
Abstract
Objectives
This study establishes a research model based on the theories of affordance and the theory of psychological empowerment to understand users’ intentions in using artificial intelligence–based medical consultations (AIMCs), offering implications for their effective design.
Methods
A two-stage mixed-methods research design was employed. The first stage involved qualitative interviews to conceptualize the main affordances of AIMCs and usage intentions, and the second phase comprised a quantitative study with 425 valid samples analyzed via partial least squares structural equation modeling.
Results
The research results identified four AIMC affordances (i.e., human–AI interaction, human-like diagnosis, personalized treatment, and health information security) and two usage intentions (i.e., assist health decisions, and relieve health anxiety). The results of the quantitative analysis indicate that the four affordances significantly enhance perceived cognitive empowerment, whereas three affordances (excluding health information security) positively influence perceived emotional empowerment. Both cognitive and emotional empowerments were found to significantly affect users’ AIMCs usage intentions. Additionally, we found that different disease types (acute and chronic) play an important moderating role in the relationship between perceived cognitive empowerment and relieve health anxiety.
Conclusions
To increase psychological motivation and user adoption, AIMCs should be optimized with intuitive interactions, human-like diagnoses, and personalized care, while features should be tailored to the needs associated with acute and chronic conditions. On the basis of affordance and psychological empowerment theories, this study provides actionable insights for the development, design, and implementation of AIMCs.
Keywords
Introduction
The World Health Organization calls for the integration of new technologies into existing healthcare infrastructure to help achieve universal health coverage. 1 Artificial intelligence (AI) provides a new approach to address the shortage of medical resources and the development of online medical services. 2 Artificial intelligence–based medical consultations (AIMCs) built on deep learning with a large amount of real consultation data and medical knowledge allow people to describe symptoms in natural language, while AI agents simulate real doctors’ consultation processes and provide targeted medical knowledge and advice. 3 Currently, AIMCs have been applied to the diagnosis of ophthalmic diseases, leprosy, and other specialized conditions. 4 They can also serve as a preliminary diagnostic tool for the diagnosis of general symptoms by general practitioners, such as Ada Health, DeepMind, and Zuoshou Doctor. 5 In real-life scenarios, AIMCs offer convenient, cost-effective, and personalized healthcare services; enhance medical care efficiency and accessibility by reducing waiting times; expand treatment opportunities; and improve the healthcare experience.6,7 For example, Chunyuhuiwen, a leading Chinese AIMC system, demonstrates clinical capability in replicating expert diagnostic patterns, effectively addressing both specialist shortages and healthcare accessibility challenges. According to a recent survey, the AI telemedicine market, including AIMCs, is expected to surge from $19.4 billion in 2024 to $156.7 billion in 2033. 8 Healthcare AI devices have become quite popular, with 80% of people expressing willingness to use them, but more than 20% of users believe that the potential benefits outweigh the risks. 9 Over time, the use of many new smart healthcare tools has become more limited and they have not been widely accepted by patients.4,10 This contradiction prompts an exploration of the key psychological motivators influencing users’ AIMCs adoption, which will provide valuable insights for developers and marketers to better understand user perceptions and to design products or strategies that align with user needs.
The literature has explored AIMCs from multiple perspectives, including the design and mechanisms from a technological perspective,11,12 application effectiveness in specific scenarios,4,13 and user psychology and behavior.14,15 Explorations from a psychological perspective primarily focus on users’ behaviors in using AIMCs and examine factors such as trust as well as perceived behavioral control, perceived value, perceived risk, and perceived usefulness to understand the influences on user behavior and decision-making in regard to AIMCs.7,14,16 These factors and perspectives provide valuable insights into understanding the use and adoption AIMCs from the user perspective. However, gaps remain that require further exploration.
First, studies have highlighted technological characteristics,5,17 user perceptions,7,15 and individual differences, 3 but have rarely focused on how the relational exchange between users and technological artifacts influences the decision-making process of AIMCs usage. Unlike traditional information technology, which merely integrates static interactive modules and functions for performing specific computational tasks, AI technology acts as a dynamic agent, actively engaging with users during interactions. 18 Especially in the diagnosis process, AIMCs enable users to perceive the program's value through the interaction process of consultation information with users. The existing research has not paid much attention to the user psychology in this interactive technological–enabling process. People expect that professional medical advice can be obtained through AIMCs diagnosis, and many patients use AIMCs to seek emotional comfort, such as relieving the tension, anxiety, fear, and other bad emotions brought on by the disease. 19 Therefore, it is more necessary to explore the impact of technological empowerment on user psychology and behavior from the perspective of human–computer interactions. Affordance theory has been extensively applied in information systems research to explore the relationship between information technology functions and their impacts. 20 Affordance theory posits that technological affordance is the technical characteristic that enables users to take actions to achieve expected outcomes. 21 Individuals must perceive this affordance and actively utilize the technology to achieve their goals, a behavior that is described as affordance actualization.22–24 Hence, affordance theory provides a comprehensive perspective for exploring how AIMCs functions influence behavioral responses. We explore the affordance dimension of AIMCs in a specific scene and attempt to reveal the affordance effect on users’ cognitive and emotional behavior decision-making.
Second, prior studies have primarily employed conventional models—such as the stimulus–organism–response framework, the technology acceptance model (TAM), and the unified theory of acceptance and use of technology (UTAUT)—to examine technology adoption. These models typically address psychological determinants such as trust or perceived usefulness and assume users passively respond to external stimuli or system attributes.3,7,15,25 However, inaccurate health diagnoses or recommendations pose significant risks to users’ lives, making AIMCs adoption and use more challenging when health concerns are addressed. Many studies have overlooked the intrinsic motivational factors driving users to proactively adopt AIMCs. In this regard, the concept of psychological empowerment provides a valuable supplement. Defined as a positive internal motivation that enables individuals to take control and make informed decisions,26,27 psychological empowerment has been shown to be influenced by technological design factors. 28 Furthermore, affordances can influence behavior by shaping personal beliefs, which can be seen as part of the affordance actualization process.22,29 When users perceive that a system affords them greater understanding (such as receiving clear, personalized health information), they may believe the AIMCs improve users’ decision-making, leading users to use AIMCs more regularly as a trusted resource for managing users’ health. We propose an integrated affordance–empowerment framework to better explain user behavior towards AIMCs. While traditional models such as TAM and UTAUT emphasize general determinants of technology use, such as perceived usefulness and performance expectancy, they often overlook how specific system features can actively empower users. In contrast, our framework emphasizes the dynamic interplay between technological affordances and users’ intrinsic psychological states. This perspective not only accounts for internal motivations but also captures the unique characteristics of AIMCs and provides a more grounded understanding of AIMC adoption.
Third, relying solely on predetermined variables and model-based quantitative research designs may not accurately reflect user experience, potentially compromising the validity of the research findings. 30 In contrast, mixed-methods research designs offer better explanatory power than single methods do and are also suitable for initial explorations of emerging phenomena, explaining user psychology. 31 Given that AIMCs are a novel self-health service, the exploration of their affordance and usage intentions is in its early stages, making it crucial to investigate the background factors that play a significant role in the successful AIMCs application. Specifically, while the research has focused primarily on adoption and reuse intentions, clarifying users’ usage intentions is crucial for understanding the factors that drive their engagement and the motivations underlying their behavior. 19 Furthermore, the current classification of medical AI affordance dimensions is generally applied,32,33 with a few studies providing more specific subdivisions in the fitness context. 20 Affordances are often contextually and must be explored within specific contexts to gain a deeper understanding of users’ perceptions and interactions with technology functionalities.29,34 This exploration should be conducted through qualitative methods rather than being restricted to quantitative research alone. Therefore, adopting a mixed-methods research design is essential to provide a comprehensive understanding of the underlying mechanisms at play.
