
Abstract
Background
The World Health Organization has identified health information systems as part of the six building blocks of a health system. A health management information system (HMIS) is part of a health information system, and it is critical in evidence-based decision-making when planning, implementing, and evaluating health programs.
Objective
The objective of this study is to determine HMIS utilization and associated factors in public and private health facilities of Somalia's Mogadishu in 2022.
Methods
A quantitative cross-sectional study was conducted from 08 May 2022 to 11 September 2022 on 411 healthcare workers in public and private healthcare facilities in Mogadishu. After obtaining consent, data were collected using self-administrated and standardized questionnaires. Collected data were then analyzed using SPSS version 26. A logistic regression model was computed to measure the factors associated with HMIS utilization. A p-value of 0.05 with a 95% CI was used as a cutoff to indicate the level of statistical significance.
Results
The study found that 237 (57.7%) (95% CI: 1.53–1.62) of the 411 respondents had good HMIS utilization practices. Healthcare workers who had not received HMIS training were 60.9% less likely to use HMIS (AOR = 0.391, 95% CI: 0.200–0.764) compared to those who had received HMIS training. Health workers who did not receive regular supportive supervision were 69.5% less likely to use HMIS (AOR = 0.432, 95% CI: 0.218–0.856) than those who did receive regular supportive supervision. Those with the skills needed to use HMIS data for decision-making were 91.1% less likely to use HMIS (AOR = 0.089; 95% CI: 0.042–0.185) compared to their nonskilled counterparts.
Conclusion
The result of this study shows that the magnitude of HMIS utilization among health workers in public and private health facilities in Mogadishu is low—237 (57.7%)—compared to its use from similar studies. The study found that skills training on HIS/HMIS and support from managers have a significant correlation with HMIS utilization. Given this, all concerned bodies should work hard to bridge the gaps identified in this study.
Keywords
Introduction
The World Health Organization identified health information systems as part of the six building blocks of a health system. The other building blocks are: a healthy workforce, leadership and governance, delivery of health services, financing of health care, and access to essential medicines. While each of the six building blocks is essential, health information systems are critical in decision-making in each of the other five building blocks and thus form the bedrock of any healthcare system. 1 The health management information system (HMIS) is part of the health information system and it is critical for evidence-based and informed decision-making during the planning, implementation, and evaluation of health programs, and for the appropriate use of resources at all levels of the healthcare system. 2 Health management information system is a tool that helps to gather, aggregate, analyze, and use information to improve the efficiency of health systems.3,4
Health management information system helps provide accurate, disaggregated, and real-time information from all levels of the healthcare system to enable disease surveillance, monitoring of activities, resources, information dissemination, and guideline formulation. It is not limited to this but it also informs patients and gives feedback to professionals in the health system, it is also a basis for public health.5,6 Good HMIS implementation indicates the existence of a strong health system. 7 Although HMIS strengthens the healthcare system and helps in making evidence-based decisions, studies have shown that its utilization is poor in developing countries and varies from 27% to 69.6% in Africa. 8 In the Strategic Plan for the Health Sector (January 2013–December 2016) of Somalia, the extension of the reporting of HMIS data to all functioning public health institutions and some private health providers to improve data interpretation and analysis and produce annual regional health reports for each region and Consolidated Zone Report was proposed. 9
Health management information system is central to the operation of other health system building blocks, but it is influenced by other determinants. Despite its benefits, many factors hinder its use. Among the factors affecting HMIS, studies show that the organization factor is crucial. These organizational factors include organizational structure and processes, unavailability of HMIS resources, and poor governance issues. 10 Systematic reviews conducted in low- and middle-income countries on challenges related to the routine use of health data also show that technical, behavioral, and organizational/environmental determinants affect HMIS. 11
As for Somalia's health system, the country has put more effort into the rehabilitation of the health system that was distracted during the conflict. According to a baseline study of Somalia's health sector, the country does not have an efficient and comprehensive health information system. Therefore, there is a lack of patient-based statistics that can inform decision-making, resource allocation, and planning in health services delivery. The Somali HMIS is characterized by enormous challenges in performance and capacity, as well as a lack of proper mechanisms to disseminate information used for decision-making. This weak health information system is also characterized by poor human resources databases and records in both public and private health sectors. 12 Thus, this study aims to find more evidence of HMIS utilization in an attempt to establish the current HMIS utilization status, and related factors in public health facilities in the Mogadishu Municipality, Somalia.
Methods and materials
Study setting
The study was conducted in Mogadishu, the capital city of the Republic of Somalia. The city is neighbors middle Shabelle in the east, lower Shabelle in the west, middle Juba in the south, and middle Juba in the north. According to central statistics, Somalia has an estimated population of 12,316,895. An estimated 2,806,787 Somalis live in rural areas, and 5,216,392 (or about 42% of the total population) live in urban areas. Around a quarter of the population—3,186,965—comprise of nomads. 13 Mogadishu is the capital city of the Benadir Region and the city has 17 districts and has eight government Health Center, 12 general hospitals, 12 referral hospital, and above 20 private primary clinics, 10 medium and higher private clinics, and 15 private hospitals.14,15 The government has around 5000 health care workers (HCWs) in the area. Of these, around 3400 are male and 2600 are females. Health workers employed in private institutions were around 7000 and of these, 3000 are males and 4000 are females.
Study design and period
In this study, a quantitative institutional-based cross-sectional study design was employed from 08 May 2022 to 11 September 2022.
