
Abstract
Background
Emerging evidence suggests that virtual reality (VR) technology can potentially improve the wellbeing of older adults living with dementia in hospital care units. Nevertheless, older patients are often excluded from VR opportunities. Meaningful engagement of patient partners, family caregivers, staff, and care leaders is needed to ensure the appropriate development and implementation of these programs.
Objective
To understand the expectations of patient partners, families, staff, and care leaders regarding development and implementation of a VR program for patients with dementia in hospitals.
Method
Drawing on principles of Collaborative Action Research and underpinned by the Person-Centred Framework, we conducted qualitative focus groups and interviews with 42 individuals including 7 patients, 9 family members, 17 frontline staff members and 9 organizational leaders.
Results
We performed a thematic analysis and identified three interconnected themes: (1) anticipating positive functions and outcomes, (2) considerations on VR program implementation, and (3) desired VR features for patients with dementia.
Conclusion
This study explored multiple partners’ needs and priorities on a VR program in hospitals, emphasizing the pivotal role of multipartner collaboration and supportive care environment essential for delivering a person-centred VR experience. Future studies are recommended to further the investigation by deploying and evaluating a person-centred VR program for patients with dementia in hospital settings through collaboration with multiple partners.
Keywords
Introduction
Dementia encompasses a range of cognitive and functional impairments, including loss of memory, language, problem-solving, and other thinking abilities that lead to interference with daily life. 1 Dementia is a general term that includes Alzheimer's disease, vascular dementia, and Lewy Body dementia. 1 By 2050, dementia is expected to affect 152 million people worldwide 2 and more than 1.7 million Canadians. 3 This population has been highlighted as a global health priority by the World Health Organization. 4 People with dementia are more likely to be admitted to hospital, 5 have an extended length of stay, 6 and experience decline during their hospital stay 7 compared with their counterparts without dementia. The hospital environment can exacerbate symptoms of anxiety, depression, and distress, often leading to risky physical and verbal behaviors that result in costly injuries for staff and patients. 8 Further, although hospital staff often aim to achieve care goals, they are generally overloaded with work and provided with limited resources to address patients’ complex needs and improve their overall wellbeing.9–11 The challenges in hospital dementia care units are potential reasons for lower satisfaction among family caregivers and staff. 12
Emerging studies have indicated that technologies, such as virtual reality (VR), are promising nonpharmacological interventions for patients in hospital settings. 13 VR uses various types of equipment to simulate a reality in which the user is immersed in a virtual environment, creating a sense of physical presence. VR experiences are typically delivered through headsets, goggles, or projectors, which provide varying levels of immersion and accessibility.14,15 A growing body of literature has reported implementing diverse VR programs with different types of VR equipment in institutional care settings. For example, Hung et al. 16 conducted a scoping review focusing on facilitators, barriers, and desired resources for the implementation of VR programs for older adults, particularly those with dementia. Other studies have shown the potential for VR programs to benefit patients with dementia in hospitals in different ways, including enhancing cognitive function and emotional wellbeing, reducing anxiety, and improving mood among dementia patients.16–19 Importantly, although the literature addressing the psychological and social needs of hospitalized patients with dementia through VR remains limited, evidence suggests that VR can help address these needs by enabling patients to relive positive memories, explore calming scenarios, and engage in meaningful activities that are otherwise inaccessible.20,21
Despite potential benefits, there are shortcomings in the current approaches to VR development and delivery for older adults to address their needs, especially for patients with dementia in hospitals to improve their wellbeing. First, the current industry-dominated technology development model overlooks contextual complexity in implementation and fails to make improvements for adoption. 22 Second, diversity in the Canadian population has been observed among people living with dementia, 3 family caregivers, 23 and staff 24 in terms of demographic features such as ethnicity, gender, and socioeconomic status. However, most of the VR content available in the market is predominantly based on Western culture, 25 and limited literature has addressed cultural sensitivity in developing and implementing this technology.25,26 Third, older adults are often subjected to ageism, and assumed to be uninterested in technology and reluctant to try new ones. 27 VR studies should focus more on older adults, especially those living with dementia, to better understand the population's experiences. 28 Lastly, some studies have reported concerns about implementing VR programs and handling the technological complexity in clinical settings, including a lack of resources (e.g. human and financial resources) and designated space, which may make VR prohibitive for many healthcare institutions.16,29
There is an urgent need to address the above-mentioned challenges and explore how VR programs can best be implemented for patients with dementia in hospital settings. One critical gap is the limited understanding of the expectations of diverse partners, including people living with dementia, family caregivers, staff, and care leaders. Existing literature has rarely captured the expectations and insights of these partners regarding the development and use of VR in acute care environments. Without this input, VR programs risk being underutilized, misaligned with user needs, or culturally insensitive. These partners have localized knowledge, expertise, and experiences in VR program delivery to the focused population in the hospital. 30 Collaborating with these partners has been recommended, as understanding expectations from their diverse perspectives can make a VR program more relevant, inclusive, and tailored to address the needs of patients and their informal and formal caregivers. 30 For example, patient partners provide invaluable insights into their needs, preferences, and experiences. 31 This study addresses this gap by exploring diverse perspectives to inform the co-development of a relevant, inclusive, and feasible VR intervention for hospitalized older adults with dementia. The study can potentially contribute by increasing the use of VR technology, reducing abandonment, and ultimately improving patients’ wellbeing during hospitalization. 12
Another research gap is the uniqueness of hospital settings where VR programs will be delivered for older patients with dementia.13,32 Existing literature mainly focuses on VR programs in long-term care (LTC) homes. 16 Hospital environments and care protocols can differ significantly from those in LTC homes, as the former are generally designed for acute care services, in which a patient receives active but short-term treatment. 33 The nature of acute care makes it difficult to deliver VR programs that address the specific needs of individuals with dementia, which can potentially compromise their wellbeing.34,35 Common issues in hospital design, such as unclear signage, poor lighting, clutter, limited space for family visits, and few opportunities for engaging in meaningful activities, lead to confusion, agitation, and anxiety in patients with dementia.36,37 Additionally, the fast-paced nature of acute care environments influences staff attitudes toward the care of individuals with dementia, leading to excessive monitoring and a diminished emphasis on meaningful interactions. 38 Due to heavy workloads and a lack of resources, staff often find themselves prioritizing immediate medical needs over the emotional and social dimensions of dementia care. 12 Also, patients’ median hospitalization period in Canada is 8 days, 39 which means staff have a relatively short time to build relationships with patients, learn more about them, and identify efficient approaches to improve their wellbeing. 12 A shorter period of hospitalization also means the challenge of gaining a reasonable understanding of patients’ psychosocial needs. 10 This study can provide hospital-specific, dementia-focused insights to support staff in 'delivering VR, improve their work experiences, and provide more person-centred care to patients with dementia.
