
Abstract
Background
The rapid development of Information and Communications Technology has made eHealth a transformative force in healthcare. However, it has also exacerbated the “digital health divide.” While urban older adults benefit from easier access to digital health information and services, their rural counterparts face significant barriers in leveraging eHealth advantages.
Objective
Guided by capital theory, this study investigates the digital health divide and its determinants among urban and rural older adults. The findings aim to inform targeted interventions that promote digital health equity.
Methods
Exploring the digital health divide among urban and rural older adults in China: a cross-sectional study based on capital theory. Analysis of variance is used to validate the digital health divide among urban and rural older adults, while structural equation modeling examines contributing factors. Additionally, the Blinder-Oaxaca decomposition method identifies the primary drivers of these disparities.
Results
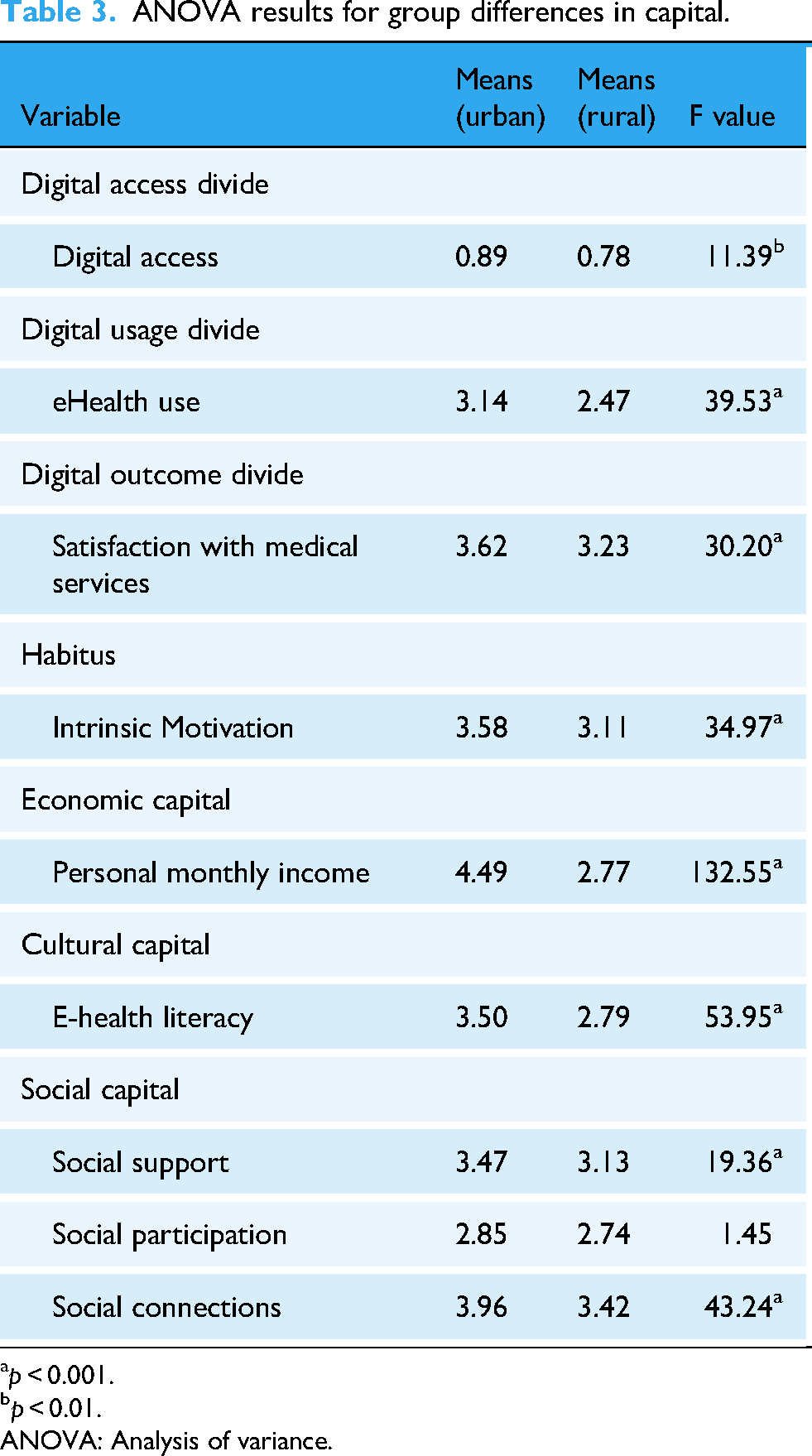
Three levels of the digital health divide exist among urban and rural older adults: digital access divide (F = 11.39, p < 0.01), digital usage divide (F = 39.53, p < 0.001), and digital outcome divide (F = 30.20, p < 0.001). The influence of these divides propagates along the digital chain, with digital access divide significantly affecting digital usage divide (β=0.060, p < 0.05) and digital usage divide further impacting digital outcome divide (β=0.363, p < 0.001). Among these, digital usage divide is the most pronounced, primarily driven by disparities in cultural capital (β=0.221, p < 0.001), social support (β=0.361, p < 0.001), economic capital (β=0.111, p < 0.01), and habits (β=0.248, p < 0.001). Blinder-Oaxaca decomposition further reveals that cultural capital (33.9%) and social capital (22.5%) are the key contributors to the urban–rural digital usage divide among older adults.
