
Abstract
Background
The deep integration of digital technology and healthcare services has propelled the healthcare system into the era of digital health. However, vulnerable populations in the field of information technology, they face challenges in benefiting from the digital dividends brought by digital health, leading to the emerging phenomenon of the “health digital divide.”
Methods
This study utilized the sample of 3547 urban from the 2021 Chinese Social Survey data for analysis. Models were constructed with digital access divide, digital usage divide, and digital outcome divide for urban residents, and structural equation modeling was implemented for analysis.
Results
The impact β coefficients (95% CI) of urban residents’ digital access on the frequency of digital use, internet healthcare utilization, and patient experience were (β = 0.737, P < 0.001), (β = 0.047, P < 0.05), and (β = 0.079, P < 0.001), respectively. Urban elderly groups were at a disadvantage in digital access and usage (β = −0.007, β = −0.024, and β = −0.004), as well as those with lower educational levels (β = 0.109, β = 0.162, and β = 0.045). However, these two factors did not have a significant direct impact on the patient experience in urban areas.
Conclusions
The health digital divide of urban residents exhibits a cascading effect, primarily manifested in the digital access and usage divide. To bridge health digital divide among urban residents, efforts must be made to improve digital access and usage among the elderly and those with lower educational levels.
Keywords
Introduction
Background
With the advent of the digital and intelligent era, the development of modern information technologies such as 5G, blockchain, and Internet+ has profoundly influenced people's production and lifestyle. The deep integration of modern information technology and healthcare services has driven the traditional healthcare system into the phase of digital health development. 1 Since 2014, the Chinese government has introduced a series of policy documents to support and guide the development of the internet healthcare utilization industry. 2 Subsequently, internet healthcare utilization platforms emerged, providing online consultations, telemedicine, and medicine delivery services, gradually gaining recognition and acceptance by users. 3 According to the 52nd Statistical Report on China's Internet Development, as of June 2023, the user base of internet healthcare utilization in China reached 364 million, accounting for 33.8% of the total number of internet users. Among them, the coverage rate of telemedicine services in counties and districts has reached 100%, and the telemedicine collaboration network has covered over 23,000 medical institutions in all prefecture-level cities. 4
However, certain population groups, such as the elderly, low-income individuals, and those with low educational levels, face inherent disadvantages in the field of modern information technology, making it difficult for them to benefit from the digital dividends brought by digital health.5–7 This has led to the growing prominence of the “health digital divide” phenomenon, which has attracted widespread attention both domestically and internationally. The health digital divide refers to the imbalance in the application and dissemination of digital technology in the healthcare field, manifested as disparities among different groups (e.g. the elderly, low-income individuals, and those in remote areas) in accessing health information, healthcare services, and health outcomes, which is one manifestation of the digital divide. 8
This phenomenon is prevalent in different countries and regions. A population survey covering 17 European countries showed that 51% of people aged 50 and above were unable to use internet healthcare services. 9 In the United States, the COVID-19 pandemic has exacerbated the impact of the digital divide on access to healthcare services for the elderly, minority groups, and people in remote areas. 10 The health digital divide not only affects patient experience and satisfaction 11 but also exacerbates social inequality and health disparities. 12 When some individuals are unable to access digital health technologies and services due to various factors, their health risks increase, further exacerbating the problem of health inequality. Additionally, due to a lack of access to health information and services, these individuals have fewer opportunities for disease prevention or early treatment, leading to increased demand and costs for healthcare resources and potential losses in socioeconomic benefits. As a result, the United Nations has recognized digital health as part of human rights and has urged member states to develop corresponding policies to promote internet accessibility and eliminate the health digital divide. 13 Previous research has shown that sociodemographic characteristics, particularly age, gender, education, and income, can predict access to and use of digital health technologies.14,15 However, previous studies have primarily focused on analyzing the divide from a single level, and focus on the research of digital access and usage divide,16–18 and systematic analyses of the three-level health digital divide are scarce.
