
Abstract
Objective
This study investigates optimal resource allocation strategies in a multichannel healthcare system that integrates telemedicine and offline services. It compares hospital-led and physician-led decision-making models under varying market coverage conditions.
Methods
A game-theoretical model is developed to analyze how hospitals and autonomous physicians make decisions regarding telemedicine and offline healthcare service provision. The model incorporates factors such as revisit risk, patient copayment ratios, and market coverage. Analytical and numerical methods are used to evaluate patient choice behavior, hospital profit, and social welfare under different decision modes.
Results
In fully covered markets, physician autonomy improves resource flexibility and maximizes social welfare. Conversely, in partially covered markets, centralized hospital decision-making yields better outcomes, particularly under moderate revisit risk and copayment conditions. In high-risk scenarios, a hybrid strategy balancing both models is most effective. Numerical simulations further validate these findings, highlighting key differences in outcomes under varied patient cost-sharing and risk settings.
Conclusion
Decision-making autonomy should be context-dependent. In fully covered healthcare markets, hospitals may benefit from empowering physicians to improve adaptability and efficiency. In contrast, centralized management remains preferable in partially covered markets. A flexible combination of both models offers the best performance under high uncertainty and revisit risk.
Introduction
The development of society has exacerbated the issue of unequal distribution of healthcare resources, making it increasingly severe. Patients in remote areas often struggle to access timely, efficient, and high-quality medical services.1–3 Currently, most specialists are concentrated in urban areas, while rural and remote regions often have few or even no specialists. 4 Consequently, patients in urban areas have much easier access to professional care, whereas many rural patients have to undertake long journeys for medical consultations. In fact, it is not uncommon for patients from rural areas to require four hours of travel time for medical appointments. 5 The advent of telemedicine presents an opportunity to improve healthcare accessibility and promote equity in health outcomes.6,7 Telemedicine allows patients to request remote consultation services from doctors in general hospitals through the use of the Internet and information technology. This service provides patients with flexible and convenient access to professional medical services without the need for travel, thereby reducing the cost of seeking care. The advantages of telemedicine are particularly pronounced for patients in remote regions or those with mobility issues.1,8
Countries such as China, the United States, Canada, and Australia are actively promoting the adoption of telemedicine. The “Digital China Development Report (2022)” indicates that “as of October 2022, more than 2700 remote medical centers had been established nationwide, and over 25.9 million Internet-based medical consultations had been conducted.” 9 However, telemedicine also has its limitations. Current telemedicine technology does not allow physicians to accurately and comprehensively diagnose patients (most doctors can only rely on viewing images and listening to patients’ descriptions on online platforms). This is particularly problematic for complex medical conditions, where patients often need to visit offline hospitals for further diagnosis and treatment. Therefore, in various healthcare settings, telemedicine is implemented through either a gatekeeper system or a dual-channel system. 10 Thus, while the multichannel healthcare model that integrates both online and offline services provides convenience for patients, it also poses challenges to the rational allocation and pricing of healthcare resources. 11
In a multichannel healthcare service model, how hospitals can effectively allocate telemedicine and offline healthcare services and set appropriate pricing has become a crucial issue in healthcare resource management. Traditional resource allocation is typically hospital as the decision-making entity, where the hospital centrally manages resources and can flexibly adjust prices and service capacity across channels based on patient flow and service demand.12,13 Recent research has introduced an alternative decision model—granting decision-making autonomy to doctors. In this model, the hospital sets the price for telemedicine, and doctors allocate resources based on their own income considerations and work preferences.14,15 However, as doctors’ workloads increase, service time and error rates also rise, leading to reduced efficiency and longer service times.16,17 Therefore, doctors, as frontline service providers, play a significant role in determining the allocation between online and offline work. Their choices not only directly affect the service capacity of both telemedicine and offline healthcare but also indirectly influence the hospital's overall performance and patients’ healthcare experiences.
Moreover, the extent of healthcare market coverage significantly impacts the effectiveness of resource allocation. 18 In a fully covered market, patient demand for medical services is relatively stable, and hospitals have sufficient service resources. However, in a partially covered market, the scarcity of resources and uncertainty in demand complicate resource allocation. Due to differences in service capacity, cost-effectiveness, and reimbursement ratios between telemedicine and physical hospitals, the resource allocation models suitable for different market environments may vary.19,20 Therefore, studying the selection of resource allocation models under varying levels of market coverage, and clarifying the relative advantages of hospital-based decision-making versus physician autonomy, is of considerable theoretical and practical importance for optimizing resource allocation, improving hospital management efficiency, and enhancing patient experience.
