
Abstract
Background
Digital health has the potential to enhance health communication efficiency. However, this potential remains underappreciated among older population due to prevalent technological challenges. The introduction of wearable devices may constitute a positive intervention to alleviate these technological concerns and improve health communication. This study aims to investigate the association between wearable device usage and health tracking data sharing intention among older adults, with digital technology self-efficacy serving as a mediator.
Methods
This study used cross-sectional secondary data from the Health Information National Trends Survey (HINTS 5 Cycle 4), conducted between February and June 2020. The sample included older adults aged 60 or older (n = 1521). Statistically significant relationships among wearable devices, digital technology self-efficacy, and health tracking data sharing intention were examined using SPSS bootstrapping procedures.
Results
The results indicate that wearable device usage, when mediated by digital technology self-efficacy, has both direct and indirect positive effect on health tracking data sharing intention (bp = .742, p < .001; bp = .006, p < .05). In addition, for moderating effect, older adults who perceived social support exhibit a stronger influence on the relationship between digital technology self-efficacy and health tracking sharing (bp = .132, p < .05).
Conclusion
This study provides empirical evidence that wearable devices play an important role in improving digital technology self-efficacy and ultimately contribute to health tracking data sharing among older adults. Understanding these relationships can encourage wearable device adoption and improve health communication and well-being among the older population in the era of digital health.
Keywords
Introduction
Given the increasing aging of the population, 1 the health management of older people become increasingly important. It is shifting towards a patient-professional partnership, with individuals taking more responsibility in daily health decisions. 2 According to Centers for Disease Control and Prevention (CDC), technology has great benefits for daily health management. 3 Statistics shows that while 80% of older adults suffer from chronic diseases, technology-enabled health management can help them establish habits such as regular exercise and a healthy diet. 3 Therefore, in response to the need for health management, wearable devices that monitor one's physiological data and activity have emerged in the market.
A wearable device is a compact technological gadget designed to be worn on different parts of the body (e.g. Fitbit, Apple Watch and Garmin Vivofit). 4 These devices can be used to track and monitor various metrics, such as health indicators, fitness activities, dietary habits, and aging-related data. 4 In recent year, the advancement of the internet, intelligent devices, and big data has driven rapid growth in wearable device technology within the healthcare sector, 5 gradually integrating it into daily life. 6 Academic and industry research has provided enough evidence that electronic wearable devices benefit users’ health management by tracking daily health data such as physical activity, 7 caloric intake, 8 and sleep duration. 9 Previous studies have identified several characteristics of wearable devices, including interactivity, intelligence, durability, ease of operation, and miniaturization, as well as portability. 10 In addition, wearable devices are associated with participatory medicine and personalized healthcare. 11 Wearable device can provide goal-related information and facilitate the adoption of healthy habits.12,13
Current research on wearable devices primarily focuses on technology acceptance,14,15 user experience (UX), 16 and the promotion of mental health (e.g. digital well-being, enhanced self-efficacy)17,18 and health behaviors (e.g. diet and exercise). 7 Furthermore, in studies of wearable devices, data sharing is an important topic, as it serves as a key cue for the health communication process in an increasingly complex health decision-making landscape within the information society.19,20 The benefits of data sharing are widely recognized, including enhanced transparency, cooperation, research replicability, improving health for all through more effective and innovative public health planning.20–22 Previous studies have shown that wearable devices usage is closely intertwined with health tracking data sharing.23,24
While previous literature has yield fruitful findings on wearable devices, there are two research gaps. First, compared to research targeting all age groups, studies specifically focusing on older adults are relatively scarce. 25 The wearable device can be an effective health promotion tool for old people as they offer several advantages. These devices enable continuous monitoring of vital signs such as heart rate, blood pressure, and sleep, which helps detect potential health issues early.7,9 Moreover, wearable devices facilitate data sharing with healthcare providers or family members, improving health management and timely interventions, 26 enabling personalized care, and reducing emergency situations. 26 However, the older population are facing disparities in technology use and digital well-being compared to the younger population, which leads to a sense of psychological alienation. 27 Given this alienation, along with age-related cognitive decline and physical impairments, the older population may experience hesitation and anxiety in embracing digital health technology. 28 Previous research based on the Technology Acceptance Model (TAM) has shown that ease of use can be a solution to promote acceptance among older individuals and enhance their digital technology self-efficacy. 29 For example, when older adults perceive wearable devices as easy to operate and feature user-friendly interfaces, their confidence and self-efficacy in adopting new technology increase, 30 and the adoption of technology facilitates effective interaction for health management.20,24,26 Therefore, more studies are needed to explore how to promote wearable device usage and data sharing among old population.