Overall, with the help of a mixed-methods research design, this study explores the dimensional composition of AIMCs affordance from the perspective of enabling human‒computer interaction technology, and the mechanisms through which such an affordance influences users’ cognitive and emotional behavioral decisions through psychological empowerment. By integrating qualitative and quantitative research methods, our research attempts to reveal the importance and pathways of affordance to make theoretical contributions and to explore methodologically the research on user psychology and behavior from the perspective of technology enabling. Moreover, the study provides practical support for AIMCs design and optimization as well as market promotion on the basis of users’ psychological demands.
The rest of this paper is organized as follows. In “Theoretical background” section, we review the literature and introduce the theoretical background. We then conducted qualitative research, conceptualizing AIMCs affordance and its components as well as user usage intentions, proposing a research model and hypotheses, followed by quantitative testing. Finally, pivotal discoveries, theoretical advancements, practical implications, limitations, and future prospects are discussed.
Theoretical background
User psychology motivations for AIMCs adoption
Artificial intelligence–based medical consultations are innovative, digital, health self-services that use AI chatbots as automated agents to independently carry out online consultations, question answering, and case analysis. 3 Different from traditional information systems, AIMCs have a humanoid diagnostic design, personalized services, cost-effectiveness, and timely service delivery. 19 Artificial intelligence–based medical consultations not only provide convenience for individuals seeking health care but also alleviate the imbalance between medical resource supply and demand as well as uneven geographical distribution, promoting medical equity. 6
The current application value of AIMCs has garnered attention from the academic community, with researchers exploring AIMCs user behavior empirically. While studies have focused primarily on users’ adoption of and continued use intentions related to AIMC systems, the research often overlooks the diverse usage intentions of users. However, some qualitative research suggests that understanding these varied intentions could provide valuable insights for system improvement and promotion. 19 In addition, studies have examined the adoption and reuse of AIMC systems through various theoretical lenses. From the perspective of technology acceptance, factors such as perceived usefulness, ease of use, performance expectations, and risk–reward assessments have been identified as key determinants of users’ adoption behavior.7,15 In terms of technical feature design, critical factors enhancing user engagement with AIMCs are anthropomorphic design, personalized services, and source expertise.5,17 From the perspective of psychological determinants, users’ interactions with AIMC technologies are collectively shaped by trust, attitude, perceived behavioral control, perceived value, and perceived risk.14,16,25 Additionally, individual differences, particularly in health and digital literacy, play a significant role in influencing user engagement with these systems. 3 However, studies have not fully examined the functional characteristics of AIMC systems and tend to assume that technology users are passive, responding solely to technology or environmental stimuli. One of the primary objectives of AIMCs design and application is to encourage users to actively use it to address health issues. However, in reality, people often take a cautious approach to health-related solutions. Therefore, we believe that it is essential to examine the intrinsic motivations behind users’ active AIMCs adoption. To this end, this study employs a mixed-methods research design to further explore the mechanisms influencing AIMCs usage, thereby enriching the AIMCs research. Through our study, we provide empirical evidence on the psychological motivations behind users’ AIMCs adoption, offering insights for system design and promotion while facilitating the adoption and application of AIMCs in health management.
Affordance theory
Gibson 35 proposed the concept of “affordance,” emphasizing it as the property generated through the interaction between subjects and the environment. Norman 21 introduced the theory of affordance into information systems research as a way of understanding the relationships and interactions between technical artifacts and agents and exploring how technology provides different interaction patterns. Hence, affordances are shaped not only by artifact design within interactive environments but also by users’ cognitive interpretations of informational artifacts. 36 Affordance is seen as a “generating mechanism,” meaning that affordance exists in reality and that individuals need to perceive and realize affordance according to their goals, leading to different outcomes; this process is known as affordance and actualization (A-A).22,24 Pozzi et al. 23 divided the actualization process into affordance existence, perception, and actualization, as well as outcomes, attempting to describe how individuals realize what an entity can provide for them, perceive or acknowledge affordance through internal evaluation, and then take action on the basis of perceived opportunities to achieve their goals.
This theory has been confirmed through research on how technological attributes interact with individuals and operate in similar usage environments. For example, Song et al. 37 studied the impact of the affordances of short video platforms (livestreaming, searching, meta-voicing, and recommending) on user experience and the intention to continue use. Luo et al. 38 focused on the customization and personalization affordances of mobile health devices and explored how these affordances affect users’ perceived value and willingness to use. Hence, affordance theory acknowledges an individual's perceptions of technology functions and follows a process sequence of technology affordances—affordance perception—affordance actualization.22,23,29
Currently, the affordance dimensions in healthcare AI are generally defined across multiple contexts, with some studies specifically exploring the fitness domain. For instance, Zhan et al. 33 suggest that the affordance dimensions include interactivity, agency, and security affordances, which can be applied to contexts such as healthcare AI and autonomous driving systems. Liang et al. 20 categorize affordances in the context of AI fitness devices into data capture affordances, classification affordances, and social affordances. The affordance dimensions vary depending on the research context.29,34,39 To gain a deeper understanding of users’ perceptions and decision-making processes regarding AIMC systems, it is necessary to explore affordances and their dimensions specifically within the AIMCs context. Hence, in this study, we integrate mixed methods to explore the underlying mechanism of AIMCs affordances on users’ use intentions. On the one hand, qualitative research provides a comprehensive understanding of users’ perceptions and interactions with AIMCs functions, uncovering key functions in AI devices with 'black box' characteristics. On the other hand, using A–A frameworks, we can develop and test a theoretical model to explore the mechanisms through which AIMCs affordances influence usage intentions.
Psychology empowerment theory
Psychological empowerment refers to an individual's psychological state and overall sense of control over relevant issues, motivating them to engage in tasks or make decisions enthusiastically. 40 Originally applied in the organizational management research, psychological empowerment theory focused on individuals’ cognitive processes related to work decisions, beliefs, and their relationship with the organization. 41 As information technology has rapidly enhanced and individuals have increased control over accessing services, the theory of psychological empowerment has gradually extended to areas such as consumer behavior and health management.26,28 Unlike trust and perceived usefulness, which are evaluative beliefs about the system, empowerment focuses on the user's self-evaluation and feelings.7,22 It reflects perceived control over their actions and outcomes in specific contexts, motivating engagement, and decision-making. 42
Empowerment helps individuals manage challenging environmental demands. 27 When facing health issues, patients often experience worry and helplessness due to limited medical knowledge and caregiving skills. As a result, patients tend to approach health decisions with greater caution and are aware that incorrect choices can have serious consequences. Empowering patients through health self-service systems means leveraging technology to help patients identify, manage, and seek assistance for health issues, thereby increasing their familiarity with health conditions and boosting their confidence in handling health-related concerns.27,43 This positive intrinsic motivation helps individuals overcome psychological barriers and is key to individuals’ proactive engagement with technology.26,44 In addition, a well-designed technology is crucial in influencing users’ perceived empowerment. For example, Li et al. 43 emphasized the impact of gamification design in mental health self-help systems on users’ perceived empowerment, whereas Zhou et al. 28 discussed how the technological features of mobile healthcare devices affect users’ psychological empowerment. Therefore, it is essential to discuss the impact of AIMCs affordances on users’ perceived empowerment, as this concept is crucial for users’ proactive engagement with AIMCs.
