
Abstract
Objective
Multiple sclerosis (MS) is a chronic neurological condition that significantly impacts the quality of life of affected individuals. Telehealth interventions (TIs) have emerged as a promising avenue for providing healthcare services remotely, potentially improving outcomes and enhancing the quality of life for people with MS. This systematic review aims to assess the impact and efficacy of TIs on outcomes of people with MS by synthesizing and comparing outcomes from related randomized controlled trials.
Methods
The systematic review protocol will involve searching electronic databases (PubMed, Web of Science, Scopus, EMBASE, CENTRAL), gray literature resources, and key journals from 1997 to June 2023 for keywords related to Telehealth and MS. The collection of research-related articles will be followed by the removal of duplicates before they are included in the study. During the screening stage, the titles and abstracts of the articles will be reviewed, and irrelevant articles will be excluded. The full text of relevant articles will be independently evaluated by two researchers, and data will be extracted from the final articles. The findings will be classified and recorded in an extraction table. The risk of bias will be assessed using the Cochrane Collaboration tool. The data will be analyzed using STATA version 14.2. The PROSPERO ID for this study is CRD42023450081.
Discussion
This study aims to address the current knowledge gap by investigating the comparative effectiveness of TIs. The findings of this research will provide valuable insights and evidence regarding the effectiveness of these interventions, assess their feasibility and accessibility, examine patient outcomes, identify research gaps, and offer guidance for clinical practice and policy-making.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic neurodegenerative disease that affects millions of people worldwide, causing physical and cognitive impairments. 1 The worldwide prevalence of MS is estimated to be 2.3 million people. Typically, the onset of the disease occurs during early adulthood. 2 The signs and symptoms of the disease are unpredictable and uncertain. 3 Its neurological condition is characterized by a wide range of symptoms, including fatigue, muscle weakness, balance problems, and cognitive impairments, which can significantly impact the quality of life (QoL) of the patients.4–6 A significant concern in MS care is the limited access to specialized healthcare services, with studies revealing that at least 31% of individuals with MS lack the necessary access to such services.7,8 Furthermore, the management of MS typically involves frequent visits to healthcare facilities, which can be particularly challenging for those with mobility issues or residing in remote areas.9–11 This emphasizes the pressing need for improved accessibility and availability of specialized care for individuals with MS. Fortunately, the emergence of Telehealth interventions (TIs) has provided new opportunities for the care and support of MS patients.8,12
Telehealth, leveraging high-speed internet, affordable cameras, and monitoring software, shows promise in bridging the gap between MS specialty care providers and patients with limited access.8,13,14 Telehealth, also referred to as telemedicine or remote healthcare, utilizes telecommunication advancements to remotely deliver medical services and interventions.15,16 This approach allows healthcare professionals to monitor, diagnose, and treat MS patients in real time, overcoming the constraints of time and location.17,18 The benefits of Telehealth include enhanced accessibility, convenience, and the potential for improved patient outcomes.19,20 Throughout the search conducted across various databases, numerous clinical trial studies were carried out to examine the impact of TIs on enhancing the well-being of patients with MS. These studies reported various outcomes, such as QoL, depression, fatigue, pain, and anxiety,21–24 but the primary outcome of the most of them focused on QoL. These researches delve into different types of telehealth (synchronous and asynchronous), such as telephone consultations, remote monitoring, mobile applications, and telerehabilitation programs. They specifically highlight the unique advantages, outcomes, and limitations associated with each modality, providing valuable insights into the diverse approaches of telehealth in improving the QoL of patients with MS.21–26 The latest review study in this field, conducted in 2018, primarily emphasized positive or significant findings, potentially disregarding negative or non-significant reports. This review study acknowledged the need for a comprehensive systematic review with accurate inclusion criteria and a wider search scope. It also recognized the importance of examining additional outcomes to provide a more comprehensive understanding of the effects of TIs in MS care. 8 Hence, the objective of the upcoming study will be to assess the impact and effectiveness of TIs on QoL in individuals with MS. This study aims to achieve its objectives by synthesizing and comparing the findings from relevant randomized controlled trials (RCTs) while also acknowledging the limitations of the existing evidence. Additionally, it seeks to identify future research needs in the field of TIs for MS.
Methods
Aims
The objective of this review is to conduct a systematic review and meta-analysis (SRMA) to estimate the effectiveness of TIs on QoL of individuals with MS.