With the increasing integration of the internet into social life, there are noticeable disparities between urban and rural residents in terms of digital access, usage, and healthcare services. Firstly, urban areas generally have broader internet coverage compared to rural areas, according to the 49th “China Internet Development Status Report,” as of December 2021, the internet penetration rate in urban and rural areas was 81.3% and 57.6% respectively. 19 Secondly, urban regions show higher usage rates of diverse online services such as e-commerce and online education. In contrast, rural internet users often focus more on instant messaging. 20 Additionally, urban residents have easier access to digital health services like online medical consultations and appointments. In contrast, rural residents face challenges accessing these services due to limited infrastructure and medical resources.16,21 Thus, the Chinese Social Survey (CSS) 2021 survey specifically targeted urban residents for internet healthcare utilization, so this study aims to identify the factors contributing to the formation of the health digital divide among urban residents, providing a scientific rationale for promoting digital health equity and social justice.
Theoretical foundation
The concept of the health digital divide is based on the digital divide and encompasses three key levels: digital access divide, digital usage divide, and digital outcome divide. 22 Firstly, the digital access divide, also known as the first-level divide, refers to the difference between users and non-users of digital technologies, 16 which is the most fundamental issue of the health digital divide. It is measured by whether to access the internet in this study. Secondly, the digital usage divide, also known as the second-level divide, pertains to variations in the way, extent, time, and skills of using digital technologies, 23 although they can all access digital technologies. In reference to previous literature, select the dimensions of usage time and content used to reflect the digital usage divide, 24 therefore, the frequency of digital use and whether to use internet healthcare of urban residents were selected to reflect the digital usage divide. Previous empirical studies have mostly focused on the first- or second-level divide.16–18
Thirdly, the digital outcome divide (the third-level divide) refers to the variations in the utilization of medical services or health outcomes among different groups due to the differences in the benefits obtained from the adoption and utilization of digital health. 18 These benefits can be classified into short-term and long-term gains. The short-term outcomes generated by internet healthcare might manifest as improved patient experience and satisfaction due to increased convenience. Among them, patient experience can be defined as both the experiences patients have during their care and the feedback on those experiences, 25 it can be used to explain changes in patient satisfaction with medical services 26 and can be measured through various items, such as waiting time, appointment time, medical level, etc. 25 While the long-term outcomes might include improvements in health outcomes (such as reducing mortality and increasing cure rates, etc.). 22 Due to the health outcome period of long-term performance indicators and the numerous influencing factors, digital health may only be a small part of them, and the impact path of health outcomes is currently difficult to verify. Thus, this study employs the short-term indicator of patient experience to measure the digital outcome divide.
The three-level digital divide framework 27 suggests that the second-level divide is influenced by the first-level divide and other contextual factors. For example, digital skills training is more impactful for computer owners, exacerbating the second-level divide. 28 The third-level divide arises from the first and second levels of digital divide and additional factors. For instance, students with poor computer skills tend to have lower e-learning outcomes. 29 It indicates that there is a cascading effect among the three-level digital divide. In the health context, interactions among the three levels likely exist, and the impact of the digital health divide will be transmitted along the digital chain, that is, there may be a cascading effect.
Based on the above, we propose a “Theoretical model of health digital divide among urban residents.” As shown in Figure 1, we aim to explore the following aspects: firstly, whether there are reciprocal influences among digital access divide, digital usage divide, and digital outcome divides, implying a cascade effect across these three levels of divide among urban residents. Secondly, we aim to assess the primary level of the health digital divide among urban residents. Finally, we investigate whether sociodemographic factors contribute to the emergence of the health digital divide in urban populations.

Theoretical model of the health digital divide among urban residents.
