
Abstract
Objective
This study aims to explore the mediating roles of technological interactivity and technological anxiety in the relationship between perceived usefulness and the willingness to use a smart health device to provide insight into the decision-making process of older adults in relation to the adoption of smart devices.
Methods
A cross-sectional survey was conducted in Jiangsu, China involving 552 older adults. The study utilized structural equation modeling (SEM) to analyze the relationship between the independent variable ‘perceived usefulness’ and the dependent variable ‘willingness to use.’ It also examined the multiple mediating effects of technological interactivity and technological anxiety between the independent and dependent variables.
Results
The results indicate that the direct effect of perceived usefulness on willingness to use was insignificant. However, technological interactivity completely mediated the relationship between perceived usefulness and willingness to use. Additionally, technological interactivity and technological anxiety were found to have a serial mediating effect on the impact of perceived usefulness on willingness to use smart healthcare devices.
Conclusions
These findings suggest that increasing older adults’ intention to use smart healthcare devices requires not only raising awareness of their usefulness, but also addressing technological anxiety and enhancing the interactivity of these devices to improve the overall user experience.
Keywords
Introduction
The emergence of smart senior healthcare driven by the rapid development of technologies, such as the Internet-of-Things (IoT), big data, cloud computing, and artificial intelligence (AI), along with the integration of the internet industry with the aging industry, has become a new strategy for addressing population aging and revolutionize traditional eldercare approaches, which relies mainly on medical treatment and non-technical human aging services. The Chinese government and various social sectors have placed significant emphasis on Smart senior healthcare. 1 In 2020, the Ministry of Industry and Information Technology (MIIT), Ministry of Civil Affairs (MCA), and National Healthcare Commission (NHC) jointly released the “Smart Healthcare Products and Services Promotion Directory.” The directory outlined serval categories of smart health and wellness technology products, including monitoring, assistive, and health management devices, service robots, and medical digitalization products, specifically encompassing diverse products, such as remote monitoring devices based on the sensor technology (e.g., sign monitoring devices, body sensors, sound and light alarm devices, etc.), smart medical kits (e.g., integrated medical examination devices and health management APPs), smart mobility assistants, health information management and service platform, and so on. 2 Currently, these products have started to be utilized in telemedicine, health management, and daily life care scenarios.
The application of smart healthcare devices has the potential to significantly enhance the independence, safety, and overall quality of life for older individuals in the community.3,4 In particular, health monitoring devices based on mobile and wearable technologies, such as smart hand badges, smart watches, and smart badges, can be worn by older persons for monitoring their physical health and activity data in real time and providing communication functions, which can be helpful in the early detection and intervention of certain health issues that are commonly found in older persons, such as deterioration of physical functions, chronic diseases, and psycho-emotional problems.5–7 Smart healthcare devices can gather substantial active or passive generation of patient-generated health data (PGHD). 8 These data encompass information like subjective self-reports of physical and mental health status, including anxiety, depression, stress, post-traumatic stress disorder (PTSD), self-rated health (SRH), chronic diseases, and activities of daily living (ADLs), by the device users and diagnostic records by healthcare providers, as well as information from the objective behaviors and body metrics from the passive monitoring of smart devices (e.g., smartphones, remote health monitoring devices, etc.) used by the individual.9–11 These also include changes in social connections as indicated by the SMS mode, changes in movement trajectories based on the location function, and changes in gait based on AI algorithms, as well as heart rate, blood pressure, body weight, sleep duration, exercise function, etc. These digital phenotypes and biomarkers generated and recorded through smart healthcare devices can provide more information about disease trends, which can help detect, interpret, or predict disease course and alert health care providers to the need of taking preventive measures.8,12,13
Despite the potential benefits of smart healthcare devices in supporting the health management of older adults, there are several challenges to their widespread adoption. Currently, the development of Chinese smart senior healthcare is primarily driven by technology, but without sufficient consideration for the willingness and needs of older adults to embrace smart healthcare devices and service options. The key challenge for industries is not just developing new products, but also ensuring that older adults incorporate smart technological products into their daily lives. 14 In order to promote the generalization of smart healthcare devices such that they can play a fully positive role in the health management of the elderly, it is important to understand the older adults’ willingness to use them and the mechanisms that influence their willingness to use.