Target population
All department heads (Case Team Leaders), HIT (ICT) Experts, Pharmacy Specialists, PHCU Directors, CEOs of Hospitals, District Head office staff (or Municipal Health Department), planning Officers, Managers/Administrators, and Medical Directors working in private and public Health Facilities of Mogadishu Municipality were the source population. The ones that were specifically targeted were the ones that had direct contact with HMIS utilization.
Inclusion and exclusion criteria
Inclusion criteria
All department heads (case team leaders), HIT (ICT) professionals, pharmacy specialists, PHCU directors, CEOs of hospitals, district head office (or municipal health departments) and planning officers who worked in private and public health facilities who have worked for more than six months and worked on HMIS were included in the study.
Exclusion criteria
Department heads (case team leaders), HIT (ICT) professionals, pharmacy specialists, PHCU directors, hospital CEOs, district headquarters (or city health departments), and planning officials who were not present due to illness at the time of data collection were excluded. Health workers who were on annual leave during data collection, those who had no direct contact with HMIS use, and those who were newly hired or had less than six months of professional experience been excluded from the study.
Sample size determination
The sample size was calculated using a single proportion formula from the target population. With the assumption of a 5% margin of error and a 95% CI, Zα/2 = Critical value = 1.96, 10% nonresponse rate and design effect = 1.5. The assumption for P, for this study was 50% since no similar published research has been conducted in the study area. So, the proportion of HMIS utilization is assumed to be 50%. So, based on this:
P (population proportion) = 50% Where n = required Sample size
d = the margin error between the sample and the population = 0.05. The formula for single proportion was applied as follows using the following single proportion formula:

Sampling procedures
A multistage sampling method (two-stage) was used to select individual respondents for the study. First, representative healthcare facilities were selected from the 32 available healthcare facilities by simple random sampling (mainly by drawing lots). In this case, six hospitals and two HC were selected, then the number of respondents to be included in the study was determined in proportion to the total number of study participants in the sampling frame of the selected healthcare facilities. Finally, respondents were selected by simple random selection from the target population. The first HCW was selected by lottery, and then the next HCWs were selected at an interval.
Data collection procedures
Data were collected using a pretested structured questionnaire. The questionnaire was adopted from published studies and from the PRISM tool with reasonable modifications. 16 The questionnaire contained variables on sociodemographic characteristics, organizational factors-related characteristics, technical factors-related characteristics, and HMIS utilization status-related questions. The questionnaire was prepared and used since it is the medical language of these health facilities. It was pretested in the same place outside the sampled health facilities by the trained data collectors, and it was revised before the start of actual data collection. After all this, internal consistency was checked for data reliability.
Data were collected by five qualified data collectors, under two supervisors. The data collectors were degreed health professionals, and they were trained for two days by the principal investigator.
Data quality assurance
A pretest was conducted in nonselected adjacent health facilities of the study area on 5% 17 of respondents before final data collection. Data quality was assured by carefully looking at the relevancy of the questionnaire to the objectives of the study. The correctness of the questionnaire in its content organization, and language was checked and modified according to the needed standards, comments, and suggestions. The data collection process was reviewed by the supervisor and principal investigator daily to check for completeness, accuracy, and consistency. Whenever there were challenges, corrective measures were taken.
Data analysis
The collected data were reviewed and checked for completeness and accuracy. Data were entered into Epi info 7.2.5 and processed by the principal investigator. Data cleaning and coding was done using SPSS version 26. Analysis of different variables’ frequencies, percentages, and tables was used to summarize the data accordingly.
Statistical analysis
Descriptive statistics were used to summarize the results of the study in the form of graphs and tables. On the other hand, binary and multivariate logistic regression analyses were used to analyze and draw the relationship between dependent and independent variables to further examine the factors associated with the HMIS.
Operational definitions
HMIS utilization: The outcome variable was the proportion of HMIS utilization. Measured using core indicators identified from the PRISM tool. HMIS utilization was be measured by combining
Using HMIS for planning Using HMIS for Budget allocation Using HMIS for requisition of manpower Using HMIS for calculation of area coverage and trend analysis and presentation of indicators using charts/graphs Using for monitoring and evaluation of program to take immediate action Using HMIS for Supply management Using HMIS for regular supportive supervision The presence of feedback provided by department heads to health workers in the department Evidence on the use of information for decision-making in management Availability of Key performance indicators Using HMIS for conducting research were the indicators applied to determine the level of HMIS utilization. The mean value for the five indicators will be calculated to categorize the level of information use among study participants. Study participants who scored above mean value will be considered as “Good HMIS utilization,” or else if they scored equal and below the mean value “Poor HMIS utilization.”
18
Organizational factors. Organizational factors were assessed using “Yes” or “No” questions to questions related to the availability of infrastructure, training Behavioral factors: Behavioral factors were individual factors influencing HMIS utilization. These determinants were assessed using five Likert scales questions related to individual competence, the confidence level of HMIS tasks, motivation, attitude, knowledge, negligence, data quality checking skills, and data analysis data demands. Technical factors: Technical determinants are those factors linked to techniques and systems and were be assessed using “Yes” or “No” questions on the availability of standard indicators, guidelines report formats, tally sheets, trained person able to fill data, computer software(eHMIS, DHIS2), and IT complexity.