Theoretical foundation
We chose the person-centred framework by McCormack et al. 40 to inform our study (see Figure 1) and address our research objectives. The framework emphasizes treating patients as individuals with unique needs, preferences, and values. It highlights that a person in care delivery refers to “all those involved in a caring interaction and therefore encompasses patients, clients, families/carers, nursing colleagues, and other members of the multidisciplinary team.” 41 Hence, the framework forms the underlying foundation for our study as it clarifies the necessity of engaging in a comprehensive partnership to investigate their expectations about a VR program. Relevant partners in this context include patient partners, family partners, staff, and care leaders.

Person-centred framework, McCormack and McCance (2006).
Furthermore, to acknowledge personhood in care delivery and implementation, the theory focuses beyond a person-centred process and expected outcomes, which are mostly carried our by individual staff members. 40 The framework highlights the significance of environmental factors, including prerequisites and the care environment, in developing person-centredness in care practice.41,42 In other words, changes in service delivery are required at “individual, organizational and strategic levels.” 42 Therefore, in our context, the framework can be used as a tool to acquire insights into the complexity of hospital settings, identifying dynamics and factors that shape the VR program delivery at environmental and structural levels. Lastly, as Canada embraces multiculturalism, 43 VR technology is expected to address the individual needs of patients with dementia, aligning well with the philosophy of person-centred care and challenging the traditional one-size-fits-all model. 40 A person-centred framework can also guide us in applying a lens of equity, diversity, and inclusivity 44 to develop and implement VR programs serving multicultural populations in countries like Canada.
Research objectives
The study aimed to understand the expectations of a VR program in hospitals for patients with dementia from the perspectives of patient partners, family caregivers, staff, and care leaders. The study also aimed to understand the psychosocial needs of older adults with dementia in hospitals and how VR could be best implemented in a complex clinical setting.
Methods
We adopted collaborative action research (CAR) to inform this qualitative study. Aiming for knowledge co-production for change, CAR is a research methodology that engages relevant partners in understanding a practice and a social process. 45 CAR is appropriate for our study for two reasons. First, CAR involves a dynamic and iterative cycle of planning, acting, observing, and reflecting. 45 The cycle can guide us in understanding the needs of relevant partners, which can inform improvements in the subsequent action. Results from the pre-intervention focus groups reported in this article can inform future VR program co-creation and delivery. Second, the value-based principle in CAR guides us in engaging multiple parties to understand and co-design interventions.16,46–48 The value-based principle refers to the commitment to respect, justice, equity, diversity, and inclusion for all partners involved in the research.
CAR addresses and challenges the traditional power dynamics in research and care practice, and enhances the richness and depth of understanding of our research topic.45,49 CAR also enables the incorporation of a lens of equity, diversity, and inclusion to ensure the participation and representation of diverse partners in collaboration, especially those who have been underrepresented and traditionally disadvantaged. 50
Study design and procedures
This qualitative study was conducted through data collection activities, including focus groups, observations, field notes, and regular multipartner research meetings (weekly and monthly). Each method was chosen for its specific benefits in gathering comprehensive insights. Focus groups facilitated dynamic discussions among participants, encouraging the exchange of ideas and experiences from various partners. 51 Field notes recorded observations and reflections in real time, adding contextual depth to the data. 52 Our regular meetings enabled discussion and reflection on research findings, ensuring future actions are aligned with the study's objectives. 53 To ensure rigor, we consistently engaged multiple partners during our research meetings. The research team benefits from this process by challenging each other's assumptions and biases and gaining a comprehensive understanding of the co-creation and delivery of VR. All research processes were meticulously documented and reported according to the Consolidated Standards for Reporting Qualitative Research (COREQ) by Tong et al 54 (see Appendix 1).
This study was approved by the University of British Columbia Research Ethics Board and the local health authority (REB number: H23-01008). All participants provided written consent. Pseudonyms were used for all participants in this article, except Dr Jim Mann, who preferred to use his real name in results.
The research team
Our team consists of a patient partner, two family partners, four care leaders, and multidisciplinary researchers. Patient partner JM is a person with living experiences of dementia. Family partners LW and CW are informal caregivers of their family members living with dementia. Care leader KS has frontline and managerial experience in dementia care delivery in a hospital. Senior researchers LH, BM, AL, and JB are from backgrounds including nursing, occupational therapy, computer science, and engineering. The Principal Investigator LH, a professor of nursing, supervised multidisciplinary trainees including LR, SK, CW, and GL in data collection and analysis.
Recruitment of participants
We recruited participants using purposive and snowball sampling. To maximize the heterogeneity and diversity among the participants and capture a wide range of perspectives and needs, this study included participants from different demographic backgrounds regarding ethnicity, age, and gender. As this was a qualitative study, we did not conduct a formal sample size calculation. Instead, our goal was to ensure representation across key groups and perspectives. See Table 1 for the inclusion criteria of patients, family caregivers, and frontline staff.
Inclusion criteria for patient partners, family caregivers, frontline staff, and care leaders.

Data collection
Data were collected between October 2023 and March 2024 in two dementia care units of a hospital in Western Canada. Supervised by LH, multidisciplinary trainees (LR, SK, and CW) facilitated the focus groups on different days to accommodate different partners’ availability. Sessions that were mainly attended by patient partners and family partners were conducted in a community-based conference room, whereas sessions for staff and care leaders were held in conference rooms within the hospital building. The locations and environment of these conference rooms were chosen to be comfortable and mutually convenient for all participants to experience VR.
Given the vulnerability of participants living with dementia, safety precautions were taken during VR use. Before the focus groups, senior researcher LH trained all trainees in measurements and practical skills to address safety and ethics in VR delivery. Other senior researchers BM, AL, and JB, patient partner JM, family caregivers, care leaders, and staff members provided feedback in preparation for each focus group during our regular meetings. We ensured that each participant was supported by staff, family caregivers and trainees when using the equipment. Ethical considerations related to VR delivery will be discussed in a separate paper.
In the focus group, the research team explained the purpose and agenda of the study and played videos of immersive experiences delivered through three-dimensional (3D) VR goggles and two-dimensional (2D) projectors (see Figure 2). Then, students offered participants the opportunity to watch four videos with different themes with VR goggles (i.e. see Figure 3). These videos were co-produced by students and a patient partner using a 360 camera in locations across Metro Vancouver. The goggles used were Meta Quest 2TM. Based on their preferences, participants could watch the video(s) that interested them by operating VR goggles independently or with students’ assistance and navigating the virtual world using fingers or hand controllers.

