
Abstract
Objective
The diffusion of online health consultations (OHCs) depends on consumers switching from offline to online channels; consumers’ offline experience on health servicer determines their decisions. Our research aims to address this gap in the literature by examining how offline experiences of doctor–patient interactions influence online switching intentions.
Methods
We conducted online surveys, and 662 samples were collected and analysed the data using structural equation model via SmartPLS. Drawing on social exchange theory, we divided offline experience into balanced (discrete and relational social exchange) and unbalanced social exchange (doctor power and patient compliance). In accordance with the dedication-constraint model, perceived value and offline habit were defined as dedication and constraint factors, respectively; the influence of offline experience on both dedication and constraint factors was revealed. Moreover, we introduced the moderation effect to reveal the boundary of the effect of offline experience.
Results
Our findings showed that balanced social exchange increases consumers’ perceived value towards OHC, whereas unbalanced social exchange increases offline habit. Additionally, we observed a positive association between perceived value and the intention to switch, whereas offline habits had a negative impact. Online trust, as a moderator, strengthens the relationship between balanced exchange and perceived value and weakens the relationship between unbalanced exchange and offline habits. These results establish a theoretical framework for comprehending cross-channel switching in online health service marketing.
Conclusions
Since offline experience of doctor–patient interactions influences consumers’ decisions, it is critical for online health service platforms to apply cross-channel integration strategy rather than depend on online channels alone.
Keywords
Introduction
Online health consultation (OHC) is maintained by professional doctors, in which patients consult online doctors to improve their health 1 ; health professionals provide patients with information for diagnosis, treatment and prevention of diseases and injuries. 2 The emergence of OHC has been shown to reduce healthcare disparity, 3 improve doctor–patient relationships 4 and increase the efficiency of the management of chronic diseases. 1 The revenue from the OHC market in China is expected to reach 29 billion dollars. 5 Patients have begun to seek medical advice and treatment through online healthcare platforms instead of traditional offline channels. 6 However, the offline channel is sticky and remains competitive, as certain consumers tend to stick with offline options; 7 patient preference for the offline channel contributes to low participation in OHC.8,9
Switching behaviour refers to consumers changing service providers while remaining within the same service category. 10 To understand patients’ adherence to offline channel, the dominant perspective in the literature highlights the distinct characteristics of the online transactional context, indicating that trust, 11 privacy concerns, 8 transition costs 12 and relative advantages13,14 determine the patients’ decisions. The second perspective gives greater attention to offline factors in health care settings like satisfaction with offline service 6 and offline habits. 11 In line with the second stream, offline experience has been used to understand consumers’ stickiness to offline channel of service, such as physical experience, shopping experience and renting experience. For health services, offline experience plays a more critical role in cross-channel switching; healthcare services are viewed as high contact and involve intimate, one-to-one interactions. 15 High-quality offline interactions, such as doctor–patient communication, adherence to prescriptions and health education, lead to positive health outcomes.16–18
However, the distinctive attributes of healthcare services and its impact on consumer decision-making have been overlooked in the context of e-commerce, particularly in comparison to the broader domain of online shopping.19,20 Firstly, the delivery of healthcare services depends on the social interactions between doctors and patients. Improved interactions have been shown to result in enhanced diagnostic and treatment outcomes.21–23 Secondly, the relationship between doctors and patients is not balanced. The doctor's superior knowledge gives them greater power over the patient, which in turn affects consumer behaviour.20,24 In conclusion, the role of offline experience in health services requires further investigation to gain insight into cross-channel switching behaviours in OHC.
To our knowledge, this is the first study to investigate the role of offline experience of provider–consumer interactions in channel switching decisions. Specifically, we draw on prior research to classified social exchange into balanced and unbalanced social exchange, balanced social exchange emphasises the role of mutual dependency or reciprocity, and actors in balanced social exchange follow the principle of mutual dependence, while unbalanced social exchange occurs when actors must rely on scarce resources (e.g. skill and knowledge), and power and authority are involved in these social interactions.25–27 Our findings extend previous studies focusing on offline experience7,19,28 and provide a comprehensive model for understanding the role of offline experience in online service marketing. Moreover, our findings reveal both constraints and dedications related to service provider–consumer interactions, which extends previous findings in OHC research.4,20
Theoretical background
Cross-channel switching
Switching behaviour refers to consumers changing service providers while remaining within the same service category. 10 Unlike traditional switching behaviour, cross-channel behaviour in the e-commerce context involves switching from offline to online channels or vice versa. 29 For example, consumers gather information about products or services in physical stores but place orders via online channels for lower prices. 30 Recent research of cross-channel switching in OHC focused on switching from offline channel to online channel.6,14 Inequality in the distribution of medical resources drives patients to transfer from local hospitals to online health platforms. 3 Specifically, owing to the scarcity of human capital possessed by doctors, hospitals in urban areas have more health workers because they are able to pay higher salaries to elite doctors. 31 For example, only 23% of healthcare workers are deployed in rural areas worldwide, 32 and OHCs have been a promising channel to narrow inequality in healthcare resource distribution.