Second, while the relationship between wearable devices and health data sharing is studied, the psychological mechanisms driven this association remained unknown. According to the concept of “outcome expectation” from social cognitive theory, when a person has a good expectation of a behavior, he or she is more likely to perform the corresponding behavior. 31 Self-efficacy for digital technology is thought to increase intentions for relevant digital health activities, including willingness to share digital health data. 32 In addition, social support is also one of the important influences on health data sharing. 33 Online and offline emotional support and information exchange from family, friends, and social media provide the receiver of data sharing intention and facilitate health data sharing behavior.34,35
To address the research gap, this study aims to: (1) focus on older adults who is facing technological challenges and investigate how the enhancement of wearable device usage impacts health tracking data sharing intention; (2) explore the roles of digital technology self-efficacy and social support on the relationship between wearable health devices usage and health tracking data sharing intention. By revealing the underlying mechanism, we wish to provide practical insights that can guide interventions and tactics designed to foster confidence and overall well-being among older population in the era of digital health. Figure 1 displays the conceptual model of moderated mediation based on this thinking.

The conceptual model of moderated mediation.
Literature review and hypothesis
Self-efficacy is conceptualized as the perception of personal capability in managing environmental demands and applicable to specific tasks.36,37 Technology self-efficacy is defined as a person's confidence in achieving a technology-related task.
38
Older adults’ acceptance and self-efficacy of digital technology is influenced by a variety of factors, including ease of use, utility of features, and strength of social support.
18
Ease of use has been shown to be positively correlated with technology acceptance in previous studies that have used the TAM as a theoretical foundation.
29
Although older adults might face barriers to technology acceptance, research has shown that when devices are simple to use and have user-friendly interfaces, older adults’ confidence in technology using increases, i.e. their sense of efficacy increases.
30
This study therefore considers wearable devices characterized by simple functionality and ease of operation as a positive intervention to enhance older adults’ digital health technology self-efficacy. In addition, the establishment of self-efficacy is associated with the mechanism of goal setting, outcome expectations, and outcome incentives,
37
and older adults’ technology self-efficacy increases when they achieve health goals through the use of technology.
39
Previous research indicates that wearable devices play an important role on “active ageing” and health well-being among older population.
16
Wearable devices have the potential to create an supportive environment that enhances functionality and facilitate the engagement of older adults in digital health.
16
For example, multiple studies have demonstrated that wearable devices can set incentive programs and monitor data, thereby promoting health management behaviors such as physical activity, sleep, and nutrition.7–9 When individuals recognize their ability to manage their health through technology, their technological self-efficacy increases.
39
Previous study has indicated that wearable devices hold promise in effectively tracking and improving the health and well-being of older adults through technology, thereby enhancing their technology self-efficacy.30,40 Thus, this study posits the first hypotheses:
H1. Among older adults, wearable device usage is positively associated with digital technology self-efficacy. (Positive a path)
While health tracking data sharing intention is influenced by various factors, including data security, privacy protection, health literacy, and social support,41,42 technology self-efficacy is a crucial predictor.26,43 Previous studies have found significant associations between technology self-efficacy and older adults’ willingness to share health data with healthcare providers.
40
Moreover, research indicates that higher technology confidence among older adults is an integral component of health management competence.
44
Improvements in health management competence contribute to motivating-related health management behaviors,45,46 such as sharing and communicating health tracking data with doctors or family members.