Based on the aforementioned context, this paper addresses the following research questions: How should the pricing and resource allocation of telemedicine and physical hospitals be managed to maximize social welfare under conditions of full and partial market coverage? How do patients’ healthcare choices and doctors’ service strategies vary under different resource allocation decision models? In particular, what are the differences in the effectiveness of resource allocation between hospital-led decision-making and physician-autonomous decision-making under varying conditions of revisit risk, patient copayment ratios, and differentiated reimbursement policies? To address these questions, this paper develops a resource allocation model for a multichannel healthcare system and examines the impact of different market coverage scenarios, considering hospitals and physicians as independent decision-makers. By setting variables such as revisit risk, copayment ratios, and reimbursement policies, this study systematically explores the impact of the two decision-making models on patient flow, physician income, and overall hospital efficiency, thereby revealing the optimal resource allocation decision model for different market environments.
Research indicates that the degree of market coverage significantly affects the suitability of decision-making models employed by hospitals and physicians. In a fully covered market, the physician-led decision model demonstrates greater flexibility, allowing for the simultaneous maximization of hospital benefits, patient satisfaction, and social welfare. This suggests that, in a diversified demand environment with complete market coverage, granting physicians greater autonomy in decision-making can contribute to optimal resource allocation. Conversely, under conditions of partial market coverage, the hospital-led decision model, due to its systematic management and resource integration advantages, achieves higher social welfare and hospital efficiency when revisitation risk is low to moderate and the out-of-pocket payment ratio is moderate. Through systematic resource management and risk control, hospitals can more effectively meet patient needs within certain boundaries. However, under high revisitation risk and high out-of-pocket costs, the physician-led model proves to be more adaptable, especially in markets with limited coverage. The flexibility of physician decision-making enables more rapid adaptation to market fluctuations in such scenarios.
The remainder of this paper is structured as follows: “Literature review” section reviews the relevant literature. In “Methods” section, we present the primary assumptions and notations used in our model and establish the patient treatment process. “Results” section analyzes the Stackelberg game by determining the equilibrium outcomes under different operational modes, and we also compare these equilibrium outcomes across the various models. “Discussion” section provides a detailed analysis of the preferences of hospitals and patients regarding telemedicine operational models and conducts numerical experiments. Conclusions are presented in “Conclusions” section.
Literature review
This study is related to the literature on healthcare service pricing, medical resource allocation, and patients’ multichannel choices for seeking medical care. First, regarding healthcare service pricing, researchers have focused on competitive healthcare service markets formed by different hospitals.21–23 Due to the fact that the pricing of offline healthcare services involves factors related to patients, health insurance, and other aspects, hospital prices are often the result of a balance among multiple stakeholders, including hospitals, health insurance companies, and the government. The emergence of telemedicine has provided patients with multiple channels for obtaining medical services. The pricing of telemedicine services is often determined by service providers.24,25 In a multichannel healthcare environment, the price differences between offline and online channels become a critical influencing factor, especially under conditions where the reimbursement ratios for health insurance vary significantly. Pricing not only affects patients’ choices but also influences the preferences of physicians and hospitals regarding different consultation channels.1,26 For example, some studies have shown that telemedicine is more attractive to patient groups with high price sensitivity, and due to its limited capacity for comprehensive diagnosis, the upper pricing limit for telemedicine is generally lower than that for offline services.27,28 However, existing literature on hospitals’ pricing decisions for telemedicine has largely ignored the differentiated reimbursement policies for online and offline healthcare services. In contrast, our study employs a differentiated patient copayment coefficient when establishing a patient utility model to depict reimbursement policies for online and offline services, thereby conducting a thorough analysis of the pricing strategy for telemedicine.
The collaboration and competition between different healthcare channels directly impact the efficiency of healthcare service systems. Patient referrals and resource allocation across different channels have become a primary concern for healthcare administrators.1,29 Research on resource allocation in multichannel healthcare models mainly focuses on the efficiency of distributing medical resources across different channels. Rajan et al. 30 analyzed the impact of telemedicine on the market share of offline hospital services and other hospitals in the region, concluding that telemedicine does not lead to a “winner-takes-all” scenario. The study showed that due to technological limitations, patients choosing telemedicine might still need to visit offline hospitals for treatment, indicating that telemedicine can further convert patients to in-person care. In a multichannel environment, resource allocation requires balancing the costs, service capacity, and patient preferences between online and offline channels. Some scholars have explored the optimal decisions regarding telemedicine service levels and hospital capacity by combining game theory and queuing theory. 25 Olanrewaju and Erkoc 31 propose an integer planning model for assigning telemedicine physicians in the emergency care scenario covering multiple hospitals. In previous studies on multichannel healthcare, it was often assumed that the value of hospital services is sufficiently high to achieve full market coverage. In contrast, our focus is on multichannel healthcare under different market structures.