Methods
Data and sample
The Chinese Social Survey (CSS) (http://css.cssn.cn/css_sy/), initiated by the Institute of Sociology of the Chinese Academy of Social Sciences in 2005, is a biennial longitudinal survey covering 31 provinces in China. It employs a multi-stage stratified sampling method, with selected households receiving informed consent letters before household visits. Following participant consent, structured questionnaires are utilized for in-person family interviews, with a token of appreciation provided post-interview. To ensure high-quality survey data, CSS surveys maintain scientific rigor across multiple levels. The surveys utilize data from the 5th and 6th Population Censuses to establish sampling frames. Map address sampling is implemented at survey locations to capture a broader sample, particularly targeting the floating population. Rigorous investigator training is conducted, and a percentage of questionnaires are reviewed at various levels—survey site, provincial, and national—to guarantee questionnaire quality. Additionally, all questionnaires undergo double data entry. Its research findings can be inferred from the population of household residents aged 18–69 nationwide.
The data for this study came from the 2021 CSS, the survey includes information on individual and household demographics, household economic conditions, social participation, social security, etc., and a total of 10,136 questionnaires were collected. Considering this survey only asked urban residents about their use of internet healthcare, the inclusion criteria for this study were: (1) urban residents; (2) the survey subject is residing at their current address; (3) Chinese citizens aged 18–69; (4) voluntary participation in the study, informed consent form. Exclusion criteria: (1) questionnaires with incomplete information; (2) the same or regular questionnaires were checked. The final sample size included in the analysis was 3547.
Variable selection
Independent variables. The independent variables are demographic information of urban residents, including Age, Gender, Education, Work status, and Socioeconomic status. The measurement of socioeconomic status consists of three items with reverse values ranging from 1(Lower) to 5(Topper).
Dependent variables. The dependent variables mainly refer to the three-level digital health divide of urban residents, constructed based on the dimensions of the digital divide proposed by Cao et al. 24 The digital access divide refers to whether urban residents have digital access; the digital usage divide is measured by frequency of digital use and internet healthcare utilization of urban residents, with four items for frequency of digital use and reverse values ranging from 0(never) to 5(almost every day); the digital outcome divide refers to urban patient experience, 25 with four items and values ranging from 1(very serious) to 4(no such issue). The measurement of latent variables in the theoretical model, including socioeconomic status, frequency of digital use, and patient experience in urban areas, is shown in Table 1, and the specific values of other variables can be found in Table 2. Details of the questionnaire can be found in Appendix 1.
Instrument measurement.

Description of variables.

Statistical analysis
Descriptive statistical analysis was conducted using SPSS, with categorical variables presented as frequencies and percentages, and continuous variables presented as means and standard deviations. In structural equation modeling (SEM) analysis, Cronbach's Alpha was used to assess the reliability of the scale. The validity test includes three parts: convergent validity, discriminant validity, and structural validity. Among them, convergent validity is determined by average variance extracted (AVE) and composite reliability (CR), while discriminant validity is determined by the fact that the square root of AVE for each factor is greater than the maximum value of the correlation coefficient between that factor and other factors. Structural validity is tested by the model's fitness SEM was performed using AMOS 24.0 software to analyze the relationship between sociodemographic variables of urban residents and digital access, frequency of digital use, internet healthcare, and patient experience.
Results
Descriptive statistics and correlation analysis
As shown in Table 3, a total of 3547 urban samples were included in the analysis, the proportion of digital access among urban residents is 80.66%, and the average age of surveyed urban residents is 45.21 (SD 14.82). The distribution of male and female ratios is similar, with 61.97% of surveyed urban residents having a high school education or above. There are differences in age, gender, education, work status, and socio-economic status between the two groups of urban residents with and without digital access. Of 2861 urban residents with digital access, only 22.93% of them have used internet healthcare. There are differences in age, gender, education, and socio-economic status between the two groups of urban residents with digital access who have used internet healthcare and those who have not.
Statistical description of sociodemographic variables.

Note: The P-value is obtained through t-test.
