
Abstract
Background
Artificial intelligence (AI) health applications developed in Global North countries are being diffused to the Global South but not without problems.
Objective
The goal of this integrative scoping review was to identify recent studies from 2022 to 2025 describing the contributions and challenges in using AI health applications in the Global South.
Methods
An integrative scoping review of 24 studies from seven databases identified four themes.
Major Findings
This review adds to previous investigations by 1) focusing on data interoperability to resolve gaps in digitizing global health data required for accurate machine learning, 2) examining formidable economic and infrastructure hurdles for adoption and implementation of health AI in low-resource countries, 3) identifying barriers faced by emerging economies for partnerships with global AI biotech companies in AI health startups, and 4) calling for regulations and global surveillance of AI health applications.
Conclusions
Practical implications for the future use of AI health applications in the Global South are discussed concluding that applications developed and trained on datasets from high income countries need to be recalibrated to work in the Global South. Additionally, due to the health-related disparities within the Global North the adoption of AI needs to be considered in its own context.
Plain language summary
This study reviews the potential of AI healthcare applications in the Global South, where healthcare challenges like poverty, resource shortages, and disease outbreaks are severe. AI offers benefits like improved disease tracking, telemedicine, and predictive models to enhance care access and equity. However, barriers include poor infrastructure, data biases from Global North-centric AI, and limited local expertise. Economic constraints, lack of biotech partnerships, and inadequate regulation further hinder progress. The study indicates need for digitization, equitable collaboration, and global regulations to ensure AI improves healthcare for underserved populations effectively.
Keywords
Introduction
Globally, the healthcare workforce is shrinking while healthcare needs continue to increase and be unmet. 1 In many Global South countries, the state of healthcare is dire with high levels of infant and maternal mortality, crushing poverty and lack of opportunity, inadequate nutrition, severe shortage of resources, lack of access to clean water, and frequent disease outbreak. 2 The rapid integration of artificial intelligence (AI) in healthcare offers a unique opportunity for a substantial change not only in terms of technology but also to reshape the political-social-economic outlook of the globe. To define, AI refers to the simulation of human intelligence in machines that are programed to think and learn like humans. 3 Such machines can perform tasks that typically require human intelligence, such as recognizing speech, making decisions, solving problems, and understanding natural language. Proponents of AI see it as a cost-effective means for optimizing patient care and a path to more equitable distribution of health resources. 4
For example, AI-driven diagnostic tools can perform non-invasive assessments remotely, thereby compensating for the scarcity of experienced medical practitioners and specialized diagnostic facilities. 5 Moreover, AI technologies can be integrated with mobile health and Internet of Medical Things platforms to enhance real-time monitoring and intervention in low-resource settings, thus increasing both the accessibility and efficiency of healthcare delivery. 6 A notable example is National Telemedicine Service launched in India in 2019 by the Ministry of Health and Family Welfare. 7 The system is called eSanjeevani designed to bridge the urban–rural healthcare divide through two modes. The first mode is about facilitating doctor-to-doctor consultations at over 130,000 Health Centers. The second mode comprises eSanjeevaniOPD which is a patient-to-doctor telemedicine system enabling remote outpatient consultation. As of October 2024, eSanjeevani has provided over 299 million consultations, making it the world's largest government-owned telemedicine platform, and has saved over USD 3 billion in out-of-pocket expenses for patients, particularly benefiting rural and underserved populations by reducing travel and infection risks.
Another example of AI for improving healthcare in low- and middle-income countries (LMICs) is Babyl Rwanda which is a digital health platform launched in 2018 in collaboration with the Rwandan Ministry of Health. The program uses machine learning (ML) models to analyze patient symptoms entered via mobile apps or kiosks, prioritizing urgent cases for consultation with remote doctors. It also provides support in multiple languages including Kinyarwanda, English, and French, making healthcare accessible to diverse populations. As of 2023, Babyl Rwanda has facilitated over 2 million consultations, with AI reducing diagnostic turnaround times by up to 40% in rural areas. 8 Even with such positive results, the advantages of AI health applications (e.g. predictive health algorithms, 3D maps of body parts) 9 are both questioned and challenged. Additionally, adoption of AI health applications developed in the Global North contexts can be a double-sided sword for improving the health conditions in Global South countries, which requires prudent evaluation and strategic planning.