Furthermore, this paper is closely related to the operational models of telemedicine. Existing research generally categorizes telemedicine operations into two types: one where hospitals independently provide telemedicine services and make decisions regarding resource allocation, and another where hospitals collaborate with companies offering telemedicine services to jointly manage operations.18,25 In practice, the former scenario is more prevalent, but the decision-making authority over telemedicine resource allocation varies. Physicians play an indispensable role in the healthcare system. Previous studies have indicated that an increased workload for physicians can lead to longer service times and higher error rates, with excessive workload further extending service time and reducing efficiency.16,17 Similarly, studies by Arora et al. 32 and Landrigan et al. 33 suggest that overly frequent physician shift changes can result in inadequate information transfer, ultimately impacting the quality of patient care. Therefore, some researchers have focused on medical resource allocation from the physician's perspective. For instance, Rajan et al. 14 analyzed how physicians, as decision-makers, allocate telemedicine service capacity from different perspectives. Shen et al. 34 examined the impact of physician decision-making on healthcare costs. However, existing research lacks a comparative analysis of different decision-making models. It remains unclear whether telemedicine resource allocation should be decided autonomously by physicians or centrally coordinated by hospitals.
Methods
This section presents the theoretical framework and assumptions of the multichannel healthcare service system. We employ a game-theoretical approach to model patient choices, hospital resource allocation, and physician autonomy under various market conditions. This study aims to explore effective resource allocation strategies in healthcare systems that integrate telemedicine, using both theoretical modeling and simulation-based analysis. The research was conducted between July 2023 and January 2024 at the School of Management, Zhengzhou University, in collaboration with the First Affiliated Hospital of Zhengzhou University. The modeling framework, equilibrium derivation, and numerical simulations were developed during this period.
In the model, we assume the presence of a comprehensive hospital in the healthcare market that provides both telemedicine and in-person medical services. Patients initially visit a local primary healthcare institution (PHI) for triage. Based on their medical needs, patients can choose to receive treatment through telemedicine from the comprehensive hospital or opt for an in-person visit. However, telemedicine, while convenient, has limitations, especially for complex conditions that require comprehensive diagnosis and physical examinations. In some cases, patients may choose telemedicine for a quick consultation, but if their condition turns out to be more severe than expected, they may need a follow-up visit to a physical hospital. This introduces the risk of follow-up visits, denoted by
The number of patients arriving at the PHI is modeled using a Poisson distribution with a mean
Offline hospitals are assumed to provide medical services valued at
The service capacities of both offline and telemedicine services are modeled with exponential distributions, with parameters
In the case that a patient's initial treatment is unsuccessful, either through telemedicine or in-person consultation, they incur an additional cost f, reflecting the worsening of their condition due to the delay in proper treatment. This cost of deterioration is significant and affects the decision-making process. Patients may weigh this additional cost when choosing between telemedicine and in-person visits, as telemedicine offers convenience but may come at the cost of a less accurate diagnosis. Finally, the equilibrium condition of the model, which reflects the trade-off between the costs of treatment failure, waiting times, and the value of care, is expressed as follows:

This condition suggests that the cost f associated with the deterioration of a patient's condition must be large enough to offset the benefits of choosing telemedicine over waiting for in-person treatment. This equilibrium is critical for understanding how patients make decisions in a healthcare system where both telemedicine and in-person services are available, with each option having its own set of benefits and costs.
Results
This section employs a backward induction method, initially calculating the scale of patients opting for offline medical care and telemedicine services. Subsequently, CH determines the optimal level of service capacity based on its own revenue.
Patient decision-making
The patients who choose telemedicine for their initial consultation, those represented by


From
Among others,
Proposition 1 reveals that under a given telemedicine service capacity, the arrival rate of patients across different channels in the healthcare service system primarily depends on the capacity of offline medical services. There exists a threshold concerning offline medical service capacity. When the offline medical service capacity exceeds this threshold, the total value of medical services obtained by patients who opt for online medical channels is always lower than the combined cost of the fee paid and waiting time. This results in all patients avoiding the online channel, and only a portion of the market chooses to seek care through physical medical channels, while the rest exit the market. Conversely, as offline medical service capacity declines, patients gradually turn to telemedicine. Moreover, when the telemedicine service capacity falls within the intermediate range, the number of patients choosing both channels will exceed the total number of patients within the healthcare system. This indicates that the benefit derived from patients choosing either channel is always greater than zero.