In an attempt to explain the determinants of the wide acceptance of computers by individuals, Davis (1989) constructed a technology acceptance model based on the Theory of Reasoned Action. 15 Since its proposal, the model has been validated in numerous different empirical studies and has become the most widely used analytical model for technology acceptance and usage. 16 Many extended models have been developed based on the TAM model, including the Advanced Technology Acceptance Model (ATAM) and the Unified Theory of Acceptance and Use of Technology (UTAUT), and have been instrumental in understanding the factors that promote technology acceptance and identifying key factors that drive adoption.17–21 Among these models, perceived usefulness and perceived ease of use emerge as two significant predictors of technology acceptance. Perceived usefulness refers to the anticipated benefits of the technology in achieving a goal, while perceived ease of use pertains to the ease with which individuals expect to adapt to the technology.19,20 Notably, the TAM and its various modified versions highlight perceived usefulness as a critical factor in technology adoption. 22 Lim et al. (2011) stated that the decision to adopt technology is mainly driven by utilitarian motives. This indicates that older adults must first be convinced that the digital health technology is beneficial to their health before they decide to use it. 23 A study of seniors in Singapore suggested that perceived usefulness significantly predicts willingness to use e-services. 24 Other studies confirmed that perceived usefulness has a positive effect on older adults’ willingness to use mobile health services.18,25,26
In general, smart health and wellness technology products have proven to be beneficial for older adults experiencing declining physical functioning. These products support healthy, comfortable, safe, and dignified living, and majority of the older adult population recognizes the usefulness of these products.7,27–29 However, older adults do not have a high willingness to use and accept these products. This conflicting situation may be strongly associated with the issue of the “digital divide.” The digital divide implies a gap in the availability and utilization of modern information technology between different social groups. 30 With inadequate skills and abilities, older persons are the more vulnerable group in the digital divide and are more likely to experience problems like difficulties in interacting with technology and technological anxiety.31–33 These challenges have become particularly prominent during the COVID-19 pandemic as many essential services, including healthcare services, have transitioned to online platforms. 34
Technological interactivity is the ability to interact between a person and the system or the feedback received from the system. 35 It is also the most important feature in a smart heath device system and has a significant impact on the willingness to use. 36 Hsu et al. (2005) suggested that interactivity involves real-time and useful information. 37 Older adults can access a variety of health information through smart health devices to help with self-health management. 38 The elderly’s ability to use the diverse functions of smart health devices as needed familiarizes themselves with various interaction mechanisms. Exchange information with others through these mechanisms can enhance their knowledge and problem-solving abilities, as well as their self-confidence, leading to a greater willingness to accept and use smart recreational devices. Some evidence suggests that interactivity contributes to older people's awareness of and interest in technology, thereby promoting its adoption and use.39,40
By contrast, technology anxiety and resistance to change can affect older adults’ uptake of technology. 41 Technology anxiety refers to the concerns and fears individuals have about using technological devices. 42 Individuals may experience varying levels of technological anxiety, which is influenced by the demographic, socioeconomic, and perceptions of technology.43–45 Older adults may face more technological barriers and inequalities due to vulnerabilities in technology contact (opportunities, skills, abilities, etc.), which make them more likely to be anxious about technology.42,46 Technology anxiety may lead individuals to experience nervousness, hesitation, and errors when actually manipulating technology, reducing the experience of technological interactivity, and affecting their confidence and willingness to use technology.42,47 There is evidence that emotional reactions, such as fear and nervousness, when using or planning to use computers can influence attitudes towardf computer products. Computer anxiety encompasses the discomfort, fear, nervousness, or worry individuals experience while learning to use a computer, using a computer, or anticipating an encounter with a computer. This negative reaction can lead to an unfavorable attitude toward computers, accompanied by physiological and psychological discomfort, which further impedes future computer learning and use.48,49
Existing studies focused on examining factors that promote technology acceptance among older adults and found that perceived usefulness has a significant impact on older adults’ willingness to use technology products. However, there is limited understanding on the willingness to use smart health devices and share health-related data with healthcare providers among Chinese older adults.27,50 There is a relative lack of studies exploring the influences of perceived usefulness on willingness to use smarter healthcare devices in China, and the underlying mechanism of these associations remains unclear. In light of the important relationships and predictive impacts between these factors, it is essential to construct a theoretical model to explicate the linkage between perceived usefulness and willingness to use smart healthcare devices. Therefore, this study aims to investigate the influence of perceived usefulness on willingness to use smart healthcare devices among Chinese older adults while also examining whether or not technology interactivity and technology anxiety play a mediating role in this relationship. The study was started in April 2023, with the whole research period taking 6 months. The findings of this study will contribute empirical evidence for relevant government departments and stakeholders (e.g., hospitals, community service providers, health care institutions, practitioners in the smart health care industries, etc.) in terms of the development of policy options and practice strategies to promote the widespread adoption of smart healthcare devices, enabling their positive impact on the health management of older adults. According to previous research findings, this study proposes the three following research hypotheses:
H1: Perceived usefulness has a positive impact on Chinese older adults’ willingness to use smart healthcare devices. H2: Technological interactivity and technological anxiety play mediating roles in the association between perceived usefulness and willingness to use smart healthcare devices. H3: There is a serial multiple mediation effect of technological interactivity and technological anxiety on the association between perceived usefulness and willingness to use smart healthcare devices.