Immersive experiences delivered through Virtual Reality goggles and projectors: (a) VR headset and (b) VR projector.
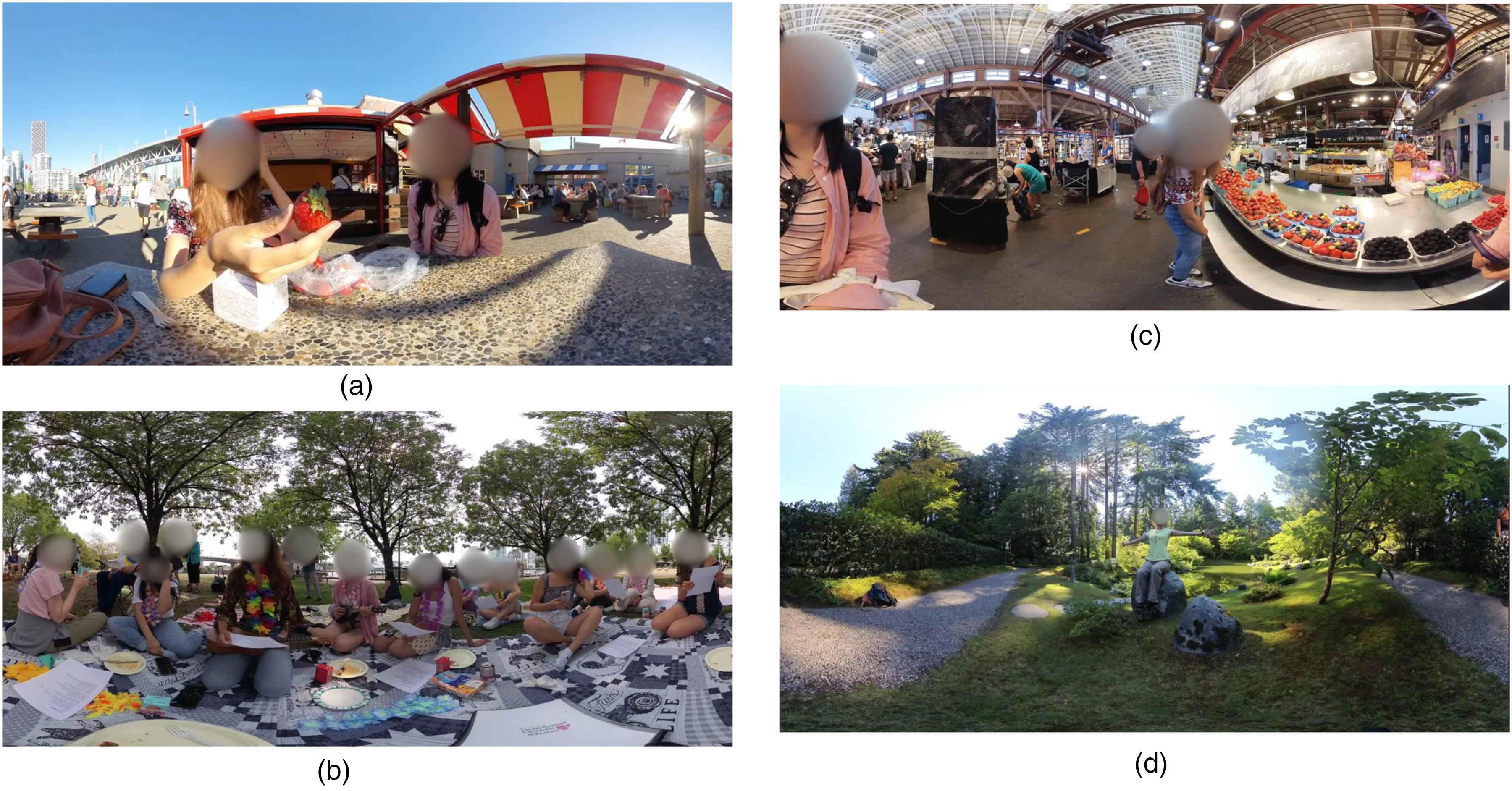
Co-produced VR videos watched by participants over Virtual Reality goggles: (a) strawberry eating video; (b) picnic video; (c) grocery shopping video; and (d) Tai Chi video.
After watching the video content for 15 minutes, we asked participants for their opinions and expectations of a VR program in hospitals for patients with dementia. Before conducting the focus group, the questions for participants were pilot-tested with patient and family partners during research meetings. Each focus group lasted between 45 minutes and an hour and had between 8 and 10 participants. Our questions for focus groups were:
What do you imagine the VR program may look like for people with dementia in hospitals? What positive experiences or outcomes do you expect?
Data collection ceased when the research team and partners agreed that the data collected were sufficient to reach our research goals. The focus groups were audio recorded and transcribed verbatim.
Data analysis
The data were analyzed using reflexive thematic analysis by Braun and Clarke, using an iterative approach.55,56 This approach facilitated the identification of key themes related to the implementation and impact of VR programs for the targeted population. The analysis aimed to uncover the psychosocial needs of patients with dementia and the factors influencing the successful integration of VR in care delivery in hospital settings. The data analysis was conducted in six steps. Step 1: Familiarization: LH conducted two training workshops with trainees in the team on how to conduct thematic analysis. All authors familiarized themselves with the transcripts and initial data. Step 2: Generating initial codes: LR started manual coding. Keywords, codes, subthemes, and themes were developed and refined inductively and deductively, informed by prior research and the Person-Centred Care Framework. Step 3: Constructing themes: Under the supervision of LH, LR reviewed and grouped the initial codes into broader categories. LR reviewed themes against the coded data and the entire dataset to ensure coherence and consistency. Step 4: Reviewing themes: LR presented emerging themes, subthemes, and representative codes to the team. Under the guidance of LH, the team held team-wide discussions, reflections, and analyses. The team collaboratively refined and reorganized themes to better capture the complexity and depth of the data in the iterative process. The team further examined whether the themes reflected meaningful stories in relation to the research objectives. The team agreed on codes, subthemes, and themes in the iterative process (see Table 2). The team collectively agreed the Person-Centred Care Framework is the most relevant underpinning theory for the article. We held four meetings to discuss the article; each meeting lasted approximately one hour. LH supervised and guided the research team in this process. Step 5: Drafting: After all discussions, LR led trainees GL, CW, and SK in writing. LH-guided trainees in the process of writing collaboratively with relevant partners. Step 6: Finalization: The research team reviewed the draft, commented, and LR followed up in discussion and amendment accordingly. The final draft was edited and agreed by all authors.
Examples of thematic analysis.