According
Hospital decision-making
In comprehensive hospitals, the primary objective is to maximize the overall hospital benefits. This requires an integrated consideration of the benefits derived from both offline medical services and telemedicine, while accounting for the total cost of service capacity. Therefore, the objective function for comprehensive hospitals can be expressed as follows:



(1) If
(2) If
(3) If
Among others,
Under a given level of offline healthcare service capacity, Proposition 2 presents the hospital's optimal decision regarding the pricing and service capacity of telemedicine. If the offline healthcare capacity is sufficiently high, the hospital can cover all patients in the healthcare system through offline services, and thus, it will refrain from allocating resources to telemedicine. In scenarios where both online and offline healthcare services coexist, the cost associated with follow-up rates in telemedicine becomes a key factor influencing the hospital's decisions. Notably, a lower follow-up rate will prompt the hospital to reduce its investment in telemedicine. This is because, compared to offline services, telemedicine yields insufficient returns for the hospital. Moreover, the follow-up rate reflects the conversion of online patients to offline visits; insufficient conversion rates lead the hospital to place greater emphasis on offline healthcare services.
Corollary 2 explores the impact of the potential patient population on the price and capacity of medical services in cases of full and partial market coverage. In a fully covered market, assuming a fixed service capacity, an increase in the potential patient population leads to a rise in the price of telemedicine services. This relationship reflects that, with the expansion of market demand, hospitals will increase the price of telemedicine services to enhance their overall revenue. When the potential patient population falls within a specific range and the severity of illness is relatively high, the capacity for telemedicine services also increases to meet the demands of more patients, further promoting the overall efficiency of medical services. In the context of a partially covered market, however, an increase in patient flow results in a decrease in both the price and capacity of telemedicine services. This may be due to the insufficiency of market demand to support an increase in service capacity, which instead puts pressure on hospitals to allocate resources effectively. In such circumstances, hospitals may need to reduce telemedicine service capacity to cope with the limitations imposed by patient flow. This dynamic relationship highlights that, in a partially covered market, hospitals must manage resource allocation prudently to avoid a decline in service capacity due to insufficient patient flow.
Doctors’ autonomous decision-making
Under the physician's independent decision-making model, the general hospital determines the price of telemedicine services with the objective of maximizing its own benefits. The objective function of the general hospital remains the same as in equation (4):



Subsequently, physicians allocate their resources to telemedicine based on the benefits they receive from it and their associated opportunity costs. We use the price difference between online and offline services to represent the opportunity cost of engaging in telemedicine, thereby reflecting a physician's sensitivity or preference concerning price disparities. The coefficient s represents the extent to which physicians prioritize these price differences or are attracted to working online. A higher opportunity cost implies that a physician foregoes more potential offline income when opting for telemedicine consultations. Therefore, the utility function for the physician can be defined as follows:

(1) If
(2) If
(3) If
Similar to Proposition 2, Proposition 3 presents the allocation of telemedicine service capacity under physicians’ decision-making. Unlike hospital-level decisions, physicians are more influenced by opportunity costs in addition to the offline service capacity impact. Specifically, the difference in earnings between online and offline services plays a crucial role. When opportunity costs are high, it indicates that physicians must forgo significant potential offline income when opting for telemedicine consultations. Consequently, under comparable conditions, physicians may prefer in-person consultations. By reducing opportunity costs, however, it is possible to enhance physicians’ willingness to engage in telemedicine services.
Corollary 3 analyzes how the interaction between hospital and physician decisions affects the dynamics of service capacity and pricing under full and partial market coverage in the context of physicians autonomously determining their telemedicine service capacity. In a fully covered market, when the scale of potential patients falls within a certain range, particularly when the patient scale is relatively low or the physicians’ price sensitivity is low, the hospital's decisions will incentivize physicians to enhance their telemedicine service capacity. This phenomenon demonstrates that in a fully covered market, hospitals can encourage physicians to optimize service capacity through appropriate pricing, thereby better meeting patient demand. Under partial market coverage, when patient volume falls below a specific threshold and physicians exhibit low price sensitivity, physicians may reduce their telemedicine service capacity. This phenomenon highlights that in a partially covered market, hospitals need to pay more attention to the impact of patient volume on service capacity to ensure rational resource allocation, preventing a decline in service capacity due to insufficient patient demand.