The four dimensions of competence, impact, self-determination, and meaning, as proposed by Thomas and Velthouse, 40 have had a significant impact on the study of empowerment and have been applied in various contexts, such as online brand communities 26 and mobile health devices. 28 However, the constructs within the empowerment framework are highly contextually dependent and should be tailored or operationalized according to the specific application scenario. 43 Previous studies suggest that information technology empowers individuals primarily through cognitive and emotional pathways.27,43 In the AIMCs context, these applications can meet patients’ cognitive needs by providing knowledge and skills, allowing users to understand their current health status, relevant disease information, and coping strategies and to make informed decisions on the basis of the patients’ circumstances. 45 On the emotional level, using AIMCs enhances users’ sense of control over their health and increases self-efficacy in managing health issues, leading to positive emotions. 27 Therefore, we define perceived empowerment as consisting of two dimensions. The first is perceived cognitive empowerment, which refers to the extent to which AIMCs help individuals better understand their health condition and improve their ability to manage health issues. The second is perceived emotional empowerment, which refers to the extent to which AIMCs increase individuals’ sense of control, self-efficacy, and other positive emotions when addressing health concerns.
Methodology
We employed a mixed-methods research design to understand the background details and relationships of the technological affordances, perceived empowerment, and usage intentions of AIMCs. This method provides stronger inferences than a single approach does.30,46 Given the limited research on identifying the key technological affordances and specific usage intentions in the AIMCs context, a sequential mixed-methods research design is appropriate. As shown in Figure 1, we conducted such a method, utilizing qualitative research findings to inform the development of the research model for the subsequent quantitative research. This study conducted qualitative research through semistructured interviews with AIMCs users, conceptualized their primary usage intentions, and identified the key technological affordances. On the basis of these findings, a research model was proposed. A large-scale online survey was subsequently designed and implemented, in which quantitative data analysis was used to validate the proposed model and examine the impact of the identified technological affordances on perceived empowerment and usage intentions.

The mixed-methods research design used in this study.
Qualitative research
We collected data through semistructured interviews and analyzed them via grounded theory. We adopted a variable-centered grounded theory approach. This method systematically analyzes qualitative data to identify, categorize, and conceptualize key variables.31,47 The primary goal is to develop a theoretical framework that explains the phenomenon under investigation and lays a solid foundation for subsequent quantitative analyses or theoretical refinements.
Recruitment of qualitative research
We randomly invited participants through online communities (e.g., Douban, a popular Chinese knowledge-sharing and Q&A platform). The inclusion criteria were as follows: (1) familiarity with the functional features of AIMCs; (2) prior experience with AIMCs, including the ability to provide proof of use; and (3) a minimum age of 18 years.
Data collection of qualitative research
The interviews were conducted by the research team, which included one female professor of management as well as one male and one female master's student in management. A detailed interview outline was developed with guidance from three management professors. The interviews focused on the participants’ AIMCs usage, their perceptions of its functionality, and the underlying motivations for their engagement (see Appendix A). The interviews were conducted online, and all researchers received training to ensure that they were adequately prepared to collect accurate and reliable information. Prior to the interviews, the researchers provided the participants with background information about AIMCs and the study's objectives to ensure that they met the inclusion criteria. All participants were required to sign an informed consent form and were reminded of their confidentiality rights. The participants were also informed that they could withdraw from the study at any time without penalty. Each interview lasted approximately 25–30 min, was conducted independently, and was recorded and transcribed for the case analysis. A total of 23 individuals with experience using AIMCs were interviewed, and no participants dropped out. At the end of the interview, the recorded information was returned to the interviewee for confirmation. The sample characteristics are detailed in Appendix B. The interviews were conducted with 19–23 respondents, at which point the responses became consistent and no new insights emerged, indicating theoretical saturation and enabling the coding process. 48
Data analysis of qualitative research
This study employed grounded theory to analyze the interview data via a three-step coding process consisting of open coding, axial coding, and selective coding to derive first-order concepts, second-order themes, and aggregate dimensions. 49 A random sample of 18 interview texts was coded using Nvivo12, with the remaining texts serving to check for theoretical saturation. The procedural steps are as follows.
a. Open coding: During the line-by-line analysis of the interview text, key sentences or fragments are marked, and labels are assigned to the extracted information to form initial concepts. The coding process has no limitations with regard to existing theoretical frameworks, and efforts are made to derive labels from the data to the greatest extent possible. Ultimately, 20 “first-order concepts” were extracted.
b. Axis coding: The concepts generated by open coding are classified and correlated, and their relationships are explored. Similar concepts were categorized into six second-order themes.
c. Selective coding: To further refine and abstract the second-order themes identified in axis coding, a core category was extracted that encompassed all of the categories.
d. Theoretical saturation: We conducted a coding analysis on the remaining five interview texts, continually comparing, associating, and analyzing them. We found that the categories generated by coding the test data could all be classified into previously coded categories, and no new categories with inconsistent relational structures were identified. Therefore, we believe that the coding results reached theoretical saturation.
Finally, to ensure the rigor and consistency of the coding process, two professors were invited to participate in the final coding stage for checking and reviewing. Discrepancies in coding results were discussed, and those that did not reach a consensus were deleted. In addition, we adhered to the principle of theoretical engagement by comparing the coded results with relevant literature to ensure the reliability and effectiveness of the concepts. 49 Details of the coding process can be found in Appendix C.
Results of qualitative research analysis
By carefully distinguishing use cases on the basis of functional attributes and referencing previous studies, we identified four key affordances of AIMCs that were most frequently mentioned in the case evidence: human–AI interaction affordance (HIA), human-like diagnosis affordance (HDA), health information security affordance (ISA), and personalized treatment affordance (PTA). We define the AIMCs affordances as the system's ability to provide relevant functions or attributes that enable users to engage in behaviors that promote their physical health. 24 Specifically, the HIA refers to the capacity of AIMCs to facilitate a communication platform that enables users to interact with the system through various communication methods at any time or place. 50 This affordance is a second-order structure composed of three components: active control, two-way communication, and synchronicity. Active control represents users’ sensing of their ability to take actions within AIMCs, two-way communication refers to the degree of interaction between users and the AI diagnosis system, and synchronicity reflects users’ perception of the immediacy and efficiency of the AI responses. The HDA refers to the ability of AIMCs to emulate cognitive intelligence and human-like conversational tones, enabling natural, fluent communication with users. Cognitive intelligence enables the system to understand and process natural language, to reason, and to learn, facilitating a comprehensive analysis of user symptoms. 51 A human-like conversational tone involves mimicking human speech patterns, emotional expressions, and social cues, creating the illusion of conversing with a real person. 17 The ISA is a second-order structure composed of identity anonymity and information confidentiality. 33 Identity anonymity refers to users’ perceptions of their personal identities being concealed or unidentifiable, whereas information confidentiality concerns the system's ability to safeguard users’ personal information from misuse or exposure. The PTA demonstrates the AIMCs’ ability to address individual needs and preferences, delivering personalized healthcare solutions effectively. 52
Additionally, we identified two primary user motivations for using AIMCs: assist health decisions (AHD) and relieve health anxiety (RHA). Assist health decision reflects the users’ proactive pursuit of medical knowledge to make informed health decisions, whereas RHA highlights users’ needs for emotional support, seeking emotional stability, and companionship. 53 Our study focused primarily on the general reduction of health anxiety using AIMC tools. These insights form the foundation for the subsequent quantitative phase of the study.