Conclusion
To address these divides among urban and rural older adults, interventions in policy, motivation, economy, culture, and society are recommended.
Introduction
Background
With the advancement of global digitalization, eHealth has emerged as a prominent service delivery model. The Chinese government has implemented a series of policies to promote eHealth development, including the April 2018 “Guidelines on Promoting the Development of eHealth” issued by the General Office of the State Council and the July 2018 “Interim During the COVID-19 pandemic, restrictions on in-person medical services accelerated the adoption of eHealth as an alternative solution in China. 2 Consequently, the number of online consultations and users of digital healthcare platforms surged rapidly within a short period. 3 While eHealth has demonstrated efficacy in pandemic response, this large-scale implementation has also revealed disparities in health outcomes. Studies indicate that inequities in access to and utilization of digital health services may exacerbate health inequalities, particularly in chronic disease management. 4
Digital health divide poses a significant challenge to global health equity as healthcare becomes increasingly digitized.5,6 In low-and middle-income countries, divides in digital infrastructure, literacy, and policy frameworks disproportionately affect marginalized populations like rural and elderly communities, denying them access to eHealth services. 7 This disparity not only hinders digital health's potential to transform chronic disease care but also widens existing health inequities,8,9 as the populations needing these innovations most often benefit least. 10 Without targeted interventions, the achievement of global health equity will remain elusive.
Health inequalities between urban and rural older adults are well-documented, with studies consistently showing that urban residents enjoy better health outcomes than their rural counterparts. 11 Rural populations exhibit higher prevalence rates of chronic diseases, functional impairments, and depression. 12 Moreover, disparities in digital health adoption may exacerbate these existing health inequities. Older adults in rural areas often face socioeconomic constraints and limited resource availability, placing them at a structural disadvantage in accessing and utilizing digital health technologies. 13 Consequently, they may struggle to benefit from the potential dividends of digital healthcare. Given these challenges, it is critical to examine the existence and underlying mechanisms of the urban–rural digital health divide among older adults. Such research holds significant implications for promoting equitable access to digital health benefits and advancing the equalization and fair distribution of digital healthcare services. This issue warrants broader societal attention as a pressing public health concern.
The disparities in access, utilization, and derived benefits from digital health among different population groups are collectively termed the “digital health divide.” 14 This divide operates across three distinct levels: The first-level divide (digital access divide) reflects inequalities in access to Information and Communications Technology (ICT); the second-level divide (digital usage divide) pertains to disparities in ICT usage capabilities; the third-level divide (digital outcome divide) captures differences in health benefits obtained through digital health engagement.14,15 While existing research has predominantly examined the first two levels,16-21 investigations into the digital outcome divide remain limited. 15 Crucially, there is a paucity of systematic studies examining all three levels concurrently. These divides are likely interrelated, as digital access serves as a prerequisite for digital health utilization, which subsequently influences healthcare accessibility and ultimately contributes to health outcome disparities. 22 A comprehensive examination of this three-tiered divide would advance our understanding of their interconnections, yielding more robust and nuanced insights. Such research holds significant policy implications, as it could guide targeted interventions to mitigate digital health divide and promote health equity.