The goal of this integrative scoping review is to identify and synthesize the content of recent government, non-government organizations (NGO), public health sources as well as scholarly publications describing advantages and limitations for using AI health applications in the Global South. The Global South refers to countries in Central and South America, the Eastern Mediterranean, Africa, Asia, and Southeast Asia that face inequity in access to healthcare. 10
The Global North–Global South binary may inadvertently obscure many insights about existing disparities in healthcare both within and between these countries. For instance, this has not translated into equitable healthcare outcomes even within the US, a leader in AI development. Studies indicate that AI's adoption in the US's clinical settings is marred by issues of validity, trust, and integration into existing care paradigms. 11 The failure to fully incorporate community perspectives in technology deployment has led to scenarios in which AI applications, despite their technical sophistication, may inadvertently reproduce or exacerbate existing biases. 12 Furthermore, surveys of public perceptions in the US have highlighted skepticisms toward AI in healthcare, especially among communities that have historically experienced discrimination and inadequate care.13,14 Overall, the assumption that advanced AI development in the Global North inherently leads to better healthcare outcomes is flawed. In the US, even as AI technologies evolve, they coexist with enduring disparities that are partly the result of systemic inequities and partly due to a lack of inclusive design and stakeholder engagement. On the other hand, the health disparities and challenges in the Global South are multifactorial and context-specific. This interplay between AI development and deep-seated social inequities highlights the need for a more granular analysis that considers how technological innovation interacts with socio-political determinants of health.
Furthermore, there has been considerable hype around AI for healthcare discussing how AI reconfigures social dynamics, economic resource allocation, and regulatory frameworks.15,16 For example, at the organizational level, AI may lead to a dual response characterized by both high expectations for improved patient outcomes but skepticism among decision-makers. Concerns about issues such as accountability and authority within healthcare institutions show the inherent complexities of AI implementation. 17 The excitement surrounding AI in healthcare is also influencing reorganization of society driven by digital innovation. Research on platform economies indicates that while AI can facilitate innovation, it may also reinforce traditional alliances that shape governance and operational practices. 18 As a consequence, there is a reallocation of risks and benefits among different stakeholders, which indicates a need for re-evaluation of conventional approaches to health governance and public accountability. 16
Additionally, Morley et al., (2020) conducted a mapping review of the ethics of AI in healthcare raising three important concerns. 19 First, AI in healthcare can produce inconclusive, inscrutable, or misguided evidence. This can lead to misdiagnosis or missed diagnosis, affecting trust in healthcare providers and potentially leading to large-scale errors. Second, AI can result in unfair outcomes and transformative effects. It can exacerbate existing inequalities, undermine patient autonomy, and lead to the deskilling of healthcare professionals. Third, the complexity of AI systems makes it difficult to trace the source of errors and assign responsibility. This lack of transparency can hinder accountability and trust in AI systems. In terms of socio-economic shift, AI is reshaping healthcare by coupling, re-coupling, and de-coupling different parts of the system. This transformation is affecting governance, accountability, and the distribution of resources. AI adoption is also raising concerns about the centralization of power and control in the hands of a few tech companies.