Methods
Participants
This study was a cross-sectional survey conducted in Wuxi City, Jiangsu Province, China from June to September 2023, encompassing 29 communities (14 urban and 15 rural). The sampling method utilized a combination of purposive and quota sampling. The participants were initially selected based on specific criteria aligned with the study's objectives (purposive sampling). The study drew upon definitions from the United Nations, 51 Chinese laws, 52 and empirical studies53,54 to target elderly individuals aged 60 years and above who were capable of independently completing the questionnaire survey and possessed some basic knowledge of smart healthcare products. Those lacking awareness of smart health services or products, as well as individuals unable to participate due to limitations in daily activities or cognitive abilities, were excluded. Furthermore, a cross-quota sampling approach was used to mitigate the sampling bias. To address the challenge of maintaining a consistent sex ratio among middle- and high-aged older adults, the age groups (60–70 and 70 + ) were used as a surrogate quota sampling indicator. The sample size was determined based on the senior population base and age groups in each community, with a certain proportion allocated to each age group (10% of the senior population base in the community, divided equally between the 60–70 and 70 + age groups). The survey was conducted through face-to-face interviews by trained surveyors. Equipped with a specialized electronic questionnaire app, surveyors posed questions to the elderly and recorded their responses on tablet computers. A total of 619 questionnaires were distributed and returned, resulting in a 100% response rate. After excluding 23 invalid questionnaires with over half of the questions unanswered or with highly repetitive responses and 44 participants who reported complete unawareness of smart healthcare devices, a total of 552 questionnaires were utilized for statistical analysis.
Measures
Perceived usefulness
The perceived usefulness of smart healthcare devices was measured using a translated Chinese version of the Perceived Usefulness Scale developed by Davis (1989). 19 Careful steps were taken to ensure the accuracy of all scale's translation, including the technological interactivity and technological anxiety. A doctoral student proficient in English and a native English speaker (a master's degree student in psychology at a Chinese university) were involved in verifying the accuracy and readability of the translated scale. The steps included initial translation, back-translation by the English major student, and verification by the native English speaker to ensure consistency with the original scale. Any discrepancies were addressed through team meetings, resulting in a finalized Chinese version of the scale. The scale consisted of two items: ‘The use of smart healthcare devices could effectively improve my health’ and ‘The use of smart healthcare devices could promote the quality of life.’ The participants were asked to rate how well these descriptions matched their own perceptions for each question on a scale of 1 to 5, with 1 indicating a poor match and 5 indicating a strong match. Higher scores on the scale indicate a higher perceived usefulness of the device. The Cronbach's α for the scale was 0.84, with a relatively great reliability.
Technological interactivity
The technological interactivity scale developed by Cyr et al. (2009) was used to measure the interaction of older adults with smart devices. 55 A Chinese translated version of the scale was used in the survey process. The scale consisted of four dimensions: feedback, control, entertainment, and connection. It contained 11 items, including ‘I can quickly search the required information through smart healthcare devices,’ ‘I can easily select the functions of smart healthcare devices,’ ‘It is interesting to use smart healthcare devices,’ and ‘I would explain how to use the smart healthcare devices when people ask me’, among others. The participants were asked to rate each item based on their own situation using a scale from 1 (completely inconsistent) to 5 (completely consistent). Higher scores indicated a higher level of technological interaction. The overall reliability of the scale was assessed using Cronbach’s α, which yielded a value of 0.87. The reliability values for each dimension were as follows: 0.87 for feedback, 0.88 for control, 0.80 for entertainment, and 0.89 for connection.
