
Abstract
Objective
This mixed-methods investigation examined relationships between digital health literacy and self-efficacy among older adults, focusing on mediating pathways involving social support and life satisfaction and the moderating effect of health consciousness.
Methods
Quantitative data from 1016 community-dwelling older adults across six Chinese provinces were analyzed using structural equation modeling with bias-corrected bootstrapping procedures. A multi-stage probability sampling strategy ensured geographic and socioeconomic diversity. Complementary in-depth semi-structured interviews with 30 purposively selected participants were conducted to explore underlying mechanisms.
Results
Digital health literacy was significantly and directly associated with self-efficacy (β = 0.21, p < .05) and indirectly associated through social support (β = 0.10, 95% CI [0.06, 0.14]) and life satisfaction (β = 0.17, 95% CI [0.12, 0.22]). A sequential mediation pathway was identified whereby digital health literacy was related to social support, which in turn was associated with life satisfaction and subsequently with self-efficacy (β = 0.05, 95% CI [0.01, 0.09]). Health consciousness significantly moderated these relationships, with stronger associations among participants with high health consciousness (direct path: β = 0.32 vs. β = 0.09; sequential indirect path: β = 0.06 vs. β = 0.01). Integrated qualitative analysis revealed information-processing strategies, social validation processes, and goal-directed feedback loops that helped translate digital competencies into psychological resources.
Conclusion
Findings clarify mechanisms through which technological competencies relate to psychological resources in later life. Digital health interventions for older adults should therefore integrate social components, emphasize feedback systems that strengthen efficacy beliefs, and adapt content based on individual levels of health consciousness to optimize psychological benefits.
Keywords
Introduction
The rapid digitalization of healthcare systems has fundamentally transformed how individuals access, evaluate, and use health information, shifting part of the locus of control from clinical settings to patient self-management.1,2 For older adults, this transformation creates a “digital paradox”: digital technologies offer unprecedented opportunities for health promotion and social connection, yet they also impose cognitive and technical demands that can exacerbate exclusion. 3 Digital health literacy (DHL)—the ability to seek, find, understand, and appraise health information from electronic sources and apply this information to health decisions—has therefore emerged as a critical determinant of health equity in aging populations.4,5 Recent studies indicate that DHL is not merely a functional skill but a dynamic resource that shapes health behaviors, chronic disease management, and quality of life among older adults.6–8
In China, this digital transition is unfolding alongside rapid population aging. According to the 56th Statistical Report on China's Internet Development, as of June 2025, internet penetration among adults aged 60 years and above reached 52.0%, representing approximately 161 million older users. 9 However, access does not automatically translate into effective use. Older adults engage in diverse digital health activities, ranging from searching for health information and scheduling telemedicine appointments to monitoring vital signs via wearable devices. 10 Yet substantial disparities remain. While some older adults leverage these tools to enhance autonomy, others experience a “usage gap,” in which digital access does not lead to tangible psychological or health benefits. 11 Clarifying the mechanisms that bridge this gap is essential for designing effective interventions.
Despite growing recognition of the importance of DHL, the psychological mechanisms through which digital competencies translate into enduring personal resources such as self-efficacy remain insufficiently understood. Existing research has largely examined single pathways. For example, Newby et al. (2021) showed that digital health interventions can improve self-efficacy in a systematic review, but the internal processes underlying this relationship were not fully specified. 12 Similarly, Yuan et al. (2018) highlighted how digital engagement can facilitate social connectedness and co-production among older adults, yet it remains unclear how these social resources are converted into internal psychological capital. 13
To address these gaps and move beyond fragmented perspectives, the present study proposes an integrated model linking DHL to self-efficacy among older adults through both social and affective mechanisms. Drawing on social cognitive theory, broaden-and-build theory, and socioemotional selectivity theory, the model posits that DHL relates to self-efficacy directly and indirectly through perceived social support and life satisfaction, with health consciousness shaping the strength of these pathways.14–17 By combining quantitative structural equation modeling (SEM) with qualitative thematic analysis, the study seeks to identify not only statistical associations but also the lived processes through which digital competencies are embedded in daily health management. This approach aims to fill the theoretical gap left by single-focus studies that have emphasized either technological skills or social resources in isolation.
Within this framework, we further examine the boundary conditions of these relationships by positioning Health Consciousness as a critical moderator. We argue that health consciousness functions not merely as an individual trait, but as a cognitive filter that differentially activates these pathways. Individuals with higher health consciousness are hypothesized to possess more robust motivation to convert digital resources into psychological capital. 18 Consequently, this study aims to (1) empirically test the direct and sequential mediation pathways from DHL to self-efficacy involving social support and life satisfaction; and (2) investigate the moderating role of health consciousness in conditioning these mechanisms. By doing so, we answer the call for more nuanced investigations into how digital technologies interact with developmental and cognitive factors to shape psychological well-being in aging populations.
Literature review and theoretical development
DHL in later life
DHL extends beyond basic technical competence and encompasses functional, interactive, and critical skills for acquiring and applying health information from electronic sources.5,6 This multidimensional construct is particularly salient for older adults who must manage multiple chronic conditions and complex treatment regimens. 19 Empirical studies document substantial variability in DHL within older populations, with differences in literacy associated with variation in health behaviors, patterns of healthcare use, and psychological outcomes. 20
The developmental context of aging introduces specific considerations for DHL. Age-related changes in cognitive processing, accumulated technology experience, and evolving health information needs shape how older adults engage with digital health resources. 21 Some older adults face barriers related to limited prior exposure to digital technologies or age-related cognitive decline, 22 whereas others successfully use digital resources to support health management. 23 This heterogeneity underscores the need to examine how DHL is linked to psychological resources in later life rather than treating older adults as a homogeneous group.
Recent theoretical developments in models of technology adoption among older adults offer useful frameworks for understanding DHL in later life. The Senior Technology Acceptance Model, for instance, identifies factors that influence technology use in older populations, including perceived usefulness, ease of use, and facilitating conditions, while incorporating age-specific factors. 24 This model suggests that older adults’ adoption of digital health technologies is shaped not only by general perceptions of technology but also by gerontechnology self-efficacy, anxiety about technology use, and contextual supports. 25 These insights highlight DHL as a situated capability that depends on both individual and environmental conditions.
Self-efficacy through social cognitive mechanisms
Self-efficacy is a core psychological resource across the life course. 26 In later life, it plays a particularly important role in adaptation to age-related challenges, influencing health behaviors, emotional well-being, and functional independence. 27 According to social cognitive theory, self-efficacy beliefs develop through four main sources: mastery experiences, vicarious experiences, social persuasion, and interpretations of physiological states. 28
DHL may contribute to self-efficacy through each of these mechanisms. Successful navigation of digital health platforms provides mastery experiences that can strengthen efficacy beliefs. Exposure to health-related content featuring similar others managing chronic conditions offers vicarious experiences that inform perceived capability.12,28 Digital communication with healthcare providers and peers supplies social persuasion that reinforces confidence in managing health. 29 Finally, the use of health monitoring applications generates physiological feedback (e.g., blood pressure readings, step counts) that individuals interpret when forming judgments about their abilities.
These processes may operate in distinctive ways in later life. Older adults may benefit especially from mastery experiences that counter negative age stereotypes about technology use.
30
Vicarious experiences may be particularly influential when they feature age-similar models successfully coping with health challenges.
31
In addition, social persuasion may carry greater weight because socioemotional selectivity processes increase the importance of close social relationships in later life.