Extant research has extensively investigated the determinants of digital health divide, with particular emphasis on demographic and socioeconomic factors.10,22-25 For instance, Tappen et al. demonstrated that individuals with higher educational attainment, income levels, or of European descent were five times more likely to access online health information compared to those with lower socioeconomic status or from ethnic minority groups. 21 While these studies have significantly advanced our understanding of digital health divide, their practical implications remain limited. Demographic characteristics such as age, gender, race, and education level are typically immutable in the short term, constraining the development of immediate interventions to mitigate disparities.
Given that digital access and usage patterns are profoundly shaped by societal and familial environments,
26
Bourdieu's capital theory provides a powerful framework to analyze these disparities. This is particularly relevant in China's context, where rapid but uneven digitalization has exacerbated existing inequalities. First, urban areas benefit from superior economic capital (e.g. digital infrastructure, disposable income) and cultural capital (e.g. digital literacy), while rural regions face compounded disadvantages due to systemic barriers like the hukou system and unequal healthcare resource allocation.
1
Second, this entrenched urban–rural divide further reinforces disparities in social capital—particularly in networks facilitating access to digital health resources.
12
By applying Bourdieu's framework through its four key dimensions (habitus, social capital, economic capital, and cultural capital), we investigate how these dimensional disparities drive digital health divide among urban and rural older adults. This theoretical foundation leads us to address the following research questions (RQ):
RQ1: Do the different levels of digital health divide exist among rural and urban older adults under eHealth conditions? RQ2: What factors contribute to the formation of different levels of the digital health divide among urban and rural older adults?
This study focuses on Beijing, a Chinese megacity with a population of 21.843 million, characterized by advanced internet infrastructure (89.7% penetration rate) 27 and widespread eHealth adoption. By examining three-level digital health divide, our research reveals how digital technologies differentially affect various demographic groups. As China's political and cultural capital, Beijing presents a unique case study with both a high urbanization rate and a persistent urban–rural dichotomy. Investigating digital health disparities among Beijing's urban and rural older adults provides valuable insights into how digital technologies impact aging populations. This research holds both theoretical and practical significance. Not only does it offer forward-looking perspectives on digital health equity, but it also provides important implications for developing countries seeking to bridge digital divides in healthcare access.
Theoretical basis and hypotheses development
The digital health divide
Digital health divide, an extension of digital divide research, manifests across three distinct dimensions: access, usage, and outcome disparities. 28 Digital access divide reflects inequalities in digital health technology adoption, typically measured by device ownership (e.g. mobile phones). 24 Digital usage divide captures variations in how different populations employ these technologies, encompassing differences in application methods, frequency, and skill levels. 14 China's recent eHealth initiatives have driven substantial growth in digital healthcare services, 1 making usage patterns particularly relevant for study. Accordingly, this research operationalizes digital usage divide through measurable indicators of eHealth engagement.
Digital outcome divide refers to the differences in benefits obtained by different groups due to adoption and utilization of digital health. 15 These benefits can be categorized into short-term and long-term outcomes. Short-term outcomes from eHealth might include improved satisfaction with medical services due to enhanced convenience, 29 while long-term outcomes might include improvements in health outcomes. Given the prolonged pathways to improving health outcomes, this study utilizes the measurement of satisfaction with medical services as a proxy for expressing digital outcome divide. Satisfaction with medical services is an important indicator in assessing the quality of healthcare services and the performance of the healthcare system, encompassing factors such as reduced waiting time, optimized medical processes, convenience in payment, and medication collection, among others.22,30
The three-level digital divide framework
31
points out that the second-level digital divide is caused by the first-level digital divide and other contextual factors. For instance, training in digital skills has a greater impact on people who own computers than on those who don’t, indicating that second-level digital divide may increase along with the first-level digital divide.
32
The third-level digital divide arises from the first and second levels of the digital divide as well as other background factors. For example, students with poor computer skills tend to have lower e-learning outcomes.