Overall, there is a need for a more balanced approach that maximizes the benefits of AI while proactively addressing ethical risks to avoid a loss of public trust. Another important factor is changing demographics, especially an aging population where the labor force is shrinking and the dependency ratio is rising, thereby increasing the demand for efficient healthcare services. 20 The integration of AI tools, when used per ethical and technical principles, can alleviate the burdens on healthcare professionals by automating routine tasks and optimizing resource allocation while maintaining the quality of patient care even during labor shortages.21,22
It is important to differentiate between actual displacement and political exploitation due to AI. Actual displacement refers to the genuine loss of jobs directly attributable to the integration of AI and automation technologies. For example, AI and automation have led to significant job displacement, particularly in sectors involving repetitive and manual tasks. 23 The study shows that AI has reshaped the workforce, leading to the elimination of certain jobs while creating new opportunities elsewhere. On the other hand, political exploitation means using AI as a convenient justification for job cuts that may be driven by other motives, such as cost-cutting or restructuring. This means some organizations may blame AI as the reason for layoffs to deflect criticism and avoid scrutiny. This tactic can obscure the real reasons behind job reductions, which might include financial pressures or strategic shifts unrelated to technological advancements. 24
Many reviews of AI health applications have been previously conducted.25–28 The majority of these reviews have focused on general discussion of AI in healthcare. Even though AI for healthcare has been around since 1970s, the focus has been more on the US and China. 29 (Hussain et al., 2024). The advantages of using AI health applications in these countries has been discussed in numerous articles with less attention directed to how AI can be implemented in low-resource countries. Only a few reviews have considered issues of adoption of health AI in emerging economies.30–32 We propose to extend these earlier reviews by conducting an integrative scoping review of sources from 2022 to early 2025 examining benefits and challenges of using AI health applications in the Global South. We focus on this time period because the creation and adoption of AI health applications have grown rapidly and general public awareness, and the usage of AI to assist personalized health decisions has exponentially increased since 2022. Validation and health outcome studies are largely not yet available. In the case where there is not an existing body of empirical data which can be used to test outcomes of AI health applications, an integrative scoping review is the optimal procedure to evaluate the current state of knowledge about attitudes toward diffusion of AI health applications. 33
Based on the discussion above, this study gathers and interprets representative works describing the advantages and disadvantages of using AI health applications in the Global South guided by two broad research questions.
Method
A scoping review was conducted following the PRISMA-ScR guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) presented in a supplemental material. 34 The scoping review method was employed because of its functionality to map the landscape of an emerging area of study, such as healthcare AI in the Global South in the present study. The integrative scoping review followed five steps articulated in Arksey and O’Malley. 35 These include (1) identifying the study aims, (2) establishing inclusion criteria and selecting sources complying with these criteria, (3) charting the data, (4) collating and summarizing the studies, and (5) reporting results. No ethics approval was required as human subjects were not part of this study. The review was based on several search terms including AI in global health, health AI in the Global South, LMICs, developing countries, emerging economies, and combinations of these search terms.