32
Taken together, these considerations suggest that older adults with higher DHL are more likely to develop stronger self-efficacy in managing health and daily life. Therefore:
Social support as intermediary mechanism
Social support is a key resource for older adults as they navigate age-related challenges, providing informational, instrumental, and emotional assistance. 29 DHL may be linked to social support through several mechanisms. Higher literacy can facilitate connection with geographically distant network members, enable participation in online health communities, and support maintenance of existing relationships through digital communication. 13
The association between social support and self-efficacy is well documented. Social networks provide informational support that enhances problem-solving, emotional support that buffers stress, and instrumental assistance that helps individuals achieve goals, all of which strengthen efficacy beliefs. 29 Social support also fosters social integration and belonging, which contribute to positive self-perceptions and confidence in managing everyday challenges. 33
For older adults, this relationship may be especially important in light of age-related changes in social networks and support needs. Although social networks tend to contract with age, older adults often maintain a smaller set of emotionally meaningful relationships that provide high-quality support.
32
Digital health engagement may complement this process by facilitating access to specialized support resources and by helping older adults maintain close relationships despite physical limitations or geographical distance.
13
These arguments suggest that social support mediates the relationship between older adults’ DHL and self-efficacy. Therefore:
Life satisfaction in sequential mediation
Life satisfaction—a cognitive evaluation of one's life as a whole—is a central indicator of subjective well-being and has particular relevance in later life. 34 Social support contributes to life satisfaction by providing emotional comfort, practical assistance, and a sense of belonging.29,33 DHL may indirectly influence life satisfaction by enabling older adults to seek support and maintain relationships through digital tools. 10 In turn, higher life satisfaction may be associated with greater willingness to engage with health-promoting behaviors and digital resources as individuals navigate age-related challenges.
Positioning life satisfaction as a mediator rather than an outcome warrants theoretical justification. Although reciprocal relationships between life satisfaction and self-efficacy have been documented, 35 the present study conceptualizes life satisfaction as preceding self-efficacy for three reasons. First, the broaden-and-build theory proposes that positive evaluative states create psychological conditions that facilitate the development of personal resources. 17 Second, empirical evidence indicates that positive affect and favorable life evaluations enhance cognitive flexibility and problem-solving confidence. 36 Third, socioemotional selectivity theory emphasizes the primacy of emotional well-being in later-life goal hierarchies, 32 suggesting that satisfaction experiences may shape subsequent efficacy beliefs. This perspective differs from models that treat efficacy as an antecedent of well-being and instead emphasizes how positive life evaluations create a context in which confidence can grow.
The relationship between life satisfaction and self-efficacy is likely dynamic. Higher life satisfaction may increase confidence in managing future challenges, while greater efficacy may further enhance life evaluations over time.35,36 In the present study, life satisfaction is modeled as a mediator to capture how affective evaluations channel the influence of DHL and social support into efficacy beliefs. Therefore:
The sequential pathway from DHL through social support and life satisfaction to self-efficacy is consistent with broaden-and-build theory.
17
Positive emotional experiences are assumed to broaden cognitive and behavioral repertoires while building enduring personal resources. Enhanced social support derived from digital engagement may improve life evaluations, which in turn foster broader perspectives and confidence in managing future challenges.
37
Considering these relational and affective processes jointly, DHL is expected to be linked to self-efficacy through a sequential pathway from social support to life satisfaction. Therefore:
Health consciousness as moderator
Health consciousness is an important individual-difference factor that may shape how older adults engage with digital health resources. 38 Individuals with higher health consciousness tend to show greater motivation to acquire health information, more systematic processing of health-related content, and stronger intentions to implement health-promoting behaviors.18,39
These characteristics are likely to influence how DHL relates to psychological resources. Older adults with higher health consciousness may derive greater benefit from digital health engagement because they search for information more strategically, process content more deeply, and are more motivated to apply what they learn. 39 They may also be more likely to recognize the value of digital health tools for managing health, thereby strengthening the association between DHL and self-efficacy. 18 Overall, these considerations suggest that health consciousness shapes the extent to which older adults translate DHL into a stronger sense of capability.
Taken together, these points lead to the following hypothesis:
The moderating role of health consciousness may also extend to indirect pathways involving social support and life satisfaction. Older adults with higher health consciousness may participate more actively in health-related social exchanges facilitated by digital platforms, thereby amplifying the social support benefits of DHL.
39
They may also derive greater satisfaction from successful health management supported by digital resources, potentially strengthening the pathway from DHL through life satisfaction to self-efficacy.
18
If health consciousness shapes whether and how older adults use DHL to build social ties and evaluate their lives positively, it should also influence the strength of the indirect pathway from DHL to self-efficacy. Therefore:
Current study
Guided primarily by social cognitive theory, the present study uses broaden-and-build theory and socioemotional selectivity theory in a targeted way to clarify how DHL may shape self-efficacy through social support, life satisfaction, and health-related motivation in later life. It responds to gaps in prior work in which DHL has mainly been linked to health behaviors or quality of life, often without treating self-efficacy as the central psychological outcome for older adults or simultaneously modeling socio-relational, affective, and motivational processes. Within this focused framework (Figure 1), the study examined whether DHL is positively associated with self-efficacy among older adults (H1), whether perceived social support mediates this association (H2), whether life satisfaction also mediates the association (H3), and whether DHL is related to self-efficacy through a sequential pathway from social support to life satisfaction (H4). In addition, health consciousness was conceptualized as a key motivational boundary condition and was expected to strengthen the direct association between DHL and self-efficacy (H5) as well as the sequential indirect pathway from DHL to self-efficacy via social support and life satisfaction (H6).

Research hypothesis model.
Methods
Research design and sampling procedure
This investigation used a sequential explanatory mixed-methods design conducted in community settings across six provinces in China between March 2024 and November 2024. The quantitative phase (March–August 2024) consisted of a cross-sectional survey of 1016 community-dwelling older adults, followed by a qualitative phase (September–November 2024) in which 30 participants completed in-depth interviews. All data were collected in community meeting rooms within residential neighborhoods to provide familiar and accessible environments for older adults. Study sites were located in eastern coastal provinces (Guangdong, Zhejiang), central provinces (Hubei, Anhui), and western provinces (Sichuan, Guangxi), which were purposively selected to capture variation in economic development, healthcare infrastructure, and digital technology penetration. This design allowed robust hypothesis testing while also generating deeper insight into the processes linking DHL with psychological outcomes in later life. 40
The sampling procedure employed multi-stage probability techniques to enhance the representativeness of the target population. The first stage involved purposive selection of six provinces representing eastern (Guangdong, Zhejiang), central (Hubei, Anhui), and western (Sichuan, Guangxi) regions of China to capture geographic and socioeconomic diversity. Within each province, three communities were randomly selected from stratified lists organized by socioeconomic indicators (high, medium, low) based on official census data. From community registries, households with older adults were selected using systematic random sampling, and one eligible participant per household was randomly selected using the Kish grid method.
Inclusion criteria were (1) age ≥60 years; (2) no severe cognitive impairment (Mini-Mental State Examination score ≥24); (3) no terminal illness; and (4) voluntary informed consent. Exclusion criteria included (1) communication barriers or inability to complete questionnaires independently; and (2) psychiatric treatment within the past six months. Community committees assisted with participant recruitment, and data collection occurred in community meeting rooms.