40
Thus, this study posits the second and third hypotheses:
H2. Digital technology self-efficacy is positively associated with health tracking data sharing intention. (Positive b path) H3. Wearable device usage is positively associated with health tracking data sharing intention mediated through digital technology self-efficacy. (Positive a*b path)
Previous studies have shown that the frequency of electronic media use and willingness to share electronic information are positively related.
47
Electronic networks are becoming reliable platforms for information sharing with target audiences due to their wide user base and the rapid spread.
47
In addition, previous research indicates that as part of digital health technology, the simple functionality and ease operation of wearable devices motivates older adults to communicate and share digital health data.
16
Health data sharing intention has the potential to help older population get social support48,49 and improve their self-management of multiple long-term health conditions.
50
This positive feedback on health outcomes will correspondingly increase their willingness to share health information.
49
In addition, in order to mitigate the impediment of privacy anxiety to the health data sharing intention, previous research has examined relevant policies such as Health Insurance Portability and Accountability Act (HIPAA) to make recommendations for data protection and sharing promotion of wearable devices.
23
This study predicts that the frequency of use of wearable devices is closely related to willingness to share data from wearable devices,
40
leading to the hypothesis:
H4. Wearable device usage has direct positive association with health tracking data sharing intention. (Positive d path)
Previous research has demonstrated that online and offline social support from family and friends plays a role in motivating individuals’ health communication and management, while support involves discussing health topics, daily medication reminders, and health decision-making.
51
Social support can be categorized into emotional support and informational support.52,53 Older adults with less social support may feel health communication withdrawal due to a lack of recipients of health information exchange.51,54,55 Previous research suggests that differences between older adults with less and more social support suggest a potential moderating effect of social support, and that technological assertiveness may be more pronounced in older adults with more social support.56,57 In addition, a moderating effect of social support was found in empirical studies.58,59 Accordingly, this study puts forward the fifth hypothesis:
H5. Social support positively moderates the relationship between digital technology self-efficacy and health tracking data sharing intention, such that higher levels of social support are associated with a weaker positive relationship between digital technology self-efficacy and health tracking data sharing intention.
Method
Data sources
This cross-sectional study uses publicly available secondary data derived from the Health Information National Trends Survey (HINTS 5 Cycle 4), collected between February 2020 and June 2020. HINTS, developed by the U.S. National Cancer Institute, collects national data on American adults’ access to health information, behaviors, and outcomes. The HINTS 5 Cycle 4 dataset is publicly accessible and does not require additional permission for use. In this study, the data are anonymized and de-identified, ensuring compliance with ethical standards. Ethics approval for this study was granted by the Westat IRB on March 28, 2016 (Project #6048.14). Additionally, HINTS 5 received a “Not Human Subjects Research” determination from the NIH Office of Human Subjects Research on April 25, 2016 (Exempt #13204). The sample consisted of 3865 respondents, and only respondents aged 60 or above were involved in this study (n = 1521). The study focuses on how older adults can benefit from wearable devices. Therefore, the sample was restricted to this age group. This age criterion aligns with previous literature, which defines older adults as those aged 60 and above. 60 The proportion of missing values is 3.5%, with the missing data resulting from refused answer and non-ascertainment. We handled the missing values in this model using the listwise deletion method. See supplementary document for STROBE checklist of this study.
Variables and measurements
Health tracking data sharing intention was measured by three items divided by different types of recipients of data sharing, adapted from surveys using the same HINTS data.61,62 Responders were asked to report: “Would you be willing to share health data from your wearable device with.” (1) Your health care provider. (2) Your family. (3) Your friend. (0 = no, 1 = yes; M = 0.91, SD = 0.40).
Wearable device usage was assessed using two items adapted from surveys using the same HINTS data that measured the frequency of wearable device use.26,63 Responders were asked: (1) “In the last 12 months, have you used an electronic wearable device to monitor or track your health or activity? For example, a Fitbit, Apple Watch, or Garmin Vivofit.” (0 = no, 1 = yes). (2) “In the past month, how often did you use a wearable device to track your health?” (1 = do not use to 5 = every day; M = 1.58, SD = 0.69).