Social exchange theory
Social exchange theory (SET) has been used to understand social interactions in health care service. 4 The SET proposes that social interactions are driven by expectations of rewards and costs, 25 with each participant possessing resources available for exchange, including intangible resources such as affect and power, in addition to tangible items such as goods, money, and information. 26 As a high-contact service, the delivery of healthcare services hinges on the social interactions between doctors and patients; therefore, high-quality interactions lead to enhanced health outcomes. Social exchange has been widely applied to investigate the social interactions between service providers and consumers.4,33 Doctor–patient social interactions play a critical role in determining the outcomes of health care, 16 and intimate one-to-one interactions, good interpersonal relationships, accurate information exchange and collaboration in decision-making contribute to high-quality health care.22,23
Social exchange is divided into balanced and unbalanced social exchange.34–37 Balanced social exchange emphasises the role of mutual dependency or reciprocity; for instance, Actor A offers resources to Actor B with the expectation that B will offer rewards of equal value in return. 38 Specifically, balanced social exchange follows the principle of mutual dependence, in which participants rely equally on each other to benefit from resource exchange. Balanced social exchange in service plays a vital role in service quality. For example, consumers evaluate the informational and interpersonal outcomes provided by service providers, 39 and perceptions of fairness increase the continuous usage of live-chat services. 40 Since patients pay physicians for health consultations, we draw on prior research and define balanced social exchange in OHC as patients paying for health consultations with the expectation that doctors provide services that are of equivalent value to the cost.23,26
Conversely, unbalanced social exchange suggests an exchange may be associated with unilateral dependence and inequality; 25 authority, control or manipulation may be involved in social exchange.27,36 For example, if Actor A controls more valuable resources than Actor B does, a relationship built on mutual dependence may shift to unbalanced dependence. 41 In healthcare services, the doctor–patient exchange is often unbalanced because of the inherent power differential between the two parties. On the one hand, doctors require authority to fulfil their professional duties, such as ensuring that patients adhere to medication schedules. 24 On the other hand, doctors have exclusive knowledge, leading to an asymmetry of knowledge in doctor–patient interactions. Therefore, online doctors who withhold professional capital developed through education can benefit from knowledge asymmetry by obtaining higher returns in exchange. 42 Taken together, we define unbalanced social exchange as patients’ dependence on doctors due to their lack of professional knowledge and authority.20,43
It is important to note that both the balanced social exchange and the unbalanced social exchange consist of two sub-dimensions, respectively. The balanced social exchange includes discrete and relational social exchange, while unbalanced social exchange involves doctor power and patient compliance. Please see Appendix 1 for a detailed definition of concepts.
Dedication-constraint model
Prevalent theoretical models such as the technology acceptance model, unified theory of acceptance and use of technology and diffusion of innovation theory (DIT) are not specifically designed to address switching behaviour; empirical research applied alternative models to investigate switching behaviour.44–46 For example, the push–pull model has been used to investigate switching behaviour, suggesting that pull factors (e.g. perceived usefulness) attract consumers to new online service providers, while push factors (e.g. learning convenience and perceived price) repel consumers from current platforms.13,46,47 Similarly, the dedication-constraint model proposes that dedication and constraint mechanisms simultaneously determine relationship maintenance in consumer behaviour. 48 The dedication-based mechanism emphasises that positive experiences with current services encourage users to anticipate the future value. In contrast, the constraint-based mechanism focus on the psychological or emotional costs associated with discontinuing a service. 49 The dedication-constraint model has an advantage over other models because it provides a dual mechanism (e.g. dedication and constraint factors) rather than a singular mechanism, and the antecedents of dedication and constraint mechanisms can be further explored. Thus, in recent research, the dedication-constraint model was used to explore switching behaviour of online service users, such as mobile payment service users 45 and mobile data service users. 44
Research model and hypotheses
Balanced social exchange between service providers and customers can be classified as discrete and relational social exchanges. 50 Discrete exchanges have a short-term focus, limited communication, and careful evaluation of returns. In the health service industry, discrete exchanges involve technical problem-solving skills, with doctors utilising their expertise to address patient consultations. 23 Discrete exchange in OHC reflects the empowerment of online channels for consumers, which offer various benefits, including convenience and efficiency, 51 and patients using online health services can perceive higher levels of value. 6 Taken together, we define discrete exchange in this research as the patients’ evaluation of whether the health outcomes he or she obtains are consistent with the cost.