VR: virtual reality.
Rigor
Rigor was demonstrated throughout the study design, data collection, and analysis. Specifically, in the analysis, we maintained an audit trail of coding decisions, engaged in peer debriefing through regular team meetings and involved some of the partners in reviewing interpretations, depending on their availability.
Results
We recruited 42 participants in total. Table 3 shows details of participants’ demographics. Our patient partners were community-dwelling older adults with lived experiences of dementia. Family caregivers were family members and informal caregivers of people living with dementia. Patient partners and family caregivers participated in focus groups and follow-up interviews, either in dyads or alone, based on their personal preferences. Staff members were from two dementia care units of a hospital in Western Canada and had frontline care delivery experience with patients with dementia. We included staff from diverse backgrounds, including registered nurses, care aids, and occupational therapists. Care leaders were from the management and leadership of a local health authority and could influence policymaking and decision making. About 70% of the patient partners and family caregivers, 20% of the care leaders, and 5% of the frontline staff had an existing relationship with the Principal Investigator (LH) or members of the research team. Participants who did not know us beforehand were introduced to the study by those who did.
Descriptive characteristics of study participants (N = 42).

Three interconnected themes were identified from our data analysis on partners’ imaginations about having a VR program for patients with dementia in hospital settings. Figure 4 summarizes the themes and subthemes, and shows the interconnection between themes.

Interconnected themes.
Theme 1: Anticipating positive functions and outcomes
Overall, partners anticipated positive outcomes from a VR program in hospital settings. These positive outcomes are grouped into the following subthemes: (1) provide patients with new and positive experiences, (2) enabling versatility and improving patients’ wellbeing, and (3) supporting staff's care delivery to patients.
Subtheme 1: Provide patients with new and positive experiences
Partners found that VR could provide patients with new experiences and distract them from their current environment where few activities are available. In the focus group, our family partner and patient partners mentioned:
Isabella (family partner): I think the main thing in the care site is boredom. There is not a lot of meaningful activities for people to do. And I think if this [VR] brings back memories that are meaningful to the person, then that would be a positive thing.
Similarly, staff believed that VR enables patients to be exposed to a different environment they prefer, which could bring excitement. “Imagine patients want to see the sunny weather outside, but they can only see through this window. If there are more natural features in the video brought to them, they will feel more excited. They want to feel a different environment.” Cecilia, Registered Nurse (RN)
Further, in one of our focus groups, our patient and family partners mentioned that another advantage of VR is its ability to enable patients to “participate” in the virtual public event with safety. Benjamin (patient partner) said, “(In virtual public events), people are all around you, pushing on you. So it is actually a safer way to experience it in VR.”
Care Leaders believed that VR could give patients a purpose of living and help them spend quality time during their hospitalization. For example, Care Leader 1 mentioned,“This [VR] could be another tool added to our toolkits. We have recreation and activities to engage our patients. We also have exercise and reminiscing programs. And this [VR] will be added to the toolbox.” Patient partner Jim mentioned benefits that VR could potentially bring to patients during their recovery process. “The whole point is to make it easier for the individual to live and flourish in that [hospital] environment. I think it [VR] could serve as a great way of assistance and be helpful in many ways. It may make them [patients] feel seen and special in the (VR) program, making the recuperation process positive, and letting the individual regain hope when they get discharged.”—Jim (Patient partner)
Subtheme 2: Enabling versatility and improving patient's wellbeing
Overall, staff thought that VR programs could support improving patients’ wellbeing by calming patients down and distracting them from discomfort. Clinical Nurse Educator (CNS) Angel said, “To us, the most important thing is the outcome. We want to help alleviate the feelings of anger and frustration in patients, and this [VR] could be part of the treatment. I believe that it [VR] could calm them down by distracting them from responsive behaviours. When they become very agitated, we understand that behind it the patient is experiencing distress. When they settle, they feel better. I am hoping the VR programs will help them feel better. I think this project is very promising.”—Angel, CNS
Similarly, Patient partner Jim shared his imagination regarding positive outcomes generated by VR programs. “I think it [VR program] could make an impact on the rehabilitation process that could last for hours (for patients). It could reduce the potential of reactive responses by reducing the pain level and anxiety in them [patients]. It could also reduce staff's use of psychotropics in the future.”—Jim, Patient partner
Some staff members positively imagined that VR made their delivery of different types of programs possible, for example, exercising sessions. “Before I did not think about it. But now I think with this [mobile VR projector], even clients in bed, can ride a bike or do some other exercise. I think it [VR] is cool. It engages patients because some of them do not want to get up or participate. So, I think this [VR] is a good incentive. And I saw you have seated exercise videos. It is good, because we do not always have to do standing exercise.”—Suzzanna, PT
Patient Partner Alice imagined that VR enables diverse program delivery without requiring an expert in the field. “In my mum's care site, they have problems getting staff in. If there is a projection, for example, someone doing tai chi, the whole group of patients could sit there and do it without an instructor per se. The instructor would be on the video. So, this could cut down on staff's training in tai chi.”—Alice, Patient Partner
Subtheme 3: Supporting staff's care delivery
Staff imagined that VR programs could support them in achieving care goals, such as medication and nutrients intake. Staff also feel good when they see if VR videos could bring patients joy and good experiences. “I think it [VR] helps me give medication to my clients during or after they watch videos of others eating fruits. We do have a lot of jams in our unit. We can put medication in strawberry jam or ice cream. Patients could watch the ice cream video and then eat. This could also help if someone does not eat or drink a lot. Now [with VR] your environment is different. They could watch a person drinking juice [in VR], and we can offer them orange juice. It is easier for them to get fluids and nutrients in.”—Lucas, OT assistant
A conversation in focus group with care leaders showed how VR could engage patients instead of having them looking for staff. Care Leader 3 said, “I think this [mobile project in individuals’ room] is a really, really good idea because you can avoid having people at the nursing station.” Care Leader 4 responded, “Yeah. I think it is a good option because sometimes we take the patients up on a chair in front of the nursing station, and they are just doing nothing and just fidgeting.”
Theme 2: Considerations on VR program implementation
Subtheme 1: Preparedness and capacity
Different partners highlighted preparedness and capacity in the care site and staff for VR program delivery from different aspects, including management and care to patients, manpower, supports to staff, safety for patients (e.g. fall prevention), and sustainability.