Digital technology self-efficacy among older population was measured by four items that pertained to older adults’ use of technology for health-related purposes, drawn from surveys of the older population using the same HINTS data.40,64 Participants were asked: “In the past 12 months, have you used electronic means to do any of” (1) “Looked for health or medical information for yourself.” (2) “Used e-mail or the Internet to communicate with a doctor or a doctor's office.” (3) “Looked up medical test results.” (4) “Made appointments with a health care provider.” (0 = no, 1 = yes; M = 1.52, SD = 0.37).
Social support was operationalized with two items, adapted from prior social support research in public health.65,66 Social support is conceptualized as support an individual receives through social connections with other groups of individuals and the larger community. 67 Accordingly, we set this variable as online social support and offline social support based on the source of social support.66,67 For online social support measurement, responders were asked whether they “participate in an online forum or support group for people with a similar health or medical issue.” For offline social support measurement, responders were asked whether they “have friends or family members that they talk to about their health.” (0 = no, 1 = yes; M = 0.45, SD = 0.25)
Sociodemographic variables were included to minimize confounding effects, comprising age (ranging from 60 to 104), birth gender (male and female), and education level (1 = less than 8 years to 7 = postgraduate).68,69 To better control for the potential impacts that could influence both wearable adoption and data sharing, several related variables were included in the analysis. Health status is considered a factor influencing the adoption of wearable devices and data sharing 18 and was controlled for in the analysis. The health status variable measured whether participants had conditions such as diabetes, hypertension, heart condition, and pulmonary diseases (1 = “yes,” 0 = “no”; M = 1.68, SD = 0.26). Additionally, patient-centered communication, which is known to influence health data exchange, 70 was also controlled for in the analysis. Patient-centered communication was measured using a validated questionnaire.71,72 Respondents shared their patient-centered communication experiences with healthcare providers over the past year, based on seven key aspects that align with the NCI Monograph and recommended evaluation methods.71,72 Respondents rated seven items assessing the perceived frequency of patient-centered communication on a four-point Likert scale (ranging from 1 = “Never” to 4 = “Always”; M = 3.26, SD = 0.91).
Statistical methods
All analyses were performed using SPSS 28. First, descriptive analyses were conducted for each variable. Second, the SPSS PROCESS macro was employed to examine the proposed mediation and moderation effects. 73 Moreover, to interpret the mediation effect, a min–max normalization was applied to rescale all variables to 0–1 range. 74 Following statisticians’ suggestions, we referred to the regression coefficients of the variables calculated on the 0–1 scale as percentage coefficients (bp),75,76 where a higher bp indicates greater efficiency. This approach enables direct comparison of coefficient values and facilitates comparisons of effect sizes. 77 The validity of this scale transformation has been supported by Cohen 78 and has been used in health studies.77,79–81 In addition, our study uses bootstrapping to measure the mediation effect because it is widely applied in mediation research and has been validated by numerous empirical studies.73,82 Bootstrapping is commonly used in mediation analysis with HINTS data. 83 In this study, we used 95% confidence intervals (CIs) to estimate the effects of all variables, employing bootstrapping with 5000 samples.
Results
A total of 1852 respondents aged 60 and above were involved in this study. Table 1 presents the descriptive characteristics of the sample in both natural scales and the 0–1 scales. The statistics indicate that the average age of the respondents was approximately 71 years and 58.6% of respondents received college or above education. Besides, 55.5% respondents are female and 44.1% are male. This study examined the bivariate correlations between the primary variables, as presented in Table 2, emphasizing the significant correlation observed among these variables.
Descriptive statistics of the independent, dependent, mediating, moderating, and controlling variables (n = 1521).