Due to the disparity in the distribution of medical resources, patients encounter lengthy waiting times when visiting top hospitals, and the quality of doctor–patient communication cannot be guaranteed owing to the rapidly increasing demand for healthcare.52,53 OHCs provide patients with prompt feedback, and the records are stored digitally, enabling access to consultations provided at any time. Patients on online health platforms receive prompt feedback, 54 benefit from superior diagnoses offered by top-tier doctors in elite hospitals 3 and acquire emotional assistance from online doctors. 21 Due to the relative advantage of online channel over offline channel, we propose the following:
H1. Discrete exchange positively influences the perceived value of OHC
Relational exchange emphasises long-term relationships, extensive communication and mutual commitment between individuals.33,55 In healthcare, relational exchange refers to the empowerment of patients so that an equal relationship can be established between doctors and patients. Relational exchange between doctors and patients is the result of the trend of patient-centred transition in health care; the concept of patient-centred is characterised by the belief that patients are experts on their own bodies and that they are encouraged to participate in decision-making about their diagnosis and treatment. 56 In other words, patients expect not only instrumental returns, as promised by discrete exchanges, but also an equal relationship with doctors. Recent research in the OHC context demonstrated the positive influence of relational exchange. Empirical research has reported that emotional support has a greater effect on patient satisfaction than pure informational support; 21 by studying patients who give virtual gifts to doctors, researchers found that OHC users seek to build solitary and long-term relationships beyond instrumental or discrete relationships. 4 Therefore, for patients expecting building an equal relationship could result in a higher OHC value. Therefore, we propose the following:
H2. Relational exchange positively influences the perceived value of OHC
As mentioned above, unbalanced social exchange suggests an exchange may be associated with unilateral dependence and inequality; authority, control or manipulation may be involved in social exchange. Power has been a major element of unbalanced social exchange. Power is the ability to influence another person by withholding resources or imposing punishment. 57 According to SET, when one party in a social exchange has more resources than the other, the advantaged party gains power over the other party, and power in social exchange can be used to explore unbalanced relations.25,27 In the service provider–consumer relationships, power is derived from an individual's knowledge and skills. 58 In unbalanced relationships, consumers lack sufficient knowledge or skills and are more sensitive to uncertainties in transactions,59–61 information derived from face-to-face transactions in offline channels is perceived to be more reliable, and choosing an offline channel can ensure consumers the safety of transaction.62,63
In the healthcare context, doctors withhold power because they have more knowledge of diagnosis, treatment and prevention. Therefore, they need the ability to change the behaviour of others. Healthcare is considered as credence goods. 64 Specifically, patients find it difficult to assess the quality of health services even after purchase, and doctors have a knowledge advantage over patients because relevant knowledge is accumulated from costly education and training. 65 Following this line, we define doctor power as the advantage that doctors have in knowledge and skills over patients. 22
Offline habits are typically associated with in-person and non-digital activities including brick-and-mortar store preferences and face-to-face communication. Retaining offline habits as a decision-making strategy is believed to avoid transaction uncertainties.66,67 For example, inexperienced customers tend to prefer traditional channels and are less likely to switch to online platforms because of their stronger offline channel habits. 68 Since the delivery of health consultations depends on professional knowledge, it is difficult for patients to assess the quality of online health services; sticking to offline channels would decrease potential risks. 69 Therefore, we propose that the experience of doctor power increase patients’ offline habits:
H3. Doctor power positively influences offline habit
Consumer compliance is the extent to which consumers adhere to recommendations or guidelines provided by a service provider or manufacturer. 70 Likewise, patient compliance refers to the degree to which a patient follows medical advice and adheres to prescribed treatment, such as taking medications, attending follow-up appointments, and implementing lifestyle changes. 71 In physician–patient interactions, patients nonrationally comply with physicians’ instructions. 72 In practice, doctors need power to fulfil their professional duties, such as ensuring that patients adhere to their medication schedules. 24 From the perspective of individual traits, the health belief model suggests that patients with stronger health beliefs are more likely to be more compliant with physicians. 73 In other words, high-compliance patients have higher demand for quality of health care. Recent research suggests that offline health care can provide more timely and comprehensive services. 69 For example, blood tests, X-rays and vaccination services depend on face-to-face visits, and multidisciplinary teams in brick-and-mortar hospitals can provide coordinated and comprehensive care plans. Therefore, high-compliance consumers are more likely to maintain offline habits due to their demands for timely and comprehensive health services. Therefore, we suggest the following:
H4. Patient compliance positively influences offline habit
In the online context, consumers face more uncertainties and risks in online commerce than in face-to-face transactions, such as the disclosure of privacy 74 and transactions with unfamiliar vendors. 75 Currently, OHCs invite offline doctors to register on these platforms. In other words, doctors on OHC platforms are not employees of OHCs, and patients have reason to suspect whether OHC managers can guarantee transactions on platforms. Online trust reflects consumer confidence in the reliability and integrity of online platforms, including their confidence in the structural assurance (e.g. institutions and policies) provided by institutions. 9 If consumers believe that OHC platforms have sufficient institutions to protect their interests, then their trust in the online transaction environment increases. Therefore, we propose the following moderation assumptions:
H5. Online trust strengthens the relationship between discrete exchange and perceived value
H6. Online trust strengthens the relationship between relational exchange and perceived value
Most patients cannot assess the quality of health services because of their lack of knowledge; thus, they turn to offline channels to avoid online risks. Such unbalanced social interactions strengthen the uncertainties of OHCs; however, a higher level of online trust indicates that patients have confidence that OHC platforms will take measures to prevent transaction fraud. Therefore, we propose the following moderation assumptions.
H7. Online trust weakens the relationship between doctor power and offline habits
H8. Online trust weakens the relationship between patient power and offline habits
Prevalent theories assume that consumers gather sufficient information about the design and functionality of technologies and evaluate their affordance, usefulness and values before deciding to adopt them. 76 Perceived value refers to an evaluation of the relative rewards associated with the adoption of technologies.77,78 Unlike other psychological evaluations of technology, the perceived value is goal oriented and serves rational and functional purposes. In the health context, research has demonstrated that the perceived value has a positive impact on patients’ intention to use online health services 11 and motivate patients to use online health service. 79 Moreover, by improving satisfaction, it promotes the intention to continue using the service. 80 In line with the dedication-constraint model, which emphasises that positive evaluation predicts future usage, we included perceived value as dedication in our study.
H9. Perceived value positively influences cross-channel switching intention
Offline habits are considered to be a major constraint in cross-switching decisions6,47,81; consumers’ offline habits hinder their intention to switch from offline to online channels.82,83 From a decision-making perspective, habits are formed through repeated practice in stable environments. 81 Although habits reduce the decision-making burden, researchers have found that they inhibit the diffusion of innovation and consumer adoption of new information systems. 67 Unlike other service sectors, offline healthcare behaviour has a more substantial impact on switching behaviour. Consumers in the healthcare industry encounter more risks and uncertainty, and patients find it challenging to rate the quality of healthcare services. Thus, maintaining the habit of meeting with familiar doctors in person can significantly mitigate these risks. The constraint-based mechanism of the dedication-constraint model proposes that perceived psychological or affective costs impede switching behaviours (see Figure 1). Hence, we hypothesise that offline habits function as a constraint when patients decide whether to opt for online healthcare services.