Quantitative research
On the basis of the qualitative analysis results, we propose a research model that integrates affordance theory and psychological empowerment theory, as illustrated in Figure 2. The second phase of the study focused primarily on examining the mechanism through which AIMCs affordances influence users’ perceived cognitive empowerment, emotional empowerment, and usage intentions via quantitative research. According to Liu et al. 17 and Kang et al., 3 individuals’ demographic factors—such as age, sex, experience, education, health status, and health literacy—may affect their attitudes and behaviors. In addition, AI-related knowledge and trust significantly affect usage behavior. 54 To mitigate potential bias, we therefore included control variables such as gender, age, education, experience, health status, health literacy, trust in AI, and understanding of AI.

Research model.
Hypothesis development of quantitative research
The strong interactivity of AI devices is a key factor in overcoming individual decision-making barriers and enhancing the understanding of recommendations.50,55 On the one hand, highly interactive systems can minimize irrelevant information in user queries, reducing information overload.
55
This factor encourages individuals to process information more deeply and to elaborate on the content, thereby enhancing their understanding of the system's recommendations.
56
Specifically, AIMCs use quick feedback and interactive communication to guide patients in detailing their health, optimizing diagnoses, and empowering them to address health issues effectively. On the other hand, interactivity fosters positive emotions such as self-efficacy and trust.
29
Users who feel in control of AIMCs gain confidence and comfort, believing that they can effectively address health issues using the system.
57
Furthermore, AIMCs require users to provide text, voice, or image inputs to obtain the necessary information. On the basis of these insights, we propose the following hypotheses:
From the affordance perspective, a human-like design enhances both the functional and social attributes of AIMCs.58,59 In terms of functional attributes, systems with human-like cognitive abilities are more responsive to user needs and can better inspire a desire among users to interact with such systems.
51
Moreover, a human-like conversational tone reduces users’ sensing unfamiliarity, enabling them to communicate more easily with the system and obtain accurate health information.
17
In addition, compared with purely computational agents, human-like agents create a sense of being treated as a whole person rather than merely a case or dataset. This experience fosters a deeper emotional connection, causing users to feel understood and respected, which enhances their sense of self-worth and motivates them to more actively address health concerns.
58
We posit that the availability of human-like diagnostic capabilities in AIMCs not only assures users of accurate and comprehensible health information but also evokes positive emotions through empathetic responses, causing users to feel understood and supported when health issues are addressed. On the basis of these insights, we propose the following hypotheses:
The personalized affordance of AIMCs is a key feature that differentiates them from traditional information systems. Personalized services enhance users’ perceptions of the relevance of service outcomes, effectively meeting their cognitive needs. In a study on smart, wearable devices, Luo et al.
38
demonstrated that personalized services help users better understand their health conditions with less effort, increasing their likelihood of engaging in healthy behaviors. Similarly, Longoni et al.
10
emphasized that when individual needs are not met, users may doubt the quality of decisions made by AI doctors. However, providing personalized services significantly boosts users’ trust in AI doctors. Hence, when AIMC systems deliver customized information tailored to users’ unique physical conditions, users can easily access the health information they need and develop trust in the system's ability to help them address health concerns. On the basis of these insights, we propose the following hypotheses:
Information security is the underlying AI operation that users are concerned about when using smart devices, and improper handling can lead to users experiencing negative emotions.33,60 On the one hand, identity anonymity and information confidentiality can create a safe and private consultation environment, which can reduce the psychological burden on users and increase their willingness to disclose personal information, which improves consultation efficiency and allows users to obtain more accurate health information. For example, Sin and Munteanu
61
reported that AI doctors can give older adults a greater sense of anonymity than traditional doctors can, which helps such users explore information more freely without fear of being judged. On the other hand, a safe and secretive environment enhances the user's sense of control over the information, leading to a significant increase in trust in the system.
62
When users believe that their personal information is adequately protected, they more actively utilize AIMCs to improve their health. Accordingly, we propose the following hypotheses:
Perceived empowerment refers to granting individuals the ability to accomplish tasks they otherwise cannot accomplish and encouraging greater participation in decision-making and activities. 42 Scholars have increasingly explored the positive impact of perceived empowerment, with various technologies identified as key drivers of this process. For example, Li et al. 27 demonstrated that psychological self-help systems provide users with a sense of control and power, helping them alleviate mental stress. These systems influence users’ cognitive and emotional pathways, empowering them and leading to positive outcomes. Similarly, Li et al. 43 reported that gamified psychological self-help systems evoke positive emotions such as enjoyment, empathy, and trust, enabling users to better manage and control their emotional well-being. In addition, the positive use of technological systems can enhance users’ capabilities and self-efficacy in problem-solving, which is subsequently reflected in their behaviors and activities. For instance, Hsieh et al. 26 reported that user empowerment is a key factor in encouraging active user participation in online brand communities.
In the AIMCs context, the design of system functions positively influences users’ perceived empowerment by enhancing their understanding of health conditions, improving their ability to address health issues, and increasing their confidence in resolving health-related problems. The generation of these positive emotions has a favorable effect on users’ behavioral intentions. Therefore, considering the positive effects of perceived empowerment, users are likely to consider using AIMCs to assist in making health decisions and alleviating their anxiety about health issues when faced with health-related concerns. On this basis, we propose the following hypotheses:
Study instruments for quantitative research
To develop measurement items tailored to the AIMCs context, we adapted a validated scale and refined it on the basis of findings from the qualitative research study. We conceptualized certain variables as second-order formative constructs to more accurately capture their multidimensional nature. Specifically, the HIA is defined as a second-order formative construct consisting of active control, two-way communication, and synchronicity.29,50 Similarly, the human-like diagnostic affordance is modeled as a second-order formative construct, incorporating cognitive intelligence and a human-like conversational tone.17,59 The health ISA is also treated as a second-order formative construct, encompassing identity anonymity and information confidentiality.33,63 All of the other variables are treated as first-order constructs. A 5-point Likert scale was used to measure the conceptualization, resulting in a scale consisting of 42 items. To ensure the content validity of the measurement scales, we conducted a pretest with two management professors and 10 graduate students specializing in information systems. On the basis of their feedback, we revised the scales to enhance content clarity, resolving issues such as ambiguous phrasing and overly complex expressions. The question items and sources for each construct are provided in Appendix D.
Participants for quantitative research
To mitigate potential homogeneity bias in the data sources, we employed a multiplatform data collection strategy. Specifically, we published our questionnaires on China's well-known, professional, third-party online survey platform wjx.cn. We then forwarded the link to WeChat (China's dominant mobile social network) and Douban (a major knowledge-sharing community). These data sources have been extensively validated in the research, and our multiplatform data collection strategy further enhances sample diversity and representativeness.31,47 Given that 71.1% of Chinese netizens have not yet been exposed to online medical services, our sampling strategy was designed to include both experienced AIMCs users and technology-naive potential adopters to ensure representativeness of the population. 64 To ensure the quality of the sample, the participants were asked to answer a “yes” or “no” screening question (“Have you ever used an AIMC system before?”). Users who had not used an AIMC system were asked to watch a 2 min 07 s video of a user's experience with the AIMC system to ensure that the participants had a true understanding of it. The experience video was excerpted from the real experience video posted by the user, and the user's face and voice were blurred to protect the privacy and rights of the video publisher.
