
Abstract
Background
Electronic health (eHealth) has been widely adopted in chronic disease management. Prior studies focused on time-based reminders as a cue to facilitate behavior change intentions, ignoring the development of automatic cue-behavior associations via other cue types.
Objective
Hence, this study utilized avatar appearance as a visual-based cue to help establish the automatic association between appearance transformation and health behavior to form habits without intention.
Methods
To better understand users’ attitudes and experiences toward applying changes in avatar appearance to develop cue-behavior associations for hypertensive patients. Fifteen participants were recruited in a 14-day experiment. After excluding one participant who dropped out of the experiment, others were randomly assigned to two groups. One group consisted of a visual-based cue (a virtual plant) and basic behavior change techniques (BCTs). The other group only included basic BCTs. Attitudes and experience outcomes were collected by interview, and qualitative data were analyzed using thematic analysis.
Results
57% of participants had been diagnosed with hypertension for more than five years, and more than 50% of participants have experience using mobile apps or wearables. 66% of participants did physical activity more than three times every week. The result shows that tailored time-based reminders, blood pressure monitoring, and daily dietary intake were the most attractive features. Additionally, hypertensive participants have positive attitudes toward avatar appearance as a visual-based cue to develop cue-behavior association, which enhances self-management motivation.
Conclusion
This study proposes a visual-based cue design for habit formation and conducts a qualitative method to explore hypertensive patients’ perceptions. The findings offer insights from user's perspectives into hypertensive patients’ attitudes toward visual-based cues and perception of the connection between avatar appearance and health behavior for self-management. Subsequent discussions present eHealth design guidelines of habit formation from intention, automatic cue-behavior association, and self-management perspectives.
Introduction
Hypertension (high blood pressure) is a prevalent chronic disease, which is a leading risk of stroke and myocardial infarction.1,2 Long-term blood pressure (BP) control could minimize the incidence and mortality of cardiovascular diseases in hypertensive patients.1,3 Prior studies have shown that healthy lifestyle behaviors, such as physical activities, healthy diet, and weight loss would be effective strategies for BP control.2,4,5 For instance, walking 10000 steps per day has shown beneficial effects in reducing BP, 6 aerobic exercises have a significant effect on BP, 7 and 2300 mg of sodium intake per day is recommended by the Dietary Guidelines for Americans. 1 However, the World Health Organization (WHO) reports that around 75% of hypertensive patients cannot maintain ideal BP control. 2 Lack of long-term maintenance of self-management habits is considered one of the major factors in the low rate of BP control. 2
Normally, habits are developed through the establishment of cue-behavior associations, in which specific behaviors are repeatedly triggered by cues in a specific context.8–10 Dual Process Theory argues that behavior results from two sets of processes: one is the unconscious, impulsive, and automatic process, and the other is the conscious, intentional, and reflective process. 11 Therefore, three key factors were summarized to form habits in prior studies: (a) intention, (b) cues, and (c) positive reinforcement.8,9,12 Intention motivates goal-directed behavior in the reflective process, which requires specific and detailed action planning. Cues are stimuli that cause impulses and intentions, triggering both reflective and automatic processes. And positive reinforcement accelerates the association between cues and behavior by rewarding. As shown in Figure 1, action is driven by individuals’ intentions initially, and these goal-directed behaviors are determined by conscious control in the reflective process. In addition, cues trigger behaviors in two parts. Explicit cues stimulate behavior by drawing human attention (e.g. reminders), and implicit cues (e.g. physiological signals, surrounding environment) evoke associative memory in the automatic process. Through consistent repetition in a stable context, the cue-behavior association is developed, which potentially be accelerated by positive reinforcement (e.g. internal and external rewards). Finally, unconscious, unaware, and automatic habitual behaviors are formed in the automatic process. To achieve a low-cost, popular, and convenient manner of chronic disease management, electronic health (eHealth) is demonstrated to facilitate behavior change by adopting ubiquitous technology (e.g. smartphones and wearables).13–17 Various behavior change techniques (BCTs) have been integrated into eHealth solutions to form habits, such as goals and planning, virtual rewards, and prompts and cues.