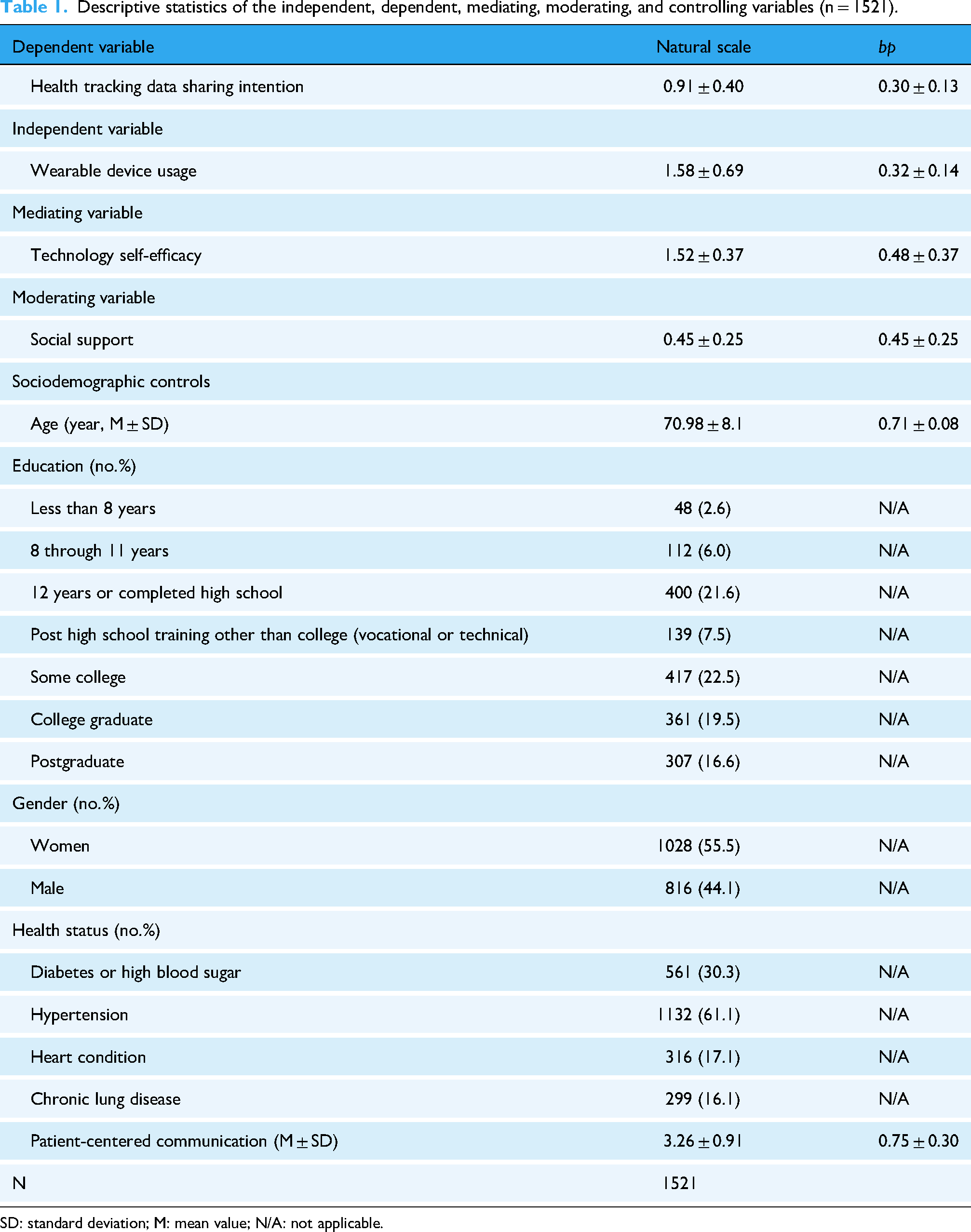
SD: standard deviation; M: mean value; N/A: not applicable.
Zero-order Pearson correlations (n = 1521).