Technological anxiety
Technological anxiety was measured using a scale developed by Spagnolli et al. (2014). 56 The Chinese translated version of this scale was employed in this study. The scale measured the participants’ level of anxiety regarding the use of smart healthcare devices. It consisted of two dimensions: operation anxiety and information exposure anxiety. The scale included statements, such as ‘I worry about not understanding how to use smart healthcare devices’ and ‘I worry about the potential leakage of personal data when using smart healthcare devices,’ along with 11 other items. Scores on the scale ranged from 1 to 5, with higher scores indicating greater anxiety about using smart healthcare devices. The overall reliability of the scale, as measured by Cronbach's α, was found to be 0.79. Specifically, the reliability for operation anxiety was 0.72, and that for information exposure anxiety was 0.74.
Willingness to use
To assess the participants’ willingness to utilize smart healthcare devices, they were shown visual aids, including pictures and images, illustrating six commonly used categories of smart healthcare devices in China. 2 These devices included monitoring devices, assistive devices, health management devices, service robots, and medical digital products, among others. The participants were then asked to rate their willingness to use each product on a fivr-point rating scale, ranging from 1 (indicating no willingness at all) to 5 (indicating a high level of willingness). The mean score was employed for analysis, where higher scores denoted a stronger willingness to use the smart device.
Control variables
This study included control variables, such as age, gender, education, and economic status. Age was a continuous variable. Gender was used as a binary variable coded as 1 for males and 0 for females. The educational level was measured by the years of education. The personal economic status of the participants was measured using the average monthly income.
Statistical analysis
The data were processed and analyzed using SPSS 25.0 and AMOS 25.0 software. The analysis steps were as follows: (1) a descriptive analysis was conducted to assess the normality of the main variables and gather the demographic and sociological characteristics of the participants; (2) a reliability analysis was performed to ensure the measurement consistency; (3) a correlation analysis was used to confirm the relationship between key variables; (4) the model fit was assessed based on the Chi-squared (χ2) test, degrees of freedom, root mean square error of approximation (RMSEA), comparative fit index (CFI), and Tucker‒Lewis index (TLI); and (5) the relationship between the independent variable, perceived usefulness, and the dependent variable, willingness to use smart healthcare devices, was analyzed using a structural equation model. The multiple mediating effects of technological interactivity and technological anxiety between the independent and dependent variables were also verified. The bootstrap method was employed to calculate the confidence interval of the mediation effect and test its significance.
Result
Descriptive statistics
Table 1 presents the general characteristics of the study participants. The participants had a mean age of 72.28 (S.E. = 8.39), with 65.9% being women and 34.1% being men. In terms of the education levels, 37% had elementary school or less education; 37.7% had middle school education; and 25.4% had high school education or above, indicating a relatively low level of education among the participants. The average monthly income of the participants was CNY 3390. The majority of the participants were married with a spouse (74.1%) and lived with their family (85.4%). On average, the elderly participants had 1.69 children. The residence distribution of the participants was relatively balanced, with 55.4% living in urban areas and 44.6% residing in rural areas. The overall physical and mental health of the participants was relatively good, with a mean number of chronic illnesses of 1.04 and a depression level of 1.45 (min = 1, max = 4).
General characteristics of participants.