As in Table 1, several databases were searched including PubMed/Medline, Google Scholar, Scopus, IRIS (WHO Institutional Repository for Information Sharing), Global Index Medicus, SciELO Health (Scientific Electronic Library Online, Latin American, the Caribbean, & South Africa), and LILACS (Latin American and Health Sciences Literature). To be included, sources must 1) focus on discussion of advantages and limitations of use of AI health applications in the Global South, 2) include journal articles and other types of documents such as government, NGO, and organization publications, reports, and conference papers, 3) publish between 2022 to January 2025, and 4) be in English or an English translation. Exclusion criteria included sources which focused on discussion of AI health applications in global health in general, use of AI in specific medical specialties/diseases, (e.g. cardiology or malaria), sources focusing on a specific country, and sources which did not describe use of AI health applications in low-resource settings.
Databases.
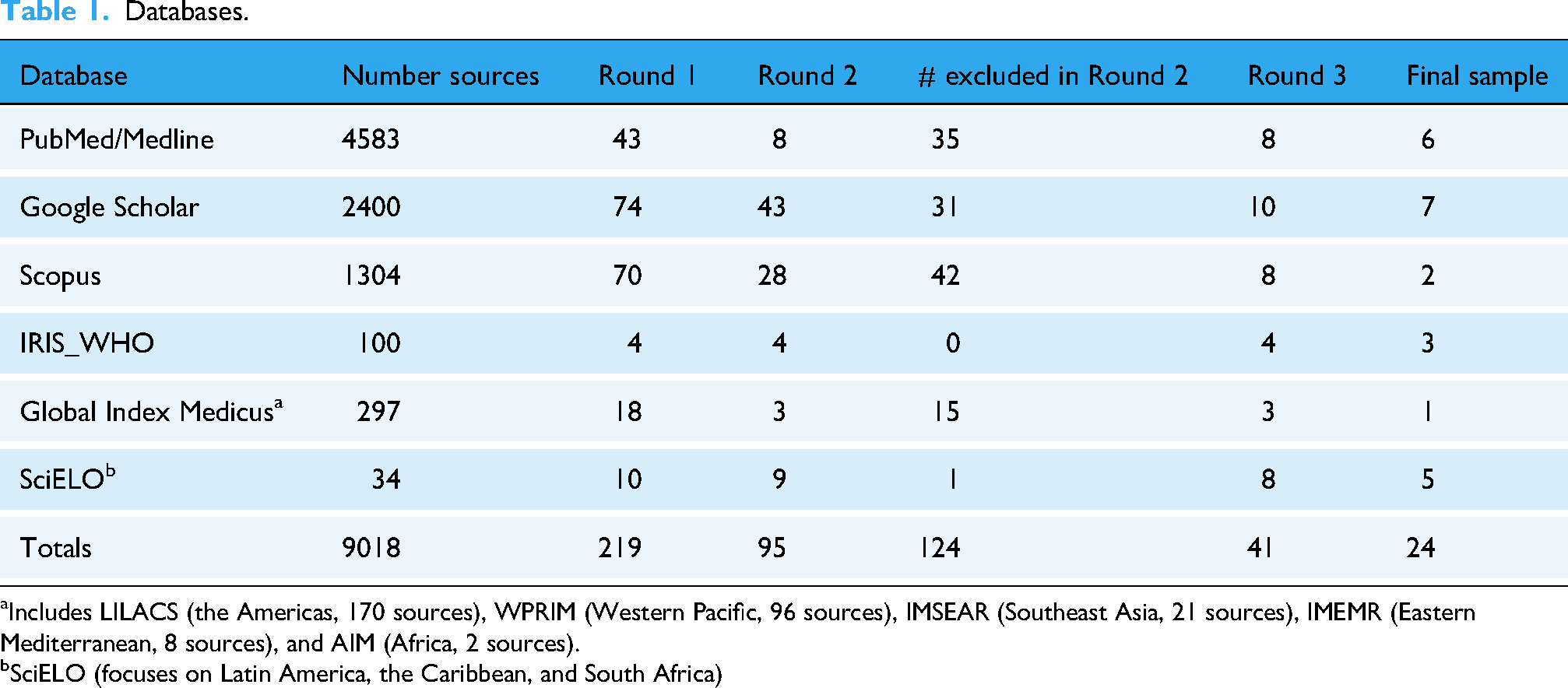
Includes LILACS (the Americas, 170 sources), WPRIM (Western Pacific, 96 sources), IMSEAR (Southeast Asia, 21 sources), IMEMR (Eastern Mediterranean, 8 sources), and AIM (Africa, 2 sources).
SciELO (focuses on Latin America, the Caribbean, and South Africa)
In the first round of review, abstracts for 9018 sources were reviewed to see whether they included any mention of AI in global health. A majority of these sources (n = 8799) primarily focused on use of AI health applications in the United States and were excluded. This left 219 sources for further review mentioning use of AI health applications in global health. Figure 1 shows the PRISMA diagram for source selection.

The PRISMA diagram for source search and selection process.
In Round 2, a second screening of descriptions for compliance with the goal of the study, which was a focus on Global South countries, left 95 potential sources. In Round 3, this was reduced to 41 sources which were then divided among the co-authors for in-depth reading yielding 24 sources ultimately selected for comprehensive analysis. At the last round, the authors screened out articles that only briefly mentioned AI health applications in Global South contexts without detailing advantages, disadvantages, or recommendations. As the co-authors independently read sources, they identified potential themes. The authors agreed on a final set of themes characterizing content of the sources. Table 2 presents a summary of the final group of sources.
Sources for inclusion listed alphabetically by author (2022–2025).

Abbreviations: GS: Google Scholar; PM: PubMed; GIM: Global Index Medicus; SciELO:
*Entries are organized alphabetically based on the first author's last name.
Results
The first research question asked about potential advantages and barriers of diffusion of AI healthcare applications in the Global South. As part of the investigation of this question, four themes describing diffusion/implementation of AI healthcare applications were identified including; 1) importance of digitizing and sharing global health information, 2) advantages and challenges for AI diffusion in low-resourced countries, 3) lack of AI biotech company partnerships with the Global South, and 4) the need for regulation of AI health applications to improve global health. These themes guide presentation of findings from this integrative analysis.