33
Based on this, it is believed that under the health context, there may still be interactions among the three levels of digital divide, and the impact of digital health divide will be transmitted along the digital chain, i.e. thus, we hypothesize as follows:
Hypothesis1a (H1a): The digital access divide will promote the generation of digital usage divide; there is a cascading effect on digital health divide among urban and rural older adults. Hypothesis1b (H1b): The digital usage will promote the generation of digital outcome divide; there is a cascading effect on digital health divide among urban and rural older adults.
Bourdieu's capital theory
The theory of capital was proposed by the renowned French philosopher Bourdieu in 1980. He posited that capital serves as the driving force behind human action, encompassing not only economic capital but also cultural and social capital. This framework can be utilized to comprehend the interplay between social structures, living conditions, and human behavior. 34 Bourdieu also introduced the concept of habitus, underscoring the internalized aspect of an individual's accumulated capital and resources, which shape various behavioral tendencies. 27 Thus, this study seeks to employ Bourdieu's capital theory to explore the disparities in capital possession among urban and rural older adults and their impact on digital health divide.
Habitus refers to individuals’ dispositional orientations toward specific behaviors and their anticipated outcomes,
34
serving as cognitive frameworks that guide action. As a psychological resource, habitus comprises both intrinsic and extrinsic motivational components.
26
Intrinsic motivation stems from internal rewards such as personal fulfillment and enjoyment, whereas extrinsic motivation derives from external incentives. Within eHealth adoption among older adults, intrinsic motivation plays a pivotal role as it reflects their internalized perceptions and values regarding technology use. This study specifically examines intrinsic motivation as a core dimension of habitus, positing that it drives active engagement with digital health technologies. Existing research substantiates the influential role of motivation in shaping health behaviors.
35
Moreover, eHealth systems enhance healthcare accessibility and efficiency. When older adults perceive that eHealth services align with their needs and expectations, this congruence fosters greater satisfaction with medical care. Based on this theoretical foundation, we propose the following hypotheses:
Hypothesis2a (H2a): Intrinsic motivation in older adults positively influences their digital access. Hypothesis2b (H2b): Intrinsic motivation in older adults positively influences their eHealth use. Hypothesis2c (H2c): Intrinsic motivation in older adults positively influences their satisfaction with medical services.
Economic capital, in Bourdieusian terms, encompasses material wealth and financial resources available to individuals or households.
36
In operational terms, researchers commonly measure this construct through personal or household income and assets, which serve as proxies for economic resource availability. For this study, we quantify older adults’ economic capital using monthly personal income. Empirical evidence demonstrates that greater economic resources facilitate digital access. Specifically, older adults with higher incomes exhibit: Greater capacity to acquire smart devices (as demonstrated by Medero et al.'s findings on income-mobile device correlation
37
), and higher propensity to utilize eHealth services. These economic advantages create a positive cascade effect: enhanced eHealth adoption leads to better healthcare accessibility, improved service quality, and ultimately greater medical satisfaction. Cao's research corroborates this relationship, showing household income significantly predicts satisfaction with healthcare process factors like wait times and treatment procedures.
22
Based on this theoretical and empirical foundation, we propose the following hypotheses:
Hypothesis3a (H3a): The personal monthly income of older adults positively impacts their digital access. Hypothesis3b (H3b): The personal monthly income of older adults positively influences their eHealth use. Hypothesis3c (H3c): The personal monthly income of older adults positively affects their satisfaction with medical services.
Cultural capital is a significant cognitive resource that signifies the possession of cultural resources by individual.
38
This study selected e-health literacy as the manifestation of cultural capital. E-health literacy, defined as the ability of individuals to seek, understand, evaluate, and apply health information from electronic sources, can influence their health behaviors related to digital technology.
39
Hence, this study selected e-health literacy as the manifestation of cultural capital. Older adults with higher eHealth literacy possess confidence in their ability to adapt to and utilize digital technologies, enhancing their digital access and usage.
40
Lastly, older adults with higher eHealth literacy effectively utilize medical services to meet their health needs,
41
preferring positive medical experiences and thus increasing their satisfaction with medical services. Thus, the following hypotheses are proposed:
Hypothesis4a (H4a): The eHealth literacy of older adults positively influences their digital access. Hypothesis4b (H4b): The eHealth literacy of older adults positively impacts their eHealth use. Hypothesis4c (H4c): The eHealth literacy of older adults positively influences their satisfaction with medical services.