A total of 572 people participated in this survey. We eliminated invalid questionnaires on the basis of the following criteria: (1) too short (less than 120 s) or too long (more than 1000 s) time to completion, (2) duplicate IP addresses, and (3) inconsistent logic (used but with 0 usage; not used but not with 0 usage). Finally, 425 valid questionnaires were collected, and the validity rate of the questionnaire was 74.30%.
The 425 sample size is sufficient to support the subsequent structural equation model analysis in this study. The reasons are as follows: First, in the case of the partial least squares structural equation modeling (PLS-SEM) approach, the criterion most widely used to determine the minimum sample size is the “10-fold rule,” according to which the sample size should be at least 10 times the number of observed variables in the model.65,66 Our sample size exceeds the minimum requirement on the basis of this rule. Second, compared with other analytical methods, PLS is more suitable for analyzing small sample sizes, meaning that the analytical method we used does not have high sample size requirements. 66
The demographic analysis of the sample is shown in Table 1. The proportions of men (50.82%) and women (49.18%) were similar, which suggests that the results of the gender analysis are relatively balanced and that gender bias does not play a part in the analysis. Most of the participants were between 20 and 39 years old and had a bachelor's degree or above, which is consistent with the user characteristics of online medical services in China. 64 The majority of the participants had experience using AIMCs (58.59%), indicating that we gained a comprehensive understanding of AIMCs. Several of the mainstream Chinese AIMC systems used by the participants were relatively evenly distributed, with no obvious differences in platform preference.
Demographic characteristics of the sample (N = 425).

Note: This study collected data in mainland China and adhered to relevant regulations. Only AIMCs with proper certification and those meeting app store review requirements are available for users to download. Accordingly, the usage statistics here focus on commonly used apps that meet these standards.
Statistical analysis
We analyzed the data using the PLS-SEM approach with Smart-PLS (V3.2.9), which is suitable for testing higher-order constructs and exploring models with formative factors. 66 Moreover, we employed a noncollaborative two-stage approach using the sequential latent variable scoring method to evaluate the measurement model, which effectively controls for measurement errors in the analysis of higher-order models. 67
Results
Common method bias
As the data in this study were collected on the basis of the respondents’ self-reports via questionnaires, potential common method bias (CMB) may have altered the true correlations between the constructs. We used two methods to control and check the CMB. First, following the suggestion of Podsakoff et al. 68 Harman's single-factor test was conducted to assess CMB. Harman's single-factor test was conducted to assess CMB. The factor analysis revealed 10 factors that collectively explained 59.437% of the total variance. The first factor accounted for only 25.293% of the variance, which was well below the 40% threshold. Second, as recommended by Liang et al. 69 we included a method factor in the PLS model. The substantive variances (R12) of the indicators were significantly larger than their method variances were (R22), with a ratio of R12/R22 = 157.658, as shown in Appendix E. Overall, CMB did not significantly impact this study.
Measurement model analysis
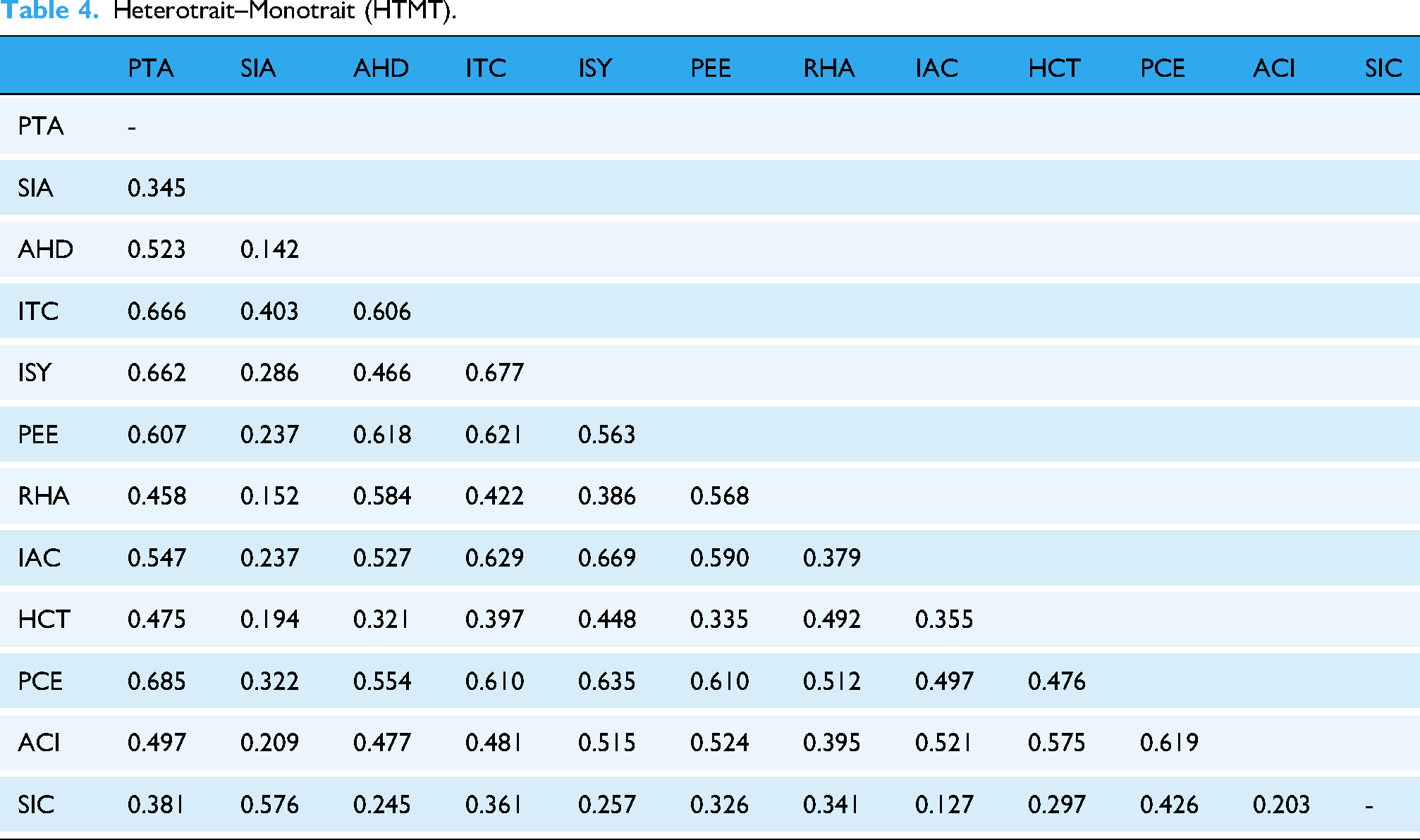
In this process, we tested the reliability, convergent validity, and discriminant validity of all constructs. Cronbach's α and composite reliability (CR) were used to assess internal consistency. Composite reliability values above 0.7, Cronbach's α above 0.6, and average variance extracted (AVE) above 0.5 indicate reliable data. 66 As shown in Table 2, after excluding items with factor loadings below 0.7 (ISY3, ACI2, and AHD3), all CR, Cronbach's α, and AVE values meet the required standards, demonstrating acceptable internal consistency, reliability, and convergent validity. Discriminant validity was assessed using the Fornell–Larcker (Table 3) and the Heterotrait–Monotrait (HTMT) (Table 4). The AVE for each construct should exceed their squared correlations with the other constructs, and the HTMT values should all be less than 0.85, indicating good discriminant validity.70,71
Indicator reliability and convergent validity statistics.