Theme 1: Importance of digitizing and sharing global health information
The first theme focused on data interoperability and approaches for collecting and merging global health data. AI systems require large amounts of data to function properly, and there are issues related to how this data will be collected, stored, and used. This is a particular concern in the Global South, where there is often a lack of diversity of available data which can result in data bias. Healthcare systems in many low-resource countries continue to rely on paper-based data collection and record keeping resulting in decentralized, fragmented analytics such as in infectious disease surveillance. 36
As a first step in addressing global health inequities, developers need to rectify data imbalances between Global North and South countries characterized by language barriers and health literacy affecting the accuracy and completeness of local data. 37 Health data scarcity in low-resource countries also poses a challenge. 38 A major impediment is that current AI health applications have been trained on datasets from high income countries (HICs). As a result, they may perform poorly or lead to the wrong results in the Global South. 39
Digitizing is based on data interoperability and equitable access to data. Data interoperability is defined as formatting data to permit merging and comparison. 40 While many countries in the Global South already use AI software to collect and upload health data, data protection continues to be a major issue for patient privacy, data ownership, and rules regarding how this data can be used. Capacity building investments must be made to incentivize and train front-line community health workers to consistently record and upload health data according to accepted comparable standards.
A number of sources described additional advantages of digitizing health data. For example, AI can be used to analyze data from electronic health records, wearables, and other sources to identify trends and patterns that may be helpful for public health surveillance and research. Furthermore, AI can be used to develop telemedicine applications allowing patients in remote areas to access healthcare services from specialists located elsewhere. Natural language processing systems can translate medical information into different languages to improve communication between healthcare providers and patients which is a major challenge in the Global South. 41 However, these efforts require sustainable economic assistance which is often not available in low-resource countries.
A barrier to digitizing data is the amount of Social Determinants of Health information publicly available between HICs and LMICs. 42 LMICs frequently lack the resources for robust, open-access, patient-level data, while data owned by private sectors may not be publicly available. This is a significant barrier to the development and validation of AI models across diverse populations. Existing efforts to standardize data are either not granular enough for research or are underutilized.
The World Health Organization (WHO) has been instrumental in efforts to digitize health data focusing on three factors: 1) preventing, detecting, and responding to pandemics, 2) developing data-driven infrastructure for health and well-being, and 3) achieving health-related sustainable development goals. 43 A report by WHO (2023a) discussed the importance of data quality and privacy for digital medical records. 44 Another WHO report (2023b) discussed the role of AI/ML technologies in consolidating health data from various sources to protect economically vulnerable families. Interoperability poses challenges between different systems for accuracy, completeness, and representativeness in data management. 45 In summary, these sources described that data availability, data collection, sharing, and security are necessary for adoption and implementation of AI health applications in low-resource regions.
Theme 2. Advantages and barriers for health AI in low-resources countries
Advantages
Proponents of AI health applications argue that big data analytics offer a unique opportunity to address unmet healthcare needs of underserved, vulnerable populations, who often live in areas where healthcare resources are scarce. 46 AI health tools offer transformative potential in identifying and tracking outbreaks of infectious diseases such as malaria, tuberculosis, HIV, cholera, polio, dengue fever, Ebola, and Zika virus. 47 Use of AI health applications has begun to have an impact on all these diseases especially in predicting and preventing outbreaks and in promoting timely, and effective interventions. AI-powered telemedicine can connect patients in remote areas with specialists and improve health outcomes. AI can also address language and cultural barriers, improving access to healthcare for diverse populations. Finally, AI can be used to develop predictive models that can identify patients who are at high risk of developing certain conditions, which can prevent costly hospitalizations. 48
Barriers
AI health applications pose many barriers for low-resource countries. For example, a simulation study using Chat-GPT with patients in LMICs showed that Chat-GPT tended to prescribe unnecessary medication and performed better with non-communicable compared to infectious diseases. 49 Numerous challenges are unique to health environments in the Global South. AI systems require access to reliable internet, electricity, and skilled personnel to develop, deploy, and maintain them. These are not always available in the Global South. Implementing AI health applications imposes additional duties on already burdened front-line community health workers expected to operate these systems. In addition, blind applications of AI in a wide variety of medical and health fields present challenges to patient health data safety. 50 The increasing use of AI in healthcare in the Global South could lead to job displacement for already burdened healthcare workers. 51
The WHO report (2023a) described additional barriers. 44 For example, AI developers may not prioritize adapting their systems for low-resource settings if the market there is less attractive. In addition, AI systems may perform differently in low-resource settings compared to HICs due to differences in disease prevalence, healthcare infrastructure, and other factors. Additionally, challenges like seasonal migration and dynamic enrollment can create hurdles to efficient beneficiary identification. LMICs face infrastructure limitations such as inadequate computing power and internet connectivity which jeopardizes AI/ML implementation. Another barrier is financial constraints as implementing AI/ML technologies requires significant financial investment which may be a challenge for resource-constrained countries. 45 In summary, these sources show that AI health technologies hold the promise for many advantages in extending healthcare to underserved individuals, but on-the-ground problems suggest that meaningful implementation will be difficult.