Ethical considerations
Written ethical clearance was obtained from the SIMAD University Research Ethics Review committee before proceeding with actual data collection on 09/08/2022 by the Ref.No.2022/IMRSU/FMHS/FR18/P070. Detailed information about the purpose, potential benefits, and side effects, the right to continue or discontinue the interview, and the aim of the study was provided to each respondents the consent was received. Each respondent was assured that the information they provide will be kept confidential and will only be used for academic research purposes. The study was conducted on the basis of respondents’ interests, and they all had the absolute right to withdraw from the study or refuse to complete any questionnaires at any time.
Results
Sociodemographic characteristics of the respondents
A total of 411 healthcare workers participated in the study with a response rate of 97.4%. Of these, 249 (60.6%) were men and 162 (39.4%) were women. The mean and standard deviation of the age of the study participants were both 32.2 ± 9.293. Regarding the age category of the respondents, 11 (2.7%) were below 20 years, nearly half of them—196 (47.7%) were between 20 and 30 years, 137 (33.3%) were between 30 and 40 years, 47 (11.4%) were between 40 and 50, and 20 (4.9%) were above 50 years (Table 1).
Sociodemographic and economic characteristics of respondents, Mogadishu public and private health facilities, 2022.
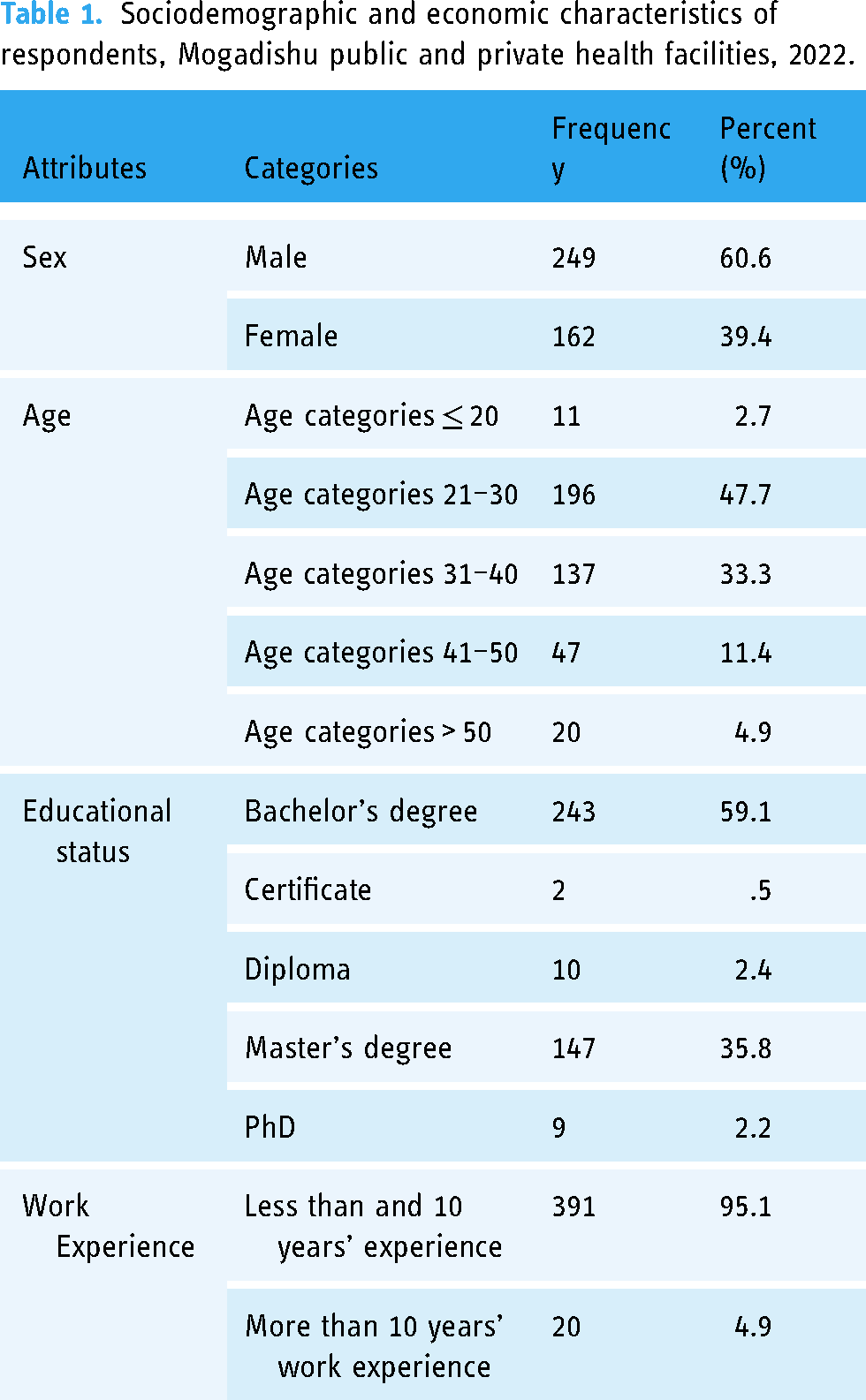
The study found that more than half of them 243 (59.1%) were has bachelor's degrees, 2 (0.5%) had certificates, 10 (2.4%) were diploma holders, 147 (35.8%) were had master's degrees, and 9 (2.2%) were PhD holders. The majority of them 391 (95.1%) had less than 10 years’ work experience, 20 (4.9%) had more than 10 years’ work experience (Table 1).
