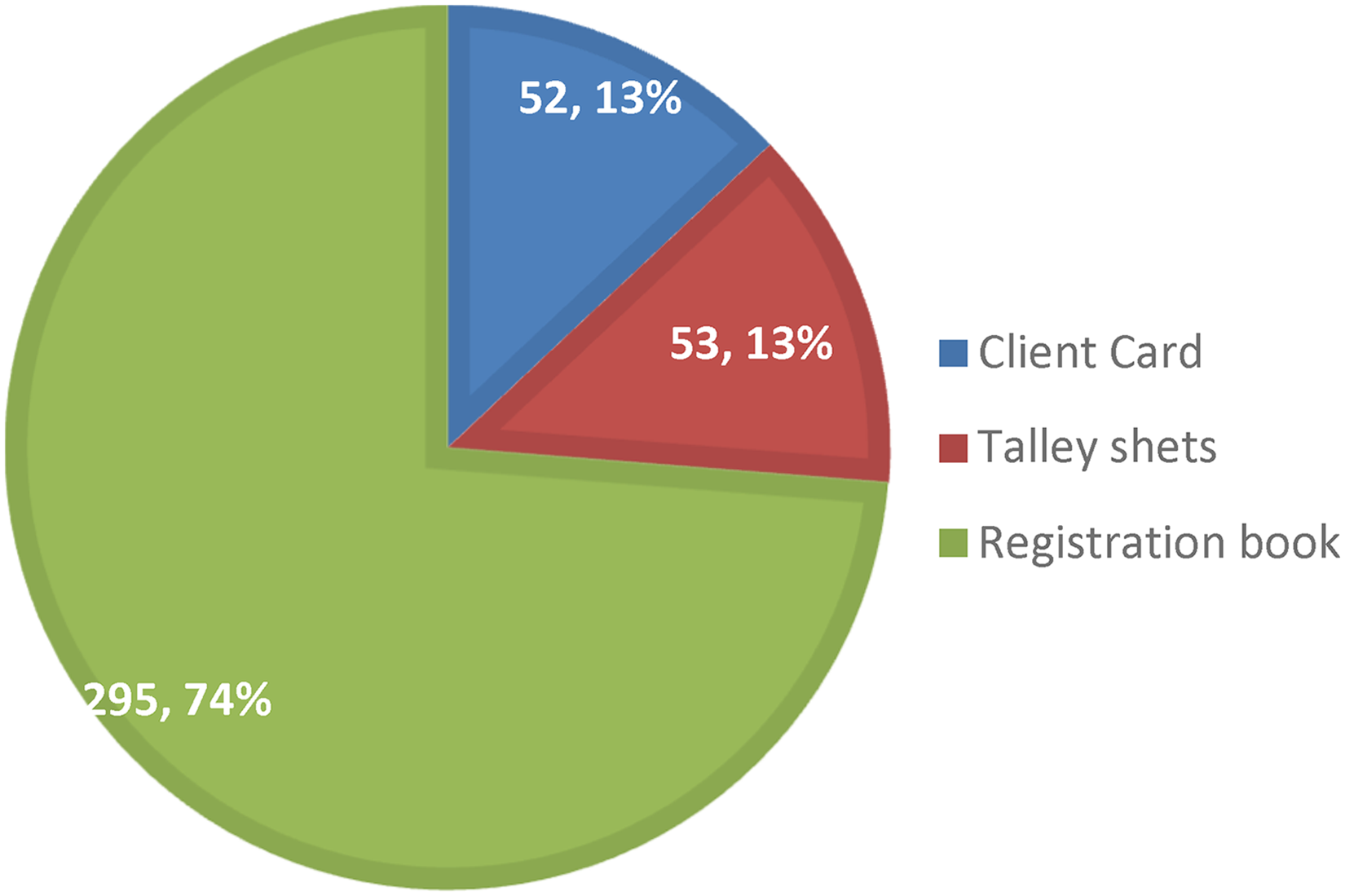
Technical and organizational factors for utilization of routine health information
From the investigation, the majority of the respondents, 295 (74%), used registration books for reporting and data collection, and 53 (13%) respondents used tally sheets for collecting data, and less than half of the respondents, 52 (13%), used client cards for data collection (Figure 1).