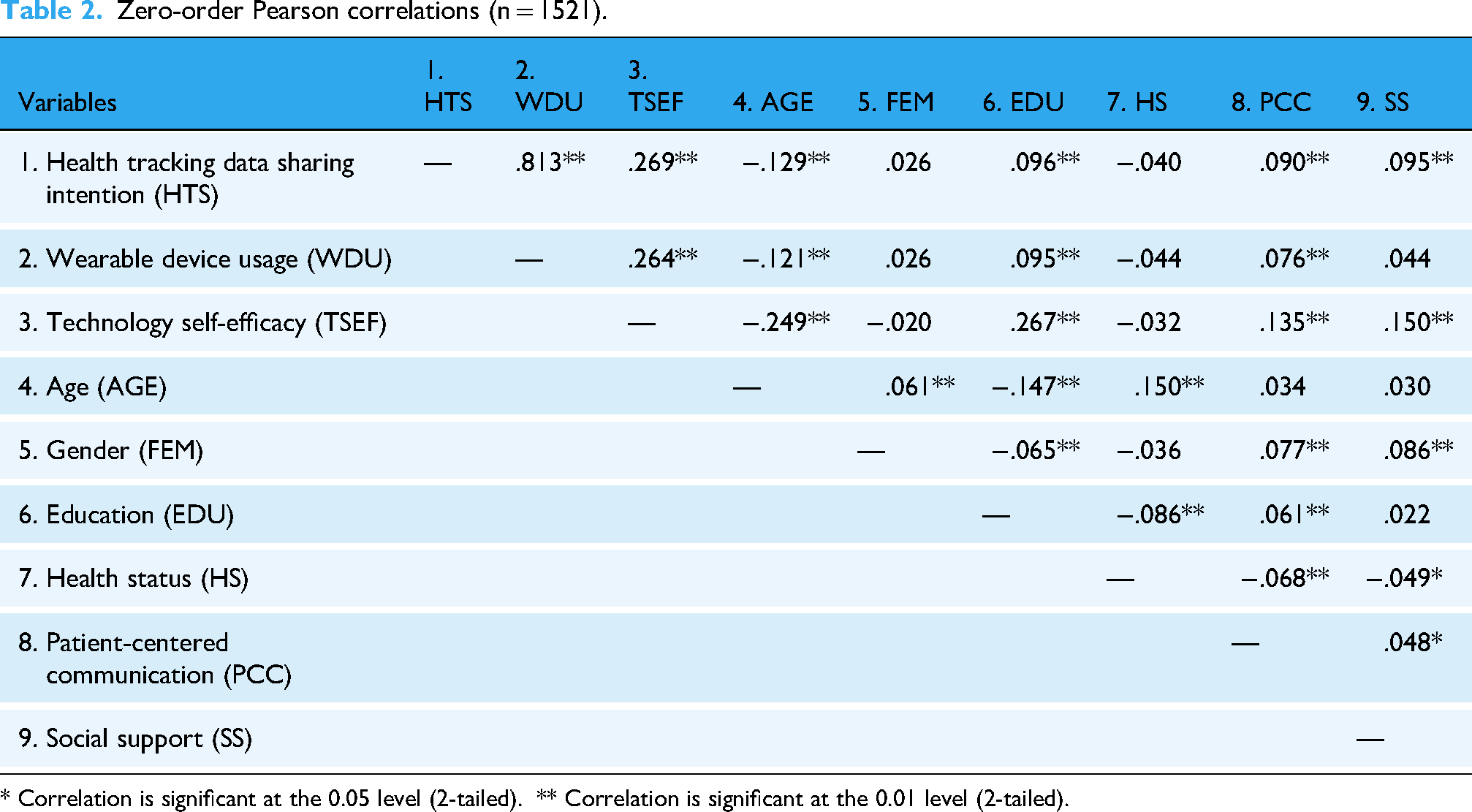
* Correlation is significant at the 0.05 level (2-tailed). ** Correlation is significant at the 0.01 level (2-tailed).
As seen in Figure 2,

Effect of WDU on HTS mediated by TSEF and moderated by SS (n = 1, 521).
Regressions testing technology self-efficacy as mediators in the relationship between wearable device usage and health tracking data sharing intention.

CI: confidence interval.

Moderating effect of social support on the association between technology self-efficacy and health tracking data sharing intention (b path).
Discussion
Contextualized in the digital health environment, this study examines the underlying mechanism of relationship between wearable device usage and health tracking data sharing, uncovering mediator of digital technology self-efficacy, extending previous literature.23,24 These findings further elucidate the benefits of older adults’ adoption of wearable devices, particularly in increasing their sharing of health data, improve health communication with others, and enhancing well-being in this digital health society. The subsequent section delves into a comprehensive discussion of the research findings.