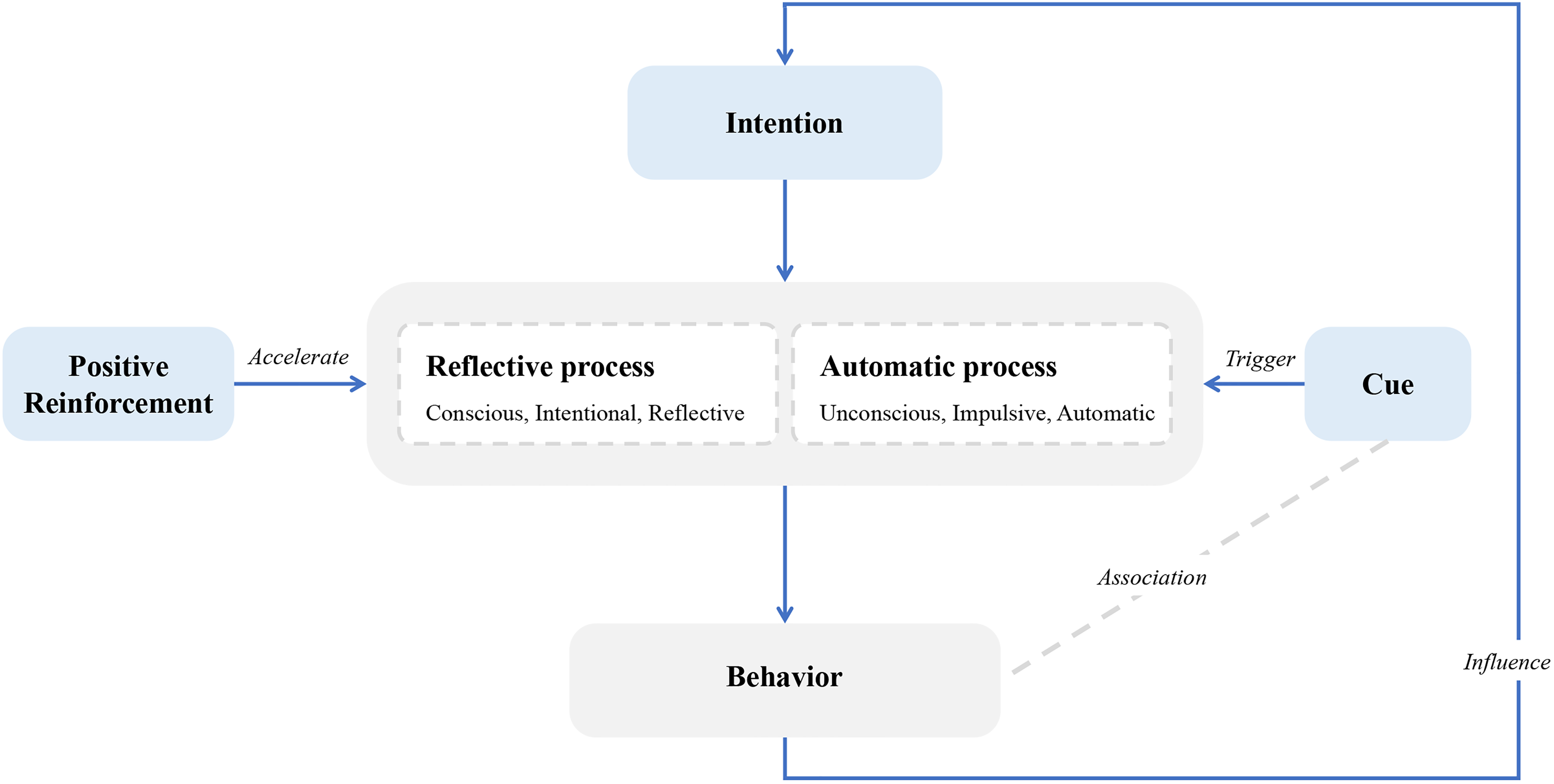
The process of habit formation through consistent repetition.
Implementations of goal-directed intentions
Goals and planning are widely used techniques in physical activity eHealth solutions, which motivate intentions to change behavior. 18 Individuals intend to change behavior through goal setting, conducting activities, and self-rewarding after goal achievement. 19 According to studies,19–21 applying proximal, specific, and difficult goals shows better performance than long-term and easy goals; meanwhile, detailed planning of action (i.e., where, when, how, and who features) could further specify the intention. Consolvo et al. explored user experience on goal sources and goal timeframes when setting goals for encouraging physical activity. 22 Different goal sources were presented in this study, such as self-set, assigned by experts, and cooperative set. According to their findings, most participants preferred to self-set their goals. On the contrary, chronic disease patients would choose goals guided by their physicians. Prior studies demonstrated that patients expected detailed and valuable recommendations from physicians. 23 Self-setting goals might not be appropriate in situations where patients lack the necessary expertise. Therefore, prior studies adopted general lifestyle guidelines as a potential approach for self-management among chronic disease patients.