Technical and organizational factors at private health facilities in Gondar city administration, Amhara, Ethiopia, 2022 (n = 400).
Organizational factors for the utilization of information
The majority of the respondents, 335 (84%), were affected by organizational rules to use health information, and 178 (45%) of the participants were not affected by poor leadership to use health information (Table 4).
Organizational factors for the utilization of information at private health facilities in Gondar city administration, Amhara, Ethiopia, 2022 (n = 400).

Behavioral factors for the utilization of information
Two hundred fifty-two (63%) of the participants disagreed with the poor attitude toward data collection, 276 (69%) disagreed with the uselessness of health information systems, and more than half (69.75%) disagreed with data not being used for patients. The majority of the respondents, 361 (90.25%), agreed that routine health information (RHI) data can measure the performance of the facilities. From the respondents, 326 (82%) were documenting and keeping the daily records, and 344 (86%) used information for evidence-based decision-making (Table 5).
Information utilization behavioral factors at private health facilities in Gondar city administration, Amhara, Ethiopia, 2022 (n = 400).

RHI: Routine Health Information.
Factors associated with routine health information utilization
Binary logistic regression was done to identify variables associated with the utilization of routine health information among healthcare providers in private health facilities in Gondar city, Ethiopia. Variables such as professional category, working unit, and having performance indicators were found to be significant factors for the utilization of health information in private health facilities.
Having a BSc professional was found to be 3.6 times more likely to utilize information as compared to a Diploma [adjusted odds ratio (AOR): 3.56, 95% CI (3.532, 23.953)]. Being a midwife in the profession was found to be 71% less likely to utilize health information as compared to medical doctors [AOR: 0.29, 95% CI (0.146, 0.776)]. Working unit was found to be another factor; the Gynecology department was found 10 times more likely to use health information as compared to the Medical Laboratory department [AOR: 10.0, 95% CI (9.648, 18.839)]. The odds of health information utilization among healthcare providers who had displayed and evaluated RHIS targets in offices were 18% less likely to use routine health information as compared to those who had no such performance indicators displayed to utilize routine health information [AOR: 0.82, 95% CI (0.748, 2.839)] (Table 6).
Associated factors for routine utilization of health information in private health facilities in Gondar city, Ethiopia, 2022 (n = 400).

COR: crude odds ratio; AOR: adjusted odds ratio; SE: standard error; 95% CI: 95% confidence interval; RHIS: routine health information system.
Discussion
The health information data are owned by the government as well as by the government health facilities; moreover, the training opportunities are also owned by them to get updated information for the health service delivery of the private health organization. On the other hand, the private healthcare delivery should be incorporated into the healthcare delivery of the country. According to our findings, the magnitude of routine health information utilization of healthcare providers was 53% [95% CI (48%–58%)]. The result is in line with the study conducted in East Wollega Zone, Oromia, Ethiopia (57.9%). 11 This result is also in line with the systematic review and meta-analysis, which found that the pooled prevalence (53.7%).
This finding is higher than the studies conducted in Jimma (32.9%), 12 East Gojjam(45.8%), 13 Addis Ababa (37.3%), 14 and in the Amhara region (37.72%) 15 of Ethiopia. This variation might be due to differences in study sites and periods; moreover, recently, the government has given special emphasis on the utilization of information for evidence-based decision-making and the improvement of healthcare providers’ information-using culture at private health facilities.