Theme 3. AI biotech company partnerships with the Global South
The third theme examined sources describing AI biomedical research partnerships between multinational biotech corporations and emerging economies. Currently, the UK, the US, and China dominate the global landscape for AI startups, with minimal Western AI biotech investment in the Global South. 29 AI startups have focused on genetics, drug discovery, chatbot medical assistance, diagnostic, early detection, and clinical decision support. Da Silva (2024) described six challenges faced by emerging economies for nascent health-AI partnerships. 52 The Global South has gaps in STEM education and often experiences medical and biotechnology talent departure causing depletion of the available workforce. Even so, countries like China, India, Taiwan, Vietnam, and Hong Kong have excelled in STEM education and AI development. The second challenge for emerging economies is inconsistent, unreliable government financial support for science research. A third problem is that emerging economies have low competitiveness in attracting global STEM talent. A fourth problem is that existing “collaborations” between multinational corporations and the Global South are often one-way exchanges without sharing technology or benefits. A fifth impediment is that fiscal and political constraints in emerging economies have prevented innovative biomedical research. Finally, Da Silva describes that many emerging economies lack regulative bodies (Theme 4) addressing biotechnological development, research ethics, and the conduct of clinical trials.
Scaling AI health technology in the Global South poses issues of fairness, accountability, transparency, and ethics. The current practice is that western biomedical companies regularly do not consider end-users in marketing deep learning systems. Local stakeholders must be included in the process of building relevant technical solutions. A successful case in point is the Global Initiative on AI for Health (GI-AI4H), launched in July 2023, by the United Nations (UN) using AI to improve global health outcomes. 53 A key aspect of this initiative is the establishment of robust governance structures and ethical standards. These frameworks are essential to guide the ethical and evidence-based adoption of AI in healthcare, ensuring that AI applications are safe, effective, and equitable. Two significant startups from this initiative are Brazil's Laura AI and South Africa's HealthQ projects. Laura AI is an AI-driven healthcare platform designed to enhance patient care by predicting and preventing health crises. It uses ML to analyze patient data, identify potential risks, and alert healthcare providers, thereby improving response times and outcomes. The South Africa's HealthQ initiative uses AI and data analytics to address public health challenges and improves healthcare delivery through predictive analytics, personalized medicine, and efficient resource allocation.
We suggest that AI health development models should not simply be replicated from the West but need to be adapted to low-resource conditions. In addition to governments in the Global South, non-government agencies and private foundations must continue to be willing to make committed investments to support implementation of AI health applications and to develop AI startups. 54 These issues pose barriers to international partnerships and speak to the need to create international ethical and regulatory networks for scientific collaboration as described in the next theme.
Theme 4. The need for regulation of AI health applications to improve global health
The second research question asked about how use of AI healthcare applications potentially contributes to global health. The recent innovation of AI health applications in the digital landscape has ushered in what has been referred to as the Fourth Industrial Revolution. 55 This revolution is felt in every sector of society, especially in healthcare. Advanced AI tools and cloud computing could assist medical personnel on the ground to more accurately diagnose illnesses and treat patients with specialized care even in the remotest areas. For example, an innovative intervention in Nigeria uses drones for delivery of medical tests and supplies to healthcare workers in remote locations. 56 However, such rapid diffusion of AI health applications has been largely unregulated in the Global South.