Table 4 shows the correlation analysis between sociodemographic variables of urban residents. The correlation between age and education (r = −0.420) is greater than 0.3 but less than 0.5, indicating a low correlation between age and education. The correlation between other variables is less than 0.3, indicating a weak correlation between these variables and the absence of serious collinearity issues between independent variables.
The correlation between sociodemographic variables.

Note: **P < 0.01, *P < 0.05.
Measurement model analysis
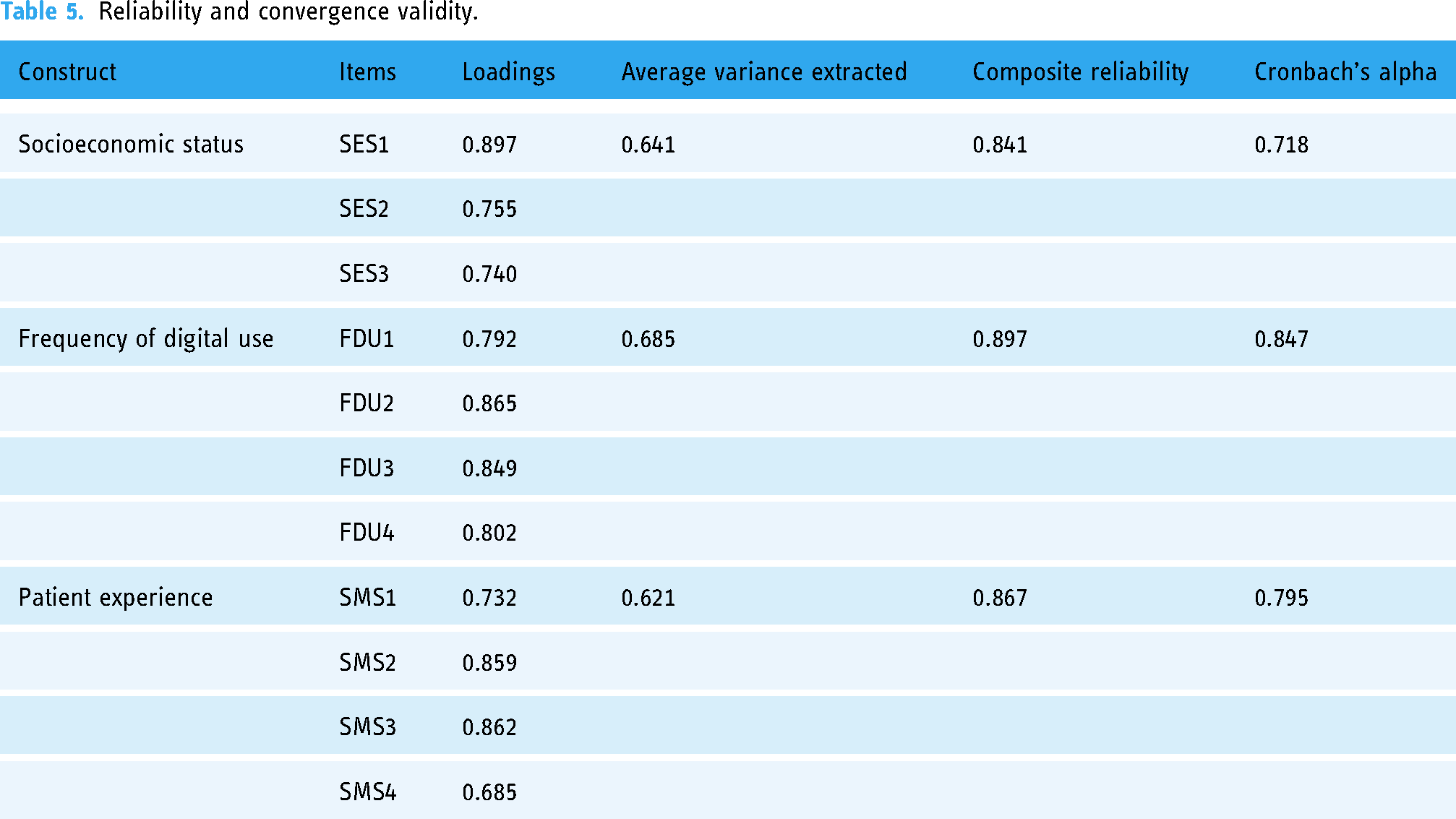
The measurement model mainly evaluated the reliability, convergent validity, and discriminant validity of the scales. Principal component analysis was applied to test the reliability and validity of each structure. The Kaiser-Meyer-Olkin (KMO) statistic was 0.743, and Bartlett's test of sphericity was statistically significant (χ250 = 13,526.13, P < 0.001), indicating that the data were suitable for factor analysis. Three factors were extracted, explaining 65.33% of the total variance. Then, the reliability and convergent validity of the structure were evaluated through Cronbach's Alpha, CR, and AVE. In Table 5, we can see that the Cronbach's Alpha values for each scale were greater than 0.7, indicating good reliability of the scales. At the same time, the AVE for each scale was greater than 0.5, and CR was greater than 0.7, indicating good convergent validity of the scales. In addition, as shown in Table 6, the square root of AVE for each scale was greater than its correlation coefficient with other scales, indicating good discriminant validity of the scales.
Reliability and convergence validity.
Discriminate validity.

Structural model analysis
The fit of the model was tested using the maximum likelihood method. As shown in Table 7, χ2/df was 2.895, the root mean square error of approximation (RMSEA) was 0.023, and the comparative fit index (CFI) was 0.993, all within an acceptable range. Other fit indices of the structural model also met the reference values, indicating an acceptable fit of the model.
Fit indices of the structural model.