The final quantitative sample (N = 1016, 92.36% response rate) demographically paralleled the older adult population in the selected regions, with no significant differences in age distribution (M = 67.11, SD = 5.92), gender ratio (50.39% male), or educational attainment when compared to census data (χ2(3) = 4.28, p = .23). Table 1 presents the geographic distribution of the final sample across provinces, demonstrating proportional representation with no significant regional differences in demographic characteristics (χ2(10) = 14.23, p = .16).
Geographic distribution of final quantitative sample after data screening.

Note. Response rates calculated as (final sample/initial contacted) × 100. Non-response primarily due to incomplete questionnaires (n = 58) or withdrawal during data collection (n = 26). Regional distribution maintained proportional representation.
A priori power analysis using G*Power 3.1 indicated that a minimum sample of 395 participants would provide 95% power to detect small-to-medium effects (f2 = 0.08) in the complex structural equation model with 22 observed variables at α = 0.05; thus, our sample substantially exceeded requirements, ensuring adequate statistical power for subgroup analyses.
For the qualitative phase, a theoretically driven purposive sampling strategy was used to select 30 interview participants stratified by health consciousness (15 high, 15 moderate, based on quantitative scores). 41 Sampling was further balanced by gender (male = 14, female = 16), age (60–70 years = 18, >70 years = 12), and educational background (lower = 17, higher = 13) to maximize variation in perspectives while maintaining the theoretical focus. The target sample size was informed by the concept of information power, 42 which proposes that smaller samples are adequate when study aims are specific, the theoretical framework is strong, interview dialogue is rich, and cross-case analysis is employed—all of which applied to the present study.
Data saturation was systematically monitored throughout the qualitative data collection process using established criteria. 43 Saturation assessment involved (1) ongoing analysis of transcripts by two independent coders after every five interviews; (2) documentation of new themes emerging from each subsequent interview; (3) determination that theoretical saturation was achieved when three consecutive interviews (interviews 28–30) yielded no new substantive themes or conceptual insights beyond those identified in earlier interviews. The saturation determination was confirmed through team consensus meetings where all qualitative researchers reviewed coded transcripts and thematic maps. This systematic approach to saturation assessment enhanced confidence that the sample size was sufficient to capture the range of experiences and perspectives relevant to the research questions.
Ethical considerations and informed consent procedures
This study received ethical approval from the Institutional Review Board (Approval No. 20231126; date of approval: February 1, 2024). All procedures involving human participants were conducted in accordance with the Declaration of Helsinki and relevant institutional guidelines and regulations. Participation in both the survey and the qualitative interviews was entirely voluntary, and written informed consent was obtained from all participants before data collection.
The consent process involved (1) providing written information sheets describing study objectives, procedures, potential risks and benefits, data confidentiality, and withdrawal rights; (2) offering opportunities for questions and clarification; (3) obtaining signatures from participants or their legally authorized representatives; and (4) giving participants copies of the signed consent form for their records. For participants with visual impairments, consent forms were read aloud by trained research assistants, and verbal consent was audio-recorded and subsequently transcribed. All consent materials and procedures were reviewed and approved by the ethics committee prior to data collection.
Measures and cultural adaptation
All instruments underwent rigorous cross-cultural adaptation following Beaton's six-stage process 44 : (1) forward translation by two independent bilingual experts; (2) synthesis of translations; (3) back-translation by two different translators; (4) expert committee review for semantic, idiomatic, experiential, and conceptual equivalence; (5) cognitive interviewing with 12 older adults; and (6) psychometric evaluation in a pilot sample (n = 50). This systematic process supported the cultural appropriateness and measurement equivalence of all instruments.
Digital Health Literacy
DHL was assessed with the culturally adapted eHealth Literacy Scale (eHEALS), 5 an eight-item measure of perceived ability to find, evaluate, and apply electronic health information. Sample items include “I know how to find helpful health resources on the Internet” and “I can tell high-quality from low-quality health resources on the Internet.” Items were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). In this sample, the scale showed excellent internal consistency (α = 0.91) and good construct validity (χ2/df = 2.66, CFI = 0.95, RMSEA = 0.06), with measurement invariance established across age and education subgroups.
Consistent with prior work, 5 it should be noted that eHEALS assesses perceived rather than objective DHL skills. While self-report measures allow efficient assessment in large samples, they may not fully capture performance-based competencies.
Self-efficacy
Self-efficacy was measured using the 10-item General Self-Efficacy Scale, 45 which assesses beliefs about one's ability to cope with challenging situations. Example items are “I can always manage to solve difficult problems if I try hard enough” and “I am confident that I could deal efficiently with unexpected events.” Items were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The scale demonstrated strong internal consistency (α = 0.84) and satisfactory factorial validity (χ2/df = 3.78, CFI = 0.93, RMSEA = 0.04).
Social support
Social support was assessed using an adapted version of the Medical Outcomes Study Social Support Survey, 46 supplemented with two items capturing offline social resources particularly relevant to older adults (“community-based support networks” and “intergenerational relationships”). The resulting five-item scale assessed both online and offline social resources. Example items include “I can get support from others when needed through online or offline social interactions” and “My social connections provide me with valuable resources for managing health issues.” Responses were recorded on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The expanded scale showed excellent reliability (α = 0.91) and good factorial validity (χ2/df = 2.11, CFI = 0.91, RMSEA = 0.03).
Life satisfaction
Life satisfaction was measured using the five-item Satisfaction with Life Scale, 47 which assesses global cognitive evaluations of one's life. Sample items include “In most ways my life is close to my ideal” and “I am satisfied with my life.” Items were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The scale demonstrated good reliability (α = 0.78) and acceptable structural validity (χ2/df = 5.12, CFI = 0.96, RMSEA = 0.07).
Health consciousness
Health consciousness was assessed using an adapted version of Gould's Health Consciousness Scale. 38 Two culturally inappropriate items were removed based on confirmatory factor analysis in the pilot sample, resulting in a seven-item scale assessing awareness of and attention to health issues. Example items include “I am very self-conscious about my health” and “I am generally attentive to my inner feelings about my health.” Items were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). The revised scale showed good reliability (α = 0.88) and good model fit (χ2/df = 3.81, CFI = 0.94, RMSEA = 0.07).
Demographic variables
Participants reported age, gender, education level, marital status, living arrangement, and self-rated health status. These variables were included as covariates in the structural models to control for potential confounding effects on the relationships of interest.
Permissions for questionnaires
All constructs were assessed with established questionnaires whose full item content and response formats have been reported in previous publications. According to information provided in the original articles and on the publishers’ or developers’ websites, these instruments may be used for non-commercial academic research without additional written permission. In the present study, all questionnaires were reproduced and administered solely for non-commercial academic purposes in line with these conditions.
Qualitative data collection procedures
Semi-structured interviews averaging 52 min (range = 41–68) were conducted by trained interviewers using a theoretically grounded interview guide with open-ended questions exploring each pathway in the hypothesized model, followed by systematic probes for clarification and elaboration. The interview protocol (available upon request) focused on three primary domains: (1) digital health information seeking and application strategies, (2) social interactions facilitated by digital health engagement, and (3) perceived impacts on life satisfaction and self-confidence.
Sample questions included: “How do you typically search for and evaluate health information using digital devices?”, “In what ways has your use of digital health resources affected your social connections?”, and “How has your ability to use digital health resources influenced your confidence in managing health challenges?” Interviews were conducted in private rooms at community centers, audio-recorded with permission, and transcribed verbatim. Transcripts were verified for accuracy by comparing audio recordings with transcribed text and reviewed by participants to ensure interpretive validity.