More than half of the respondents were not technically affected by the use of information utilization. The result of this study is lower than the study conducted in East Wollega Zone, Oromia (70%), and Hadiya zone, Southern Ethiopia (62%), 11 Ethiopia, and Illuba Bore zone, western Ethiopia, at public health facilities (62.7%).14,16 The finding is also lower than the study conducted in Gondar, Ethiopia (78.5%). 17 The probable reason may be that governmental health institutions could get training and UpToDate information for healthcare providers early.
Utilization of information by healthcare providers has high agreement on the use of information for treating patients (69.75%). Healthcare providers strongly agreed on collecting health information using standard tools. About 70% of the respondents agreed with the data quality checking system, which is consistent with the study conducted in Addis Ababa, Ethiopia. 14 The result was different from the studies conducted at public health facilities in North Gondar, Jimma, and East Gojjam of Ethiopia.12,17,18
The technical factors in the use of electronic devices for data management to utilize health information were poor. The study is consistent with the systematic review (combinations of technology enhancement along with capacity building activities were found useful in improving data quality). 19 As the Global Health: Science and Practice, many barriers are linked to organizational and behavioral factors, as explained in the PRISM framework, which identified that poor attitudes toward data, limited technical skills, and lack of supportive supervision were major barriers to RHIS use. 20 The comparative study in Dire-Dawa revealed that routine health information utilization was significantly lower in private health facilities (28.7%) compared to public ones (59.8%). Factors such as lack of training, poor information utilization culture, and limited access to guidelines were more pronounced in private health facilities. It may be due to a lack of computer skills, complex electronic devices, and a lack of supporting staff to use them.
Being a BSc professional was found to be 3.6 times more likely to utilize information as compared to a Diploma [AOR: 3.56, 95% CI (3.532, 23.953)]. Being a midwife in the profession was found to be 71% less likely to utilize health information as compared to medical doctors [AOR: 0.29, 95% CI (0.146, 1.776)]. Working unit was found to be another factor; the Gynecology department was found 10 times more likely to use health information as compared to the Medical Laboratory department [AOR: 10.0, 95% CI (9.648, 18.839)]. This is consistent with the study conducted in the Harari Region, and Gonad, Ethiopia.17,21 The odds of health information utilization among healthcare providers who had displayed RHIS targets in offices were 18% less likely to use routine health information as compared to those who had no such performance indicators displayed to utilize routine health information [AOR: 0.82, 95% CI (0.748, 2.839)]. This might be due to the absence of standard indicators, which provide information for evidence-based decision-making at private health facilities.
Conclusion
Despite moderate uptake, RHIS utilization at private health facilities in Gondar City should be improved through targeted interventions. Training, use of electronic tools, and routine supervision are critical. Incorporating private health facilities fully into the system of national RHIS strategies is imperative for holistic health system strengthening.
Level of education, type of profession, on-the-job training, and use of electronic devices for data collection were significantly associated with the utilization of routine health information. Building the capacity of healthcare providers and understanding their HIS roles and responsibilities would enhance the application of technical skills to analyze, interpret, and use routinely collected data and information for planning, implementation, or decision-making for all health facility healthcare providers. Stronger government involvement and standardized procedures may enhance RHIS integration and data culture in the private sector.
Therefore, on-the-job training and use of electronic devices in private clinics are highly recommended; moreover, routine supportive supervision is mandatory from the government health administrators.
Limitations of the study
The study focused only on technical, behavioral, and organizational determinants without looking at the management system factors and existing constraints and opportunities for effective routine health information utilization.
Recommendation
Footnotes
Acknowledgments
We sincerely acknowledge the University of Gondar for giving permission letters to conduct this research. Our next appreciation goes to the study participants, coordinators, data collection facilitators, and the staff of the respective colleges.
Ethics approval and consent to participate
Ethical clearance was obtained from the University of Gondar Ethical Review Board. The study participants were also informed about the objectives of the study, privacy, and data protection, and gave informed verbal consent before being enrolled in the study. Additionally, the confidentiality and privacy of the information were maintained.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data
The original data are available at hand and may be delivered upon request via the corresponding author.