Authorities have published various reports on non-pharmacological intervention approaches to instructing physicians and patients with chronic diseases.1,2,5 These quantified standards with the clinic trail evidence are recommended for clinic treatment. Increasing physical activity and controlling dietary supplements are widely applied behavioral strategies for chronic diseases, such as hypertension and diabetes.16,24,25 According to studies from the American College of Cardiology, 5 aerobic exercise could reduce systolic blood pressure (SBP) by 5–8 mm Hg in adults with hypertension, and lifestyle modifications have been evaluated to contribute to a reduction in daily sodium intake by approximately 25%, which can have positive effects on blood pressure control. In addition, studies demonstrated that the Dietary Approaches to Stop Hypertension (DASH) diet is an effective plan for lowing blood pressure, 26 which could reduce SBP by around 11 mm Hg for hypertensive patients. The DASH eating plan 27 suggests 2100 kcal energy, 567 kcal fat, 378 kcal protein, 1155 kcal carbohydrate, 4700 mg potassium, 500 mg magnesium, 1240 mg calcium, and 3000 mg sodium in daily servings. Existing eHealth solutions are widely used for chronic disease self-management. 28 However, the effectiveness of these eHealth solutions is insufficient, 28 which may be improved by integrating quantified standards into the eHealth systems.
Implementations of positive reinforcement
Virtual rewards (e.g. points, trophies, and badges) are used as positive reinforcement, which boosts engagement for eHealth solutions. 29 Positive reinforcement stimulates the successful performance of behavior and makes pleasurable emotions in order to promote the repeated performance of the behavior.8,10 Prior studies have shown that intrinsic and extrinsic rewards could enhance user immersion and motivate engagement. 30 Virtual points, badges, and trophies are commonly utilized gamification elements that serve as intrinsic rewards to provide positive feedback on behavior. For instance, Lee et al. proposed a gamified mobile game to enhance physical activity levels, which included puzzle games that could earn virtual points by winning the game. 29 Fuemmeler et al. metaphorized physical activity as an adventure game in which users could collect virtual badges by completing expeditions. 31 Additionally, motivational text messages could be an intrinsic reward to prompt repeated behavior. Oppezzo et al. encouraged sharing information in social networks by sending motivational messages to reinforce sharing behaviors. 32
Implementations of cues
In addition, reminders or notifications are commonly used implementations of prompts and cues. 33 Cues refer to internal and external events or features that trigger impulse and intention.8,10 Time-based cues (e.g. push notifications and reminders) are strategies with higher perceptibility to prompt reflection and intention for behavior change. However, some researchers argue that most existing studies focus on applying strategies to change goal-directed behavior rather than the automatic process of habit formation, which ignores other cues that trigger associative memory in everyday life. 34 For instance, Stawarz et al. compared the difference between a time-based reminder and an event-based trigger on habit formation. 33 They argued that event-based cues (e.g. “Please remember to go for a walk after lunch”) had benefits for developing cue-behavior association rather than a fixed time-based reminder, since the latter may cause users to rely on self-tracking technology instead of automatically forming unconscious connections between cues and behavior. Some implicit cues influence behavior without deliberation, such as visual-based cues and physiological-based cues (e.g. heart rate, auditory, olfaction). For instance, the size and color of plates could manipulate users’ perceptions via attention bias. 34 Food may be perceived larger portion on small plates than on a large plate. Thus, implicit cues may activate user behavior subconsciously rather than attracting conscious attention, which requires investigating how other types of cues in eHealth are perceived by users.
Avatars, visualized representations of users, can reflect individual behavior consequences, which are commonly utilized gamification elements. 30 On the one hand, the changes in avatar appearances have been shown to influence self-concept and lead to behavior change.35–37 For instance, Mönninghoff et al. proposed a future-self avatar to represent users’ physical activity and diet intake behavior, which aims to enhance awareness of self-efficiency. 38 Users altered their behavior when the appearance of avatars became worse. On the other hand, prior studies have demonstrated that changes in avatar appearances are effective methods of boosting user engagement.17,39–41 It is widely applied to different health behaviors (e.g. physical activity38,42 and diet management 16 ) and different contexts (e.g. diabetes, 43 medication adherence, 44 and survivors of childhood cancer 31 ). Therefore, changes in avatar appearances serve as a visual-based cue that stimulates user behavior in a subtle and intuitive way that reduces user attention and cognitive processing, which potentially prompts the automatic process of cue-behavior association for habit formation.
Research aims
Existing studies have assessed the effectiveness of adopting BCTs for hypertension in the short-term.28,45 To achieve long-term behavior change goals, researchers argue that current research lacks exploration of engagement and user experience.46,47 According to the findings of the Sharpe et al. study, engagement not only refers to investigating which BCTs could enhance the engagement of interventions but also means encouraging the collection of user attitudes in the early stages of intervention development. 47 In addition, Oinas-Kukkonen 46 argued that despite existing studies applying the BCTs in interventions, the description of implementations was vague, and few studies reported on the user experience of these techniques.