First, patient and family partners mentioned the management at the care site is an important factor for a smooth VR program operation to meet patients’ needs. Family partner Isabella gave an example of patients wearing hearing aids. “People that wear hearing aids may have problems to use this [VR program]. My husband wore hearing aids in both ears, and the staff keeps them at the front desk so that they would not get lost. But if they do not put his hearing aids on him, he could not hear. I could imagine a similar situation for those with glasses.”—Isabella, Family partner
Patient partner Alice, and Family partners Isabella and Rachel had a small-group conversation during the focus group, which highlighted the importance of staff' presence and necessary involvement in VR programs. Alice stated, “I would like to see that there is a staff when the [VR] program is running. The staff does not have to be totally trained in, for example, tai chi, as what people are doing in the [VR] video.” Isabella agreed, “Yeah. It could be less staff, but not without staff.” Rachel followed, “Also, not enough staff in this [VR program] could result in less cleaning of the headsets.”
Second, for manpower, Patient Partner Jim expressed his view on staff preparedness regarding person-centred communication with patients for VR program delivery. “It is about the ‘how’. The biggest concern is how does the workforce deal with the patient and VR. It is about how staff approach the patient, how they have that conversation, how to communicate the message with emotions, how much time they would allocate to the patient per VR session, and how open they are to the conversation with the patient.”—Jim, Patient Partner
Care leaders were concerned about the care unit's capacity for implementing the VR program. Care Leader 9 expressed, “This [VR] is really beneficial, but one limitation I could think of is staffing. It would be great to have it [VR] run 12 hours a day, 7 days a week for direct therapy. But it [VR] takes up staff time to do the work.” Similarly, Care Management Leader Anne mentioned, “For understaffed units, this [running VR program] could be hard. There are more patients than staff. Staff already have extra tasks, so they might not be ready for additional activities for the patient. She (pointing to the recreational therapist) is doing an activity. I think she is doing it alone. I do not know if other staff can help her out.”
Interestingly, leaders also discussed introducing supportive policies to facilitate staff's operation of the anticipated VR program. Care Leader 2 asked, “Would we use it 24/7? They [patients] cannot be in the activity room [where the VR program will be implemented] after 10 o’clock.” Care leader 7 answered, “Some patients do not sleep at 9, some are night owls and up till midnight. If the room is closed at 10 o’clock, it does not sound right.” Care leader 5 proposed, “We could change that, depending on whether staff are there at nights.”
Third, staff members with previous successful technology implementation showed more confidence and motivation about the new VR program implementation. “I do not think this [VR] is hard to implement. We are already in a computer age. Mostly we are using computers, videos and cell phones. Here, we used iPads before. Some patients are really agitated, and we give them something to do over the iPad. They are really interested in old movies, then we put old movies on the iPad. Sometimes it calms them down. So, it [playing VR] will not be a problem. In this unit, they [patients] need a lot of help because 90% of them are really sick. I will help them [playing VR] as it does not take a lot of time.”—Katherine, RN
Lastly, staff and leaders mentioned environmental readiness for fall prevention for the care team to engage patients doing exercise with VR. “I always think about fall risk. I think in this (dementia) unit, people can do any kind of activities with this [VR], but we are not sure if the environment is ready or appropriate for this type of patient or program. Any fall risk is my big one.”—Suzzanna, PT
In our focus groups, care leaders raised similar concerns. Care Leader 9 mentioned, “If they are in a wheelchair and they do not want the restraint, but they got this [VR goggles] on and decide to get up…” “They might fall.” Care leader 7 followed. Care leader 3 added, “I guess we could just gauge the distance between the projector and the seat and make the whole thing closer to the nursing station, at least we could watch patients while working.”
Nevertheless, family caregiver Rachel held a different point of view: “I hope the VR program could motivate them (patients) to get up. Maybe they are not as frail as staff think.”
Subtheme 2: Person-centredness
Partners highlighted person-centredness should be embedded throughout the process of program delivery, spanning from introducing the VR opportunity to patients to the maintenance of social connections after program completion.
A key priority is the acknowledgement of a patient's personhood during the introduction and operation of the VR program. This includes a relation-based approach rather than a prescriptive or task-oriented style in communication with patients. “To me, the whole point of a VR program is that ‘We see you as an individual, you are somebody’. In other words, make the person feel from ‘I am nobody’ to ‘I am special and here is something special for me’. We do not want somebody rushing into the patient's room and just treat the session as one of the tasks to be checked off quickly. If the way the staff approach VR with patients is wrong, then the whole point of VR is lost.”—Jim, Patient Partner “From a family perspective, they [staff] have to keep in mind that the person is still a person with feelings, and very deep feelings. In the middle stage of his dementia, my husband would get frustrated when he was not able to do things anymore, and he kept calling himself stupid. And what I used to have to say is ‘You are not stupid. You are very smart. It is the disease.’”—Isabella, Family Partner
Family partner Lisa highlighted the togetherness in the invitation to the patient: “I think the word together is really important to incorporate that word into this project. ‘Let's do this together. Let's listen to a concert together.’ The word together is really important. And that is often a motivator on its own.”
Further, both patient partners and staff highlighted the importance of timing to introduce the program to the patient, which means choosing a time when the patient was calm and in a good mood to try out VR. Patient partner Jim expressed: “The timing of the introduction is important. It is not simply, ‘Mr A, let's do this and we have 10 minutes for it.’ How do we help the patient and help the process matter the most. Maintaining the positive human interaction is the key. It is about ‘How can we make it work for you?’ Also, be prepared-you may need to test the waters a lot.”
Staff recognized the heterogeneity among patients and emphasized that introducing VR must be adapted based on their local expertise. As Anne (Care Management Leader) mentioned, “Sometimes it depends on the patient. If they are not cooperative, maybe we skip their room and move on to the next patient. When the patient has calmed down, we can go back to do it (VR program). Because you do not want to make them more aggressive or angry. You want to finish your tasks as well.” OT assistant Lucas further shared his frontline experiences of his patient introduction of new devices, wireless headphones, to patients with dementia. In his conversation with Dr Hung in a focus group, he highlighted strategies of making patients feel that they are in control.
Lucas: “We could try to just let them [patients] look into the goggles first without putting on the strap. That could make the process easier. Patients can also hold VR goggles themselves [without putting on straps] and hold it open so that it feels like binoculars or something familiar.”
Dr Hung: “That is a good point. They feel they are in control.”
Lucas: “They can also have, for example, lanyards [for the goggles]. I have a patient that would probably like to hold it. I have my fair share of experience with the wireless headphones. I have patients throw them [headphones] away, because they do not like them on their head. But I just said “Hey, this is your favorite song. Try it in one ear.’ And they agreed: ‘Oh, yeah, it's good.’ Eventually, I put it [the whole earphone] on [their head]. Now they've been asking me for headphones every single day.”