(1) When the hospital achieves full market coverage, if
Proposition 4 compares the telemedicine service capacity and patient choice behavior under the physician autonomous decision model and the hospital decision model. In a fully covered market, when the risk associated with telemedicine falls within a certain range, and both the hospital reimbursement rate and patient volume exceed specific thresholds, the service capacity under the hospital decision model is significantly higher than that under the physician autonomous decision model. This indicates that hospitals can allocate resources more effectively and optimize service processes, thereby improving the overall quality and efficiency of healthcare. In such a context, patients are more inclined to choose telemedicine services, reflecting the positive impact of the hospital decision model on enhancing the appeal of telemedicine. In a partially covered market, when the risk of telemedicine is below a certain threshold, and the hospital reimbursement rate and patient volume meet certain conditions, the hospital decision model similarly enhances service capacity and attracts more patients to choose telemedicine. This demonstrates that in a partially covered market, the hospital decision model is better positioned to respond to patient needs and optimize resource allocation, allowing patients to receive higher-quality telemedicine services.
Proposition 5 investigates the impact of hospital decision-making versus physician autonomous decision-making on offline hospital patients’ choice in both fully covered and partially covered markets, revealing the underlying mechanisms of these two decision models. In a fully covered market, the number of patients choosing offline hospitals increases under the hospital decision model, primarily due to the hospital's comprehensive understanding of patient needs and effective resource allocation. When the hospital sets reasonable reimbursement ratios and service prices within a manageable risk range, it can significantly reduce patients’ healthcare costs and increase their willingness to choose offline hospitals. Furthermore, by optimizing the quality and efficiency of offline medical services, the hospital provides more comprehensive diagnostic and treatment assurances, thereby improving patient satisfaction. In this context, the hospital's overall operational strategy is better able to meet market demands, attract patients back to offline consultations, and foster positive interactions between offline and telemedicine services. In contrast, in a partially covered market, the influence of both hospital and physician decision models on the number of patients at offline hospitals tends to converge. This phenomenon indicates that, regardless of whether the decision is made by the hospital or autonomously by physicians, the service capacity and resource allocation of offline hospitals have become relatively stable, and patient choice largely depends on their own medical needs and preferences. In this scenario, changes in market supply do not significantly affect patient flow, reflecting patients’ autonomy and stability in choosing healthcare channels.
Discussion
Due to the complexity of the model, it is difficult to conduct comparative analyses across different modes using the model itself. Therefore, this paper employs numerical simulations to investigate how parameters such as the price of telemedicine services, the proportion of treatment costs borne by patients, and the probability of telemedicine treatment failure affect equilibrium outcomes under different modes. Based on previous research, the default parameter settings for this paper are as follows:

Scale of patients receiving telemedicine services.
Figure 1 illustrates the impact of varying patient cost-sharing ratios on the scale of telemedicine patients under conditions of complete and partial market coverage. It also compares the performance of hospital-led decision-making versus physician-led decision-making across different levels of revisit risk. In Figure 1(a), under a complete market setting, when the patient cost-sharing ratio is low, the scale of patients under the hospital-led decision model is significantly greater compared to the physician-led decision model. This phenomenon can be attributed to the hospital's ability to make integrated decisions regarding resource allocation and service capacity, which more effectively attracts patients to telemedicine services. Since hospitals can systematically optimize online services to meet the demand of a fully covered market, patient trust and reliance on telemedicine are enhanced. As the patient cost-sharing ratio increases, the difference in patient scale between hospital-led and physician-led models gradually diminishes. In Figure 1(b), under partial market coverage, as the patient cost-sharing ratio increases, the patient scale under the hospital-led decision model shows more significant growth, particularly under conditions of lower revisit risk. This suggests that in a partially covered market, hospital-driven decisions are more conducive to encouraging patients to choose telemedicine. Conversely, the growth in patient numbers under the physician-led decision model is relatively modest, potentially due to the limitations of physicians in resource allocation, making it challenging to respond to fluctuations in market demand, especially under higher revisit risk conditions, where its effectiveness is even more constrained.
In Figure 2(a), as the proportion of out-of-pocket payment ratio value increases in a fully covered market, the overall effectiveness of the hospital decision model significantly improves, especially under conditions of low revisit risk. This improvement is attributed to the hospital's effective coordination of online and offline resources, which not only reduce the referral costs of online channels but also balance the workload of physicians, thereby avoiding overconcentration in any single channel. Furthermore, patients’ preferences for online services further enhance the utilization rate of telemedicine. In contrast, the physician autonomous decision model, due to its excessive focus on individual gains, fails to fully exploit economies of scale, resulting in relatively limited growth in overall effectiveness. As can be seen in Figure 2(b), under partial market coverage, the hospital decision model continues to demonstrate superior performance, particularly in situations where resources are constrained and demand is highly variable. In such scenarios, concentrating resources to ensure the quality of offline services, while maintaining basic coverage for online services, proves advantageous. Although an increase in the out-of-pocket payment ratio value reduces patients’ price sensitivity, high revisit risk makes it challenging for the physician autonomous decision model to allocate resources effectively, leading to suboptimal patient diversion and lower overall effectiveness. Additionally, under autonomous decision-making, physicians need to devote extra effort to service adjustments, further increasing their workload and limiting the model's overall effectiveness.