Therefore, this study conducts a qualitative method to explore user attitudes toward utilizing BCTs in the self-management of hypertension. Specifically, this study focuses on exploring user perception of changes in avatar appearance for developing cue-behavior associations in forming self-management habits for hypertensive patients. Our research objectives include the following: (1) to explore hypertensive patients’ attitudes toward the visual-based cues for developing self-management habits; (2) to investigate the experiences of hypertensive patients on associating avatar appearance with health behavior for their self-management; (3) to propose the design guidelines of habit formation for hypertension self-management. Two versions of Android mobile apps were designed in this study by integrating several effective BCTs and avatars. A two-week empirical study was conducted to investigate the user experience of avatars as visual-based cues. Fifteen participants with hypertension were recruited. Findings have suggested implications from the design perspective, which can be serviced as practical guidelines for future habit formation eHealth design.
Methods
To develop mobile applications to facilitate comparative studies: one that adopted avatar appearance as a visual-based cue and another one without avatars. Fifteen hypertension patients were recruited to experience the apps in two weeks.
Implementations of BCTs
Prior studies showed that quantified measurements were lacking in most of the eHealth applications, resulting that the users were wondered if the task was finished or not. In contrast, medical advice could provide detailed and quantified measurements to the patients for their therapy, which serves as a beneficial standard to follow. As a result, medical advice from famous hypertension management communities was extracted and integrated into our study as the goal of blood pressure management. In this study, we focused on three kinds of hypertension management behaviors: moderate physical activities, healthy diets, and continuous blood pressure monitoring.
According to investigating the popular sports among Hong Kong residents, 48 hiking, jogging, bicycling, swimming, and dancing were included as the recommended sports in this study. Meanwhile, with the guidance of WHO and the American College of Cardiology,2,5 90–150 min of aerobic exercise is recommended per week. Considering specific and proximal goals may potentially improve goal performance, the physical activity goals were set to daily tasks with 30 min.
Dietary intake is also a crucial part of hypertension management. According to DASH diet recommendations, 27 seven kinds of ingredients (calories, fat, proteins, carbohydrates, potassium, magnesium, and sodium) were considered to be the goals in this study. The detailed intake recommendations for meals are described in Table 1.
Ingredient intake recommendation by DASH. 27

Moreover, continuous blood pressure monitoring was also recommended by the medical communities but often neglected by the patients. According to prior studies, 5 patients are recommended to sit quietly or lay down for 5 min before blood pressure measurement. Therefore, tailored reminders were sent to individuals based on their wake-up time, which included content with instructions for accurate measurement of blood pressure and hypertensive management tips. Table 2 shows the implementation of BCTs in this study.
Implementation of BCTs in this study.

C: control group; I: intervention group.
Study design
The standard features are daily medical advice-guided goals, self-reporting of physical activity, dietary intake, and blood pressure, notifying with tailored time-based reminders, and motivational messages. A virtual plant serves as a visual-based cue, which was an additional feature of the interventional group. Figure 2 presents the major difference between the home page in the two versions.

The difference between the layouts of the home page in the control group (a) and the intervention group (b). The major component of the intervention group is an avatar (c) and the transformation of avatar appearances (d).
The standard hypertension management system (control group) only included self-management goals extracted from medical advice with a time-based cue (reminder). Several BCTs implementations were designed for this app, such as daily tasks with a progress bar and tailored time-based reminders based on the individuals’ wake-up times. In the dietary management function, an open-source database was adopted that could transform the food into ingredients with certain weights.
Participants’ demographics.

PA: physical activity.
*Participant who dropped out of the experiment.
The achievement of lifestyle modification goals in the intervention group was guided and facilitated by a visual-based cue (avatar). As shown in Figure 2(c), the major component of the home page layout was the virtual plant. The design of the avatar has been demonstrated to enhance persuasion and self-affirmation. 49 Different goals were transformed into different virtual rewards to make the avatar live better, such as sunlight, moisture, and fertilizers. In particular, each goal was tailored with different reward ingredients to fulfill the avatar's needs. When the avatar stays healthy for a certain period, its level and appearance will be updated (shown in Figure 2(d)).
Participants and recruitment
As shown in Table 3, N = 15 participants (8 female, 7 male) were recruited from posters, aged 31–80 years old. The inclusion criteria were that the participant should use Android mobile phones and be diagnosed with hypertension by the physician. Fifty-seven percent of participants had been diagnosed with hypertension for more than five years. Most (10/15) participants did physical activity more than three times every week. Furthermore, 6 participants identified as having employment status and being less than 60 years old. Participants were randomly assigned into two groups: the intervention group (an app with a visual-based cue) and the control group.