Analytical strategy
Our analytical strategy combined SEM for hypothesis testing with thematic analysis of interview data, using methodological triangulation to enhance the validity of findings. 40 This approach enabled examination of the hypothesized relationships and, simultaneously, exploration of the mechanisms through which DHL relates to psychological outcomes in later life. Given the cross-sectional design, all reported associations are interpreted as non-causal. Although the theoretical model specifies directional relationships based on social cognitive theory, socioemotional selectivity theory, and broaden-and-build theory, the present data cannot establish temporal precedence or rule out alternative causal orderings.
Preliminary analyses
Preliminary analyses examined missing data patterns, multivariate normality, common method variance, and multicollinearity. Missing data were minimal (0.8%) and were consistent with a missing-completely-at-random pattern. Multivariate normality was acceptable (Mardia's coefficient = 3.74). Harman's single-factor test indicated that a single factor accounted for 29.62% of the variance, suggesting that common method variance was unlikely to be a major concern. All variance inflation factor values were below 3.0, indicating no multicollinearity problems. To further reduce common method bias, we implemented procedural remedies during data collection, including counterbalancing question order, assuring anonymity, and using different response formats where feasible. 48 These checks supported the suitability of the data for SEM using maximum likelihood estimation with robust standard errors.
Composite score construction and handling
All multi-item scales were modeled as latent variables in the SEM analyses rather than as summed or averaged composite scores. This approach offers several advantages: (1) it accounts for measurement error in observed indicators; (2) it permits explicit assessment of construct validity via confirmatory factor analysis; (3) it enables tests of measurement invariance across groups; and (4) it yields more accurate estimates of structural relationships. 49 Each latent construct (DHL, self-efficacy, social support, life satisfaction, health consciousness) was specified with its respective items as indicators, with factor loadings estimated from the data. For descriptive statistics and correlations in Table 2, scale scores were computed as arithmetic means of item responses to aid interpretability. Missing item responses (<0.8% across all items) were handled using an expectation-maximization algorithm before averaging. All hypothesis tests, however, were conducted using latent variable models rather than composite scores, thereby maximizing psychometric rigor and statistical power.
Descriptive statistics and correlations among study variables.
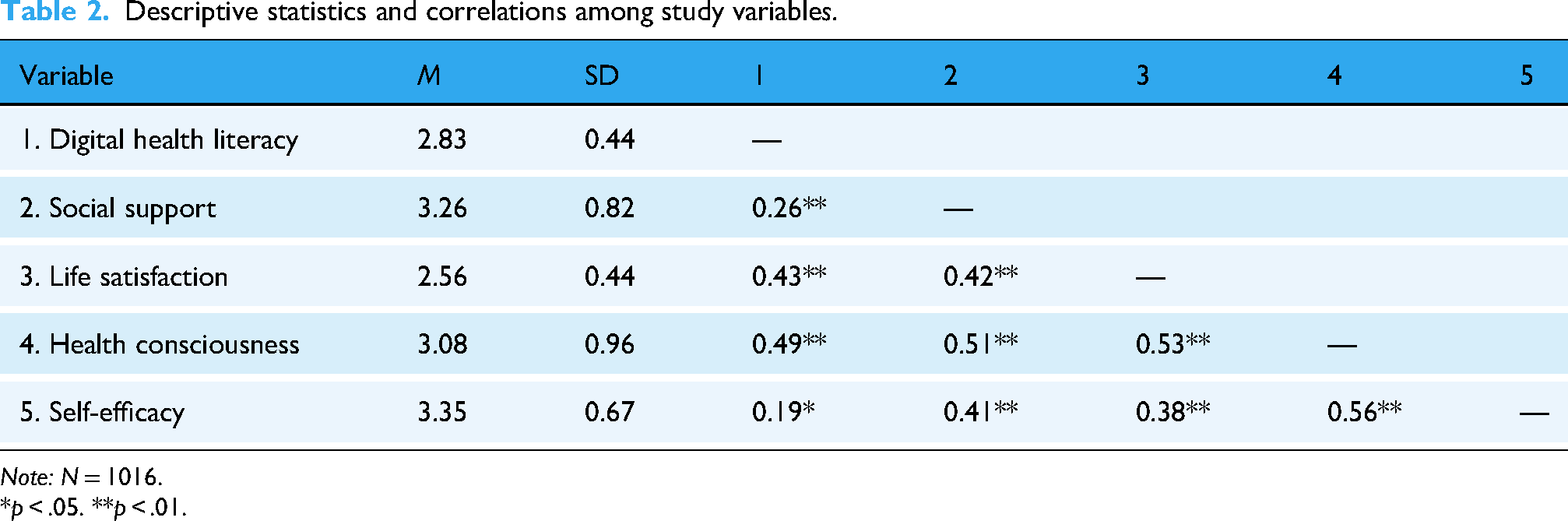
Note: N = 1016.
*p < .05. **p < .01.
Structural Equation Modeling
SEM models were estimated using maximum likelihood with robust standard errors to account for minor deviations from normality. Model fit was evaluated using multiple indices: comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Acceptable fit was defined as CFI and TLI ≥0.90 and RMSEA and SRMR ≤0.08, and good fit as CFI and TLI ≥0.95 and RMSEA and SRMR ≤0.06. 50 Competing models were compared using χ2 difference tests and changes in fit indices to evaluate alternative theoretical specifications of the relationships among variables.
Mediation analysis
Mediation hypotheses were tested using bias-corrected bootstrapping with 5000 resamples to generate 95% confidence intervals for indirect effects. We also decomposed specific indirect effects following the recommendations of Preacher and Hayes. 51 This approach provides a robust assessment of mediation without relying on normality assumptions for the sampling distribution of indirect effects.
Moderation analysis
Moderation hypotheses were examined using multi-group SEM by health consciousness level. We first tested measurement invariance across high versus moderate health consciousness groups (configural, metric, and scalar levels), using χ2 difference tests and changes in fit indices to evaluate equivalence. After at least partial scalar invariance was established, structural paths were constrained to be equal across groups. Significant deterioration in model fit was interpreted as evidence of moderation.
Qualitative analysis
Interview transcripts were analyzed thematically in NVivo 12 using Braun and Clarke's six-step approach. 52 Two independent coders achieved substantial inter-coder reliability (Cohen's κ = 0.87), and member checking with five participants further enhanced interpretive validity. The analysis involved (1) familiarization with the data through repeated reading; (2) generating initial codes; (3) searching for candidate themes; (4) reviewing themes; (5) defining and naming themes; and (6) producing the final analysis. Initial coding was informed by the theoretical framework but remained open to emergent themes. A codebook was developed iteratively, with regular team discussions to refine codes and themes and to strengthen analytic rigor. The study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 53
Mixed-methods integration
Following Fetters et al.'s integration framework, 54 we used connecting, building, and merging strategies to systematically integrate quantitative and qualitative data. Connecting occurred when interview participants were selected based on quantitative results; building occurred when preliminary quantitative findings informed the development of interview questions; and merging occurred through joint displays and narrative integration of statistical results with qualitative themes. This integration enabled a more comprehensive understanding of how DHL relates to psychological outcomes in later life.
Results
Measurement model evaluation
Confirmatory factor analysis supported a five-factor measurement model with excellent fit (χ2(220) = 497.06, p < .001, χ2/df = 2.26, CFI = 0.94, TLI = 0.93, RMSEA = 0.035, 90% CI [0.031, 0.039]). All standardized factor loadings were statistically significant (range = 0.62–0.89, p < .001), and inter-factor correlations were below 0.60, indicating adequate discriminant validity. Alternative models, including a four-factor model combining social support and life satisfaction (χ2(224) = 789.34, p < .001, χ2/df = 3.52, CFI = 0.83, TLI = 0.81, RMSEA = 0.063) and a single-factor model (χ2(230) = 1457.21, p < .001, χ2/df = 6.33, CFI = 0.57, TLI = 0.53, RMSEA = 0.112), showed substantially poorer fit, further supporting the discriminant validity of the constructs.