Social capital, defined as the resources and relationship networks within social networks, plays a crucial role in determining the size of resources available to individual. 42 It is mainly divided into cognitive and structural social capital. Cognitive social capital refers to shared values between individuals, including trust, reciprocity, and cohesion. 43 Structural social capital refers to the forms of connections between individuals, including social support, social connections, and social participation. This article focuses on structural social capital. By studying structural social capital, we can more accurately understand the differences in the positions and resource acquisition abilities of urban and rural older adults in social networks, as well as the direct impact of these differences on the digital health divide.
Social participation refers to an individual's involvement in activities that facilitate interaction within the community or society. This encompasses a wide range of actions, including leisure pursuits and volunteer work.
12
Social support, on the other hand, denotes the assistance and resources—both emotional and material—provided by others.
44
Meanwhile, social connection pertains to the broader network of relationships and interactions that foster a sense of belonging and attachment.
45
For older adults, higher levels of social support, active social participation, and extensive social connections can enhance access to information and resources, thereby increasing their likelihood of adopting digital technologies. Empirical evidence suggests a causal relationship between social capital and improved digital access.
46
Moreover, social support plays a critical role in helping older adults overcome technical barriers associated with eHealth. Active social participation and robust social networks also facilitate their access to medical services. Studies have demonstrated that older adults are less likely to utilize eHealth services if they lack proximity to their children.
47
Hypothesis5a (H5a): The social support, social participation, and social connection of older adults have a positive impact on their digital access Hypothesis5b (H5b): The social support, social participation, and social connections of older adults have a positive impact on their eHealth use. Hypothesis5c (H5c): The social support, social participation, and social connection of the older adults have a positive impact on their satisfaction with medical services.
Based on the above analysis, the research model for this study is shown in Figure 1.

Theoretical model of digital health divide among urban and rural older adults.
Methods
Study design and sample
This cross-sectional study was conducted in Beijing, China, between October and December 2023, using paper-based questionnaires. A multi-stage sampling approach was employed to ensure geographic diversity: first, one district was selected from each of the urban, suburban, and rural regions. Subsequently, one urban community and one rural community were randomly chosen within each selected district.
In structural equation modeling (SEM), a baseline sample size of 200 is recommended, with an increment of 5–10 participants per observed variable. Given the 7 latent variables in this study and accounting for a 20% potential invalid response rate, the estimated minimum required sample size was 294–338 participants. A total of 520 questionnaires were collected, with 501 deemed valid after logical checking, resulting in a high effective response rate of 96.3%.
In this study, the inclusion criteria for participants were 1) aged 55 or above; 2) willing to participate and sign an informed consent form; 3) capable of oral communication in Chinese. The exclusion criteria were 1) serious physical or mental illnesses that may affect health assessment and quality of life; 2) inability to understand or answer the survey questionnaire.
Instrument measurement
The independent variables in this study comprised habit (representing intrinsic motivation) and three forms of capital, economic capital: measured by personal monthly income; cultural capital: assessed through e-health literacy; social capital: operationalized as social support, social participation, and social connections. These variables were treated as latent constructs, with their specific measurement items detailed in Table 1. Importantly, we controlled for several potential confounding variables: age, education level, and self-rated health. Self-rated health was measured on a 5-point Likert scale (1 = very poor to 5 = excellent). These covariates were selected based on previous research demonstrating their influence on digital health divide formation. 22
Instrument measurement.

The dependent variables in this study operationalize three-level digital health divide, conceptualized based on the framework proposed by Cao. 22 Specifically: digital access divide: assessed by whether participants owned a mobile phone; digital usage divide: measured through older adults’ engagement with eHealth services; digital outcome divide: evaluated based on participants’ satisfaction with healthcare services. Detailed measurement items for each variable are presented in Table 1, with the complete survey instrument available in Multimedia Appendix 1.