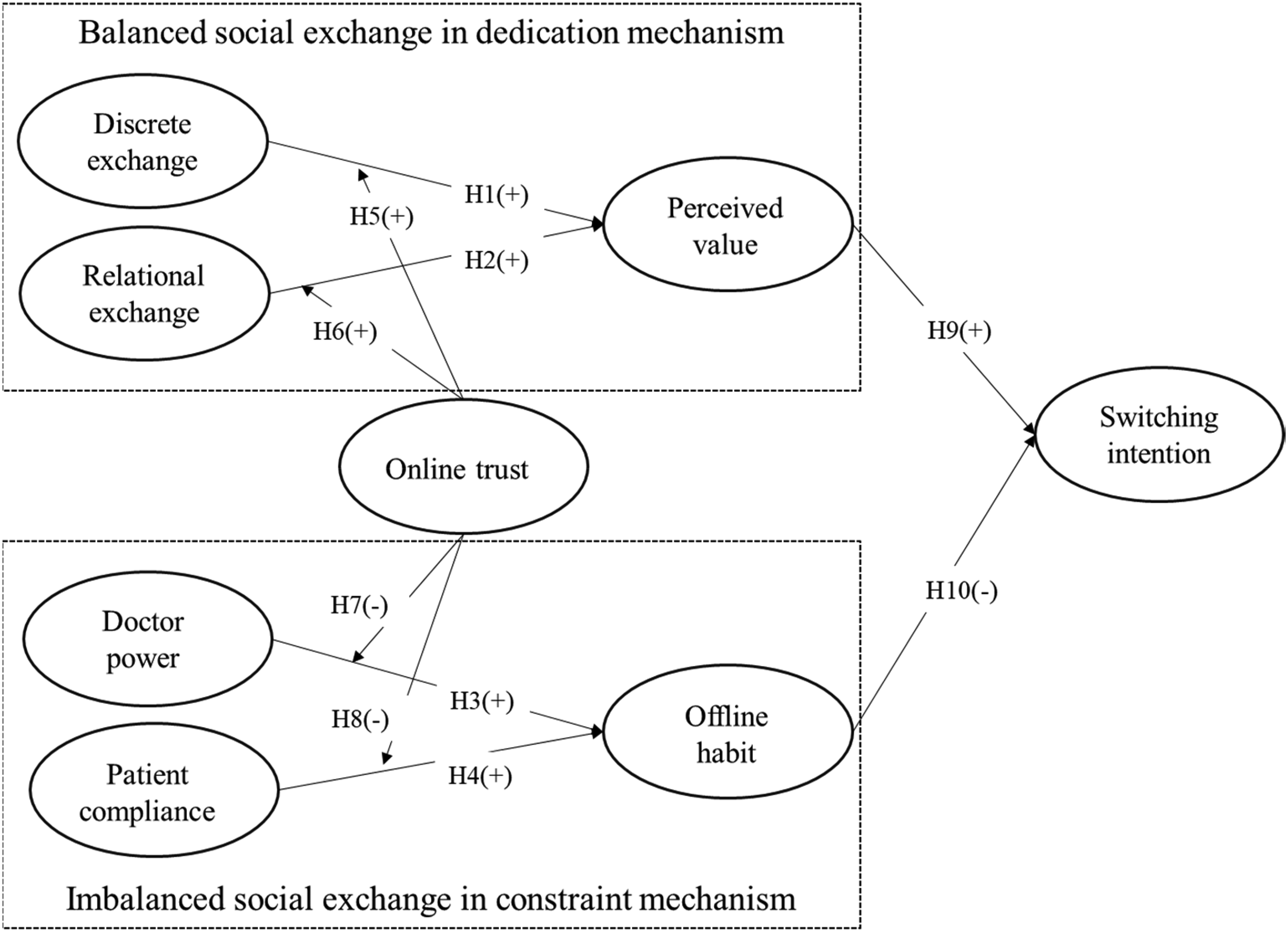
Theoretical model.
H10. Offline habit negatively influences cross-channel switching intention
Methodology
Data collection
This study is empirical research using structural equation model (SEM) to explore consumers’ intention to use OHC services; data were collected via online survey in China. We hired a professional survey company, Wenjuanxing, to collect survey data. The questionnaire was distributed in two waves. The first wave took place in November 2021 and lasted for 7 days, yielding a total of 258 valid responses. The second wave occurred in January 2022 and lasted for 3 days, resulting in 404 valid responses.
Because not all respondents were aware of the meaning of OHC, it has different names in daily life, such as telemedicine, e-health or online health services. In the introduction part of the survey, we (1) asked whether the respondents had visited offline hospitals in the past three months (e.g. community hospitals and general hospitals); (2) explained the meaning of OHC and specific functions of OHC (e.g. you can receive consultation services like in physical hospitals); and (3) listed famous OHC platforms in China (e.g. have you ever used the following OHC platforms in the past three months?) To ensure that respondents fully understood the terms of OHC, we ensured that 20.53% of respondents had used OHC in the past 3 months, which is close to the 28.5% in the national survey. 84 In addition, to control for the effect of health status, we added a question to assess respondents’ health status: “Would you say your health is very good, good, fair, poor, or very poor?”