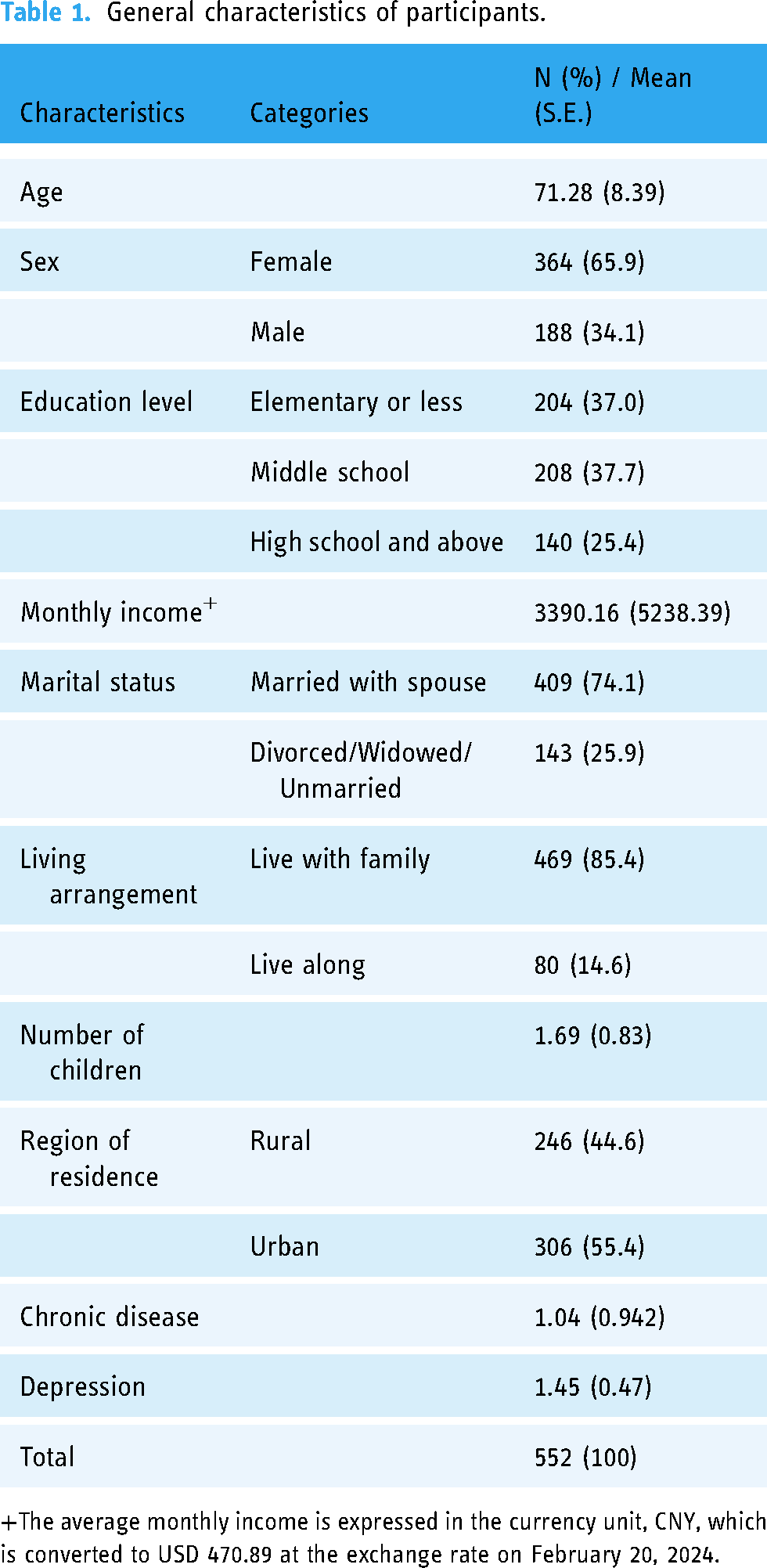
The average monthly income is expressed in the currency unit, CNY, which is converted to USD 470.89 at the exchange rate on February 20, 2024.
As shown in Table 2, the participants reported a high level of perceived usefulness for smart healthcare devices (mean = 3.89, S.E. = 0.988). As regards technology interactivity and technology anxiety, the participants described themselves as having better interactivity (mean = 3.28, S.E. = 0.803) and expressing a lesser technologically anxious tendency (mean = 2.57, S.E. = 1.071). Comparatively, the participants had lower scores for willingness to use (mean = 2.83, S.E. = 1.037). All main variables had a skewness (ranging from −1.185 to 0.430) of less than 2 and a kurtosis (ranging from −1.588 to 1.196) of less than 7, indicating a normal distribution. 57 The correlation coefficients between the variables ranged from 0.131 to 0.470, and all of them were statistically significant. To determine multicollinearity, we conducted multiple linear regression analysis and found that all variables had a tolerance greater than 0.1 (ranging from 0.735 to 0.927). All variance inflation factor (VIF) values were less than 10 (ranging from 1.079 to 1.361), indicating no multicollinearity problem.