Impact of the ratio of patients' out-of-pocket payments on the benefits of hospitals.
Figure 3 examines how hospital benefit varies with offline service capacity

Effect of offline service capacity on hospital benefits.
Figure 4(a) shows that under a fully covered market, the out-of-pocket ratio markedly influences patients’ choice of optimal decision models. When this ratio is low, patients are less sensitive to cost and prioritize service quality and convenience. In such cases, hospitals tend to adopt centralized decision models that optimize online service capacity, reduce revisit and referral risks, and alleviate offline workload pressure—ultimately improving service efficiency. In contrast, when the out-of-pocket ratio is high, patients favor cost-effective options. Here, hospital-led models enhance patient utility by optimizing the pricing and quality of telemedicine services. At moderate out-of-pocket levels, the physician-led model offers greater flexibility. Patients weigh both cost and quality, and physicians can dynamically allocate resources between channels to match diverse needs, balance profit distribution, and ease channel-specific burdens. Moreover, higher revisit risks at this level heighten quality concerns, further favoring the physician-led model due to its adaptive and service-matching strengths. Figure 4(b) shows that the impact of patient revisit risk on patient utility dominates under the partial coverage market. The higher risk of repeat visits leads to higher patient utility under hospital decision-making.
Impact of revision risk and patient co-payment rates on patient utility.
Figure 5 illustrates that, under a fully covered market scenario, when revisit risk is low and the out-of-pocket proportion for offline services is high, the hospital decision-making model can maximize social welfare. This indicates that, in situations with lower risk, the hospital's systematic resource allocation and comprehensive management can more effectively coordinate the interests of all stakeholders, including patient convenience, hospital operational efficiency, and physician earnings, thereby maximizing overall social welfare. However, when revisit risk or the out-of-pocket proportion is high, the physician decision-making model tends to show a higher level of social welfare. This may be because, under high-risk or high out-of-pocket conditions, physicians can flexibly adjust their service models based on individual interests and service capacity, thereby better adapting to high-risk environments and improving overall social welfare. In a partially covered market scenario, as the revisit risk increases, the physician decision-making model demonstrates superior social welfare across a wider range, whereas the hospital decision-making model only shows advantages in regions with low revisit risk and moderate-to-high out-of-pocket proportions.

Impact of revision risk and patient co-payment rates on social welfare.
Figure 6 illustrates how social welfare responds to changes in offline service capacity

Impact of waiting costs and offline service capacity on social welfare.
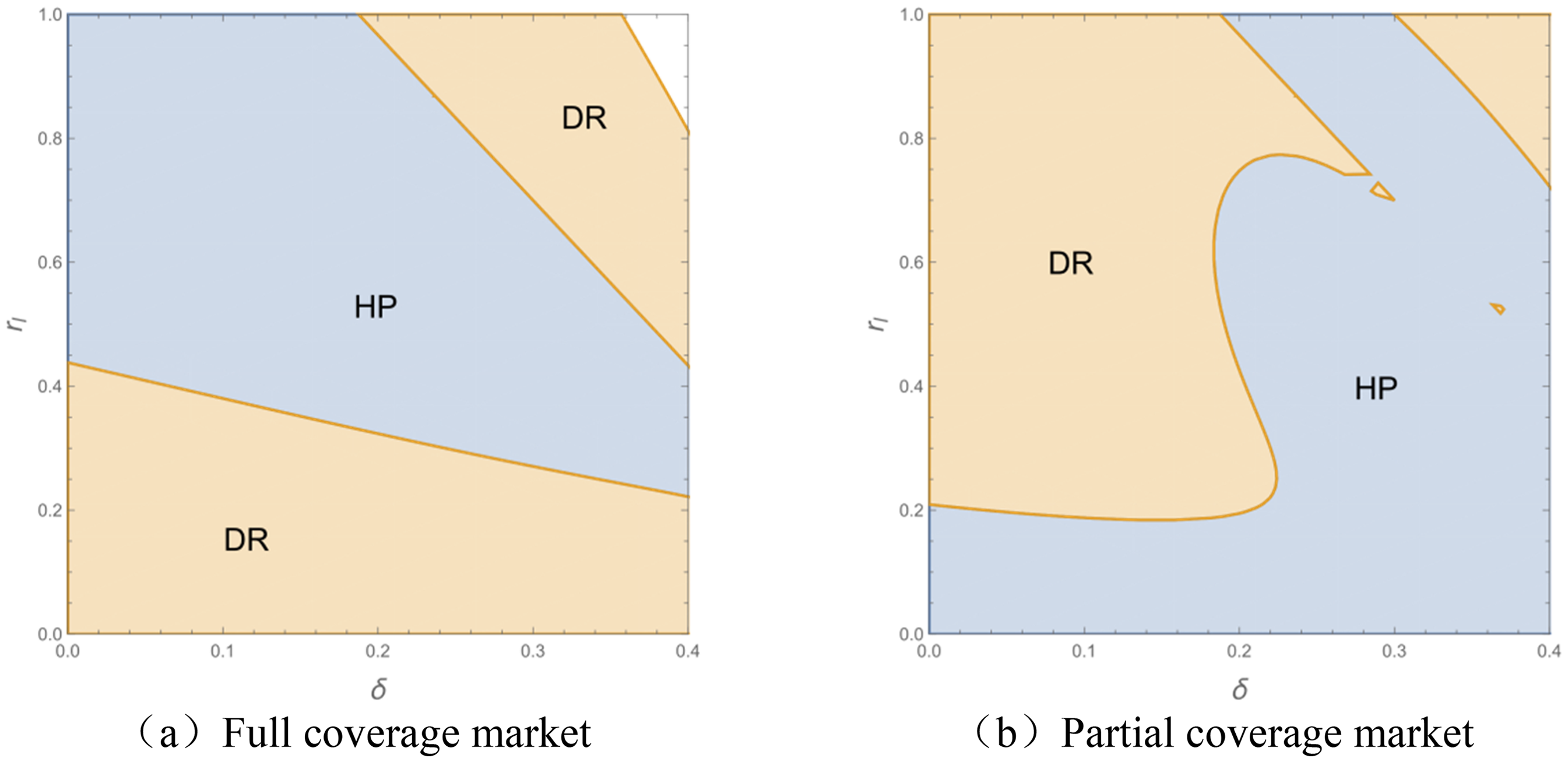