Health management information system utilization status among health workers in Mogadishu
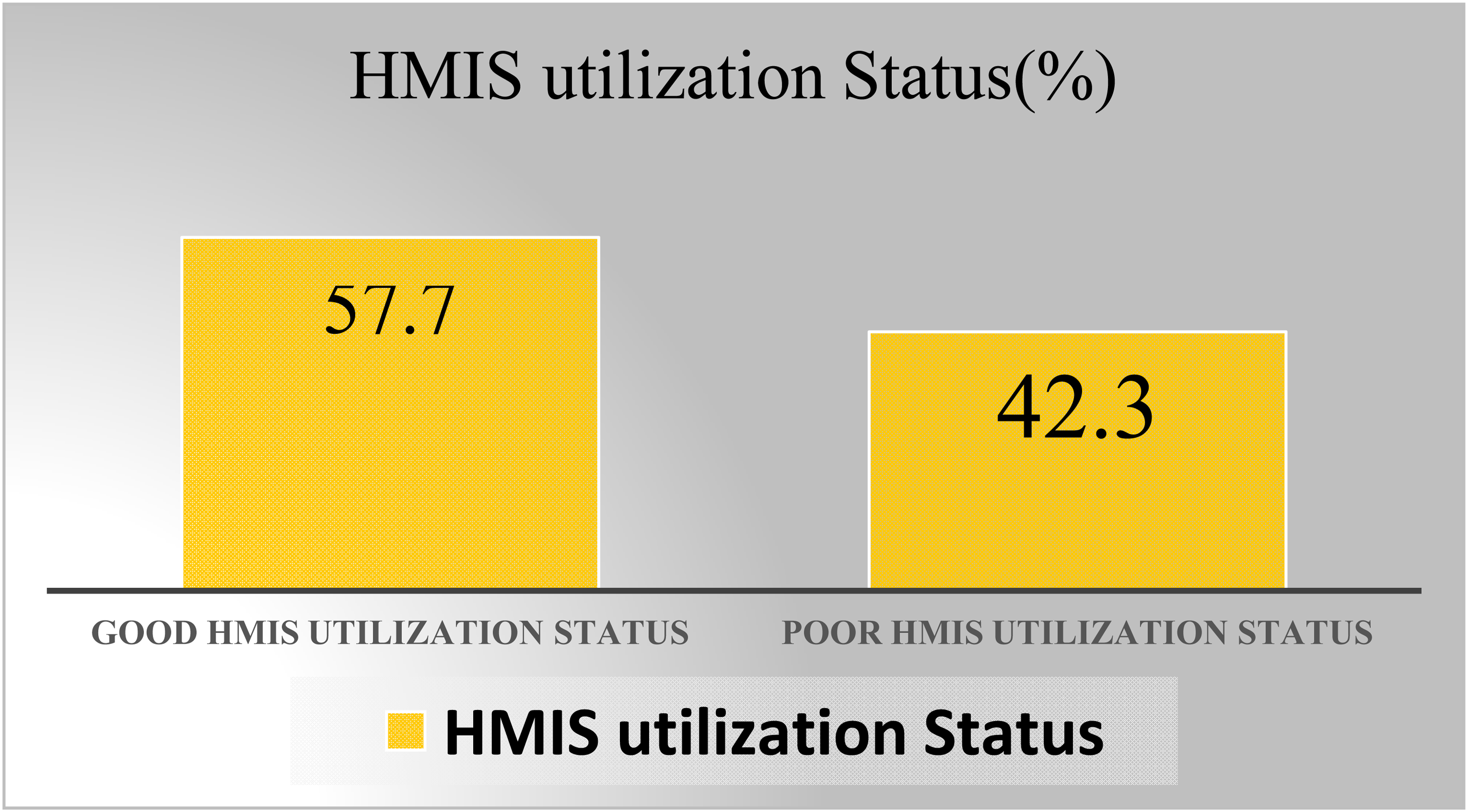
The study found that 237 (57.7%; 95% CI: 1.53–1.62) of the 411 respondents had good HMIS utilization practices (Figure 1). To assess the status of HMIS utilization, 11 questions based on HMIS utilization were prioritized and used. To assess whether they use HMIS data in preparation for planning health program activities, respondents were asked to give their opinion and 273 (66.4%) agreed that they use HMIS data in preparation for planning health program activities, while their peers 138 (33.6%) disagreed. According to respondents, more than three-quarters of respondents, 313 (76.2%), agreed that they have a key performance indicator to generate and analyze performance to make decisions, while only a few of respondents—98 (23.8%)—disagreed. On the other hand, the study participants were asked whether their offices/departments use HMIS data to calculate indicator coverage and trend analysis and to display indicators using charts/graphs, and the majority of them 250 (60.8%) assured that they officially use indicator coverage and trend analysis for calculation and to display indicators using charts/graphs, while the remaining 161 (39.2) did not (Table 2).
Infection prevention status among health workers working in public and private health facilities in Mogadishu.
HMIS utilization status of health workers working in public and private health facilities of Mogadishu, Somalia, 2022.

Health management information system is useful to improve the monitoring and evaluation of programs and based on this, respondents were asked whether they use HMIS for the monitoring and evaluation of programs in their case team. More than half of them, 261 (63.5%) demonstrated that they use HMIS data for monitoring and evaluation, while the remaining 150 (36.5%) indicated that they do not use HMIS to monitor and evaluate programs (Table 2). The other benefit of HMIS data is simply to measure the performance of activities and provide feedback to healthcare workers, departments, and teams. In this context, respondents were asked if HMIS is used to provide feedback to healthcare workers, departments, and teams, and the majority of them, 252 (61.3%), answered yes, while 159 (38.7%) answered that HMIS is not used to provide feedback to health workers, departments/teams (Table 2).