Measurement invariance tests across health-consciousness groups (high vs. moderate, based on a median split) supported configural invariance (χ2(440) = 753.89, p < .001, CFI = 0.93, RMSEA = 0.038), metric invariance (Δχ2(18) = 24.31, p = .15, ΔCFI = 0.004), and scalar invariance (Δχ2(18) = 29.27, p = .09, ΔCFI = 0.007, ΔRMSEA = 0.005). These findings indicate that the measurement structure was equivalent across groups, allowing meaningful comparison of structural parameters.
Descriptive statistics and correlations
Descriptive statistics indicated moderate levels of DHL (M = 2.83, SD = 0.44) and generally favorable psychological profiles (Table 2). DHL was positively correlated with social support (r = .26, p < .01), life satisfaction (r = .43, p < .01), health consciousness (r = .49, p < .01), and self-efficacy (r = .19, p < .05). Social support correlated positively with life satisfaction (r = .42, p < .01), health consciousness (r = .51, p < .01), and self-efficacy (r = .41, p < .01). Life satisfaction was positively associated with health consciousness (r = .53, p < .01) and self-efficacy (r = .38, p < .01). Health consciousness also correlated positively with self-efficacy (r = .56, p < .01).
To examine potential demographic correlates, we conducted additional analyses of differences in key variables by education level, gender, and urban versus rural residence. Education was significantly associated with DHL (F(3, 1012) = 18.42, p < .001), with higher education corresponding to higher DHL scores. Urban–rural differences were observed for DHL (t(1014) = 4.26, p < .001) and social support (t(1014) = 2.85, p < .01), with urban residents reporting higher levels of both. These patterns underscore the importance of considering demographic factors when interpreting the associations between DHL and psychological outcomes.
Structural model and mediation analysis
The hypothesized structural model demonstrated excellent fit (χ2/df = 2.27, CFI = 0.93, TLI = 0.92, RMSEA = 0.03). To evaluate explanatory power, we examined the squared multiple correlations (R2) for the endogenous constructs. The model accounted for 16% of the variance in social support (R2 = .16), 31% in life satisfaction (R2 = .31), and 48% in self-efficacy (R2 = .48). These effect sizes indicate that the integrated digital health model had substantial predictive utility for psychological outcomes in older adults.
With respect to specific pathways, DHL was directly associated with self-efficacy (β = 0.21, p < .05), supporting H1. To evaluate alternative theoretical specifications, we estimated competing models, including a model with only direct effects (χ2/df = 3.45, CFI = 0.85, TLI = 0.83, RMSEA = 0.059) and a model with reversed directionality in which self-efficacy predicted DHL (χ2/df = 3.62, CFI = 0.84, TLI = 0.82, RMSEA = 0.061). Both alternatives showed substantially poorer fit, lending support to the hypothesized model.
Bootstrap analyses revealed significant indirect effects of DHL on self-efficacy through social support (β = 0.10, 95% CI [0.06, 0.14]) and life satisfaction (β = 0.17, 95% CI [0.12, 0.22]), supporting H2 and H3. Decomposition of the total effect (β = 0.53) indicated that the direct effect accounted for 39.62% of the total effect, while the indirect effect through social support accounted for 18.87% and the indirect effect through life satisfaction accounted for 32.08%.
Sequential mediation analysis
Bootstrap analysis further supported the sequential mediation pathway from DHL to self-efficacy through social support and life satisfaction (β = 0.05, 95% CI [0.01, 0.09]), which accounted for 9.43% of the total effect and supported H4. The full model, including all direct and indirect paths, showed a better fit than simpler mediation models, with specific path coefficients displayed in Figure 2.

Structural equation model showing direct and indirect pathways from digital health literacy to self-efficacy. Note: Standardized coefficients are presented.
The sequential pathway operated as follows. DHL was positively associated with social support (β = 0.25, p < .05). Social support was positively associated with life satisfaction (β = 0.38, p < .01) while controlling for the direct association between DHL and life satisfaction (β = 0.32, p < .01). Life satisfaction was positively associated with self-efficacy (β = 0.55, p < .01) while controlling for the direct paths from DHL (β = 0.21, p < .05) and social support (β = 0.41, p < .01) to self-efficacy. Together, these results support the hypothesized sequential mediation process whereby DHL relates to social support, which in turn relates to life satisfaction and ultimately to self-efficacy.
Moderation analysis
Multi-group SEM, conducted after confirming scalar measurement invariance (ΔCFI = 0.007, ΔRMSEA = 0.005), showed that health consciousness moderated the direct association between DHL and self-efficacy (Δχ2(1) = 7.42, p < .01). The association was stronger in the high health consciousness group (β = 0.32, p < .01) than in the moderate group (β = 0.09, p < .05), supporting H5. Examination of specific paths in the moderation model (Table 3) also revealed significant group differences in the paths from DHL to self-efficacy, DHL to social support, social support to life satisfaction, life satisfaction to self-efficacy, and the sequential indirect pathway from DHL to self-efficacy through social support and life satisfaction.
Path coefficients by health consciousness level.
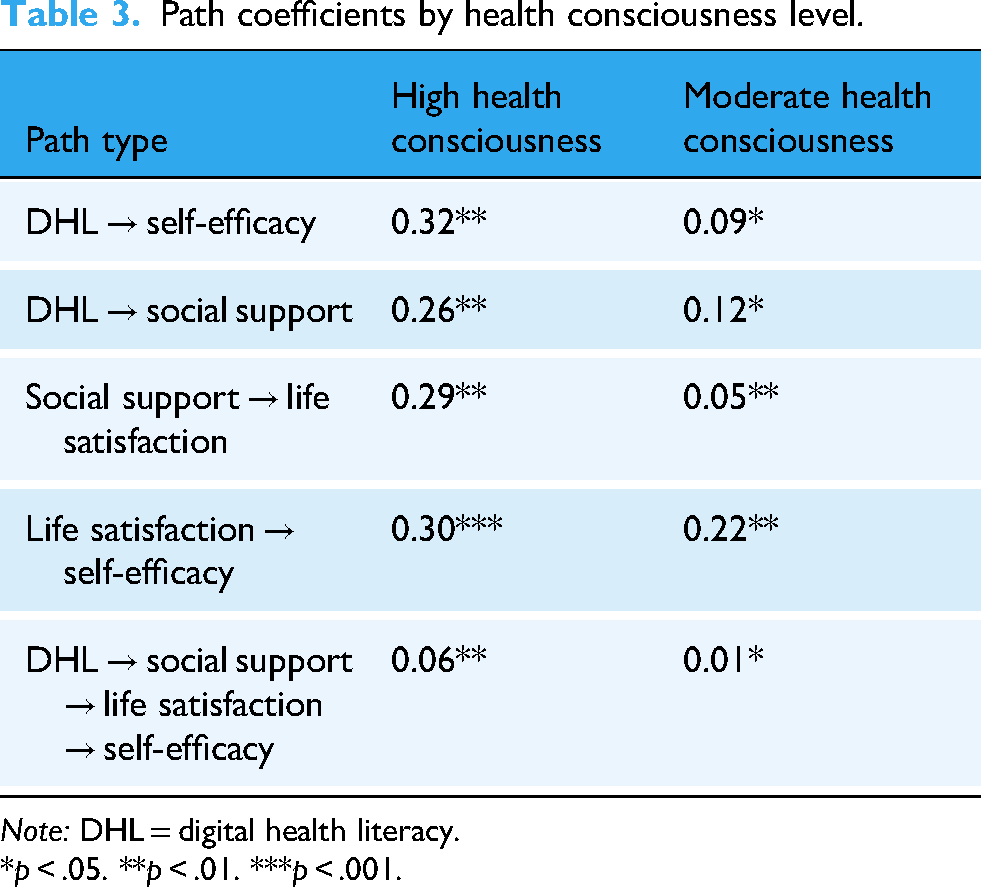
Note: DHL = digital health literacy.