Procedure
Before the experiment, participants were invited to participate in a 60-min pre-test session. Firstly, we explained the study objectives and experimental procedures to the participants. After obtaining signed consent from each participant, an entry survey was conducted to collect participants’ demographic information, duration, and frequency of physical activity per week, and average time of physical activity. Meanwhile, an interview was conducted to explore participants’ attitudes toward hypertension management, the barriers to maintaining self-management, past experience with mobile apps, and expectations for eHealth. Finally, to better assist users in experiencing the proposed design and understanding their attitudes toward the barriers faced in maintaining long-term self-management habits with the use of eHealth solutions, participants are required to engage with the developed app for a period of 14 days. The Android app was installed based on the participants’ assigned groups, with instructions on how to use the application. During the two-week experiment, participants were required to self-report daily tasks through the assigned Android app. The weekly survey was hosted on an online questionnaire platform, and a text message with the link was sent to participants separately. After two weeks, participants visited the lab again for a 60-min offboarding session, which included a semi-structured interview. The overall experience with the assigned app, attitudes, and experience with visual-based cues was collected. All lab sessions were audio recorded with the participant's agreement.
Data collection and analysis
After excluding the participants who gave up during the experiment, 14 valid data were kept. Interview data were manually transcribed into text by two research assistants who are native speakers of Mandarin and Cantonese. The final proofreading was done by first three authors. To illustrate insights from the results, first three authors coded and analyzed qualitative interpretations of interview data using thematic analysis. 50 The identified themes were reviewed and revised by the senior researchers.
Results
According to the semi-structured interview in the entry session, more than 50% of participants have experience using mobile apps or wearables. Step count is the most commonly used function for self-monitoring. Most participants (10/14) received medical advice from physicians or attended public lectures hosted by authorities. Findings focus on exploring participants’ attitudes and experiences with the proposed strategies for habit formation based on the offboarding interview and weekly survey. The results show that tailored time-based reminders, blood pressure monitoring, and daily dietary intake were the most attractive features.
Goals and time-based reminders
Medical advice-guided goals were perceived as appropriate proximity and specificity goals. As shown in Table 4, most participants emphasized that daily tasks with quantified goals are easier to achieve, especially when they are busy. One participant from the control group highlighted that the goals provided by the system were perceived as the standard, which could be specific medical advice for them. Moreover, comparing individuals’ behavior with the standard has positive effects on goal achievement, which is presented by all groups. The process of self-reflection is also discovered during the comparison. Time-based reminders are the most accepted feature by participants. It contributes to knowledge acquisition and goal achievement.
Participants’ attitudes toward goals and time-based reminders.

In addition, participants also demonstrated that they expected to add more healthy dimensions to their self-management goals, such as sleep and emotion monitoring: “I hope to connect my work status, life status, and my health status. I think it would be better if there was other information that could be enriched besides exercise and dietary intake, such as sleep.” (P11) Some participants tried to adjust their goals by testing their hypotheses since the assigned app only provided static medical advice-guided goals: “I tested it. If I eat too much salt, my blood pressure will go up. I will check or test it according to my own records.” (P14)
Visual-based cues (avatar) and virtual rewards
Table 5 shows the participants’ attitudes toward visual-based cues, rewards, and levels among the two groups. Most participants perceived the metaphoric linkage between the avatar and the individual's health status. The transformation of the avatar's appearance was expected to have higher-level changes in the intervention group. The result could be explained by the fact that the average age of participants in this group is younger than that of the control group, and they also have more prior experience with mobile apps. Participants were motivated to maintain physical activity and self-management habits by changing their avatar's appearance. However, personalized avatar customization was proposed by some participants since it might lead to more motivation and engagement. Meanwhile, the transformation of avatar appearances in developing cue-behavior associations may be influenced once participants have formed healthy lifestyle habits.
Participants’ attitudes toward gamified elements.

Virtual rewards and levels were effective gamified elements to boost engagement. Participants perceived the relationship between virtual rewards (sunlight, moisture, and fertilizers) and levels of avatar; meanwhile, the positive effects on behavior consequences were recognized. In addition, participants expected various types of virtual rewards, such as rewards for long-time achievements. Combined short-term and long-term achievement rewards could enhance engagement and boost their motivation for habit formation. However, participants with retired status argued that they would not change their lifestyle for upgrades or virtual rewards. The established self-management habits and routines may be one of the reasons.