Data were collected from 12 provinces, covering the main regions of China. To increase the response rate, we offered a monetary incentive value of 1 dollar for participation. Finally, a total of 662 valid responses were obtained (see Table 1).
Demographic profile (n = 662).

To guarantee the quality of the data collection, (1) all questions were randomly ranked to eliminate potential common method bias, (2) attention-trap questions were randomly set to verify the quality of the survey data, and (3) the data of respondents who took less than 2 minutes were deleted. Since our data were collected from one questionnaire, we applied the full collinearity assessment approach to evaluate the common method bias in our research. The full collinearity assessment approach uses variance inflation factors (VIFs) to assess the common method bias. 85 As suggested by Appendix 2, the VIFs of all constructs were lower than the threshold of 3.3, indicating that the model was not contaminated by common method bias.
To address ethic issues, we employed multiple strategies. (1) We adhered to the principle of transparency, ensuring that participants are fully informed about the study's content. On the first page of the questionnaire, participants were provided with detailed information regarding the academic purpose of the study, the legal provisions safeguarding data security and the contact information of the project manager. (2) Written informed consent was obtained from all subjects prior to the commencement of the study. Participants were fully informed and agreed to share sensitive data for academic purposes. Sensitive data, including self-reported health status, were collected only after participants explicitly provided their consent. (3) We adhered to strict ethical principles to ensure that the questionnaire items posed no psychological harm to participants. All data collected were anonymised and identified only by a system-generated random ID. The IRB of Harbin Institute of Technology School of Management approved this research (ref no:jgxy202010221).
Measures
We modified previously validated measures in the literature to operationalise the variables in our research. The necessary permissions to use all applicable tools and questionnaires have been obtained. In this study, we used two variables, discrete exchange and relational exchange, to investigate the role of balanced social exchange. To measure discrete exchange, we adopted two items of the exchange relationship developed by Johnson and Grimm. 86 To measure relational exchange, we used four items of participative decision-making, which were first developed by and Spekman 87 and then modified by Hausman 16 to be adaptable to health consumption.
To study the effect of unbalanced exchange, we employed the notions of doctor power and patient compliance. The three items developed by Raven et al. 88 were used to measure doctor power. We used three items to measure patient compliance; these items were developed by Hausman. 89
We used three items to measure the perceived value, developed by Liang and Xue 90 to explore online health information use. Two items adapted from Zhang et al. 9 were used to measure the offline habits.
Two items adapted from Zhang et al. 6 were used to measure switching intention. Table 2 provides a detailed description of items applied in this research.
Constructs and scales.

Statistics analysis
Data analysis was performed using SEM with partial least squares (PLS-SEM) in SmartPLS. Since PLS is recommended for examining less-developed models, 91 it was applied instead of traditional covariance-based structural equation (CB-SEM). Unlike traditional CB-SEM, PLS-SEM uses weighted composites of indicator variables as proxies, making it suitable for situations where the theory is less developed. As the theory used in our model was not estimated in prior studies, we used PLS-SEM instead of CB-SEM to introduce new variables and paths.
Results
Reliability and validity
To assess reliability and validity, factor loadings, average variance extracted (AVE), composite reliability (CR) and Fornell and Larcker's criterion were used to evaluate the measurement model.
As shown in Table 2, the factor loadings of items were all above or close to the threshold of 0.7, and the CR values ranged from 0.773 to 0.890, indicating that the measurement of constructs possessed internal consistency, and the reliability of measurement was guaranteed.