Further, involving family caregivers in a program, including VR program, is mentioned across different groups of partners. Family Partners Isabella explained her experiences. “My husband was never a joiner of things. He is a very, very private person and would only share his emotions with me. But if I was there and said to him ‘Come on, try it, you might like it.’, he would go ahead and do it. But if I wasn't there, he would say no instantly; even if he wanted to, he would say no. So, he would never participate any program unless I was there. That's why I used to go [to the care site] every day, and I would have to participate [programs] too. The staff understand this. For a VR program, I think we have to look at a way to try and get families involved. Staff could approach family members as well to help them coach their loved ones to join.”—Isabella, Family Partner
A staff member mentioned ongoing engagement with patients during and after the VR session. “I think having patients watching this [VR] means engaging them for a longer period. Maintain the engagement after the video ends.”—Suzzanna, PT
Lastly, a conversation between patient and family members in the focus group highlighted that regardless of patients’ levels of cognitive impairment, VR program should show respect to their age, experiences, and adulthood instead of infantilizing them. Alice, a Patient Partner mentioned, “We have to make sure that we do not infantilize the person or make them feel like they are children. Unless they want to watch videos of cartoon or if that is what they enjoy. The videos must be age-appropriate for them.” Isabella, a family partner added: “That is true. I remember they [a care site] had a Christmas party. They had a Santa Clause come in, who was a fairly young guy. He dressed all patients as boys and girls. These people are old enough to be his grandfather. It really rankled me. So, for any program delivery, you really have to respect that though they are older, and their functions are impaired, they are still people, they are still them.”
Subtheme 3: Strategic usage of VR equipment
Partners imagined that projectors and goggles have distinctive advantages in providing immersive experiences to patients, and different equipment could be adopted for different needs and situations. Overall, partners anticipate that compared with goggles, projectors may be easier for staff to operate, and more accessible for patients to watch the VR program in a group. Goggles are advantageous in providing individual and personal immersive experiences, or the “me” time. Partners further provided considerations to increase the success of running group sessions with VR projectors to better meet individual needs. “It depends on which unit. For example, in dementia unit, sometimes they [patients] do not want to talk to each other or be disturbed. They have other options or use this [goggles]. Also, those that do not want big groups can use this one [goggles] for their own time. The big projector can be for smaller groups. It has more patient access, and they can talk to each other or share ideas while watching.”—Anne, Care Management Leader
Family Partner Rachel has a similar expectation about hosting group sessions with a VR projector. She also mentioned the need to reach group consensus before operating the program. “I think they could watch in a group and discuss this [what they watched]. The show can enable the socialization between the residents. But when you show it in a large screen, some people might not like certain subject, so you need people to reach consensus. You cannot force some people to watch something they do not like.”
Similarly, Clinical Nurse Educator Angel expects that VR video projector could increase accessibility, flexibility, and capacity for the program. She even imagines that such a program could benefit patients living on different floors of the hospital. “Letting the patient use the headset may need to be selective, but the video projected to the wall will be easier to manage. I remember years ago the staff did Zumba. When we started doing it, they [patients heard the music and just joined without being asked. So, if we exposed them to that kind of [VR] program [projected] on the wall, they will be encouraged to participate, especially if they have a love for music and dancing. Also, the majority of our patients are diagnosed with dementia, so this is the right unit for them. But there are other patients with dementia in other floors. When this program is on, we can bring them over. We can probably expand to other units.”—Angel, Clinical Nurse Educator
Nevertheless, Louisa, family caregiver and former staff, underscored the design in VR goggles for staff, which requires time and labor input. “Sometimes the VR program is pleasing for them; other times it is not. You can go both ways. Staff have to take it [goggles] off and find another program and pass it to them. If there is added step and work for staff, it is not going to happen.”
Some partners commented on strengths and expected usage in both VR goggles and projectors for situational needs. Their expectation is that watching VR videos through projectors could be more acceptable by patients than through headsets. Jack, a Patient Partner shared, “I think VR headsets need other's help to set up so it could be inconvenient to use it. I could see that with the projector, people can just sit back and be immersed. That is my initial reaction to the projector, which may have some distinctive advantages from my point of view.” Amanda, a Personal Care Assistant held a similar view: “Thenbsp;projector is more visible. You do not have to put anything on the patient's head.”
Subtheme 4: Just needing to start
Lastly, a staff member highlighted the importance of starting to trying the VR program with different patients in practice to deepen the understanding of its outcomes. “It really depends on what kind of patients (trying VR) and their level of agitation and comfort. Some are very calm, and you can spend more time on them watching more video clips. If you see they are restless, I do not know if this can calm them down. You really need to try and see.”—Cecilia, RN
Theme 3: VR program features
Subtheme 1: Interactive and connected with the outside world
Interactivity features were cited as the most expected aspect of a VR application by patient partners, family partners, staff, and care leaders. To increase levels of interaction in VR videos for patients, our partners highlighted that the VR program needs to be designed in a way that enables patients to take active roles, and even a leading role in the virtual world journey.
For example, family partner Mia watched two videos through VR goggles: walking in a local market and two students eating strawberries. To make the watching experience more interactive, Mia expects a VR video is first-person view and makes users feel that they are leading in the virtual journey. “I think how the video is created will affect the experience of patients. I realized that if I turn my head to the side or behind me or above, I saw different parts of the market. So that's the really cool part. I also expect that if I turn my head to the left, I can go to the left. But I can't actually go in the direction that I would like to explore more. Another expectation was that I could have some interaction [with people in the video]. When she [the person in the VR video] asks, “Would you like this?” I didn't really get a chance to say, “Are these sprayed strawberries?”. She just went on to the next and ignored me.”
More family partners shared similar experiences and imagination for a more interactive video that facilitates conversation with the person in the virtual world. “We could not have videos that you have certain expectation, but with little programs for interaction. [In the virtual world], I was trying to pick up a berry and when being asked ‘Would you like one of these?’ My reaction was, ‘Well, are they organic?’ There was the flow, and it should just go to the next step naturally. Definitely I want to pick one of them and pop one to my mouth, rather than just moving around [in the virtual world] but was not involved in the conversation.”—Lisa, Family Partner
A staff member explained that interactiveness means enabling a patient to participate in a game. “You have shown me beach, dog, 70 s jazz…yes patients love them, but when we are talking about interaction, I am thinking what else can they [patients] do. This is just the tip of the iceberg. You have not shown me the next capability of it [VR]. Maybe they can play a game, like playing bingo or bowling.”—Sebastian, RN
Another feature highlighted by family partners is fostering patients’ feeling of socially connected with the outside world, through enabling users being part of the crowd and public events that they are watching. Louisa shared, “With a VR program, a patient could be going to the park, watching the ship going by, children playing on the playground… something that that really connects them to the outside world. Because, come on, how often do patients go out to see the outside world?” Lisa also mentioned, “We could create VR videos that give us a feeling of just sitting in a concert hall and watch someone playing the cello or piano. No camera panning. I think this is not complicated from a camera perspective.”