The WHO has called for global governance of AI health applications based on six principles. 57 First is protecting human autonomy and consent. The second principle is promoting safety and the human interest based on quality control and evaluation. The third concern is the issue of transparency. People must be able to understand explanations of what AI contributes. The fourth principle is accountability. Health providers must use AI responsibly. The fifth undergirding principle is inclusiveness and equity. Favoritism should not be extended to specific groups of people. The final principle is sustainability. Providers must work to continue to develop the positive impacts of AI health applications over time.
Along the same lines, the Lekadir group (2023) developed best practices for technical, clinical, ethical, and legal dimensions for use of AI health applications. 58 Their detailed recommendations were based on an international survey conducted with a large number of computer scientists, healthcare practitioners, ethicists, social scientists, legal experts, and industry professionals working with health AI applications. They recommended community standards be considered in design, development, validation, and deployment of an AI health application. Continuous quality control care and risk assessment must be taken to evaluate the validity of local AI clinical outcomes.
Many other sources have called for governance and surveillance of AI health applications. Ayana and colleagues (2024) argued that to maximize the utility of AI in promoting global health, it is crucial to dismantle Western-centric cognitive frameworks that promote disparities and inequities in AI access. 59 Abbasi (2024) suggested three areas of intervention to improve global regulation of AI health applications: data protection, ethics, safety, and efficacy. 41 Finally, Goodman et al., (2023) emphasized the need for multifaceted governance, involving software developers, their employers, institutions using the systems, professional societies, and potentially even lay oversight. 43 Legislative action is also crucial to enforce testing, evaluation, and adherence to best practices, along with a robust regulatory framework to implement these laws effectively. Active involvement of civil society, patients, and communities is needed for the development and use of AI in healthcare.
Summary
This integrative scoping review identified four areas of concern for diffusion of AI health applications in the Global South including issues with data, barriers to adoption and implementation of health AI, the difficulty of partnership with global AI biotech companies, and the need for surveillance and regulation of health AI. Gathering and managing health data has resulted in problems of data interoperability, identification of health data scarcity and imbalances, issues of data security, problems with data literacy, biased western data being used uncritically for health applications in the Global South, and reluctance of already overtaxed health workers to carefully gather data for AI ML.
The sources included in this review showed that AI health applications have the potential to meet the healthcare needs of underserved populations and to reduce costs. AI health tools can extend healthcare to remote areas without doctors or clinics. Especially in the Global South, AI can identify and track infectious disease outbreaks and assist in health interventions. But there are many hurdles that need to be addressed for health AI to effectively serve intended populations. Many countries in the Global South have been unable to effectively implement AI health applications because of economic uncertainty and infrastructure problems such as rolling brownouts (Rolling brownouts are intentional, temporary reductions in electricity supply to specific areas, initiated by utility companies to prevent a complete power grid failure during times of high demand or limited supply.) and poor internet connectivity. There is the additional problem of potential health worker job displacement from use of AI health applications. Finally, biotech company collaboration and surveillance/regulation of AI health applications are also critical issues. To this point, there have been minimal health AI startups in the Global South. Often western biotech ‘collaboration’ with countries in the Global South is one-sided without sharing technology and benefits. The Global South is hampered by lack of adequate STEM education and technical talent departure. While there is strong consensus that regulation and surveillance of AI health applications is needed, these efforts are just beginning to occur.
Discussion
For the first time in human history, AI health applications carry the potential for achieving global health equity in low-resource countries. Even so, many formidable barriers for diffusion and implementation of health AI remain. The sources in this review provide a realistic portrait of on-the-ground barriers to adoption and implementation of AI health applications in low-resource settings including economic, infrastructure, and surveillance problems. Proponents of AI health applications continue to show optimism that AI health applications could help achieve universal access to healthcare, optimize prediction and spread of pandemics and delivery of vaccines, assist in the development of new drugs, offer Chat-GPT-based health support, contribute to genomic advances in curtailing pathogens, and promote diagnosis and treatment of disease in medically underserved, and marginalized populations.
The future of AI in healthcare in the Global South
Together these sources map out components of a strategic plan for the diffusion, implementation, and surveillance of AI health applications in LMICs. The need to digitize health data is essential for an accurate evaluation of the specific health needs of people whose health experience is not currently included in the development of health algorithms and other applications. This information guides accurate diagnosis and tracking of disease. Interoperability poses a formidable hurdle to digitizing global health data requiring capacity building investments.