Table 2 showed that AVEs surpassed 0.5, thus confirming the convergent validity of the measurements. In addition to evaluating convergent validity, we evaluated discriminant validity by Fornell and Larcker's criterion; to determine the discriminant validity, the square root of each construct's AVE is expected to be above the coefficient of bivariate correlations with other constructs. The results in Table 3 suggest discriminant validity.
Fornell and Larcker's criterion.
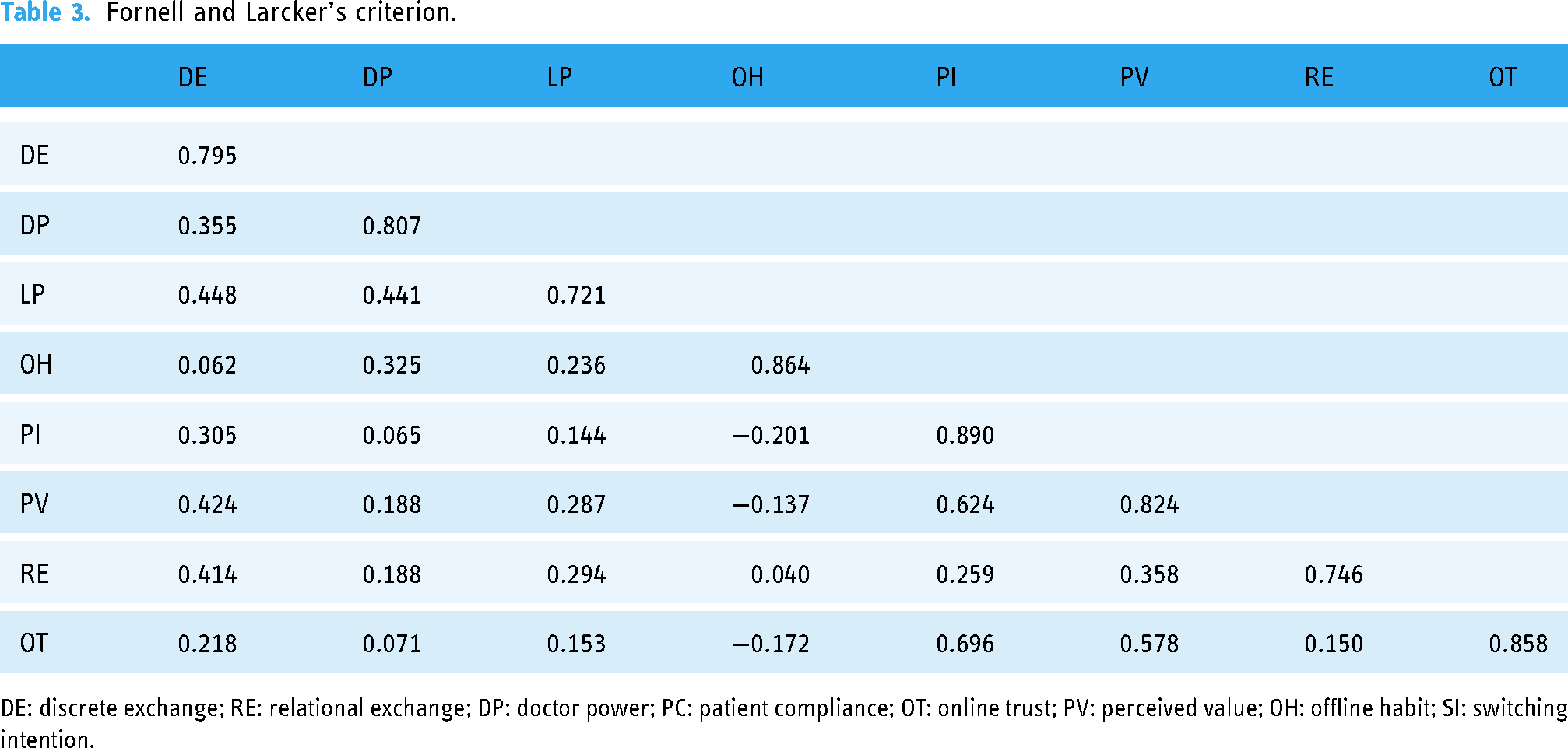
DE: discrete exchange; RE: relational exchange; DP: doctor power; PC: patient compliance; OT: online trust; PV: perceived value; OH: offline habit; SI: switching intention.
Hypotheses testing
We performed SEM with SmartPLS 3.3.9 to test the hypotheses (see Figure 2). We use PLS-SEM for two reasons. First, this study entails multiple moderation requirements, and PLS is recommended for complex model estimations. Second, SmartPLS weighted composites of indicator variables as proxies, which relaxes the assumptions of CB-SEM based on sum scores, making it suitable for situations in which the theory is less developed.

Results of structural model.
The results demonstrated that discrete exchange (β = 0.266; p < 0.001) exerted a significant influence on perceived value, indicating that H1 was supported. The positive effect of relational exchange on perceived value (β = 0.179; p < 0.001) supports H2, indicating that patients with higher expectation in sharing decision rights of doctors are more likely to perceive the value of OHC; these results are consistent with the assumption that online channel possesses a relative advantage over offline channel, which is in line with the results from previous studies emphasising the relative advantage of OHC over offline channel.4,42 Meanwhile, doctor power (β = 0.245; p < 0.001) and patient compliance (β = 0.142, p < 0.01) had a positive effect on offline habits, thereby accepting H3 and H4; by adding unbalanced exchange as antecedents of constraints, these results extended prior work focusing on constraints in cross-channel switching in OHC. 9
Regarding the moderation role of online trust in dedication mechanism, the interaction effect between online trust and discrete exchange was significant (β = 0.064; p < 0.1), suggesting that the relationship between discrete exchange and perceived value was stronger in higher degree of online trust (see Figure 3); thus, H5 was supported. However, the moderating effect between online trust and relational exchange was not significant, and H6 was not supported. Turning to the moderating effect of online trust on unbalanced exchange (doctor power and patient compliance), the interaction effect between doctor power and online trust (β = −0.148; p < 0.01) was significant, but the effect was not significant between patient compliance and online trust, revealing that stronger trust on health service providers would weaken the impacts of doctor power; therefore, among H7 and H8, only H7 was supported (see Figure 4). Researchers have proposed that when users are confronted with new technology, they are more likely to stick to habits to avoid uncertainties, 67 and our findings further suggest that consumers who perceive unbalanced social exchanges (e.g. service providers possess more power) would also stick to offline habits, but a higher level of online trust could weaken this relationship.

Interaction between online trust and discrete exchange.

Interaction between online trust and doctor power.
Finally, perceived value (β = 0.582; p < 0.001) positively affected switching intention, while offline habits (β = −0.123; p < 0.001) were negatively associated with switching intention, thereby confirming H7 and H8; the results showed that when deciding whether transferring to online channel, offline habit acts as constraints in cross-channel switching, these results are in line with prior research that cross-channel switching decision is determined by more than one single mechanism.45,48
Discussion
Key findings
This research aimed to investigate the mechanism by which health care consumers switch from offline channel towards online channels. We adopted the dedication-constraint model proposed by research performed in e-commerce.45,48 Given that the healthcare service context is characterised by social exchange between doctors and patients,20,21 we added balanced and unbalanced exchanges as antecedent variables in the dedication-constraint model. Drawing on two online surveys of 662 consumers, we introduced a moderation effect to reveal the boundary of the effect. Our results indicated that 41.3% of the variance could be explained using this model.