Subtheme 2: Personal and relevant
Partners expected VR videos to be personal and relevant to patients. This includes showing videos that reflect a patient's past experiences and meeting the patient's needs at the moment. To achieve these expectations, staff and care leaders expect collaboration with families in producing such videos. Further, partners highlighted the importance of diversity and inclusiveness, and leveraging a media management system that is easy for families to navigate.
First, personalization in VR videos means showing patients’ family in VR and addressing their needs for seeing their families in different scenarios, enabling them to virtually stay together with families. “We can invite a family filming, say, a birthday party for the grandchild, and show it to the patient, ‘Hey, your grandchild turned six, and here's the video of his/her birthday.’ Maybe show the first grandchild-the first one is usually very important to them, and they may remember.”—Jack, patient partner
To make such videos possible, staff and care leaders further expect that patients’ families could be involved in the VR co-creation process. For example, Care leader 8 said: “We can engage with families in this process, especially when they are too far away from the patient to visit.” Further, Jasmine, a Nursing Unit Assistant imagined, “If the family members would be able to send videos and clients could watch them in this [VR], it would be probably beneficial to them [patients]. This makes them feel like they are with their families. The distance between them does not seem too far away. Families showing in the video will just make that big difference. And they [patients] just sit and watch them, and they feel they are close to their families.”
From his perspective, Family Partner Cheng shared a corresponding need to collaborate with staff to achieve the shared goal. Further, he highlighted user-friendliness in a future media sharing system. “For the case of my wife [the patient partner], when I show her old photos for 30 minutes, she is always happy. I think this [reminiscence] could be beneficial to other patients. This could be applicable to VR, but it requires guidance or instructions, because some family caregivers may not know how to upload the media to the system or drive. It also needs staff's coordination with caregivers to provide photos or videos.”—Cheng, Family Partner
Staff understood creating a personal VR program that meets patients’ diverse needs and interests at the moment. They mentioned showing different scenes in VR which are not usually accessible for patients in their context. Katherine, a Unit Clerk, shared: “We have a garden, but most of our patients are certified [as living with dementia] so we cannot bring them unless they are accompanied by their families. It will be nice if you could make something about gardening and I think our clients will love to watch. Especially the ladies. They love to see trees and plants. Others like to see flowers and animals. Something outdoor.”
In addition to gardens, staff and care leaders also elaborated grocery shopping and traveling. Cecilia, an RN, added: “Some patients always say ‘I want to go grocery shopping’. If you have a grocery store and there are fruits, they would be happy to see. They said they want to see nature, animals, mountains, snowing, marketplace. Some said ocean view because they want to see cruise ship, even though they are confused. Also gardens. Maybe the Butchart Gardens.” Further, care leader 4 mentioned, “Travel would be nice. In the past, when we show travel videos, our patients say ‘I've been here/there.’ Maybe travel videos can bring back memories. Especially for our immigrant patients. It would be really good for them.”
Lastly, Family Caregiver Cheng expects VR videos should be tailored to patients' education level. “I think there could be videos speaking to people's diverse education levels, because the stimulation components are different. I see the difference between those received higher education and those who are not, for example my wife [the patient]. So, we could consider education as a factor in making VR videos.”—Cheng, Family Caregiver
Other patient and family partners suggested similar expectations to make a VR program culturally relevant and more engaging for the patient.
Discussion
Our study examined what patient partners, family partners, hospital staff, and care leaders imagine what a VR program would look like for patients with dementia in hospitals. Our results indicated multiple partners’ needs, including person-centred VR programs, multipartner collaboration and a supportive care environment, to improve patients’ wellbeing and support staff in care delivery through VR. To our knowledge, our study is the first of its kind in the field.
The need for person-centred VR programs
Our partners with different backgrounds voiced the diverse and dynamic needs of heterogenous patients with dementia, and expressed their positive expectations of VR opportunities to meet these needs. Their expectations are consistent with findings from existing literature on the effects and impact of VR for older adults with dementia in hospitals.56,57 The positive impacts include evoked memories, enjoyment, relaxation, emotional wellbeing, and socialization.57–61 Furthermore, multiple partners underscored that VR program can further address person-centredness in VR program delivery through multisensory stimulation and more diverse video choices, which aligns with existing literature.60,61 This includes creating more multisensory VR programs. The expectations from multiple partners can inform the design of future VR programs to be more relevant and tailored to the needs of patients with dementia, who are traditionally underrepresented in technology development yet deserve access to and benefit from technology.
Further, our findings indicate that in our focused context, partners expected staff to act beyond simply showing patients VR videos. Our results aligned with the general expectations on staff reported in the literature that they are at the forefront to engage patients and lead in care delivery. 62 Our findings expanded partners’ expectation on staff, including (1) be strategic in approaching patients and introducing VR opportunities; (2) be prepared in engaging patients throughout the VR watching; (3) be trained in maintaining hygiene for VR equipment; (4) be flexible in involving family caregivers when necessary; and (5) be capable to address equitable access to VR opportunities (e.g. for patients with visual/hearing impairments).
These expectations enriched key concepts in the Person-Centred process (e.g. engaging patients authentically, being sympathetically present and working holistically) in our focused context. 41 Our findings can inform the design of future VR programs by integrating more features expected by different partners. Our results can also be the basis for future training and education programs for staff and care leaders to deliver more person-centred VR programs for patients with dementia.
The need for multipartner collaboration
Although increasing studies have involved partners in the design of VR programs and in exploring the needs of relevant users, most of the studies have not involved patients, family caregivers, staff, and care leaders within a single study.63,64 Notably, all partners in our study expressed their desire and enthusiasm to collaborate for a better VR program delivery. Further, underpinned by CAR, partners deepened their understanding of the role they are expected to play in the care environment by others. For example, family caregivers are expected to work with staff to address patients’ psychosocial needs, staff are expected to lead in the delivery of VR programs, and care leaders are assumed to be responsible for policymaking. CAR benefits leaders in gaining insights about considerations and desired supports for the expected implementation of a VR program in the frontline, which can inform their policymaking and could potentially enable shared decision making in the focused area. Moreover, we identified conflicting perspectives. For example, family caregivers hope VR could benefit patients physically by engaging them in more movements. However, staff are concerned about the potential risks of falling from programs with the same purpose.