Descriptive and correlation analysis of the main variables.

*p < .05, **p < .01.
Structural model analysis and testing of mediation effects
This study utilized a structural equation model (SEM) to examine the effects of technological interactivity and technological anxiety as mediators between perceived usefulness and willingness to use smart healthcare devices (Figure 1). The results presented in Table 3 indicate that the path coefficients for perceived usefulness to technological interactivity (C.R. = 12.047, p < .001), technological interactivity to willingness to use (C.R. = 3.63, p < .001), perceived usefulness to technological anxiety (C.R. = 2.454, p < .01), technological anxiety to technological interactivity (C.R. = −5.337, p < .001), and monthly income to willingness to use (C.R. = 1.973, p < .05) were all statistically significant. However, the path coefficient for technological anxiety to willingness to use (C.R. = 1.676, p = .091) and perceived usefulness to willingness to use (C.R. = 1.689, p = .095) were found to be insignificant. H1 has not been supported.

Multiple mediating effect model.
Results of the mediating effect test.

*p < .05, **p < .01, ***p < .001.
PU: perceived usefulness; TI: technology interactivity; TA: technology anxiety; WTU: willingness to use.
Our study examined the mediating effects of technological anxiety and technological interactivity on the association between perceived usefulness and willingness to use a smart health device through bootstrapping. The bootstrap method was employed to estimate the standard errors of the direct and indirect effects of the mediating variables. The confidence interval values were also determined using this method to demonstrate the statistical significance of the indirect or direct effects of the mediating variables. A confidence interval value not containing 0 indicates significance. 58 The results of the bootstrapping test are shown in Table 4, where there is a statistically significant mediating effect of technological anxiety and technological interactivity on the relationship between perceived usefulness and willingness to use (95% CI = 0.171–0.752). The total effect was 0.744, with a direct effect of 0.304 and an indirect effect of 0.440. These results indicate that technological anxiety and technological interactivity play a role in the impact of perceived usefulness on willingness to use. The technological interactivity having a significant complete mediating effect (coef. = 0.434, 95% CI = 0.14–0.724) and technological anxiety having a non-significant mediating effect (coef. = 0.029, 95% CI = −0.003–0.1) provide partial support for H2. There were also significant serial mediating effects of technological anxiety and technological interactivity (coef. = −0.023, 95% CI = −0.089 to −0.003). Therefore, H3 was supported.
Bootstrapping on pathways of the multiple mediation models.

PU: perceived usefulness; TI: technology interactivity; TA: technology anxiety; WTU: willingness to use.
Discussion
This study examines the relationship between perceived usefulness, technological interactivity, technological anxiety, and willingness to use smart healthcare devices from the perspective of Chinese elderly. The first main finding of this study revealed that the relationship between perceptive usefulness and willingness to use was completely mediated by technological interactivity. The results showed that older adult participants with higher levels of perceived usefulness also demonstrated higher levels of technological interactivity, which further increased their willingness to use smart healthcare devices. This is consistent with previous findings that when older adults perceive certain technologies as having utility, it facilitates their interactions with those technologies, thereby increasing their willingness to use them. 59 Therefore, in addition to raising awareness about the usefulness of these devices, it is crucial to enhance their interactivity and interactive experience for older adults. Many older adults are unfamiliar with and skeptical of new technologies, leading to a conservative attitude. However, this attitude can be changed through positive education and effective interventions.
One possible approach is to provide training and guidance on the basic capabilities of smart device use and establish links with community school resources. Specifically, government departments, schools, and relevant enterprises can enter communities or elderly institutions to jointly organize regular education on network information security, smart healthcare product publicity, experiential activities, and so on. These can increase older people's awareness of and familiarity with relevant products and improve their digital literacy. The role of social networks and interpersonal interaction can also be utilized. By inviting friends and relatives to participate with older adults can enhance the influence, trust, intimacy, learning atmosphere, and continuity of the activities, thereby improving the promotion and educational effect of the activities. 60 Intergenerational mutual assistance can also be leveraged, involving teenage high school and college student volunteers who can teach older adults the methods and knowledge of smart device utilization. 61
Furthermore, there is a need to optimize the interface and the functionality of smart health care devices to make them simple and intuitive, bear a reduced visual strain, become easy to operate, etc. These age-friendly designs can help reduce learning costs and barriers to use while increasing the emotional value and sense of acquisition associated with using these devices. For instance, the DESAY mobile phone in China, through Shi suitable for the elderly device interface and function design, differentiated services to bring a good user experience to the elderly (Liu Yuan, Li Shiguo 2015). When technology delivers the expected benefits, and seniors have a positive interactive experience, it strengthens their connections with family, friends, and the community, boosts their confidence in their own abilities, and subsequently enhances their positive attitudes and willingness to use smart healthcare devices.