We found that balanced exchange (discrete and relational) between doctors and patients was positively related to the perceived value; in other words, balanced exchange acted as an antecedent in the dedication mechanism. These empirical results are in line with prior research conducted on e-commerce, and previous findings agree that information technology empowers offline service providers by providing more efficient services. In addition, the classification of discrete and relational exchanges indicates that social interaction should not be ignored in the health care service context.
In our research, unbalanced exchanges were proven to enhance offline habits, and doctor power and patient compliance had a positive effect on offline habits. In short, consumers who believe that doctors have more knowledge and authority over them are more likely to stick to the offline channel. To further reveal the role of unbalanced exchange, online trust was found to positively moderate the link between doctor power and offline habits, suggesting that the online environment (e.g. risks and uncertainties) strengthened the association between unbalanced exchange and offline habits.
Theoretical implications
This study has three implications for the theoretical development of cross-channel switching behaviours.
First, we identified the key factors of balanced and unbalanced social interactions switching behaviour; it is one of the first to investigate how offline experience of social interactions in determining switching decision. Although the role of social interactions in determining consumer decision-making has been explored,20,63 the balanced and unbalanced characteristics of social interactions have been ignored. Based on SET and the literature on health service,22,23 we found that both balanced and unbalanced relations exist in social interactions between doctors and patients, acting as antecedents in the dedication-constraint framework. These results deepen our understanding of the social interactions between professionals and consumers (e.g. doctors and patients) and reveal the mechanism by which offline social interactions influence consumers’ attitudes towards online services.
Second, our findings extend previous studies focusing on offline experience and provide a comprehensive model for understanding the role of offline experience in online service marketing. So far, previous literature has realised the effect of offline factors in cross-channel switching. 6 However, offline experience has not been clearly identified in the OHC context, and the mechanism by which offline experience work has not been fully explored. With the introduction of dedication- and constraint-based paths, the mechanism by which offline social interactions influence online behaviour was further revealed. The dedication-constraint framework has been used to study switching behaviour in an online context; our research suggests that this framework is also applicable to cross-channel switching.
Third, the introduction of the moderating effect of online trust sheds light on the boundary conditions that restrict switching from offline health service channels to online channels. In China, online shopping platforms have formed perfect governance institutions, including payment institutions and delivery systems, to guarantee consumer interests. However, our results demonstrate that a lack of online trust inhibits switching intention in the OHC context and extend prior work by revealing how online transaction environments influence cross-channel switching in the OHC context.
Practical implications
Practitioners and scholars have long realised that healthcare differs from other services because of the credence feature and social interactions involved, making it difficult to predict consumer behaviour in the health context. Our results suggest that online transaction environments may complicate the situation in OHC. The bad news is that there is a challenge for the online health industry to continuously attract more offline patients, as suggested by our findings. Furthermore, while practitioners have noted the potential of combining AI and OHC in this area, this study demonstrates the importance of face-to-face communication for health services from a social interaction perspective.
Constraint-based mechanisms affect consumers’ switching decisions from offline to online channels, but the good news is that the dedication-based mechanism was proven to promote switching intention, indicating the relative advantage of online channels in healthcare settings. There are several suggestions for OHC industry practitioners.
First, OHC platforms should increase their relative advantages over offline health service channels by consolidating the relationships between consumers. In developing countries, the disparity in health resource distribution and the low efficiency of service delivery highlight the advantages of OHC. In the online channel, patients can choose elite doctors from different hospitals without geographic limitations. Our results suggest that consumers who prefer relational exchanges are more likely to perceive OHC benefits. To build a better relationship with consumers, doctors in OHC can update personal bloggers to interact with visitors, publish health tips and provide short videos of professional suggestions. OHC apps enable doctors to send instant messages regarding diet and exercise notifications to patients, which is important for chronic patients.
Second, to narrow the negative effect of constraints, it is critical for OHC platforms to apply cross-channel integration strategy rather than depend on online channels alone. Recent research has pointed out that efficiency improvements in online channels (e.g. speed, effort and flexibility) cannot fully substitute the role of the offline channel; in the OHC context, patients’ experiences and expectations derived from offline social interactions could be an obstacle to switching intentions. From a more general perspective, as demonstrated by our research, consumers in developing countries who perceive more knowledge advantage of doctors are more likely to adhere to offline habits, indicating that offline channels in healthcare still play a key role in consumers with low health literacy. It is important for OHC providers to cooperate with offline hospitals to attract consumers with strong offline habits, for instance, the hierarchical healthcare system founded by the government, in which community hospitals typically serve as the first point of contact for patients and handle a wide range of general medical conditions. Patients are encouraged to visit community hospitals during their first visit rather than directly visiting elite general hospitals. As community residents, consumers are familiar with doctors in community hospitals. Cooperation between OHC and community hospitals could convince more consumers to switch to online channels for health services.
Additionally, establishing better governance in OHC is important for consolidating consumer trust. Our findings suggest that although perceived doctor power strengthens offline habits, a higher level of trust in OHC weakens the effect of unbalanced exchanges on offline habits. Enhancing the transparency of privacy and transaction policies can improve perceptions of certainty.