Interestingly, one participant was concerned that changing avatar appearances and rewards might lead to potential stress, which conflicts with the medical advice to maintain healthy emotions. “It made me feel stressed because high blood pressure is generally more affected by emotion. I don't think this gamification design is suitable for hypertensive patients.” (P2)
Barriers to maintaining the self-managed habits
Participants mentioned obstacles to self-management. Firstly, the issue of irregular medication was frequently mentioned, especially among participants with employment status who had limited time. Busy work and disrupted routines were leading risk factors for medication adherence. Moreover, some of them are worried about the side effects of long-term medication. Therefore, participants preferred non-pharmacological therapy or traditional Chinese medicine. Sometimes I forget to take medicine. Even if I set the alarm, I didn’t have the medicine with me when it alerted, and I will forget it later. (P4) Basically, there is no difficulty taking medicine every morning. But if I go abroad for business, I will forget. (P7) Medicines should not be taken for a long time. I hope to try Chinese herbs. (P13)
Secondly, despite the participants who were currently employed having a strong desire to change their behavior, they struggled to maintain regular physical activity due to a lack of time. On the other hand, retired participants were bothered by other complications that meant not every physical activity was suitable for them. I’m busy during the daytime. When I go home, I have to take care of my kids, which makes it more difficult. I don’t have time until 23 o’clock, but it's time to go to bed. (P5) The doctor suggested me to jog more. But it was too hard because my leg has some issues, so I replaced it with walking or stretching. (P6)
Lastly, dietary intake was influenced by other external factors, such as cooking by other family members or social activities. Even if participants hoped to control sodium intake, it was difficult to trace without nutrition labels. My mother cooked. We communicated about sodium intake reduction, but nothing has changed. (P5) Meals cooked by other family members. I don’t know how much salt they have used. (P7) Social activities increased a lot after I retired. (P3)
Discussion
This study proposes a visual-based cue design for habit formation, and hypertension is presented as a case to explore how chronic disease patients would perceive the proposed method. The qualitative findings reveal that participants found it easier to achieve daily tasks when specific goals were established. Moreover, participants expressed their desire to expand their self-management goals to include additional dimensions of health, such as monitoring sleep and emotions. In terms of hypertensive patients’ attitudes toward the visual-based cues, a strong connection between the avatar and their own health status was perceived, highlighting the significance of this metaphoric linkage. In addition, the results indicate that tailored time-based reminders, blood pressure monitoring, and daily dietary intake were the most appealing features. On the other hand, participants also mentioned some barriers they encountered in maintaining self-management habits. The demands of busy work and disruptions in routines were identified as risk factors for medication adherence. External factors, such as family members preparing meals or social activities, also had an impact on dietary intake.
To better reflect the proposed design and contribute to future eHealth design for habit formation, we discuss implications from perspectives of designing intention, automatic cue-behavior association, and self-management. By aligning behavior change strategies with the suggested design implications for the habit formation eHealth design, our findings could serve as a guideline for future studies (as shown in Table 6).
Design implications for the habit formation eHealth design.

Design for intention
When designing eHealth solutions for self-managed habit formation, it is crucial to consider not only the general goals of the non-pharmacological interventions but also adapted goals that align with individuals’ health status. Physician's medical advice that includes various critical interventions has been demonstrated to reduce blood pressure, such as weight loss, sodium reduction, or increased physical activity,2,28 which proposes an ideal guideline for chronic disease. Despite clinic medical advice providing professional, multidimensional, and customized instructions for patients, it is challenged by ambiguous and long-term goals, vague information, and sufficient expertise requirements when utilized in eHealth solutions.
Clear, quantitative, and narrow properties should be applied to medical advice-guided goals. These specific requirements could reduce learning barriers and increase self-efficacy to perform a specific behavior.19,20 Interview results reflect that participants prefer to set reduction targets to avoid the influence of internal and external factors, such as laziness, lack of knowledge, or being busy at work. In addition to implementing medical advice by reducing complex activities to multiple specific goals, participants perceive it easier to use the eHealth solution to do decision-making based on quantified goals. For instance, general medical advice suggests reducing sodium intake. However, patients report that they do not know the standard for sodium intake, and it is hard to measure the sodium content of each food. Through self-monitoring, the proposed design provides scientifically quantified goals and feedback, which could assist in deciding whether to reduce the intake of some foods. Additionally, our findings reveal that integrating personal health status and phases into goals to provide adaptive goals has benefits for individual habit formation. Existing studies have proposed rule-based adaptive goals to enhance physical activity levels, such as increasing 10% goals each week.32,51 However, this rule-based goal setting fails to achieve fully personalized goal adjustment based on individuals’ circumstances. Future studies could assess individuals’ status based on behavior data through advanced technology to provide tailored and adaptive goals in the appropriate context.