*p < .05. **p < .01. ***p < .001.
Moderated mediation analysis
The sequential indirect effect of DHL on self-efficacy through social support and life satisfaction was significantly stronger at high levels of health consciousness (β = 0.06, 95% CI [0.02, 0.09]) than at moderate levels (β = 0.01, 95% CI [0.001, 0.03]). The index of moderated mediation was significant (Index = 0.05, 95% CI [0.01, 0.08]), supporting H6. These results suggest that health consciousness not only moderates the direct association between DHL and self-efficacy but also conditions the strength of the sequential mediation pathway through social support and life satisfaction.
Qualitative findings
Thematic analysis yielded three overarching themes that elaborated on the quantitative findings: (1) behavioral transformation pathways linking digital literacy to efficacy beliefs, (2) socio-emotional support mechanisms facilitating resource accumulation, and (3) cognitive-motivational processes underlying the moderating role of health consciousness.
Behavioral transformation pathways
Participants described how DHL related to self-efficacy through concrete behavioral mechanisms, with notable differences in information filtering strategies between high and moderate health consciousness groups. Those with high health consciousness (e.g., Participant 12, female, 68 years, college education) reported active information evaluation: “I compare recommendations from different apps like ‘DingXiang Doctor’ and ‘PingAnHao Doctor’ (Note: These are the names of 2 internet medical consulting apps.), checking which aligns with scientific evidence.” This strategic approach is related to perceived control over health management, potentially contributing to stronger efficacy beliefs.
In contrast, participants with moderate health consciousness (e.g., Participant 23, male, 71 years, primary education) described more passive information reception: “My daughter downloaded the app for me. I use whatever she recommends.” This reliance on others potentially limited the efficacy-enhancing benefits of DHL.
Quantified health monitoring emerged as a powerful mechanism linking DHL to enhanced efficacy beliefs. Participant 7 (female, 65 years, high school education) explained: “Checking my blood pressure daily with the app and seeing normal readings makes me feel I can manage my health effectively.” This immediate feedback loop is related to confidence in health management abilities, particularly among those with higher health consciousness who engaged more systematically with monitoring features.
Socio-emotional support mechanisms
Participants illuminated how DHL facilitated access to social support through both online and offline channels, with emotional support and vicarious learning emerging as key mechanisms linking social resources to enhanced efficacy beliefs. Participant 9 (male, 69 years, middle school education) described how online health communities provided vicarious experiences that strengthened efficacy beliefs: “In the diabetes forum, seeing others successfully control their blood sugar makes me believe I can do it too.” This observational learning process aligned with social cognitive theory's emphasis on vicarious experiences as sources of efficacy beliefs.
For participants with limited digital skills, community-based digital health activities served as bridges to social support. Participant 18 (female, 73 years, primary education) explained: “The ‘smartphone health class’ at our community center taught us to use health apps, and afterward, we discuss what we learned with neighbors. It makes me feel more secure.” These hybrid online-offline interactions enhanced social connectedness while facilitating digital health engagement, particularly benefiting those with lower initial DHL.
Social validation emerged as a mechanism linking social support to life satisfaction and subsequently to self-efficacy. Participant 5 (male, 68 years, high school education) noted: “When I share my walking achievements in our WeChat group and receive encouragement, I feel more satisfied with my daily routine and more confident about staying healthy.” This social reinforcement strengthened the connection between digital health engagement, life satisfaction, and efficacy beliefs.
Cognitive-motivational processes
Qualitative findings illuminated cognitive-motivational processes underlying the moderating role of health consciousness. Participants with high health consciousness demonstrated goal-directed approaches to digital health engagement that enhanced self-regulatory capacities. Participant 3 (female, 66 years, college education) explained: “I set an 8000-step daily goal on my phone. Achieving it gives me a sense of accomplishment that carries over to other health behaviors.” This goal orientation strengthened the connection between DHL and self-efficacy by facilitating successful experiences that enhanced confidence.
Information complexity management differed markedly between high and moderate health consciousness groups. Participants with high health consciousness described systematic approaches to managing contradictory health information, while those with moderate health consciousness reported confusion and anxiety when confronted with inconsistent advice. Participant 27 (male, 70 years, middle school education) expressed frustration: “There's too much information online—some say oatmeal is good, others say it's not. I don't know what to believe.” This cognitive overload potentially diminished the efficacy-enhancing benefits of DHL for those with moderate health consciousness.
The value orientation toward health emerged as a cognitive framework that influenced how digital health experiences related to efficacy beliefs. Participants with high health consciousness interpreted digital health engagement as an expression of personal health values, enhancing the psychological significance of these activities. Participant 15 (female, 64 years, college education) reflected: “Using health apps aligns with my belief that prevention is better than cure. Each time I log my activities, I'm affirming my commitment to staying healthy.” This value integration strengthened the connection between DHL and psychological outcomes.
Integrated mixed-methods findings
Joint display analysis revealed strong convergence between quantitative and qualitative findings, with participant narratives providing experiential context for statistical relationships (Table 4). The integrated analysis revealed that while quantitative findings established the presence and magnitude of relationships between DHL, mediating factors, and self-efficacy, qualitative findings illuminated the experiential mechanisms through which these relationships operate in daily life.
Integration of quantitative and qualitative findings.

Convergence and complementarity in mixed-methods integration
The systematic integration of quantitative and qualitative findings through connecting, building, and merging strategies yielded insights unattainable through either method alone 54 :
Quantitative-Qualitative Convergence: Statistical associations between constructs (e.g., DHL-social support correlation r = .26, p < .01) found direct experiential confirmation in participant narratives describing how digital health knowledge facilitated valued social exchanges. This convergence across methods strengthens confidence in the validity of findings (methodological triangulation).
Qualitative Elaboration of Quantitative Patterns: While SEM analyses established the statistical significance of mediation pathways, qualitative data revealed the experiential mechanisms underlying these pathways. For instance, the sequential mediation through social support and life satisfaction (β = 0.05, 95% CI [0.01, 0.09]) might appear modest in magnitude, but qualitative insights revealed this reflects a meaningful multi-step process: digital literacy → social connection → reduced loneliness → positive life evaluation → enhanced confidence. The modest coefficient reflects the cumulative attenuation across multiple steps, each representing psychologically meaningful transitions described by participants.