Limitations and future research
Although this study reveals the influence of balanced and unbalanced social interactions on OHC users’ switching intentions, we acknowledge some limitations. First, demand for health services differs across patients. Prior research has shown that chronic patients are more inclined to choose online channels because they demand more continuous feedback from doctors. Future research should investigate the behaviour of patients with different diseases. Second, we proposed that both balanced and unbalanced social interactions exist in healthcare settings. In service marketing, balanced and unbalanced relationships have been widely observed in fields such as education, finance and consultation. Thus, the generalisability of our empirical findings should be explored in future studies conducted in different contexts. Lastly, from the cultural difference perspective, our samples were collected in China, where the pattern of doctor–patient social interaction may be different from those in countries outside East Asia (e.g. attitudes towards authority). Future research should compare the results of respondents from different cultural backgrounds. In addition, during the pilot phase of this study, qualitative methods were used to ensure the contextual relevance of the questionnaire. However, formal reliability and validity assessments using a small-scale sample were not conducted.
Conclusion
In the past decades, providing services via online channels has been prevalent in the business world; however, as revealed by our findings, the social interactions involved in providing services may have different influences on consumers’ crossing-switching decisions. Although the empowerment of digital technologies enables timely feedback and convenient social interactions in online channels, the pursuit of balanced relationships (e.g. discrete and relational social exchange) drives consumers to use online services, and unbalanced relationships between consumers and professionals may consolidate the negative effect of constraints.
Due to the prevalence of COVID-19, the market size of OHC has increased significantly in recent years. More importantly, policymakers in developing countries have realised the positive role of OHC in reducing health inequalities. Understanding why some patients still adhere to offline channels is of great value to investors and policymakers. Prior literature has paid more attention to consumers’ switching behaviour from one online provider to another; only a few have noticed the phenomenon of cross-channel switching from the perspective of social interaction. Our research extends the dedication-constraint model by investigating the role of social interactions as antecedents and provides a comprehensive framework for understanding cross-channels in health service marketing. Drawing on the dedication-constraint model and SET, we found that balanced and unbalanced social exchanges play positive roles in dedication- and constraint-based mechanisms, respectively.
Additionally, online trust moderates the effect of unbalanced exchange, suggesting that OHC shares similarities with other types of e-commerce in that uncertainties and risks determine consumers’ decisions, which is in line with prior research conducted in e-commerce.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251326135 - Supplemental material for Impact of offline experiences on consumer decisions: Balanced vs. unbalanced social exchange in switching to online health services
Supplemental material, sj-docx-1-dhj-10.1177_20552076251326135 for Impact of offline experiences on consumer decisions: Balanced vs. unbalanced social exchange in switching to online health services by Teng Wang and Yongqiang Sun in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to express their gratitude and appreciation to all those participants who gave them the possibility to complete this study.
Contributorship
T Wang conceived the study and contributed to funding acquisition, formal analysis and validation. YQ Sun visualised, reviewed and edited the study and contributed to methodology and validation. T Wang conceptualised the study and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The IRB of Harbin Institute of Technology School of Management approved this research (jgxy202010221). Participants were informed about the purpose of the study, their rights and the guarantees provided. They signed a consent form to participate in the survey, acknowledging their voluntary participation and understanding of the terms. The written consent details are as follows: ‘To inform evidence-based healthcare policy formulation, the research team at Harbin Institute of Technology is conducting a scientific survey on digital healthcare engagement. This anonymous questionnaire complies with the Statistical Law of the People's Republic of China (Article 39) regarding data confidentiality. The survey will collect health-related information, which will only be used for academic research purposes. Your participation is voluntary, and your responses will only be recorded if you provide explicit consent. If you are uncomfortable with any of its contents, you have the right to withdraw at any time without providing a reason. Your responses will significantly contribute to academic research, and we sincerely appreciate your participation’.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Natural Science Foundation of Shandong Province (ZR2024QG117).
Natural Science Foundation of Shandong Province (grant number ZR2024QG117).
Supplemental material
Supplemental material for this article is available online.
Definitions of key concepts
Concepts
Definition
Source
Balanced social exchange
Balanced social exchange emphasizes the role of mutual dependency or reciprocity
(Cook, 1978)
-Discrete social exchange
We define discrete exchange in this research as the patients’ evaluation of whether the health outcomes he or she obtains are consistent with the cost
(Macneil 1982)
-Relational social exchange
In healthcare, relational exchange refers to the empowerment of patients so that an equal relationship can be established between doctors and patients
(Keith et al. 2004; Shore et al. 2006)
Unbalanced social exchange
Unbalanced social exchange suggests an exchange may be associated with unilateral dependence and inequality
(Blau 1964; Emerson 1962)
-Doctor power
The advantage that doctors have in knowledge and skills over patients
(Ha et al. 2010)
-Patient compliance
Patient compliance refers to the degree to which a patient follows medical advice and adheres to prescribed treatment, such as taking medications, attending follow-up appointments and implementing lifestyle changes
(Garrity 1981)
Results of full collinearity assessment DE, discrete exchange; RE, relational exchange; DP, doctor power; PC, patient compliance; OT, online trust; PV, perceived value; OH, offline habit; SI, switching intention.
Constructs
Items
Outer VIF values
Inner VIF values
AW
PV
SI
DE
DE1
1.079
\
1.404
\
DE2
1.079
RE
RE1
1.840
\
1.219
\
RE2
1.320
RE3
1.249
RE4
1.665
DP
DP1
1.571
1.307
\
\
DP2
1.409
DP3
1.422
PC
PC1
1.154
1.333
\
\
PC2
1.302
PC3
1.417
OT
OT1
2.043
1.079
1.071
\
OT2
2.009
OT3
1.651
PV
PV1
1.533
\
\
1.099
PV2
1.568
PV3
1.553
OH
AW1
1.325
\
\
1.077
AW2
1.325
SI
SI1
1.520
\
\
\
SI2
1.520
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.