Comparing standard medical advice with individual behaviors is another key insight found in this study, which highlighted the importance of medical advice-guided goal-setting design. Individuals seek feedback by comparing it with the standard in order to understand and reflect on their behavior. However, one limitation of clinical consultation is that patients perceive pervasive and valueless feedback. 23 Patients may struggle to understand why and how to modify their behavior without detailed explanations. They desire to know the gap or progress of goal achievement and adjust their activities to enhance goal effects. Previous studies have utilized visual feedback to represent users’ overall status and the gap with standard medical suggestions. 52 In contrast, this study proposed detailed and explicit feedback (visualized progress bar) for each key medical recommendation, aiming to help users understand the consequences of their actions and compare them to standard and quantitative medical advice. Some participants adjusted their daily diets based on this visualized feedback during the experiment.
Time-based Reminders integrated with goal-setting could enhance goal performance and assist decision-making, which is consistent with findings from other research.28,53 Two types of reminders are reported by participants, including behavior reminders and alerts when standards are exceeded. Behavior reminders (e.g. medication reminders) are mentioned frequently by patients with limited time since their routines are easily disrupted by various situations. Moreover, participants present that alerts are acceptable when they maintain unhealthy behavior for a few days, or their health condition is predicted to be dangerous. It is necessary for them to monitor and understand their health conditions. Therefore, customized reminders are recommended to explore the chronic disease context to satisfy the complex requirements of patients, as most of them may have complications.
Community-based social support could potentially improve adherence. Most participants explore chronic disease-related knowledge from physicians or authorities. However, seeking suggestions from people in the same situation is also found to be a possible solution in this study. Individuals reflect on their behavior by learning lifestyle modification methods from others in similar situations. Prior studies have demonstrated the effectiveness of social support techniques in eHealth solutions,31,32,54 which aligned with the findings in this study.
Design for automatic cue-behavior association
Despite the positive attitudes expressed by all participants toward avatar appearances as the visual-based cues for habit formation, user demographic information such as age or available time should be considered a moderator in future design.
Personalized, implicit, and metaphoric avatar appearance transformation, in this study, represents the user's health condition and progression of medical advice goals. Most participants accepted that the changing of avatar appearances could enhance their motivation to self-management. In addition, avatar appearances serve as an implicit cue that links self-management behavior with visual change, allowing the cue-behavior association to develop without the need for additional attention. Although the metaphorical information of the avatar could be perceived by all participants, the randomness of the avatar's appearance is only highlighted by the participants with younger ages. Unpredictable outcomes could enhance individuals’ curiosity, encouraging them to keep using the app. These participants may have more experience with mobile applications, which may be one of the reasons. They can easily predict the shape changes of avatars based on their experience. In terms of retirement groups, those with less experience with mobile applications perceive a vivid transformation of the avatar's appearance. In contrast, older participants with retired status are less affected by the virtual avatar since they have a constant lifestyle routine. Future studies are suggested to consider the target group's characteristics.
Different reward properties have the potential to stimulate engagement. On the one hand, rewards could be the means of knowledge acquisition. Information related to chronic diseases could inform patient guidance, which could improve patients’ health literacy. On the other hand, personalized recommendations could be the reward. Individuals receive tailored feedback based on their behavior, which could enhance self-reflection and facilitate lifestyle modification.
Others
In addition to design suggestions for intention and cue-behavior association in eHealth solutions, some interesting findings are explored in this study.
Multi-dimensional health data monitoring has been discovered to play a vital role in future lifestyle modification eHealth solutions. Almost all participants expected the need to track their health condition in multiple dimensions, such as physical activity, dietary intake, sleep, and emotion. In particular, emotion has an influence on blood pressure control, which pay much attention by hypertensive patients. What's more, the mutual effect may be found between different dimensions. Most prior medical advice is evidenced by quantitative and one-dimensional standards (e.g. aerobic exercise could reduce systolic blood pressure by 5–8 mm Hg in adults with hypertension 5 ). The mutual effect of multi-dimension may influence the effectiveness of medical advice. Future research could focus on predicting the connection between different health data through multimodal deep learning.
Conducting self-experimentation is one of the characteristics of chronic disease patients. Self-experimentation for behavior change was proposed by Karkar et al., which is a process for formulating and testing proposed hypotheses. 55 In this study, some patients performed this process since they hoped to test whether specific foods would make their blood pressure unstable. Due to the complexity of managing chronic diseases and the fact that individuals may have different complications, patients cannot receive detailed explanations of their individual conditions. They could only explore their personalized plans through self-experimentation. Therefore, future work could apply a self-experimentation strategy for chronic disease that integrates big data to create a digital twin of patients to predict the results of patients’ hypotheses and assist lifestyle modification.