Figure 2 shows the regression of all paths, with solid lines representing significant relationships and dashed lines representing non-significant relationships. The standardized and unstandardized β coefficients and detailed P values from sociodemographic variables to the three-level health digital divide of urban residents are shown in Table 8. Firstly, the digital access of urban residents has a significant positive impact on their frequency of digital use (β = 0.737, P < 0.001), which is followed by the frequency of digital use to promote the use of internet healthcare (β = 0.047, P < 0.05), which in turn is beneficial to improve their patient experience (β = 0.079, P < 0.001). It also reflects that the digital access divide of urban residents will promote the generation of a digital usage divide, which will eventually lead to the formation of a digital outcome divide among urban residents, suggesting that there is a cascading effect among the three-level divide of urban residents.

The impact of sociodemographic factors on third level divide among urban residents.
Path coefficient analysis of the health digital divide among urban residents.

Secondly, the influence of sociodemographic factors among urban residents reflects the main level of the health digital divide, with variables and coefficients related to digital access, frequency of internet use, and internet healthcare utilization being greater than patient experience. Therefore, our study indicates that the digital access divide and the digital usage divide of urban residents are the primary levels of the current state of the digital health divide.
Thirdly, age and education are closely related to both the digital access divide and the digital usage divide. Urban elderly are less likely to have digital access (β = −0.265, P < 0.001), use the internet less frequently (β = −0.204, P < 0.001), and low internet healthcare utilization (β = −0.160, P < 0.001). On the other hand, a higher educational level is associated with a greater likelihood of digital access (β = 0.288, P < 0.001), a higher frequency of digital use (β = 0.098, P < 0.001), and greater internet healthcare utilization (β = 0.118, P < 0.001). Furthermore, there are gender differences in digital access, frequency of internet use, internet healthcare utilization, and patient experience among urban residents. Urban females are more likely than urban males to engage with digital technologies. Additionally, urban individuals with higher socioeconomic status exhibit a higher frequency of digital use (β = 0.030, P < 0.01), greater internet healthcare utilization (β = 0.032, P < 0.05), and higher patient experience (β = 0.039, P < 0.05). There is a weak relationship between work status and frequency of internet use of urban residents (β = 0.030, P < 0.01).