On the other hand, HMIS data is useful to perform integrated supportive supervision to health workers, departments/teams, and respondents were asked to indicate whether the HMIS is used to perform regular supportive supervision to health workers, departments, and teams. More than that half of them, 243 (59.1%) agreed that HMIS would be used provide supportive supervision to respective healthcare workers, departments, and teams, while 168 (40.9%) disagreed with the idea (Table 2).
In addition, HMIS data is useful for requesting budgets to allocate budgets for healthcare programs during planning. In this context, study participants were asked if they use HMIS data for budget request/budget allocation and more than half of them 237 (57.7%) agreed that they use HMIS data for budget allocation and the remaining 174 (42.3%) did not agree with this idea (Table 2).
The other purpose of HMIS data is to estimate and request manpower to fill the human resource gaps to implement health-related deprograms. The majority of respondents, 238 (57.9%) agreed that they use HMIS for manpower requisition and 173 (42.1%) didn’t share this idea (Table 2).
On the other hand, HMIS helps to assess the availability of supply (supply management) in healthcare facilities. In this study, this issue was raised as a question and 262 (63.7%) agreed that HMIS is useful to assess the availability of supplies, while 149 (36.3%) disagreed (Table 2).
The other important aspect of HMIS is that it is useful in conducting research to solve public and private health problems. Study participants were asked if they use HMIS data to conduct research to solve public and private health problems and 259 (63%) answered yes, while 152 (37%) answered “no” (Table 2).
Organizational factors associated with HMIS utilization
To assess the organizational factors affecting HMIS utilization, 19 organizational factor-related questions were used. Health management information system needs the responsible HIT/ICT experts deployed to handle HMIS-related activities. The study showed that almost three-quarters of the study participants 301 (73.2%) assured that there is a HIT/ICT expert involved in the HMIS activities, while the remaining 110 (26.8%) of the study participants did stated that there is no dedicated HIT/HMIS expert (Table 3).
Organizational factors affecting HMIS utilization among private and public health facilities of Mogadishu, Somalia, 2022.

Health workers should be supported by senior managers to improve data analysis and use for decision-making. Based on this, 328 (79.8%) of the study participants confirmed that they could get support from their manager, while 83 (20.2%) did not (Table 3).
Those who reported receiving support from their senior managers were asked to explain the type of support they receive and 87 (21.2%) reported receiving support from their manager regarding the data collection tool, 50 (12.2%) receive supportive supervision, 33 (8%) receive resources for a review meeting, 148 (36%) attend on job training, 58 (14.1%) receive funding for HMIS activities, and 35 (8.5%) receive support for data quality audits from their senior managers (Table 3).
The other organizational factor affecting the use of HMIS is the availability and use of the HMIS guideline. Respondents were asked if they have an HMIS guideline in their department/office. A total of 324 (78.8%) affirmed that they have an HMIS guideline on information use in their department, while 87 (21.2%) stated that they have no HMIS/information use guideline in their department or office (Table 3).
Health information systems that include HMIS should be well planned in the annual and strategic plan of the health care facilities. To know if healthcare facilities are planning HMIS, study participants were asked and a majority of them 297 (72.3%) confirmed that HIS/HMIS is planned and 114 (27.7%) said that there is no plan for HMIS in the annual and strategic plan (Table 3).
The other very important manual is the HMIS/HIS standard operations manual. According to the study, 263 (64%) offices/departments have a standard HMIS operations manual, while 148 (36%) confirmed the lack of a standard manual. Health workers are expected to keep copies of monthly/quarterly/annual reports and 260 (63.3%) reported having a copy of the reports while 151 (36.7%) reported no copy of the reports to have (Table 3).
The organization is expected to organize training for employees on how to use HMIS/HIS information to implement the HMIS well, and 245 (59.6%) of the respondents ensured the availability of training, while 166 (40.4%) did not (Table 3).
Supportive supervision is very important to support health workers in using HMIS and improving the performance of their activities. On this basis, this study found that 240 (58.4%) of the respondents had ever received supportive supervision for HMIS/HIS to improve their activities, while 171 (41.6%) confirmed that they had not received supportive supervision for received HMIS/HIS (Table 3).
The fundamentally important tool that must be used to implement HMIS is the computer dedicated to the work of HMIS/HIS and healthcare workers should have access to it. However, in this study, 271 (65.6%) of study participants ensured the availability of computers for HMIS/HIS work, while 140 (34.1%) indicated that no computer was provided for HMIS/HIS work (Table 3).
On the other hand, budget is very important to facilitate the implementation of HMIS and it should be allocated. Two hundred and two (49.1%) ensured that adequate budget was allocated for HIS/HMIS activities, while more than half of the study participants agreed that there was a lack of budget for HMIS activities (Table 3).
The HMIS/HIS work depends on the availability of the internet connection, and the organization is expected to use the internet connection to facilitate the good work of the HMIS/HIS work. More than half of the study participants, 287 (69.8%) confirmed the availability of an internet connection, while 124 (30.2%) reported the lack of an internet connection to perform HMIS activities (Table 3).
On the other hand, since HMIS is dependent on the computer, light is very important to run the computer's programs. According to 293 (71.3%) respondents there is a light for HMIS/HIS work, while 118 (28.7%) said it is a challenge to get light for HMIS work (Table 3).