Direct Pathway (DHL → Self-Efficacy, β = 0.21, p < .05): Qualitative findings illuminated that this direct association operates through mastery experiences. Participant 11 explicitly described the psychological process: “Each time I successfully find health information online, I feel more capable of managing my health problems"—illustrating how successful digital navigation provides performance accomplishments that directly strengthen efficacy beliefs, consistent with social cognitive theory's primary efficacy source. 28
Social Support Mediation (Indirect effect β = 0.10, 95% CI [0.06, 0.14]): The quantitative mediation effect gains explanatory depth through qualitative insights revealing two specific mechanisms. First, Participant 8's narrative illustrated informational support: “The health knowledge I gain online gives me something valuable to share with friends, which strengthens our connections"—showing how Digital Health Literacy facilitates social resource accumulation. Second, Participant 9 described vicarious learning: “In the diabetes forum, seeing others successfully control their blood sugar makes me believe I can do it too"—demonstrating how digitally accessed social support provides observational experiences that enhance efficacy beliefs. This dual mechanism (resource accumulation + vicarious learning) explains the statistically significant mediation pathway.
Life Satisfaction Mediation (Indirect effect β = 0.17, 95% CI [0.12, 0.22]): The substantial mediation through life satisfaction—accounting for 32.08% of total effect—receives mechanistic clarification through qualitative data. Participant 14 described the affective pathway: “Having friends to discuss health information with makes me feel less alone in managing health issues, which makes life more satisfying.” Subsequently, Participant 20 articulated the satisfaction-to-efficacy link: “When I'm satisfied with life, I approach new health challenges with more confidence.” This sequential process aligns with the broaden-and-build theory, with qualitative evidence supporting the proposed mechanism whereby positive evaluative states expand cognitive resources underlying confidence.
Unexpected Qualitative Insights: The qualitative analysis revealed mechanisms not explicitly hypothesized in the quantitative model, including (1) goal-directed feedback loops whereby achievement notifications from health apps provided efficacy-enhancing reinforcement; (2) cognitive overload experiences among moderate health consciousness participants that limited DHL benefits; (3) value-congruence processes strengthening identity integration of digital health competencies. These emergent themes suggest refinements for future theoretical models and measurement approaches.
Explanation of Moderation Magnitude: The stronger path coefficients in the high health consciousness group (DHL → Self-Efficacy: β = 0.32 vs. β = 0.09) gain substantive interpretation through qualitative comparisons revealing fundamentally different information processing strategies, attribution patterns, and emotional engagement between groups—demonstrating that the statistical moderation reflects meaningful psychological differences rather than mere statistical artifact.
This integrated interpretation demonstrates how quantitative pathways identified through SEM correspond to lived experiences described by participants, with qualitative data revealing the cognitive, emotional, and social processes through which statistical relationships manifest in daily life. Particularly valuable was the qualitative insight into how information processing strategies, social validation experiences, and goal-directed feedback loops facilitate the translation of digital competencies into psychological resources in the developmental context of later life.
Discussion
The rapid digitalization of healthcare systems creates a complex landscape for aging populations, offering new opportunities for autonomy while also introducing barriers to inclusion. Although digital engagement is increasingly recognized as a determinant of health equity, the psychological mechanisms through which digital competencies relate to adaptive outcomes in later life remain insufficiently specified. Previous studies have mainly focused on functional outcomes or technology adoption behaviors.6–8,55 As a result, we still know little about how cognitive, social, and affective processes work together to shape psychological resilience. This mixed-methods study examined how DHL relates to self-efficacy among older adults through direct and indirect pathways, with particular attention to the mediating roles of social support and life satisfaction and the moderating role of health consciousness. The findings show that DHL is associated with self-efficacy both directly and indirectly via social support and life satisfaction, and that these associations are stronger among older adults with higher health consciousness. These results extend existing knowledge of how technological competencies are embedded in the developmental context of later life and offer both theoretical and practical implications for digital health interventions.
Direct association between DHL and self-efficacy
Our results confirm a significant direct association between DHL and self-efficacy, supporting the application of social cognitive theory in digital health contexts. This pattern aligns with Park et al., 14 who identified electronic health literacy as a robust predictor of self-efficacy among community-dwelling older adults. In contrast to general internet use, health-specific digital competencies—such as verifying medical information or navigating appointment systems—provide older adults with mastery experiences. These successful interactions constitute performance accomplishments, which Bandura identified as the most influential source of efficacy beliefs.
Qualitative findings further reinforced this interpretation through the theme of “behavioral transformation.” Participants reported that being able to monitor vital signs independently or cross-check health advice reduced their dependence on others. These experiences also changed how they viewed their ability to manage health challenges. Together, the quantitative and qualitative results suggest that the psychological impact of DHL arises from an enhanced sense of control over one's health management trajectory rather than from functional skills alone.
Mediating roles of social support and life satisfaction
Beyond the direct effect, the mediation analysis clarifies the socio-affective pathways that link DHL to self-efficacy. The finding that social support mediates this relationship is consistent with socioemotional selectivity theory, which emphasizes that older adults prioritize emotionally meaningful social interactions. 13 In the digital era, DHL becomes a key tool for sustaining and expanding these connections. This result is compatible with Song et al., 3 who showed that overcoming technological barriers is crucial for reducing social isolation.
Qualitative data echoed this mechanism in the theme of “socio-emotional support,” where participants described how digital platforms facilitated health information sharing within family and peer networks. Exchanging digital health information also worked as a form of social currency. It strengthened intergenerational ties and peer support and, in turn, increased psychological confidence. In this context, DHL does more than enable information acquisition. It also reshapes how older adults participate in relational networks that support health management and everyday coping.
Life satisfaction also emerged as a mediator in the relationship between DHL and self-efficacy. While previous research has documented bidirectional associations between life satisfaction and self-efficacy,35,36 the present study demonstrates that life satisfaction can function as a pathway through which digital competencies and social resources contribute to enhanced efficacy beliefs. This finding is consistent with the broaden-and-build theory, which proposes that positive emotional states expand cognitive and behavioral repertoires while helping individuals build durable personal resources. 17 This process may be especially salient in later life, when positive emotional experiences increasingly guide goal setting and prioritization. 32 Conceptually, this perspective differs from models that position efficacy as an antecedent of well-being and instead emphasizes how positive life evaluations create a psychological context in which confidence can develop. However, because the data are cross-sectional, longitudinal studies are needed to test the temporal ordering of these relationships and to examine potential reciprocal influences between life satisfaction and self-efficacy over time.
Sequential mediation pathway
The sequential mediation pathway from DHL through social support and life satisfaction to self-efficacy represents an important theoretical contribution. It specifies a multi-step process through which technological competencies are converted into psychological resources in later life, extending previous research on digital engagement among older adults.12,13 The mixed-methods analysis also showed how this statistical pathway appeared in everyday life. DHL made it easier for older adults to connect with others by sharing health information and joining online communities. These social resources reduced isolation and fostered a sense of belonging. Higher life satisfaction then supported more positive emotional states and broader thinking. Together, these changes strengthened confidence in managing future challenges. 8
The modest size of this indirect effect (9.43% of the total effect) reflects cumulative attenuation across multiple steps rather than limited theoretical importance. Each step marks a substantive transition from digital engagement to perceived social support, from social connection to positive life evaluation, and from life evaluation to self-efficacy. This pathway highlights that digital interventions may be most effective when they are designed not only to improve individual skills but also to shape the relational and emotional environments in which these skills are used.
Moderating role of health consciousness
The moderation analysis further refines this picture by identifying health consciousness as a critical boundary condition. Associations between DHL and psychological outcomes were significantly stronger among participants with high health consciousness. This pattern is consistent with the Integrative Model of eHealth Use, which highlights the role of motivational factors in determining how efficiently individuals convert resources into health outcomes. 16 Participants with high health consciousness engaged in what Liu et al. 16 describe as “health-promoting lifestyles,” actively using digital resources to pursue specific health goals.