Discussion and conclusions
This study constructed a three-level framework for the health digital divide among urban residents and systematically analyzed the cascading relationships from the digital access divide to the digital usage divide and then to the digital outcome divide using SEM. The study also assessed the potential flow of influences along these cascades, considering the impact of sociodemographic factors, and analyzed the main level of the health digital divide among urban residents. Among the participants, 80% of urban residents had digital access, but less than 20% of urban residents utilized internet healthcare. The following are the key findings of this study.
The study identified a series of potential cascading effects in the health digital divide of urban residents, where the effects propagate along the digital pathway, indicating a cascading progression in the health digital divide of urban residents. The disparities between urban residents in access or use of digital health technologies eventually manifest as a divide in healthcare utilization or health outcomes. This cascading effect may contribute to the perpetuation of the health digital divide and further exacerbate health inequalities among urban residents. 30 Similar to our study, research conducted by Wei et al. found that the first-level digital divide affects the second-level digital divide, which, in turn, influences the third-level digital divide, based on social cognitive theory and in the context of e-learning. 27
The potential influences of sociodemographic characteristics reflect the extent of the health digital divide among urban residents. 24 The number and size of variables related to the digital access and usage divide are greater than those related to digital outcome divide, indicating that the health digital divide among urban residents primarily manifests in the levels of access and usage. Firstly, this is because access to digital health technologies is a prerequisite for use and benefit. Although the internet penetration rate in China has been increasing in recent years, there are still differences in the demographic structure of urban internet users. 4 Secondly, sociodemographic factors may influence urban people's ability and opportunities to use digital health technologies, thereby creating digital usage divide among different urban residents. 24 Lastly, it may be because inequalities in access or usage among urban residents are easier to observe and measure, while the measurement of digital outcome divide varies depending on the research context. 31 In addition, the digital outcome divide may be a cumulative effect that takes longer to fully manifest. Consistent with previous research, the health digital divide exists in at least two dimensions: the digital access and usage divide.32,33
Among the sociodemographic variables examined in the survey, the age and education of urban residents emerged as stronger potential influencing factors. Both variables have direct and independent effects on the digital access and usage divide, but they do not have a direct impact on the digital outcome divide. Their effects occur in the early stages of the digital pathway. This is mainly because older residents may be associated with lower experience and ability to engage in digital technology, leading to greater barriers to digital technology access and usage. 34 Similarly, a lower educational level may result in insufficient digital skills and application capabilities, 35 limiting the ability of this population to utilize digital health services and contributing to the existence of the digital access and usage divide. These findings have been supported by other studies as well.35–37
Furthermore, the gender of urban residents has a certain influence on the digital access, usage, and outcome divide, with females showing higher levels of digital access, usage, and satisfaction with medical services compared to males. This goes against the findings of some existing research 38 and may be attributed to higher health concerns and service needs among females. Females often shoulder greater responsibilities for caregiving within households, 39 and digitalized healthcare services provide a convenient, efficient, and privacy-protected avenue that enhances their engagement in the realm of digital healthcare services and improves accessibility to healthcare services. The work status of urban residents is associated with the digital access and usage divide, primarily driven by the occupational needs of employees. Employees may require internet usage for information search and communication with clients and colleagues, thereby increasing their digital access and usage frequency. This finding is similar with the research by Cao et al., which found a correlation between employment status and digital technology use. 24 The socioeconomic statuses of urban residents also have a certain influence on the digital usage and outcome divide. On one hand, individuals with higher socioeconomic status tend to have higher digital health literacy, which promotes the use of digital health technologies. 40 On the other hand, individuals with higher socioeconomic status often have more opportunities to access health knowledge and information, making them more likely to encounter information related to digital health and healthcare services, 41 thus improving the patient experience.