Quality control
Questionnaire Design Phase: The questionnaire was developed following a thorough literature review, expert consultations, and team discussions; Pilot Survey Phase: A pilot experiment was conducted in Fengtai District, Beijing in September 2023. Feedback from 34 collected questionnaires led to questionnaire modifications; Enumerator Training Phase: In September 2023, enumerators were recruited and trained on survey purposes, data collection techniques, and ethical considerations; Questionnaire Distribution Phase: Adherence to sampling requirements and randomization principles ensured an expanded sample size. Surveys were conducted during health education sessions at community healthcare centers; Data Processing Phase: Following questionnaire collection, two individuals conducted logic checks and data screening. Criteria included excluding inconsistent logic, completion rates below 90%, and patterns in selected options.
Statistical analysis
Descriptive analyses were performed using SPSS 26. Categorical variables are reported as n (%), while continuous variables are expressed M ± SD. To assess regional differences in study indicators, one-way analysis of variance was employed to compare outcomes among urban and rural older adults.
In SEM analysis, scale reliability was evaluated using Cronbach's alpha coefficients. For scale validation, we assessed: convergent validity, discriminant validity, and structural validity. SEM was performed using AMOS 24 software to analyze the influence of capital dimension factor on digital access, eHealth use, and satisfaction with medical services.
Blinder-Oaxaca decomposition analysis, after confirming the presence of digital health divide and the influence of capital factors on it, the Blinder-Oaxaca decomposition analysis was employed to evaluate the relative significance of these driving factors in mitigating the divide. Utilizing Stata 17 software, this method calculates the contribution rates of each factor, elucidating the primary factors influencing the divide's formation.
Results
Characteristics of the study participants
A total of 501 participants were included in the analysis, among them, 50.50% were in urban areas and 49.50% were in rural areas. The average age was 64.69 ± 6.82 years, about half of the older adults had a high school education or above, and over four out of five older adults had digital access. Table 2 summarizes other demographic characteristics.
Characteristics of the older adults in urban and rural areas.

The existence of digital health divide and capital disparities
As shown in Table 3, there are significant differences in digital access, e-health use, and medical service satisfaction among older adults in urban and rural areas, which indicates that there is a three-level divide. There are also significant differences in intrinsic motivation, personal monthly income, e-health literacy, social support, and social connections among urban and rural older adults. However, there was no significant difference in social participation.
ANOVA results for group differences in capital.
p < 0.001.
p < 0.01.
ANOVA: Analysis of variance.
Reliability and validity tests of digital health divide model
To evaluate the reliability and validity of the scales, we performed a principal component analysis. The Kaiser–Meyer–Olkin measure of sampling adequacy was excellent (0.943), and Bartlett's test of sphericity was significant (p < 0.05), confirming the suitability of the data for factor analysis. The analysis yielded seven factors, collectively accounting for 85.80% of the total variance.
We further examined scale reliability using Cronbach's alpha, with all values exceeding 0.8, demonstrating strong internal consistency. Convergent validity was supported by composite reliability values above 0.7 and average variance extracted (AVE) values exceeding 0.5 (see Table 4). Discriminant validity was established, as the square root of each scale's AVE was greater than its correlation coefficients with other scales (see Table 5).
Reliability and convergence validity.

CR: composite reliability; AVE: average variance extract.
Discriminate validity.

Note. The bolded numbers represent the square roots of the AVE for each variable, which are used to assess whether the scale has sufficient discriminant validity.
The relationship between capital factors and digital health divide
The fit of the model was examined using maximum-likelihood estimation, as shown in Table 6. The CMIN/DF ratio was 2.715, the RMSEA was 0.059, and the CFI was 0.957, all of which fell within an acceptable range. Other fit indices of the structural model also met the reference values, indicating an acceptable model fit.
Fit indices of the structural model.

Table 7 presents both standardized and unstandardized coefficients (β) with corresponding p-values. Figure 2 displays the path analysis results, where significant (p < 0.05) and non-significant relationships are represented by solid and dashed lines, respectively. The analysis revealed a significant sequential pathway: digital access positively predicted eHealth use (β = 0.060, p < 0.05), which in turn predicted greater satisfaction with medical services (β = 0.363, p < 0.001). This cascade effect supports hypotheses H1a and H1b, demonstrating a progressive digital health divide.

Path diagram of digital health divide model.
Path coefficient analysis of digital health divide model.

The latent influence of older adults’ capital reflects the extent of digital health divide, with the variables and coefficients of eHealth use being greater than those of digital access and satisfaction with medical services. Therefore, our study suggests that digital usage divide is the main level of digital health divide.