Fornell–Larcker.

Note(s): IAC: active control; ITC: two-way communication; ISY: synchronicity; ACI: cognitive intelligence; HCT: human-like conversational tone; PTA: personalized treatment affordance; SIA: identify anonymity; SIC: information confidentiality; PCE: perceived cognitive empowerment; PEE: perceived emotional empowerment; AHD: assist health decision; RHA: relieve health anxiety.
The bold values refer to the correlation of this correlation matrix.
Heterotrait–Monotrait (HTMT).
We employed the Gaussian copula to test for potential endogeneity issues. The Gaussian copula is considered to be the preferred test for users of PLS-SEM. 72 We conducted both the Kolmogorov–Smirnov test and the Gaussian copula test. 73 The results of the Kolmogorov–Smirnov test indicated that all constructs were non-normally distributed (p < 0.05), which justifies the use of the Gaussian copula approach. 74 The results show that neither of the Gaussian copulas (i.e., PCE and PEE) are significant. Specifically, AHD's two predictor constructs as potentially endogenous yield nonsignificant copulas of PCE (95% CI: −0.144 to 0.719) and PEE (95% CI: −0.371 to 0.345). Similarly, RHA's two predictor constructs as potentially endogenous yield nonsignificant copulas of PCE (95% CI: −0.415 to 0.382) and PEE (95% CI: −0.202 to 0.529). Therefore, these results confirm the robustness of our research findings. 73
Additionally, we examined the role of multicollinearity in the formative constructs. Table 5 shows that the weights of the first-order constructs differ from those of second-order constructs, confirming their distinct roles. All variance inflation factor values are below the threshold of 3.3, suggesting that multicollinearity is not an issue in our study. 75 This finding supports the conceptualization of HIA as a formative structure consisting active control, two-way communication, and synchronicity; HDA as a formative structure of cognitive intelligence and a human-like conversational tone; and health ISA as a formative structure of identity anonymity and information confidentiality.
Formative indicator weights and VIFs.

Note: ***p < 0.001
Hypothesis testing
Bootstrapping with 5000 iterations was implemented to calculate the robust estimators and significance levels. We evaluated the structural model of the study by analyzing the path coefficients along with their associated t-values, as displayed in Figure 3 and Table 6. The model indicated that the R2 value for the assisted health decision was 30.7% and for the RHA was 31.0%, whereas those values for perceived cognitive empowerment were 41.6% and for the perceived cognitive empowerment was 36.7%, indicating a strong explanatory capacity. Specifically, the HIA significantly affected perceived cognitive empowerment (β = 0.239, p < 0.001, 95% CI: 0.131 to 0.341) and perceived emotional empowerment (β = 0.364, p < 0.001, 95% CI: 0.257 to 0.468), supporting H1a and H1b. Human-like diagnosis affordance had a significant effect on perceived cognitive empowerment (β = 0.255, p < 0.001, 95% CI: 0.176 to 0.343) and perceived emotional empowerment (β = 0.152, p < 0.05, 95% CI: 0.053 to 0.262), supporting H2a and H2b. Personalized treatment affordance had a significant effect on perceived cognitive empowerment (β = 0.231, p < 0.001, 95% CI: 0.074 to 0.278) and perceived emotional empowerment (β = 0.178, p < 0.01, 95% CI: 0.105 to 0.305), supporting H3a and H3b. Health ISA significantly influenced perceived cognitive empowerment (H4a: β = 0.136, p < 0.01, 95% CI: 0.068 to 0.205), whereas it did not significantly influence perceived emotional empowerment (H4b: β = 0.072, p > 0.05, 95% CI: −0.010 to 0.150), supporting H4a, but not H4b. Perceived cognitive empowerment significantly influenced willingness to AHD (β = 0.202, p < 0.01, 95% CI: 0.105 to 0.305) and willingness to RHA (β = 0.185, p < 0.001, 95% CI: 0.103 to 0.273) supporting H5a and H5b. Moreover, perceived emotional empowerment had a significant effect on willingness to AHD (β = 0.281, p < 0.001, 95% CI: 0.194 to 0.371) and willingness to RHA (β = 0.294, p < 0.001, 95% CI: 0.202 to 0.388) had a significant effect, supporting H6a and H6b.In addition, we analyzed about the potential impact of the control variables on users’ intention to use intention. The results revealed that understanding of AI positively affected AHD (β = 0.153, p < 0.001, 95% CI: 0.075 to 0.238), trust of AI positively affected diagnosis (β = 0.137, p < 0.05, 95% CI: 0.048 to 0.226), and that the other control variables did not.

Results of the hypothesis testing. Note(s): *p < 0.05; **p < 0.01; ***p < 0.001; (n.s.) represents nonsignificant.
Hypotheses and outcomes.

Post hoc test
During the interview process, individuals exhibited varying attitudes toward AIMCs use to address different types of illnesses. For example, one participant stated, “I am more inclined to use AIMCs for less urgent and milder symptoms, such as diabetes. Since I am already quite knowledgeable about my health condition, I might use it to clarify medication instructions.” Another participant remarked, “When I experience more severe symptoms, such as a sudden high fever, I start to question whether it's the flu or pneumonia. I might only use AIMCs to clarify my symptoms and alleviate my anxiety.” We distinguished between different usage intentions by setting the category wanting to solve specific types of diseases through AIMCs’ to differentiate between the disease types (acute and chronic) that users aimed to address through AIMCs.
We compared and analyzed these two groups using two different methods, the multigroup analysis (MGA) and the permutation test, which are considered the most conservative PLS-SEM techniques for evaluating differences in path coefficients between two groups.76,77 Before conducting the MGA, measurement invariance was assessed using MICOM, which is a necessary condition for comparing and interpreting the group-specific differences in the MGA PLS-SEM results. See Appendix F for the results, which indicate unequal means and variances in both groups, allowing for an MGA. The results of the MGA and permutation test are presented in Table 7. For the PCE→RHA path, Henseler's MGA yielded a p value of 0.023 < 0.05, and the permutation test resulted in a p value of 0.045 < 0.05; both methods confirmed a significant moderating effect of acute and chronic disease tendencies on the relationship between perceived cognitive empowerment and relief from health anxiety.76,77 The acute disease group (β = 0.271) had significantly higher values than the chronic disease group did (β = 0.065).
Results of Henseler's MGA and permutation test.

Note(s): *p < 0.05. PCE: perceived cognitive empowerment; PEE: perceived emotional empowerment; AHD: assist health decision; RHA: relieve health anxiety; HIA: human–AI interaction affordance; HAD: human-like diagnosis affordance; PTA: personalized treatment affordance; ISA: Health Information Security Affordance.