Echoing to prior literature, wearable device usage has direct positive association with health tracking data sharing intention. 24 In addition, the hypothesized mediation effects of technology self-efficacy in the relationship between wearable device usage and health tracking data sharing intention were supported.16,40 Older adults’ engaging in wearable device can improve technology self-efficacy, which subsequently facilitate health tracking data sharing intention.47,50 The findings indicate that technological self-efficacy plays a crucial role in shaping older adults’ technology-related behaviors. Technological self-efficacy can be influenced by various factors, including social support, digital literacy, and privacy concerns. 18 For example, higher digital literacy enables older adults to navigate digital tools more effectively, reducing frustration and increasing their willingness to adopt technology. 84 Interventions that mitigate privacy concerns may also enhance older adults’ confidence in adopting new technologies by alleviating fears about data security. 85 In addition, research has shown that ease of use is positively correlated with technology self-efficacy. 29 When devices are simple to operate and feature user-friendly interfaces, older adults are more willing to engage with them, which in turn enhances their sense of technology competence. 30 Wearable devices, characterized by their simplicity and ease of use, serve as an effective intervention to improve older adults’ technology self-efficacy in digital health management. Furthermore, previous studies have shown that incentive strategies 86 and personalized plans 87 can enhance older adults’ confidence in using digital technology. Incentive mechanisms and long-term management plans in wearable device usage help people to monitor their health data which trigger healthy habit like physical exercise, 88 regular routine and balanced diet, 3 thereby improve their health management. 89 The establishment of self-efficacy is associated with the mechanism of goal setting, outcome expectations and outcome incentives, 37 and older adults’ technology self-efficacy increases when they achieve health goals through the use of technology. 39
Secondly, the positive association between technology self-efficacy and health information sharing intention aligns with previous literature.32,65–67 According to the definition of self-efficacy in Social cognitive theory, self-efficacy influences an individual's motivation. 31 When a person perceives themselves as capable of accomplishing a task, their motivation to repeat the behavior becomes stronger. 31 The digital technology self-efficacy increases the digital health management behavior, 46 including health tracking data sharing intention which trigger appropriate health communication and be helpful for health promotion of older adults. In addition, according to the percentage coefficient (bp) method we use, result shows that the mediation effect of self-efficacy is smaller than the direct effect of wearable use itself. This finding indicates that within the existing digital health ecosystem, the mediation effect of digital technology self-efficacy on relationship between wearable devices usage and health information sharing remains underdeveloped. The observed strong direct effect suggests that individuals’ decision to share health information via wearable devices may not necessarily result from an increased self-efficacy in digital technologies for health-related purposes. Instead, other motives, such as entertainment and social interaction, might also play a role. 90 For instance, some individuals use these devices to compare their exercise levels within social networks. A study on the health data sharing behaviors of Chinese WeChat users revealed that social interaction, acting both as social capital and gratification factor directly and indirectly generated positive effects on health data sharing intention. 90 However, our mediation model primarily focuses on information sharing driven by health communication objectives. Future research could consider exploring the mediation of health data sharing for social or entertainment purposes.