Another important finding is that there is a serial mediating effect of technological interactivity and technological anxiety on the influence of perceived usefulness on willingness to use. In other words, when older adults have a greater awareness of the uses and advantages of smart devices, their level of technology anxiety increases. However, positive technological interactions mitigate the negative effects of technology anxiety and ultimately increase the older adults’ willingness to use smart devices. Older adults’ desire to use new technology is often accompanied by concerns about its complexity and safety. 10 Good interactive experiences and feedback (human–computer interactions with the device or device-based interpersonal interactions), by contrast, can be effective in reducing these concerns and ultimately increase older adults’ willingness to use smart devices.18,29,62 Therefore, it is crucial to pay attention to the security of smart devices and products for the elderly, ensuring the safety of their data and privacy during use, and addressing anxiety and personal risks related to privacy and data leakage while enhancing the age-friendliness of the devices and improving the interactive experience. For instance, Singapore's “Dr Covid + ” App reduces the risk of privacy breaches and data linkage by using Telegram IDs for patient-care communication and patient health tracking instead of saving mobile numbers linked to electronic medical records. 6 Additionally, companies and developers of intelligent health equipment should focus on meeting the actual needs of elderly users, enhancing the age-oriented design of intelligent health devices and products, reducing the learning costs and barriers to utilization for the elderly, and improving the user experience and comfort of the human–computer interaction. Effective marketing and promotion strategies should also be implemented to motivate older adults to continue using smart healthcare devices.
Finally, the descriptive analysis found that older adult participants generally had positive attitudes toward the perceived usefulness (mean = 3.89, S.E. = 0.99) of smart healthcare devices. They believed that these devices could enhance health management efficiency and improve daily life convenience. The recognition of smart healthcare products and services for the elderly has been increasing in recent years due to the efforts of the Chinese government to emphasize and promote them. However, the willingness to use smart devices (mean = 2.83, S.E. = 1.04) is only moderate and not particularly strong. This indicates that Chinese seniors have a lukewarm demand for smart healthcare devices, and that these products have not been effectively integrated into their daily lives. 14 These results also imply that an increased recognition of perceived usefulness does not necessarily translate into a higher willingness to use such devices. There may be additional critical factors influencing the willingness to use smart devices, such as technological interactivity and technological anxiety.
On technological interactivity (mean = 3.28, S.E. = 0.80), participants exhibited a relatively optimistic attitude toward their ability to use smart healthcare devices independently and actively. They also expressed willingness to recommend these devices to others if given the opportunity. This challenges the stereotype that older adults are generally apprehensive or inept at using technological devices. 63 In terms of technology anxiety, which refers to concerns about information security and usability, the participants responded neutrally (mean = 2.57, S.E. = 1.07). This suggests that while they do have some concerns about technological issues, such as privacy breaches and operational errors, these concerns are not particularly strong. Further investigation is necessary to explore the more nuanced aspects of technology anxiety and gain insights into specific issues and their impact on the adoption of these technologies. Specifically, for smart health products targeting older adults, prioritizing system security is essential. By utilizing mobile software to display and collect a significant amount of activity data, older adults can easily manage their diseases, while service providers can offer personalized services based on the collected health data.8,13,64 For example, according to the health assessment dataset, personalized health plans are formulated, including guidance and recommendations on diet, exercise, sleep, and mental health. Health-related knowledge and education are provided in response to individual health needs and characteristics, and health plans are adjusted promptly to ensure the effectiveness of individual health management through regularly monitoring the individual's health indicators and behavioral changes. However, it is crucial to carefully consider the issue of personal privacy and determine the content or scope of shared information. Failing to do so may lead to negative consequences associated with the use of technological products.