Figure 7 illustrates the overlap between the socially optimal decision model and the hospital benefit-optimal decision model under complete and incomplete market conditions. In a complete market, the hospital decision model achieves dual optimization of social welfare and hospital benefits under high revisit risk. The centralized allocation of resources and the synergy between online and offline services enable the hospital decision model to optimize resource utilization, reduce follow-up and referral costs, and attract more patients to choose online channels, thereby improving patient utility. A relatively high out-of-pocket ratio further enhances hospital revenue. However, when revisit risk increases or the out-of-pocket ratio is low, the physician-autonomous decision model gradually becomes dominant. In an incomplete market, the applicable scope of the hospital decision model is significantly reduced, while the physician-autonomous decision model prevails in regions with high revisit risk and low out-of-pocket ratios. This reflects the flexibility advantage of the physician-autonomous decision model in environments with limited resources and high demand uncertainty. High revisit risk reduces patients’ trust in online channels, while a low out-of-pocket ratio further weakens patients’ price sensitivity regarding channel choice. In such cases, the physician-autonomous decision model more effectively meets patient needs by dynamically adjusting the allocation of resources between online and offline services, while adapting to market fluctuations.

Nash-Equilibrium in the context of hospitals and social welfare.
Conclusions
This study investigates the impact of different decision-making models by hospitals and physicians on resource allocation within a multichannel healthcare system that integrates telemedicine with traditional offline hospitals. By constructing a game-theoretical model, the paper analyzes the effects of hospital-driven decisions versus physician-autonomous decisions on patient utility, hospital profitability, and social welfare under varying conditions of market coverage, revisit risk, and patient self-payment ratios. The study further reveals the relative advantages of each decision-making model.
The study finds that in a fully covered market, under conditions of low revisit risk and high patient cost-sharing ratio, the hospital decision model significantly increases both the scale of telemedicine utilization and the capacity for delivering telemedicine services. By optimizing resource allocation and reducing service costs, the hospital decision model provides telemedicine services at lower prices, thereby enhancing patients’ preference for online medical care. Moreover, patient utility reaches a higher level under the hospital decision model, particularly when telemedicine prices are low and the cost-sharing proportion is high, allowing patients to benefit from cost-effective online services. Social welfare trends align closely with hospital benefits in a fully covered market, and the hospital decision model can maximize social welfare in an environment of sufficient resources and stable demand. The lower revisit risk rates and higher patient cost-sharing ratio in telemedicine lead to greater social welfare under physician-led decision-making compared to the hospital decision model. Additionally, the hospital decision model achieves both optimal social welfare and hospital benefit under conditions of high revisit risk.