Thirdly, findings indicated that there is positive moderation effect of social support on the effect of digital technology self-efficacy on health tracking data sharing intention. Prior research has shown that social support can enhance health management self-efficacy of older population, including health technology using, health information exchange and sharing.33,40,91 And this kind of information exchange and interaction have both informational support and emotional company. 53 The moderation effect of social support shows that the transmission and reception of health data and information is influenced by the receiver, 92 and when the older population is surrounded by more social support from family and friends, increased technology self-efficacy is more likely to facilitate their health information sharing and improve their health communication. Conversely, it is less effective. This validates the helpfulness of online and offline social support for health communication and promotion among older population. 93
Practical implication and limitation
This study has practical implications for ageing and digital health research, encouraging the learning and use of wearable devices can help older people to better benefit from the development of digital health society. From the results, wearable devices can directly or indirectly enhance their health information exchange and communication. Digital technology self-efficacy is important for health data sharing and communication. This study also finds that social support moderates the link between digital technology self-efficacy and health data sharing intentions. This highlights the crucial role of community, family, and friends in helping older adults adopt and engage with digital health technology and actively communicate with it. However, the adoption of wearable device can be influenced by the cost, usefulness, and privacy. Research indicates that the financial burden and the need for user-friendly pose significant barriers to widespread adoption, while apprehensions regarding data security further diminish consumer confidence. 94 Moreover, the misalignment between technology design and the unique needs of older adults exacerbates reluctance to integrate these devices into daily health management practices. 18 To this end, the wearable device industry can design features tailored to the older population, such as psychological care and medication taking reminder, 95 as well as novel wearable applications such as fall detection 96 and cognitive training, 97 to motivate their use and enhance self-efficacy. Additionally, user interface and UX design should prioritize simplicity, larger fonts, and voice commands to improve accessibility and ease of use, making the devices more intuitive for the older population. 98 Family and friends need to give more support to help older people understand the functions and maximize the effectiveness of these devices, and engaging in health data communication for both information and companionship. 99 Community health workers can strengthen publicity, experiential and education activities on wearable devices for the older population to promote health sharing and help them better integrate into the digital health society. 100 Healthcare professionals should provide authoritative and patient-centered training, support, and digital health knowledge popularization, addressing older adults’ concerns and enhancing their self-efficacy. 101 Policymakers should establish and enforce regulations to safeguard user privacy and data security, with particular emphasis on protecting older adults from health information fraud. 23
Several limitations of this study warrant consideration. First, the cross-sectional design of data limited a more accurate understanding of the causal relationships between wearables use, technology self-efficacy and health tracking data sharing intention, panel research and experimental research are essential. Secondly, this study regards technology self-efficacy as mediator in the relationship between wearable device usage and health tracking data sharing intention, possibly ignore other relevant mediating variables. Future research should endeavor to bridge this research gap by surveying factors such as functional adaptability of wearable devices to the older population, connectivity of wearable devices, and other electronic information sharing devices, as well as digital literacy and privacy concern. Thirdly, because of the limitations of the questions covered by the HINTS questionnaire, more relevant in-depth interviews are needed.
Conclusion
This study provides empirical evidence that wearable devices play an important role in improving digital technology self-efficacy and ultimately contributing to increased health tracking data sharing intention among older adults. Understanding these relationships can help promote the adoption of wearable device and improve health communication and well-being among older population in an increasingly digital health age.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076251337948 - Supplemental material for Willing or reluctant to share health data? A moderated mediation analysis of wearable device usage and data-sharing intentions among older adults
Supplemental material, sj-doc-1-dhj-10.1177_20552076251337948 for Willing or reluctant to share health data? A moderated mediation analysis of wearable device usage and data-sharing intentions among older adults by Luxi Zhang, Qingqing Xie, Sha Qiu, Muhan Liu, Fei You and Xinshu Zhao in DIGITAL HEALTH
Footnotes
Ethical considerations and consent to participate
The HINTS 5 general population survey underwent expedited review and was approved by the Westat IRB on March 28, 2016 (Project #6048.14). HINTS 5 also received a “Not Human Subjects Research” determination from the NIH Office of Human Subjects Research on April 25, 2016 (Exempt #13204).
Author contributions
LZ and QX contributed equally to this work and are co-first authors. LZ conceptualized the study, analyzed data, and provided substantial guidance throughout the manuscript writing process. QX conceptualized the study and wrote the original draft of the manuscript. SQ, ML and FY contributed to methodology and replicating results. XZ contributed to reviewing the manuscript and served as the guarantor for the research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by grants of University of Macau, including CRG2021-00002-ICI, ICI-RTO-0010-2021, CPG2021-00028-FSS and SRG2018-00143-FSS, Xinshu Zhao PI; Macau Higher Education Fund, HSS-UMAC-2020-02, Xinshu Zhao PI.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statements
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.