Employee motivation by providing incentives is very important to improve the implementation of programs like HMIS. A total of 197 (47.9%) confirmed the availability of incentives/rewards for the workers, while more than half of the study participants 214 (52.1%) claimed that there is a lack of incentive/reward for the good work of the health workers in the field of HMIS-Implementation (Table 3).
In order to fully implement the use of HMIs components, there should be a performance monitoring committee that regularly reviews performance. This study found that 264 (64.2%) of the study participants appreciated the availability of the performance monitoring committee, while 147 (35.8%) confirmed the lack of a performance monitoring team (Table 3).
One of the components of data quality management is storing data for further use, and HMIS needs to pay special attention to data storage. However, 164 (39.9%) of the respondents have no data storage/power bank devices, while 247 (60.1%) have devices to store HMIS data (Table 3).
One of the meanings of HMIS utilization is the presentation of data, and health workers of the respective departments are expected to display data in charts/graphs and 257 (62.5%) confirmed that the activity performance in their office/department analyzed and displayed (represented in graphs/charts, while the rest of the respondents 154 (37.5%) did not (Table 3).
HIS/HMIS needs the culture of using data for decision-making and 262 (63.7%) of the respondents have evidence of the culture of using information for decision-making (minute books, feedback, reports, documents), while 149 (36.3%)) did not (Table 3).
The technical factors associated with HMIS utilization
Nine technical-related factors were assessed using technical-related questions. These technical factors are related to the technical skill of the health workers regarding HMIS utilization. Health management information system needs computer applications like District Health information (DHIS2) or electronic health information (eHMIS) in order to enter data, store, aggregate, analyze, and display data. In this study, it was identified that 269 (65.5%) study participants confirmed the availability of computer application software's, while 142 (34.5%) confirmed that there is no dedicated computer applications/software's for HMIS in their department (Table 4).
Technical factors affecting HMIS utilization among public and private health facilities in Mogadishu, 2022.

The other technical factor affecting the implementation of HMIS is the ability of healthcare workers to analyze and use data to accelerate evidence-based decisions. In this context, respondents were asked to rate their ability to analyze data and use information, and the result shows that more than half of the study participants 322 (78.3%) confirmed that they are able to analyze and use data use, while the remaining 89 (21.7%) indicated that they are unable to analyze and use data (Table 4).
Those who responded having analytical skills responded that 117 (28.5%) had computer application skills such as MS-Word, Excel, and Microsoft Powerpoint, 42 (10.2%) had data analysis skills in addition to computer skills, 136 (33.1%) have computer skills, data analysis skills, and planning skills, the other remaining study participants reported having the skills to use HMIS data 116 (28.2%) (Table 4).
Those respondents who had data analysis skills were also asked if they could perform data analysis on the data they collected, and 327 (79.6%) of them use their data analysis skills and 84 (20.4%) do not. In addition, respondents who can perform data analysis asked how they analyze data and 104 (25.3%) use manual methods of data analysis, 67 (16.3%) use eHMIs, 73 (17.8%) use DHIS2, and 167 (40.6%) use computer programs (Table 4).
Regarding capacity building, respondents were asked if they had received training on HMIS and computer software such as DHIS2, eHMIS, and the study found that 271 (65.9%) had received training on HMIS and software, while 140 (34.1%) did not (Table 4).
Standard indicators are the necessary component of HMIS, and program managers and healthcare workers are expected to use standard indicators to correctly calculate and process data. In this context, study participants were asked whether they use HMIS indicators and 275 (66.9%) indicated that they use standard indicators to calculate and process data correctly, while their peers did not (Table 4).
The other technical part of HMIS utilization uses the available HMIS guidelines and 282 (68.6%) use the guidelines and 129 (31.4%) do not use the guideline. On the other hand, the use of tally sheets, report formats, charts, and other recording tools is mandatory and according to respondents, 276 (67.2%) use these tools while 135 (32.8%) did not (Table 4).
Individual factors (behavioral factors) influencing HMIS utilization
The other factors affecting HMIS implementation are individual factors. To assess these individual (behavioral) factors, five Likert-scale form questions were selected and used to assess the behavioral factors influencing HMIS implementation.
To determine respondents’ confidence in performing HMIS-related activities such as data entry, analysis, and interpretation, study participants were asked to rate their confidence, and 56 (13.6%) agreed that they do so able, 53 (12.9%) disagreed, 126 (30.7%) were neutral to rate their confidence, and 150 (36.5%) agreed that they have confidence, 26 (6.3%) strongly agreed that they are confident in HMIS-related activities such as data entry, analysis, and interpretation (Table 5).
Individual factors (behavioral factors) influencing the HMIS utilization among public and private health facilities in Mogadishu, 2022.

On the other hand, respondents were asked to rate the level of motivation to create and retain health information for use, and some of them rated it as very low (7.3%), 98 (23.8%) rated their motivation as low, 123 (29.9) rated them as moderate, 129 (31.4%) rated them as high and the remaining 31 (7.5%) rated their motivation as very high (Table 5).
In terms of knowledge to perform HMIS-related activities such as data entry, analysis, and interpretation, the study showed that 20 (4.9%) of study participants reported having very low knowledge, 14 (36%) low, 117 (28.5%) moderate, 95 (23.1%) high, and 31 (7.5%) very high (Table 5).