Under conditions of an incomplete market, the physician's autonomous decision-making model plays a more significant role in optimizing the scale of offline patient visits, particularly in scenarios characterized by high rates of revisit and low patient copayment ratios. This suggests that the model is well-adapted to meeting diverse patient needs. Furthermore, under the physician's autonomous decision-making model, hospitals are more inclined to adjust service pricing to bridge the revenue gap between online and offline services. However, the effectiveness of pricing strategies is limited by high revisit risks, thereby diminishing the relative advantage of online healthcare pricing. The significant impact of revisit risks and copayment ratios indicates that, in scenarios of high revisit risks, the physician's autonomous decision-making model is better able to meet patients’ demand for high-quality offline healthcare services, thus enhancing patient utility. When telemedicine follow-up rates and patient copayment ratios are high, physician autonomy in decision-making is more conducive to improving social welfare.
The study provides important theoretical guidance and practical insights for hospital administrators and policymakers when selecting resource allocation models. In fully covered markets, it is recommended that administrators gradually delegate decision-making authority to physicians. This can be achieved through incentive mechanisms such as performance-based contracts, flexible scheduling systems, and online service quotas that encourage physicians to take greater initiative in allocating their own service time and capacity. Additionally, hospitals should establish digital monitoring tools to ensure service quality while allowing autonomy. For partially covered markets, a centralized resource allocation approach should be adopted, especially when patient demand is uncertain or revisit risk is moderate to high. Administrators can implement integrated scheduling systems and centralized capacity planning models that balance both online and offline resources. Training and communication protocols should also be reinforced to ensure consistent care quality and responsiveness across departments.
To facilitate smoother transitions between centralized and decentralized models, hybrid governance structures should be actively implemented in practice. This could involve a clear framework for periodically assessing key market conditions—such as coverage rates, revisit rates, patient satisfaction, and financial performance—which will help administrators determine the optimal level of physician autonomy at any given time. These assessments can be supported by data-driven dashboards that provide real-time insights into market changes and patient behaviors, enabling administrators to make informed, timely decisions. Furthermore, establishing cross-functional decision-making teams that include both hospital managers and frontline physicians is crucial. These teams should meet regularly to discuss patient demand patterns, resource allocation, and quality control measures, thus ensuring both operational flexibility and consistent care delivery. In practice, this could include setting specific thresholds for when to shift from a more centralized to a decentralized model, based on real-time data inputs such as patient flow or system stress levels. For example, when revisit rates increase or coverage decreases, it may be necessary to temporarily centralize decision-making to better manage resources. Ultimately, hospitals should adopt a phased, adaptable approach to resource allocation that incorporates both centralized and decentralized strategies, continuously adjusting based on evolving market dynamics, revisit risks, and financial constraints. By integrating continuous data feedback and strategic adaptability, administrators can maintain a balance between efficiency, control, and responsiveness to patient needs.
While this study provides valuable theoretical insights into resource allocation strategies in multichannel healthcare systems, it has certain limitations. The model is based on theoretical assumptions and simulations, without empirical data or real-world validation. As a result, it does not account for patient heterogeneity, real-time decision-making, or dynamic resource adjustments that may arise in actual healthcare settings. These simplifications may limit the model's applicability across diverse clinical contexts. Future empirical studies using hospital-level data could validate the findings, capturing actual patient behavior and resource utilization. Additionally, operational challenges, such as aligning physician incentives and managing fluctuating demand, should be addressed in future research, along with exploring flexible, data-driven decision-making frameworks for transitioning between centralized and decentralized strategies.
Footnotes
Acknowledgement
The authors would like to express their sincere gratitude to Zhengzhou University and The First Affiliated Hospital of Zhengzhou University for their valuable support throughout this study. Their assistance in data access, research coordination, and institutional resources was essential to the successful completion of this work.
Ethical considerations
This study does not involve human participants, animals, or sensitive data; therefore, ethical approval is not required.
Author contributions
DW contributed to the conception and writing of the paper. LY, WL, and YZ provided critical revisions and intellectual input. All authors have reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Postdoctoral Fellowship Program (Grade C), Henan Provincial Science and Technology Research Project, China Postdoctoral Science Foundation, Joint construction project of Henan Medical Science and Technology Research Program, Independent Innovation Program for Graduate Students of Zhengzhou University, (grant number No.GZC20232414, No.242102310140, No.2024M763013, No. LHGJ20240274, No.20250401).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
No data was used for the research described in the article.
Guarantor
DW.