Limitations
In this study, dietary preferences and lifestyle habits are restricted in the Hong Kong context, which requires more regional exploration in the future. Findings show that different demographic information about participants is a potential moderator for eHealth solutions. We will consider more detailed groups in the future to explore the user experience of chronic diseases based on varied demographic traits.
Conclusions and future work
This study proposed that visual-based cues could help form self-management habits for hypertension. Results from this study show that medical advice-guided proximal and specific goals could be an effective strategy for chronic disease management. In addition, avatar appearance changes could be a visual-based cue to develop cue-behavior associations but were limited by demographic traits.
Currently, the medical advice applied in this study is based on general recommendations based on the authority's reports. Future studies will apply advanced technologies such as deep learning (DL) and natural language processing (NLP) to transfer medical advice based on the user's input to detailed and valuable sub-goals in order to achieve personalized self-management of chronic disease. 56 Meanwhile, we found that patients try to verify the influence of different lifestyles on blood pressure control. Future work could use digital twins 57 to establish an individual disease prediction model that can present the influence of different lifestyles in an intuitive way. The results of the current study show that retired patients (the elderly) perceived the gamification design as less impressive. The revisit results indicated that a lack of mobile application experience might be a potential barrier. Hence, we plan to conduct a large-scale survey to explore mobile application experience among the elderly with chronic diseases (e.g. an elderly-centered design approach 58 ) to explore their preferred design elements and interactive features. In addition, more empirical studies should investigate the mechanisms of visual-based cues and other types of cues in order to support self-management habit formation in different contexts. This will contribute to improve the design and development of future habit formation studies for chronic disease management.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241265217 - Supplemental material for Developing cue-behavior association for habit formation: A qualitative study to explore the role of avatar in hypertension
Supplemental material, sj-docx-1-dhj-10.1177_20552076241265217 for Developing cue-behavior association for habit formation: A qualitative study to explore the role of avatar in hypertension by Yujie Zhu, Yonghao Long, Lai Wei, Yaqi Zhang, Zhengtao Ma, Kun-Pyo Lee, Lie Zhang and Stephen J. Wang in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241265217 - Supplemental material for Developing cue-behavior association for habit formation: A qualitative study to explore the role of avatar in hypertension
Supplemental material, sj-docx-2-dhj-10.1177_20552076241265217 for Developing cue-behavior association for habit formation: A qualitative study to explore the role of avatar in hypertension by Yujie Zhu, Yonghao Long, Lai Wei, Yaqi Zhang, Zhengtao Ma, Kun-Pyo Lee, Lie Zhang and Stephen J. Wang in DIGITAL HEALTH
Supplemental Material
sj-xlsx-3-dhj-10.1177_20552076241265217 - Supplemental material for Developing cue-behavior association for habit formation: A qualitative study to explore the role of avatar in hypertension
Supplemental material, sj-xlsx-3-dhj-10.1177_20552076241265217 for Developing cue-behavior association for habit formation: A qualitative study to explore the role of avatar in hypertension by Yujie Zhu, Yonghao Long, Lai Wei, Yaqi Zhang, Zhengtao Ma, Kun-Pyo Lee, Lie Zhang and Stephen J. Wang in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors wish to thank all participants for their time and commitment to this study.
Author contributions
YZhu, YLong, and YZhang researched literature and conceived the study. LWei and ZMa were involved in prototype development, gaining ethical approval, patient recruitment, and data analysis. YZhu wrote the first draft of the manuscript. SJWang supported the key concept develop, supervised the overall project progress, edited and prove-red the manuscript and secured funding support for this study. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Consent statement
All participants were provided with detailed information regarding the research objectives, experimental procedures, and the types of data collected during the experiments. Each participant signed a consent form indicating their voluntary agreement to take part in the study.
Data availability
The interview data are confidential due to the consent commitments signed by participants. The results can only be viewed by researchers in this study, but data is available upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The project has been approved by the PolyU Institutional Review Board (PolyU IRB) (HSESC Reference Number: HSEARS20211006003).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Laboratory for Artificial Intelligence in Design (Project Code: RP2-4) under the InnoHK Research Clusters, Hong Kong Special Administrative Region Government; the work was substantially supported by the Projects of Strategic Importance of The Hong Kong Polytechnic University (Project ID: P0036851, P0043542) and the University's Research Centre for Future (Caring) Mobility (Project ID: P0042701) of The Hong Kong Polytechnic University.
Guarantor
YZhu.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.