Theoretical implications
This study has several theoretical implications. Firstly, by systematically constructing and analyzing the health digital divide among urban residents, this study confirms the existence of cascading effects between different levels, providing a foundation for a deeper understanding of the health digital divide among urban residents in the literature. Secondly, revealing the influence of urban sociodemographic factors on the cascades and the flow of influence along the digital pathway provides a more comprehensive understanding of the factors and pathways influencing the health digital divide among urban residents, thus providing theoretical support for bridging the health digital divide among urban residents. Lastly, by using large-scale national survey data (CSS2021), this study verifies that the digital access and usage divide is the main level of the health digital divide among urban residents, which can serve as a reference for future empirical research on these divides.
Practical implications
Based on the empirical findings, this study provides the following recommendations. Firstly, it is recognized that as the health digital divide among urban residents progresses, it may bring more profound social impacts and health inequalities to urban residents. To this end, it is necessary to clarify the development direction and goals of digital health, strengthen cooperation among multiple departments such as healthcare, medical insurance, and medicine, and improve the application level of digital health among urban residents. Secondly, more attention should be paid to the issue of digital access and usage divide. It is necessary to increase the government's financial investment in the popularization of digital technology, improve the digitalization level in the health field, and lay a good foundation for ensuring the accessibility and accessibility of digital health services. Thirdly, attention should be paid to specific urban social population groups: age and education have a significant impact on the acquisition and use of numbers. Therefore, for the urban elderly, a dedicated elderly area can be set up on the mobile end, and the user interface can be modified to adapt to aging, achieving accessibility for the elderly; Promoting digital health services centered around urban households and fully leverage the role of family and friends in improving the health of the urban elderly; Be able to use easy to understand language, visual aids such as hieroglyphs, to minimize text input and minimize technical barriers for low-educated urban residents.
Limitations
There are certain limitations to the current study. Firstly, it is a cross-sectional study, which may limit the establishment of causal relationships using SEM. Sociodemographic variables are long-term values and do not change significantly over time. However, the development of digital health is constantly evolving in our environment, so further research may yield different results. Secondly, this study analyzes the formation of the health digital divide among urban residents from the perspective of sociodemographic factors and suggests that future research should delve deeper into the fundamental reasons and mechanisms behind its formation. Thirdly, due to data limitations, the study focused only on the health digital divide among urban residents. It is recommended for future research to expand the scope and explore the mechanisms of the health digital divide more comprehensively.
Conclusions
This study confirms the existence of cascading effects in the health digital divide among urban residents, where the impacts of digital access and usage divide may further lead to the formation of digital outcome divide. Currently, the health digital divide among urban residents primarily manifests in the levels of digital access and usage. Therefore, to prevent the widening of the health digital divide among urban residents, it is important to improve digital access and usage among urban elderly, those with lower educational levels, and males. This study significantly enhances our theoretical understanding of the health digital divide among urban residents and can assist governments and relevant organizations in formulating policies to bridge the health digital divide among urban residents.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241271812 - Supplemental material for Sociodemographic factors and health digital divide among urban residents: Evidence from a population-based survey in China
Supplemental material, sj-docx-1-dhj-10.1177_20552076241271812 for Sociodemographic factors and health digital divide among urban residents: Evidence from a population-based survey in China by Yanbin Yang and Chengyu Ma in DIGITAL HEALTH
Footnotes
Acknowledgments
Some of the data used in this paper came from the major project of the Chinese Academy of Social Sciences, “2021 Comprehensive Survey of China's Social Situation.” The survey was conducted by the Institute of Sociology, Chinese Academy of Social Sciences, with project leaders Chen Guangjin and Li Wei. The author thanks the above-mentioned institutions and their personnel for providing data assistance. The content of this paper is the authors’ own responsibility.
Contributorship
All authors contributed to the study conception and design. YY: analyzed data, wrote and modify the manuscript. CM: designed the study, wrote and edited the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical review and approval were waived for this study, as the study used the open database of the Chinese Social Survey (CSS) and did not include experimentation that may bring possible risk of harm to participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been funded by the General Project of Ministry of Education Foundation on Humanities and Social Sciences, China (grant number: 22YJAZH082).
Guarantor
CM
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.