Among them, intrinsic motivation (β=0.248, p < 0.001), personal monthly income (β=0.111, p < 0.01), e-health literacy (β=0.221, p < 0.001), and social support (β=0.361, p < 0.001) have significant positive effects on eHealth use among the older adults, supporting H2b, H3b, H4b, and partial supporting H5b. Social connections have a weak relationship with digital access (β=0.184, p < 0.05) and satisfaction with medical services (β=0.180, p < 0.01), partial supporting H5a and H5b.
The major contributors to digital health divide
As presented in Table 8, the explanatory variables account for 55.0% of digital access divide among urban and rural older adults, with social connections (96.7%) emerging as the most influential factor. For digital usage divide, the variables explain 89.6% of the variance, where improvements in e-health literacy (30.9%), social support (22.5%), personal income (20.6%), and intrinsic motivation (18.7%) could collectively mitigate this divide. Regarding digital outcome divide, the model clarifies 98.9% of its formation, primarily driven by eHealth use (51.2%). These findings align with our SEM analysis, demonstrating a cascading effect in digital health divide, where capital factors indirectly shape disparities in digital outcomes.
Blinder-Oaxaca decomposition results of digital health divide.

p < 0.001.
p < 0.01.
p < 0.05.
N/A: not applicable.
Discussion
Findings related to digital health divide among urban and rural older adults
Applying capital theory, this study empirically validates the three-level digital health divide (access, usage, and outcome) among urban and rural older adults. SEM confirms a cascading mechanism across these levels, with digital usage divide serving as the central nexus. Our analysis identifies social connections as the predominant factor influencing access disparities, while e-health literacy, social support, and intrinsic motivation constitute the core determinants of usage inequality. Crucially, digital usage divide directly predicts outcome disparities. The principal findings reveal that:
First, our empirical results demonstrate significant urban–rural disparities in older adults’ digital health engagement, spanning access, usage, and outcomes. This finding aligns with Lum et al.'s pandemic-era research showing rural patients’ lower telemedicine adoption rates compared to their urban counterparts. 52 Second, we identify a propagation mechanism where digital health disparities create cascading effects that amplify health inequalities. This phenomenon mirrors Cao et al.'s findings regarding sequential disparities in mobile health application use among Chinese outpatients. 22
Third, our analysis reveals critical dimensions of digital health divide. Digital usage divide represents the most pronounced manifestation, evidenced by both a greater number of significant variables and stronger path coefficients compared to access and outcome divides. Our findings establish a clear hierarchy of contributing factors to usage disparities: cultural capital (primary), followed by social capital, economic capital, and habitual factors. While infrastructure improvements have mitigated access disparities between urban and rural regions, 53 and outcome disparities currently reflect latent cumulative effects whose full impact remains unrealized, 26 persistent usage inequalities continue to constitute the most substantial driver of digital health inequities.
Fourth, capital dimension analysis reveals four key influencing factors. 1) Habitual factors positively contribute to digital usage divide. Older adults with intrinsic motivation—such as technological adaptability and strong health consciousness—demonstrate more active engagement with eHealth tools for health management. 54 2)Economic capital exacerbates usage disparities, as greater financial resources facilitate access to eHealth services (e.g. purchasing devices) and reduce cost-related barriers. 55 3) Cultural capital, particularly e-health literacy, promotes digital usage inequality by enabling older adults to navigate online health resources, schedule appointments, and purchase medications more efficiently, thereby increasing eHealth adoption. 56 4) Social capital plays a multifaceted role: social support directly fosters the digital usage divide by enhancing willingness to use eHealth tools through family/peer encouragement, technical assistance, and knowledge sharing. 57 Social connections further amplify access and outcome disparities by providing information resources and support networks, improving comprehension of eHealth services. 58
Contribute to the literature on digital health divide
This study has several theoretical implications. It contributes to the literature on digital health divide by providing evidence of digital health divide among rural and urban older adults in China. While previous research has mainly focused on digital access and usage divides,46,59 this study offers a more systematic analysis of a three-levels divide. It confirms that rural older adults have lower levels of digital access, eHealth use, and satisfaction with medical services, with these disparities showing cumulative effects. Furthermore, in this study, the three-levels divide in the current context is manifested as digital access, eHealth use, and satisfaction with medical services of different social groups (such as rural and urban older adults), which is helpful for future research to measure the three-levels divide.