The need for a supportive care environment
Our findings highlighted the complexity of the care environment in which the VR program will be introduced. For example, partners highlighted using VR under a safe environment for patients, which corroborated findings from previous studies.65–67 Further, partners were concerned about resources for deploying VR spanned human resources, material supply to funding (e.g. engaging patients and maintenance of equipment). These concerns were interwoven with longstanding challenges in hospital settings, including the characteristic high turnover of patients, staff shortages, and risk-averse organizational culture (e.g. low motivation to take reasonable risks to increase patients’ benefits from VR programs).68,69 Our results indicated the need to train and educate staff and managers, and to make policies for care team development.16,70,71
The complexity and dynamics in the care environment were also highlighted in the person-centred framework, which includes an organizational system for innovations (e.g. VR programs), organizational culture in technology deployment, and shared decision making. 41 Existing literature reports these complexities. Wilding et al. 63 identified that introducing VR requires substantive input including time, money, and institutional supports, 62 and broader social context should be considered-specifically care and relational resources-for successful VR design and implementation. Wong et al. 72 recommended that sufficient support to staff is essential, without which VR could be viewed as a “burden” taking up staff's limited time in care delivery. Further, involving family partners as a companion to patients can also shape the environment in which new technology is introduced.52,73 Future studies are recommended to explore practices that address the complexity of the local care environment and strategies for improvement. This can include strengthening a supportive organizational system for innovations like VR programs and building a more open organizational culture for technology deployment and shared decision making.
Limitations
Our study has several limitations. First, data were collected from community-dwelling patient partners with experiences of dementia, who may have different experiences from the target patient population in terms of acuity and living settings. Second, although we provided VR videos with different themes, videos were not fully personalized to the individual preferences of the patient partners. Third, this study was conducted in an urban area in Western Canada, where VR co-creation and delivery can be different from the process in rural areas. Fourth, we did not calculate the sample size in advance, which may limit the generalizability of the findings. However, the focus of our study is to capture diverse perspectives across different partners. This informed our recruitment strategy, which aimed to ensure diverse representation among participants, which is appropriate for qualitative research. Fifth, there may be participant selection bias. Participants with an existing interest VR before the study started are more likely to contribute to data collection and share positive perspectives for the use of technology in hospitals. Sixth, although our paper analyzed partners’ expectations on VR program delivery, additional aspects from an implementation science lens were underdiscussed, such as staff training and costs. Lastly, some participants had pre-existing relationships with the research team, which may have introduced selection bias or influenced responses. However, these existing relationships may enhance the quality of the data, as trust was built and a safe space was created for participants to openly share their experiences. Future research can benefit from engaging patient partners with recent hospitalization experiences, providing personalized VR videos for partners to watch and including partners from different geographic locations, including rural areas. Future studies can also explore similar topics by adopting theories and frameworks in implementation science, or by engaging patient partners with more diverse impairments (e.g. hearing/visual impairment and mobility challenges) to enhance VR program inclusivity.
Conclusion
Our study advanced knowledge about partners’ expectations of a VR program in hospitals for patients with dementia from patient partners, family caregivers, staff, and care leaders. Further, our findings can inform the development of VR programs that can better meet patients’ needs. Partners’ expectations focused on positive VR functions and outcomes, implementation considerations and VR features to improve patients’ wellbeing and staff's delivery of person-centred care. Our themes identified the complexity of introducing new technology to patients due to both shared and different understandings of a person-centred VR program by multiple partners, the complexity of the care environment, and the need for ongoing exploration of multipartner collaboration. Partners also shared their enthusiasm for cross-sectoral collaboration. Future studies should continue to explore approaches to foster multipartner collaboration for a person-centred VR program in hospitals and other care settings for patients with dementia.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251382099 - Supplemental material for Expectations of a virtual reality program for older adults with dementia in hospitals: Perspectives of patient partners, families, staff, and care leaders
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251382099 for Expectations of a virtual reality program for older adults with dementia in hospitals: Perspectives of patient partners, families, staff, and care leaders by Lily Haopu Ren, Grace Yaqian Liu, Julia Nolte, Catherine Wu, Sena Kholmatov, Jim Mann, Christine Wallsworth, Lily Wong, Kennedy Schaffner, W. Ben Mortenson, Angelica Lim, Jennifer Boger and Lillian Hung in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251382099 - Supplemental material for Expectations of a virtual reality program for older adults with dementia in hospitals: Perspectives of patient partners, families, staff, and care leaders
Supplemental material, sj-docx-2-dhj-10.1177_20552076251382099 for Expectations of a virtual reality program for older adults with dementia in hospitals: Perspectives of patient partners, families, staff, and care leaders by Lily Haopu Ren, Grace Yaqian Liu, Julia Nolte, Catherine Wu, Sena Kholmatov, Jim Mann, Christine Wallsworth, Lily Wong, Kennedy Schaffner, W. Ben Mortenson, Angelica Lim, Jennifer Boger and Lillian Hung in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all partners and participants for generously sharing their time and perspectives, including patient partners, family caregivers, staff and care leaders throughout the research process. They also thank all volunteers of the Innovation in DEmentia and Aging (IDEA) Lab, University of British Columbia who supported in data collection in this process.
Ethics approval
This study is approved by the University of British Columbia Research Ethics Board and local health authority (REB number: H23-01008).
Informed consent
All participants provided written consent. Pseudonyms were used for all participants in this article except Dr Jim Mann, who preferred to use his real name in results.
Consent for publication
All participants provided written informed consent for participation and for the use of anonymized quotes and images in publications except Dr Jim Mann, who preferred to use his real name in results.
Contributorship
LHR performed the data collection and data analysis; wrote method, results, discussion and conclusion; revised the draft; provided all figures except Figure 2; and provided all tables and the appendix. GYL performed the data analysis; wrote the method; and revised the draft. JN performed the data analysis; wrote the results; and revised the draft. CW performed the data collection; wrote the introduction; and revised the draft. SK performed the data collection; wrote the discussion; and provided Figure 2. JM, CW, and LW participated in discussion and reflection on data collection and data analysis; and revised the draft. KS and JB revised the draft. WBM, AL supported the discussion and reflection on data collection and data analysis; and revised the draft. LH led the study design; supervised the entire team in the overall operation of the multiphase study; supported and guided the team in data collection and engagement with multiple partners; guided the data analysis; and revised the draft. All authors agreed on the final draft of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the funding from the New Frontiers in Research Fund (grant number: GR028180) to support this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Data and materials are available upon request to the corresponding author.
Guarantor
Dr. Lillian Hung is the guarantor of this work and, as such, had full access to the data, takes responsibility for the integrity of the data and the accuracy of the data analysis, and controlled the decision to publish.
Peer review
This paper was externally peer reviewed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.