The qualitative theme of “cognitive-motivational processes” helped explain these results. Participants with higher health consciousness described more systematic ways of processing information and reported deliberately integrating digital advice into their daily routines. In contrast, participants with lower health consciousness tended to consume information more passively. They were less likely to act on what they had learned, which limited the translation of digital skills into psychological efficacy. These findings suggest that DHL provides the basic capability for self-efficacy, whereas health consciousness determines how strongly this capability is used.
Cultural context and generalizability
The cultural specificity of the Chinese context introduces important boundary conditions for interpreting these findings. First, the prominence of the social support pathway may be especially salient in a collectivistic value system that emphasizes interdependence and social harmony. In contexts where interpersonal relationships are central to self-concept, digital health engagement may yield distinctive psychological benefits through social connection. Whether the socially mediated pathway identified here operates with the same strength in more individualistic cultures, where autonomy is emphasized, remains an open empirical question. In such settings, direct pathways from competence to efficacy might play a larger role.
Second, traditional Confucian values of filial piety are likely to shape technology-use patterns, as adult children often act as primary facilitators of their parents’ digital engagement, as illustrated by Participant 23's reliance on their daughter. 24 This configuration may not generalize to contexts where older adults prioritize independence or rely more heavily on formal training and peer networks. Finally, China's digital ecosystem—dominated by integrated super-apps such as WeChat—and its rapidly digitizing healthcare system create a distinctive environment for digital health engagement. Future cross-cultural studies are needed to separate general psychological mechanisms (such as the sources of efficacy described in social cognitive theory) from culture-specific patterns.
Practical implications for digital health interventions
The findings of this study have practical implications for policymakers, healthcare practitioners, and technology developers seeking to narrow the digital divide in aging populations. The results suggest that fostering self-efficacy requires a shift from interventions that focus solely on functional skills to a broader, resource-oriented empowerment approach.
Given that social support significantly mediates the relationship between DHL and self-efficacy, interventions should move beyond solitary instruction. Community-based programs can establish “digital health circles”—peer-learning groups in which older adults learn collaboratively. 8 Such programs activate the social support pathway from the outset, transforming learning into a social bonding experience. In light of the importance of intergenerational relationships in the Chinese context, educational initiatives should also involve family members as “digital health partners,” equipping them with strategies to support older relatives while avoiding over-dependence. 13 Because this study relied on perceived DHL, future intervention trials should also include objective performance-based assessments. This will help check whether gains in self-reported confidence translate into actual competence in core digital health tasks.
The moderating role of health consciousness indicates that a “one-size-fits-all” approach is unlikely to be effective. Interventions should be tailored to different levels of health consciousness. For older adults with lower health consciousness, the primary barrier is often motivational. Programs for this group should first highlight the practical value of digital tools, such as easier appointment booking or medication refills, rather than focusing on abstract long-term health benefits. Simplified interfaces and immediate positive feedback can help reduce cognitive load and prevent disengagement. 16 For older adults with higher health consciousness, the focus should shift toward “critical digital literacy.” Because these individuals actively seek information, they may be particularly vulnerable to misinformation. Training should therefore stress source verification, critical appraisal of online content, and the ability to distinguish evidence-based advice from commercial advertising. 14
Because life satisfaction operates as a cognitive and affective expansion mechanism, digital health platforms should incorporate principles from positive psychology. User interfaces can also provide small emotional rewards, such as visualizing health trends, celebrating adherence milestones, or acknowledging incremental progress. These features may help start positive emotional cycles. 6 By recognizing users’ achievements and making progress visible, digital technologies can support positive self-evaluations and, over time, stronger self-efficacy.
Limitations and future research directions
Although this study provides robust support for the proposed integrated model, several limitations should be acknowledged. First, the reliance on self-reported measures of DHL, particularly the eHEALS, 55 means that the study captures perceived confidence rather than objective performance. As recent critiques have noted, 5 self-reports may be affected by the Dunning–Kruger effect: some older adults may overestimate their competence, while others underestimate their skills because of low technology confidence. Our findings indicate that perceived capability is an important predictor of psychological self-efficacy, but future research should integrate performance-based assessments (e.g., simulated tasks such as booking appointments or locating reliable information) to examine how perceived and actual competencies align. Second, the cross-sectional design precludes causal inference. Longitudinal studies using cross-lagged panel models are needed to disentangle the reciprocal dynamics between DHL and self-efficacy over time.
Third, sampling constraints limit the generalizability of the findings. The quantitative sample was drawn primarily from community centers in established neighborhoods, which may underrepresent older adults who are homebound, lack internet access, or live in remote rural areas. These groups are likely to encounter different barriers from those faced by participants in the current study. Future research should use stratified sampling strategies to include these hard-to-reach populations so that digital health interventions can be designed to meet the needs of the most vulnerable segments of the aging population. 8
Conclusion
Despite the increasing digitization of healthcare, the psychological mechanisms through which technological competencies become enduring personal resources in later life have not been clearly specified. This mixed-methods study examined how DHL relates to self-efficacy among older adults and identified a sequential pathway involving social support and life satisfaction, with health consciousness shaping the strength of these associations. The findings indicate that higher DHL is associated with greater self-efficacy in part because it is linked to stronger perceived social support and more positive life evaluations, and that these links are more pronounced among older adults with higher health consciousness.
This study contributes to theory by integrating social cognitive, broaden-and-build, and socioemotional selectivity perspectives into a focused model that connects perceived digital health capabilities with socio-relational and affective resources in later life. Practically, the results suggest that digital health interventions for older adults should extend beyond skills training to also cultivate supportive social environments and positive health orientations. Future research should test these mechanisms using longitudinal and cross-cultural designs and incorporate objective measures of DHL alongside self-reported confidence.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261415930 - Supplemental material for Digital health literacy and self-efficacy among older adults: Mediating roles of social support and life satisfaction and the moderating role of health consciousness
Supplemental material, sj-docx-1-dhj-10.1177_20552076261415930 for Digital health literacy and self-efficacy among older adults: Mediating roles of social support and life satisfaction and the moderating role of health consciousness by Yang Xin and Luo Minyang in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076261415930 - Supplemental material for Digital health literacy and self-efficacy among older adults: Mediating roles of social support and life satisfaction and the moderating role of health consciousness
Supplemental material, sj-pdf-2-dhj-10.1177_20552076261415930 for Digital health literacy and self-efficacy among older adults: Mediating roles of social support and life satisfaction and the moderating role of health consciousness by Yang Xin and Luo Minyang in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors want to thank all the participants who helped them complete this study.
Ethics approval and consent to participate
The Ethics Committee of Guangxi University approved this study (No. 20231126). All participants took part voluntarily and provided written informed consent prior to participation.
Consent for publication
This manuscript does not contain any identifying images or personal/clinical details of participants.
Authors’ contributions
Yang Xin: writing–original draft, software, project administration, methodology, funding acquisition, formal analysis, data curation, and conceptualization. Luo Minyang: writing–review and editing, validation, supervision, project administration, methodology, funding acquisition, formal analysis, and conceptualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovation Project of Health Economic and Social Development Research Center, 2023 Guangxi Philosophy and Social Sciences Planning Research Project, and Philosophy and Social Science Research Project of Guangxi Medical University (Grant Numbers: 2025RWB15, 23CSH015, and 2025B08).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Use of AI tools in the writing process
The authors did not use generative AI or AI-assisted technologies in the conception, analysis, or writing of this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.