Second, it provides literature support for research in developing countries by highlighting that digital health divide among urban and rural older adults in China primarily manifests as digital usage divide. For developing nations, where the costs of digital access are decreasing and digital technologies become more widespread, digital access divide may not be the main issue. 22 Therefore, targeted interventions can only be effectively implemented if the current stage of digital health divide is clear, which can provide relevant references for this.
Last, it contributes to the literature on digital health divide by uncovering the determinant factors in current context. As mentioned earlier, research on the determinants of digital health divide is lacking, with few studies investigating demographic or socioeconomic determinants such as age and socioeconomic factors.22-24 This study is from the capital perspective and highlights that different levels of divide necessitate different responses, with digital access divide closely linked to social connections, digital usage divide tied to cultural capital and intrinsic motivation, and digital outcome divide primarily stemming from digital usage divide.
Interventions are carried out from: policy, motivation, economy, culture, and society
Table 9 summarizes interventions to bridge digital health divide among urban and rural older adults. Based on the empirical findings, this study provides recommendations for industry practitioners from five aspects: policy intervention, motivational intervention, economic intervention, cultural intervention, social intervention.
Practical suggestions of current study.

Limitations
This study has several limitations that warrant consideration. First, as a cross-sectional design, the causal relationships inferred through SEM should be interpreted with caution. Second, the reliance on self-reported measures could introduce response biases (e.g. social desirability bias or recall bias), which may affect the accuracy of the data. Third, while the sampling strategy accounted for geographic and economic factors, the exclusive focus on Beijing's urban and rural residents may limit generalizability to other regions with different socioeconomic or cultural contexts. Future studies could expand data collection to diverse regions to enhance external validity. Finally, the operationalization of digital outcome divide relied solely on short-term service satisfaction metrics. Longitudinal research tracking multidimensional outcomes—such as health status improvements and healthcare cost reduction—would provide a more robust assessment of long-term effects.
Conclusions
Using Beijing, China, as a case study, this research examines the urban–rural digital health divide among older adults, revealing a cascading effect across three levels: access, usage, and outcomes. The findings indicate that disparities in digital access and usage collectively contribute to unequal digital health outcomes, with usage differences being the primary driver. Grounded in capital theory, the study highlights the distinct roles of social and cultural capital in shaping these divides—social capital predominantly influences access disparities, while both cultural and social capital significantly affect usage patterns, ultimately impacting health outcomes. To bridge these divides, policymakers and society must prioritize improving older adults’ e-health literacy and strengthening social support systems.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251374122 - Supplemental material for Based on capital theory to exploring the digital health divide and determinants among urban and rural older adults in China: Cross-sectional study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251374122 for Based on capital theory to exploring the digital health divide and determinants among urban and rural older adults in China: Cross-sectional study by Yanbin Yang, Chengyu Ma, Haopeng Liu, Siyu Lv and Weizhen Liao in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank the General Project of Ministry of Education Foundation on Humanities and Social Sciences, China for their support, and every participant who volunteered to participate in our study.
Ethical approval
This study was approved by the Ethics Committee of Capital Medical University (approval no. Z2022SY076), we certify that the study was performed by the Declaration of Helsinki of the World Medical Association. Informed consents were obtained from the participants prior to the official start of the study. Participants’ information was anonymized throughout the study. After completing the survey, each participant was given a gift as gratitude.
Consent for publication
Consent for publication was obtained from each of our study participants.
Authors’ contributions
All authors contributed to the study conception and design. YY collected and analyzed data, wrote and modify the manuscript. CM designed the study, reviewed and edited the manuscript. HL assisted with data collected and analysis. SL assisted with data collected and analysis. WL assisted with data collected and analysis. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been funded by the General Project of Ministry of Education Foundation on Humanities and Social Sciences, China (grant number: 22YJAZH082).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
CM.
Multimedia appendix1
The survey questionnaire for this paper can be accessed through the following method: Multimedia Appendix1.docx
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.