The other individual factor influencing HMIS utilization is the attitude of healthcare workers, and this study also found that 310 (75.4%) had a positive attitude toward performing HMIS-related activities such as data entry, analysis, and interpretation, while 101 (24.6%) have negative attitudes (Table 5).
The other very important factor influencing HMIS utilization is healthcare workers’ satisfaction with the incentives/rewards they receive for doing good work in the HMIS/HIS, and 17 (4.1%) reported that they were very dissatisfied, 81 (19.7%) dissatisfied, 123 (29.9%) rated their satisfaction neutrally, 159 (38.7%) satisfied, and 31 (7.5%) were very satisfied with the incentives (Table 5).
Factors associated with the infection prevention practice
Bivariate logistic regression and multivariable analysis were carried out to determine independent predictors of HMIS utilization. Those candidate variables with a p-value <0.25 in bivariate logistic regression were included in the multivariable logistic regression model and considered significant in the model at a p-value <0.05 (Table 6).
Multivariate analysis of factors associated with HMIS utilization among health care workers working in public and private health facilities in Mogadishu, 2022.

A result of bivariate logistic regression applied to identify significant independent variables showed that HMIS utilization was significantly (p < 0.25) associated with staff motivation, training on HIS/HMIS, skills to use HMIS data, utilizing HMIS data for decision-making, using HMIS planning purposes, having standardized indicator in office/department, having standard HMIS procedure, receiving feedback, support from manager, and using report formats/tally sheets. However, in the multivariate logistic regression analysis, training on HIS/HMIS, skills to use HMIS data, having standardized indicator in office/department, receiving feedback, support from manager, and using report formats/tally sheets were found to have a significant association with HMIS utilization practice (Table 6).
The study found that those HWs who did not receive feedback from managers to improve data analysis and use for decision-making were 67.5% less likely to use HMIS well (AOR = 0.325, 95% CI: 0.149–0.707) compared to those supported by their managers. The odds of HWs who did not have an HMIS standard operating procedures manual in their office/department were 79% less likely to use HMIS (AOR = 0.210, 95% CI: 0.105–0.421) compared to those who have HMIs standard—Have operating procedures manual. Healthcare workers who had not received HMIS training were 60.9% less likely to use HMIS (AOR = 0.391, 95% CI: 0.200–0.764) than those who had HMIS/ completed HIS training. Health workers who did not receive regular supportive supervision were 69.5% less likely to use HMIS (AOR = 0.432, 95% CI: 0.218–0.856) than those who did receive regular supportive supervision received (Table 6).
On the other hand, those who did not have data storage devices were 67.5% less likely to use HMIS (AOR = 0.305, 95% CI: 0.154–0.603) compared to those who have storage equipment in their office (Table 6).
The odds of those who did not perform office/department activity performance analysis and display were 84.5% less likely to use HMIS (AOR = 0.155, 95% CI: 0.078–0.307) in comparison to her colleagues. Those with the skills needed to analyze and use data and information to aid in decision-making were 91.1% less likely to use HMIS (AOR = 0.089.95% CI: 0.042–0.185) compared to their peers.
Those who did not use standard indicators to correctly calculate and process data were 74.3% less likely to use HMIS when using HMIS data (AOR = 0.257, 95% CI: 0.129–0.514) compared with those that used standard indicators for correct calculation and process data. The likelihood of using HMIS among those who did not use tally lists, report formats, graphs, and charts to record, report, and view data was less likely to use HMIS compared to their counterparts (AOR = 0.227, 95% CI: 0.111–0.461) (Table 6).
Discussion
The study found that 237 (57.7%) (95% CI: 1.53–1.62) of 411 respondents among health professionals working in public and private health facilities in Mogadishu, Somalia, had good HMIS utilization practices. The finding is higher compared to the study conducted in Addis Ababa (Ethiopia) which found that the utilization rate of HMIS in health centers was 41.7%, 19 and the other study, conducted in Addis Ababa, Ethiopia, showed that the rate of routine use of health information among health professionals was 37.3%. 20 It is also higher compared to studies that have shown that its use is low in developing countries and varies from 27% to 69.6% in Africa. 8 On the other hand, the result of this study is found to be lower compared to the study conducted in Tanzania to assess information utilization and factors affecting the performance of HMIS implementation system showed that 60% of the institutions surveyed responded that they use HMIS data for decision-making 21 and lower compared to the study conducted in Uganda, Luuka District, evaluating the use of the HMIS system by the Health Unit Management committee that it was reported that 94% of the study participants confirmed that information generated by patients in the different health units used by the committee to plan, monitor, and inform is well-managed and the effectiveness of using HMIS is moderate. 22 It also differs from the study conducted at Muhimbili National Hospital in Tanzania, which found 61.6% of routine health data for decision-making with an interaction of individual skills. 23 The discrepancies between the studies could have been resulted due to the difference in study design, source population, and difference in focus of managers to sustain HMIS utilization.
In this study, those who did not perform activity performance analysis and display in the office/departments were found to be 84.5% less likely to use HMIS (AOR = 0.155, 95% CI: 0.078–0.307) compared to their counterparts. This result contrasts with the study conducted in the Amhara region of north-western Ethiopia, which showed that department heads using HMIS to display their performance were 12.42 times more likely to use the health management information for decision-making compared to those not display HMIS data in their office. Managers who displayed performance data for monitoring and provided data quality feedback to health professionals were 2.29 times more likely to use information to make decisions than their counterparts who did not. 18 The difference may have arisen from the difference in study area, time and ability of healthcare workers to use HMIS for further decision-making.