There are several limitations to this study that need to be addressed in subsequent studies. First, this study used purposive sampling to survey older adults in Wuxi, Jiangsu Province, which may lead to limitations in the generalization of the results. In other words, the findings may not be applicable to all older persons, and the conclusions need to be interpreted and generalized cautiously. Especially given the diversity of older adults in China and globally, further verification is required before inferring the findings to other groups or intelligence devices. Future studies will aim to expand the geographical area of the survey and increase the sample diversity to enhance the validity of generalizing the findings. Second, in this study, the measures of technology anxiety and technology interactivity were evaluated collectively for smart health care devices, rather than asking for perceptions of different devices separately. Considering the variability of the usage features and the scenarios of different smart healthcare devices, the emergence of technology anxiety and interaction difficulties will be different. Therefore, the statistical model has limitations, namely, it can only provide clues to the generalized relationship between the variables, but cannot present the situation in different devices and usage scenarios in a detailed way. It is necessary to conduct more elaborate investigations on specific devices in subsequent studies to increase the accuracy of the research results. Third, this study relied on self-reporting tools for data collection. However, such instruments have limitations in capturing dynamic variables like perception of usefulness, technological interactivity, technological anxiety, and willingness to use smart healthcare devices. People's subjective views on these variables may change over time. Therefore, future work should assess the relationship between variables longitudinally. Fourth, this study utilized cross-sectional data for analysis, restricting the ability to establish causal relationships between variables. In subsequent studies, the relationships between variables will be verified through longitudinal data tracking and analysis or by conducting randomized experimental/control group studies to strengthen the credibility of the findings. Fifth, the limitations of our survey data prevented us from considering other potential factors that could influence the willingness to use smart healthcare devices among elderly. These factors include sociocultural context, health literacy and beliefs, cognitive ability, and others. Future research should focus on studying the contributions of these factors in understanding willingness to use and accept smart health and wellness technology products.
Conclusion
Older adults adopt newer technologies at a slower rate compared to younger adults, and this can impact the adoption and use of healthcare technologies that might facilitate the detection of and intervention for age-related health problems.65,66 However, the potential of these technologies for improving the health and independence of older adults depends crucially on adoption by older adults, which depends on their willingness to use. This study explores the complex decision-making process of older adults using smart devices by investigating how the perceptive usefulness affects willingness to use smart health devices in Chinese elderly. The study also examines the multiple mediating effects of technological interactivity and technological anxiety on this relationship. The SEM analyses indicated statistically insignificant path coefficients for perceived usefulness and willingness to use. However, a significant fully mediating effect was found for technological interactivity, while a non-significant mediating effect was observed for technological anxiety. Additionally, there was a significant serial mediating effect observed for technology anxiety and technology interactivity. Therefore, the findings did not align with Hypothesis 1, only partially supported Hypothesis 2, and supported Hypothesis 3. The findings emphasize that improving the willingness to use smart healthcare devices among seniors not only takes increasing their perceived usefulness of these devices, but also addressing technical anxieties and enhancing their interactivity. This would effectively improve the overall user experience, promote the widespread adoption of smart healthcare devices; and lead to a positive impact on elderly people's health management.
Footnotes
Acknowledgements
The authors would like to thank all researchers, participants, and others who were involved directly or indirectly during data collection and reviewed this manuscript.
Contributorship
All authors made significant contributions to the conception or design of the study, as well as the data processing and interpretation. Additionally, all authors participated in the critical review and revision of the manuscript and approved the final version. Furthermore, all authors agreed to take responsibility for all aspects of the work.
Ethical approval and participant consent statement
This paper has been approved by the Jiangnan University Medical Ethics Committee (JNU20230901IRB09). The participants were informed about the purpose of this research and provided written informed consent before administering the questionnaire. To maintain confidentiality, personal identifiers were omitted from the questionnaires, and the collected data were stored in a secure, password-protected database without identifiers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Social Science funds of China (21BSH163), General Project of Philosophy and Social Science Research in Colleges and Universities of Jiangsu Province (2022SJYB0950), and Beijing Municipal Financial System Reform and Development Project (1020239718KF001-21) and the Jiangnan University Youth Research Fund (JUSRP12071).
Guarantor
YZ.