Discussion
Key findings
First, through qualitative interviews, we identified two primary usage intentions for AIMCs and four key affordances, which were confirmed through an SEM analysis. Specifically, we found that users engage with AIMCs to assist in health decisions and RHA. This aligns with Wilson, 53 who reported that individuals seek help from formal or informal health service providers on the basis of their cognitive and emotional needs. The study also identified four main AIMCs affordances: human–AI interaction, human-like diagnosis, health information security, and personalized treatment. Notably, we also captured second-order formative structures for the human–AI interaction, human-like diagnosis, and health ISAs.
Second, regarding the determinants of perceived empowerment, the SEM results show that the four affordances can empower users both cognitively and emotionally. These findings confirm that system functionality design is one of the key factors influencing user empowerment. Specifically, the human-like diagnosis, human–AI interaction, and PTAs similarly impact users’ perceived cognitive empowerment, whereas the health ISA has the weakest effect. Additionally, with the exception of the health ISA, the other three affordances significantly influence perceived emotional empowerment, with the human–computer interaction affordance being the most critical predictor. Overall, compared to the other affordances, the impact of health ISA on users’ empowerment is relatively weaker. This finding is consistent with the research by Nelson et al. 78 on mobile health devices. In addition, we believe that privacy cynicism can help explain why health ISA significantly influences perceived cognitive empowerment but has no significant impact on perceived emotional empowerment. Privacy cynicism suggests that the complexity of the online environment makes it easier for third parties to access personal data, causing individuals to feel powerless and develop distrust toward privacy protection measures. 79 Although people distrust the health information security features provided by internet platforms, studies have shown that this attitude may encourage people to disclose more personal information. 80 Therefore, we believe that this attitude results in a lack of positive feedback on AIMCs’ information security measures, despite the potential of AIMCs to increase the relevance and accuracy of the information that users receive.
Third, both perceived cognitive and emotional empowerment significantly influence users’ two types of usage intentions. The research has suggested that technology's ability to empower users on cognitive and emotional levels can positively influence user behavior, which is consistent with our findings. 27 Notably, the SEM results indicate that, compared with perceived cognitive empowerment, perceived emotional empowerment is more strongly correlated with both usage intentions. User engagement with AIMCs is closely linked to its professionalism and the positive emotions it generates in users, which help address their health issues. A review of the interview data revealed that most respondents indicated that one of the reasons they used AIMCs was that they trusted in its professional capabilities. They suggested that AIMCs are systems specifically developed on the basis of medical data and that their diagnostic accuracy is unquestionable.
Finally, the results of the group analysis of chronic and acute diseases show that the disease type affects the relationship between perceived empowerment and use intention. Specifically, in the pathway of perceived cognitive authorization to RHA, the path coefficient when using AIMCs to solve acute diseases (β = 0.271) is significantly greater than that when used to solve chronic diseases (β = 0.065). This result indicates that users prefer to obtain sufficient health information to alleviate their health anxiety when using AIMCs to address acute diseases. This finding is similar to those of previous studies on disease characteristics. 17 Specifically, patients with acute diseases experience increased uncertainty, which makes the frequency and implementation of online medical services more crucial, although patients often underestimate the effectiveness of these services.81,82
Theoretical contributions
First, this study enriches our understanding of AIMCs user behavior from an affordance perspective. It responds to the call to apply affordance theory to the specific contexts of technology-driven user behavior, particularly in the context of intelligent systems.22,24,29 This research is among the first to establish a conceptual foundation for identifying AIMCs affordances and uses a quantitative analysis to reveal the impact of technological affordances on user intentions. Importantly, we capture the multidimensionality of HIA, human-like diagnostic affordance, and health ISA, contributing to their definition and measurement as formative, second-order constructs. Overall, we expand the AIMCs research and enhance our understanding of user AIMCs behavior.
Second, this study reveals the mechanisms behind individuals’ AIMC use in daily life. It responds to the call to explore users’ intrinsic motivations for proactively engaging with health, self-service platforms.27,43 The application of psychological empowerment theory to the AIMC context better explains the psychological motivations behind individual AIMC use. Furthermore, this research represents an early attempt to apply affordance theory to explore user empowerment. While studies have examined the impact of technological affordances on user beliefs (such as trust and privacy concerns), there has been little empirical validation of the relationship between affordances and user empowerment.22,29 Therefore, this study expands the research on psychological empowerment and provides a novel perspective for the research on intelligent systems.
Third, this study reveals the boundary condition of how empowerment influences usage intention, specifically the moderating role of disease type. The research on health, self-service systems has focused primarily on chronic conditions, 83 overlooking acute disease groups. To address this gap, we introduce disease type to extend the research and use an MGA to examine behavioral differences across different disease contexts. Overall, our study provides a new perspective on the decision-making process underlying AIMCs user adoption.
Finally, a mixed-methods research design combining qualitative and quantitative techniques is used to explore the complexity of users’ decision-making processes in AIMCs adoption. Unlike previous studies that rely on predefined variables and models, the mixed-methods approach provides new insights that are more aligned with the research context. 47 The qualitative phase identifies key user intentions and AIMCs affordances, whereas the quantitative phase validates the discovered concepts and relationships. Thus, this study makes a unique contribution to the AIMCs literature through its systematic approach.
Practical implications
First, our research offers valuable insights into adopting effective AIMCs design principles and developing user-centered products. Developers should prioritize key affordances such as interactivity, human-like diagnoses, personalized treatments, and health information security. Optimizing human‒AI interaction interfaces, improving system responsiveness, and tailoring healthcare plans on the basis of user characteristics (e.g., age, gender, and lifestyle) can significantly improve user experience. In addition, AIMCs should simulate the workflow of real doctors to reduce users’ unfamiliarity with and resistance to artificial intelligence during the consultation process, thereby fostering trust in the system. Privacy protection measures, such as anonymous usage and data deletion options, remain crucial for creating a secure consultation environment, despite being a secondary factor in user preferences.
Second, we believe that emphasizing users’ perceived empowerment is crucial for AIMCs adoption and engagement. System designers should prioritize a user-centered approach, fostering collaboration between users and AIMCs to address health issues. This process includes enhancing system transparency by clearly presenting reasoning and judgments, enabling users to feel informed and in control. Systems that are designed to encourage meaningful user interaction can provide clear and actionable feedback and can adapt to individual preferences. Through these designs, AIMCs can increase users’ motivation to actively participate in their own healthcare management.
Third, system design and marketing strategies should differentiate between chronic and acute disease use cases to better cater to diverse user needs. For chronic disease patients, AIMCs could incorporate features such as periodic reminders for medication, lifestyle adjustments, or routine check-ups, enhancing long-term health management. For acute cases, AIMCs could assist users in promptly contacting medical facilities and providing urgent health alerts to ensure timely treatment. From a marketing perspective, tailored campaigns could highlight different benefits: for chronic conditions, AIMCs’ role in preventive care and supportive treatment should be emphasized, whereas for acute conditions, its capabilities in delivering timely health warnings and emergency coordination should be highlighted.
Finally, governments should implement strong privacy regulations and security guidelines to ensure safer use of AIMCs and increase public trust in privacy. Ethical guidelines should emphasize transparency, ensuring that AI decisions are explainable and that users understand medical recommendations. In addition, the role of AI in clinical decision-making needs to be regulated to ensure essential human oversight in critical diagnoses. By addressing these regulatory and ethical issues, governments can ensure that AI in healthcare is effective, safe, and trustworthy.