This study also found that the odds of good HMIS use among the HWs who did not receive feedback from managers to improve data analysis and use for decision-making (AOR = 0.325, 95% CI: 0.149–0.707) were 67.5% lower to those supported by their managers. This finding is inconsistent with the other study conducted in the eastern part of Ethiopia which found that managers who provide regular feedback to their employees were 2.42 times more likely to use HIS and managers who provide feedback to employees, were significantly associated with HIS. 24 The differences in the results of the study could be due to the difference between the managers’ obligation to provide regular feedback to their respective healthcare professionals on the use of HMIIS for decision-making, and the other reasons could be due to a lack of similarities in the feedback mechanism between the study areas.
The other finding of this study is that those who did not use standard indicators to correctly calculate and process data were 74.3% less likely to use HMIS compared to (AOR = 0.257, 95% CI: 0.129–0.514) those who use standard indicators to correctly calculate and process data. This finding contrasts with the study conducted in eastern Ethiopia, which examined factors associated with low health information utilization in a resource-constrained setting, and health departments with a standard indicators were 2.39 times more likely to use HIS compared to those lacking standard indicators. 24 The difference between the study could be due to the lack of standard indicators and the managers’ lack of commitment to make standard indicators available in all departments of the health care facilities. The other reason could also be due to the different attitude of health workers to use standard health indicators.
On the other hand, it was also found that education is the factor affecting the effective use of the HMIS. According to this study, healthcare professionals who had not received HMIS training were 60.9% less likely (AOR = 0.391, 95% CI: 0.200–0.764) to use HMIS compared to those who had HMIS/HIS—Completed training. This study also disagrees with the study conducted in Cameroon, which showed that healthcare professionals who received training on HIS were 3.33 times more likely to use HIS data than those who did not receive training. 25 The differences could result from differences in the study area, differences in healthcare system settings, and the lack of adequate resources for training healthcare workers in HMIS.
Conclusion
The result of this study shows that the extent of HMIS utilization among health workers working in public and private health facilities in Mogadishu is low compared to other studies conducted in other areas 237 (57.7%). The study found that training on HIS/HMIS, skills in using HMIS data, standardized indicator in office/department, receiving feedback, support from manager, and use of report formats/lists had a significant correlation with the practice of HMIS utilization exhibit. All concerned bodies should work hard to fill the gaps identified in this study.
Recommendation
To all levels of hospital administrations, health offices, and the Ministry of Health
The Ministry of Health and health institutions should commit to train staff on HMIS, use guidelines and HMIS tools, provide feedback and supportive supervision, motivate health workers, and allocate budget to improve the HMIS and health system. Healthcare workers working in various departments (case teams), records office staff (registration staff), health information technicians, health management information department staff, planning officers, CEOs and department heads, and performance monitoring team members should be personally trained (face to face training) in HMIS and health information utilization, data quality, and the use of HMIS tools and applications. In addition to training, the Ministry of Health should strengthen on-site mentorship, integrated supportive supervision, and data quality assurance activities to identify gaps and take corrective actions. There should be a performance monitoring team tracking the implementation of HMIS in all healthcare facilities and Health bureaus. The role of leaders in changing the status of HMIS use by identifying gaps and taking corrective action through the development of policies, strategies, and guidelines is critical, and all levels of leadership concerned, from the Ministry of Health to the health unit lower level, should work synergistically to improve the use of HMISs. Finally, the various levels of health sector management, health workers, and stakeholders should use the results of this study as a starting point for improving HMIS use.
To all HCWs working in public and private health facilities
Healthcare workers should work to fill the gaps identified in this study by improving their skills in using HMIS data for evidence-based decision-making in healthcare settings.
To researchers and scholars
Researchers should use the findings of the study as a starting point and focus in advance on the factors associated with HMIS and health care system, and further studies should be conducted to learn more about the factors affecting the practice of using HMIS among health workers in public and private Affecting healthcare facilities as no adequate studies have been conducted in Somalia.
Additional points
Strength of the study: This research can help health professionals, hospital CEOs, health service managers, the Ministry of Health, and other sectors to focus on HMIS-related factors. Because the information was collected by healthcare workers, it helps to improve health management information strategies. Data were collected from trained government health workers and the private health sector who voluntarily completed a self-administered questionnaire. Data collection and data entry were strictly supervised, and analysis and cleanup were carefully performed using the latest versions of computer applications, SPSS version 26.
Limitation of the study: The study aimed to determine all aspects related to using HMIS among health workers in public and private health but was not exhaustive and other factors might exist that were not discovered well in this study. Some associated factors could not be compared to other studies due to the lack of similar studies. The other drawback of the study is that there were not enough comparable studies in Somalia and the study area to use as a literature review and therefore it was difficult to make comparisons. The study included government health facilities and private health facilities this may limit the inference to the general health workers in Mogadishu.
Footnotes
Acknowledgements
The author gratitude goes to Public and Private health facilities who allowed to conduct the data thanks to SIMAD University for providing me with Ethical approval. The author special thanks go to all my data collectors, supervisors, respondents, and coworkers.
Contributorship
The authors contributed significantly to the work of this study and the correspondent participated in its drafting, revision/review. All authors agree to be responsible for the content of the work. The agreement was made with the journal to which the article was sent for publication.
Data availability
The data used to support the findings of this study are available and can be accessed from the primary author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable; no human subjects involvement.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.