A more pressing barrier for adoption of health AI is posed by economic uncertainty, infrastructure breakdowns, and rapid largely unregulated diffusion of health AI. Global North biotech companies are often reluctant to share lucrative AI health applications with low-resource countries and to collaborate with them in AI startups. This has often excluded the Global South from having any input into AI health application development. Using health AI developed for Global North countries and populations is often irrelevant and unworkable when health resources are challenged. While there have been numerous calls for surveillance of AI health applications, global regulation and monitoring has not been achieved.
Since 2020, several Global South countries have developed healthcare interventions using AI. For example, in Jordan, the deployment of AI and big data analytics has transformed healthcare outcomes. Al-Dmour et al., (2025) demonstrate how Jordanian healthcare institutions integrated AI routines to optimize clinical decision-making, improving diagnostic accuracy and operational efficiency. 60 The study showed that enhanced perceived usefulness and ease of integration of AI have resulted in a more resilient healthcare system despite the limitations typical to LMICs. Ethiopia has also demonstrated significant AI transformation in healthcare, with special attention on pediatric care and digital health literacy. For instance, Tadese et al., (2024) reported the successful application of ensemble ML techniques with interpretable outputs such as Shapley additive explanations to predict acute respiratory infections among under-five children. 61 This approach has improved early diagnosis and targeted interventions in a country where healthcare resources are often constrained. Collectively, this shows a dynamic and heterogeneous revolution of AI in improving healthcare in LMICs deploying AI not only as a tool for immediate operational gains but also as a catalyst for broader systemic reform in healthcare.
It is important to briefly discuss the challenges of digitalizing data, specifically, the abuse of data, data accessibility, and political surveillance. In India, there have been instances where personal health information was publicly accessible, raising serious privacy concerns. 62 In terms of data accessibility, the commercialization of healthcare data is a critical issue. Healthcare data is often sold to private entities, making it inaccessible to the general public and researchers. 63 This raises ethical questions about the ownership and use of personal health information. Also, the use of healthcare data for political surveillance is a concern. For example, in India, the Aadhaar biometric system has been scrutinized for its potential misuse in surveillance. 64
Limitations
This review did not examine the difficulty of adoption and implementation of AI health applications in specific low-resource countries. This information could have contributed to understanding of challenges based on lack of resources that specific Global South countries have experienced and what they did to begin to address them. Many countries in the Global South have developed innovative uses of AI health applications to work in their situation. Future investigation might focus on in-depth review of the use of health AI in specific countries. Additionally, this review did not include analysis of use of AI tools for specific diseases in Global South countries, e.g. coronary disease or malaria. Our investigation revealed that there are numerous sources focusing on implementation of AI health applications to meet the needs of specific countries, e.g. South Africa or India and specific diseases. While we provided several examples of how AI health applications have been implemented in specific situations, both of these issues exceeded the scope of the current review. A future study might take a deep-dive into how AI health applications have been used in specific countries.
Conclusion
Twenty-four sources included in this review revealed that while some AI health applications are starting to be used in the Global South, many challenges must be resolved for the benefits of AI health applications to reach people that need them the most. Given economic, infrastructure, resource instability, problems in digital literacy, and talent departure in the Global South, an unresolved question is whether use of AI will result in improving healthcare for clinically underserved, marginalized people in the short and the long term. Nikitenko and colleagues (2025) call for digital humanism using AI health applications to create a humane and just global society. This review shows that we have a long way to go to achieve the goal of equitable universal healthcare supported by AI health applications.
Footnotes
Acknowledgements
We have acknowledged all authors’ contributions in the session above.
Ethical considerations
Ethical approval and consent were not required as there were no human subjects.
Author contributions
Conceptualization was done by SAH and MB; methodology was done by SAH, JZ, and MB; data curation was done by SAH, JZ, and MB; analysis was done by SAH, JZ, and MB; original draft preparation was done by MB; writing—review and editing was done by SAH, MB, and JZ; supervision was done by MB. All of the authors have been involved in this project at every stage and have read and approved of the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.