Limitations and future research
First, as noted in a previous study by Zhang et al., 84 national culture can significantly influence the adoption of AI tools in health care. Furthermore, differences in healthcare systems, such as variations in data capture and processing, can impact user trust and the willingness to adopt these technologies. 85 Importantly, the sample is limited to a single-country context. This limitation may restrict the generalizability of the findings to other healthcare systems and regions with different cultural and systemic characteristics. Therefore, future research in more diverse geographic and healthcare contexts is essential to validate these findings and assess their broader applicability.
Second, this study used cross-sectional data, which limits the insights into how users’ attitudes toward AIMCs may evolve over time. Future research should adopt a longitudinal approach to track changes in trust, expectations, and reliance at different usage stages. Additionally, exploring how an awareness of system biases and responses to service failures influences user behavior could further improve AIMCs adoption and effectiveness.
Third, while AI systems can enhance healthcare delivery, they also pose risks, such as misdiagnosis and overreliance on automation. Additionally, system features may negatively impact users, as they could experience resistance due to privacy concerns while benefiting from personalized services. 29 Future research should focus on strategies to mitigate these risks and negative effects, such as implementing safeguards, ensuring human oversight, and examining the psychological and behavioral impact on users. This will help ensure that the functionality of AIMCs remains accurate and reliable in clinical settings.
Fourth, while our study did not directly measure the prevalence of illness anxiety disorder (IAD), understanding the relationship between health anxiety, including IAD, and AIMCs use is important. Health anxiety influences people's health information-seeking behaviors, 86 and future research should explore how AIMCs impact individuals with different levels of health anxiety to improve the generalizability of the findings
Finally, through the interviews, we found significant differences between users’ intentions and compliance. Some respondents indicated that despite their willingness to seek health advice through AI consultations, they did not always follow the advice provided by AI. Health information adoption involves transitioning from cognitive awareness to actionable decisions, directly impacting healthcare intervention efficacy. 87 Future research could explore the factors influencing the relationship between user intentions and compliance from various dimensions, such as technology and individual traits.
Conclusions
Rooted in the AIMCs context, this study not only clarifies users’ actual intentions to use AIMCs but also provides a comprehensive exploration of AIMCs affordance and its key dimensions. By applying affordance theory and psychological empowerment theory, this study reveals the crucial role of AIMCs affordance in enhancing users’ sense of empowerment, demonstrating how perceived empowerment significantly influences the users’ intention to use AIMCs. Moreover, the study identifies the moderating effect of disease type on the relationship between perceived empowerment and intention to use, thus expanding our understanding of how different factors impact AIMCs usage.
In terms of practical contributions, the findings offer critical insights into the key elements and behaviors influencing the public's use of AIMCs. These results provide valuable decision support for AIMC system design and marketing strategies, particularly from the perspective of user psychology and behavior. By understanding users’ psychological empowerment and how it interacts with specific disease types, stakeholders can better design AIMCs that cater to user needs and improve adoption rates.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076251350001 - Supplemental material for How the affordance and psychological empowerment promoting AI-based medical consultation usage: A mixed-methods approach
Supplemental material, sj-doc-1-dhj-10.1177_20552076251350001 for How the affordance and psychological empowerment promoting AI-based medical consultation usage: A mixed-methods approach by Song Zhang, Benhao Han and Mengnan Fan in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076251350001 - Supplemental material for How the affordance and psychological empowerment promoting AI-based medical consultation usage: A mixed-methods approach
Supplemental material, sj-doc-2-dhj-10.1177_20552076251350001 for How the affordance and psychological empowerment promoting AI-based medical consultation usage: A mixed-methods approach by Song Zhang, Benhao Han and Mengnan Fan in DIGITAL HEALTH
Supplemental Material
sj-doc-3-dhj-10.1177_20552076251350001 - Supplemental material for How the affordance and psychological empowerment promoting AI-based medical consultation usage: A mixed-methods approach
Supplemental material, sj-doc-3-dhj-10.1177_20552076251350001 for How the affordance and psychological empowerment promoting AI-based medical consultation usage: A mixed-methods approach by Song Zhang, Benhao Han and Mengnan Fan in DIGITAL HEALTH
Footnotes
Acknowledgements
This work was supported by the National Social Science Foundation of China (No. 20AGL007), which funded data collection, analysis, interpretation, and manuscript development. We gratefully acknowledge all participants for their contributions to this study.
Ethical considerations
This study has been performed in accordance with the Declaration of Helsinki. The IRB of Medical College of Qingdao University approved this research (QDU-HEC-2024473). Written informed consent was obtained from respondents who participated in the survey.
Author contributions
SZ: Conceptualization, methodology, resources, validation, and writing—review and editing. BH: Conceptualization, methodology, investigation, formal analysis, and writing—original draft preparation. MF: Investigation, formal analysis, and visualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Social Science Fund of China, (grant number No. 20AGL007).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.
Guarantor
SZ.
Supplemental material
Supplemental material for this article is available online.
Appendix
Results of invariance measurement testing using permutation.

| Constructs | Configurational invariance (step 1) | Configurational invariance (step 2) | Partial measurement invariance | Equal mean assessment (step 3a) | Equal variance assessment (step 3b) | Full measurement invariance | |||
|---|---|---|---|---|---|---|---|---|---|
| Original correlation | 5.00% | Original differences | Confidence interval [2.5%,97.5%] | Original differences | Confidence interval [2.5%,97.5%] | ||||
| PCE | Yes | 0.996 | 0.998 | Yes | −0.296 | [−0.184, 0.202] | 0.381 | [−0.339, 0.330] | No/No |
| PEE | Yes | 1.000 | 0.999 | Yes | −0.301 | [−0.003, −0.191] | 0.600 | [−0.351, 0.351] | No/No |
| HIA | Yes | 0.995 | 0.944 | Yes | −0.226 | [0.001, −0.200] | 0.243 | [−0.360, 0.353] | No/yes |
| HDA | Yes | 0.999 | 0.987 | Yes | −0.309 | [−0.003, −0.189] | 0.202 | [−0.341, 0.367] | No/Yes |
| PTA | Yes | 0.999 | 0.994 | Yes | −0.321 | [−0.175, 0.194] | 0.358 | [−0.431, 0.438] | No/Yes |
| ISA | Yes | 0.966 | 0.966 | Yes | −0.191 | [0.002, −0.188] | 0.307 | [−0.312, 0.313] | No/Yes |
| AHD | Yes | 0.999 | 0.998 | Yes | −0.247 | [0.000, −0.192] | 0.312 | [−0.390,0.401] | No/Yes |
| RHA | Yes | 1.000 | 0.999 | Yes | −0.267 | [0.000, −0.189] | 0.123 | [−0.220, 0.229] | No/Yes |
Note: PCE: perceived cognitive empowerment; PEE: perceived emotional empowerment; AHD: assist health decision; RHA: relieve health anxiety; HIA: Human–AI interaction affordance; HDA: Human-like diagnosis affordance; PTA: personalized treatment affordance; ISA: Health Information Security Affordance.
MICOM test: Step 1: Normally, this is automatically established. Step 2: The original correlation is higher than 5% and the permutation p-value is higher than 0.05. Step 3: (a) Not all confidence intervals of latent variable score mean include the original differences value, so there is not equal means. (b) Not all confidence intervals of latent variable score variances include the original differences value, so there are not equal variances.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.