Methodology
This SRMA adhered to the methodological guidelines outlined in the Cochrane Handbook, 27 as well as the reporting standards set by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P).28,29 These established frameworks were followed to ensure the rigorous and transparent execution of the review process. The PROSPERO ID for this study is CRD42023450081. It is important to note that this study is part of RHS's grant, which has been approved and registered at TUMS under the registration number 1401-4-160-63983.
Criteria for study selection
Inclusion criteria
This SRMA includes RCTs that examine the impact of TIs on outcomes related to MS, such as QoL, fatigue, and depression. There are no restrictions regarding the age or sex of the patients included in the studies. Published articles in any language will be considered, as long as they have full English abstracts.
The PICO components based on the questions in the present study are as follows:
P (Population): Patients with a confirmed diagnosis of MS. I (Intervention): Interactive and non-interactive interventions (both synchronous and asynchronous) that are delivered by healthcare providers will be included. Device-based interventions such as stimulators, sensors, robots, and mechanical devices (e.g. vibrators, cooling vests, and wheelchairs) will be excluded. C (Comparison): The control group consists of patients who have not received any interventions or have not received TIs. O (Outcome): The primary outcome is QoL, measured using questionnaires such as the Multiple Sclerosis Impact Scale (MSIS), Hamburg Quality of Life in Multiple Sclerosis (HAQUAMS), Short Form 36 (SF-36), Short Form 12 (SF-12), EuroQol 5-Dimension (EQ-5D), Assessment of Quality of Life (AQoL), World Health Organization Quality of Life (WHOQOL), Leeds Multiple Sclerosis Quality of Life Scale (LMSQoL), Multiple Sclerosis International Quality of Life (MusiQoL), Functional Assessment of Multiple Sclerosis (FAMS), Leeds Multiple Sclerosis Quality of Life Scale (LEEDS QoL), Quality of Well-Being (QWB), and Multiple Sclerosis Quality of Life-54 (MSQOL-54).30–34
Exclusion criteria
Duplicate and redundant publications: If a study has been published in multiple journals, only the most recent and complete version will be included.
Exclusion of certain publication types: Narrative reviews, book chapters, opinion pieces, letters, and any other publications lacking primary data or explicit method descriptions.
Availability of required findings: Studies that do not provide the necessary findings for SRMA.
Studies that include populations other than MS patients or have mixed populations.
Data sources and search strategy
A comprehensive search will be conducted in the following electronic databases: PubMed, SCOPUS, EMBASE, ISI Web of Science, EBSCO, and the Cochrane Central Register of Controlled Trials (CENTRAL). The search will include articles published from 1997 to June 2023. There will be no restrictions on language, ensuring that a wide range of studies are included in the review.
In addition to the databases mentioned, other resources will be utilized to identify relevant studies for the review. These resources include:
Reference lists: The reference lists of relevant primary studies and related reviews will be examined to identify additional studies that may be relevant to the research question.
Gray literature resources: Google Scholar, Open Grey, ProQuest, and Scopus will be searched for gray literature publications that may not be indexed in traditional databases. Contacting experts in the field and conferences paper will also be undertaken to gather additional information. Protocol databases such as ClinicalTrials.gov, International Standard Randomized Controlled Trial Number (ISRCTN), and The WHO International Clinical Trials Registry Platform (ICTRP) will be searched for ongoing or unpublished studies.
The search terms will include multiple sclerosis, telehealth, and QoL. Table 1 outlines the search strategy utilized for PubMed. It presents a summary of the search terms and keywords used to identify pertinen studies investigating the impact of TIs on QoL in individuals with MS.
PubMed search strategy (to be adapted for the other databases).

Note. aAs it was discovered during the initial search that some studies did not refer to the QoL or TIs in their titles and abstracts, a revised search approach was developed, focusing on the full text of the articles to ensure a comprehensive range of studies is included in the review.
Screening procedures of eligible studies
After conducting the systematic search, the obtained results will be imported into Endnote software version X7. The software will be used to identify and remove any duplicate articles, ensuring that each study is considered only once in the review process. In the screening phase, two reviewers (RHS and MD) will independently screen the titles and abstracts of the articles based on the predefined inclusion criteria. This process aims to identify potentially eligible articles for further evaluation. For the titles and abstracts that meet the inclusion criteria, the corresponding full-text articles will be obtained. These full-text articles will then be independently assessed by the reviewers to determine if they meet all the inclusion criteria for the SRMA. Any discrepancies or disagreements between the two reviewers during the screening and assessment process will be resolved through consensus. Both reviewers will discuss and reach an agreement on the inclusion or exclusion of the article. However, if a consensus cannot be reached, a third author (RN or LS) will independently assess the article and provide the final decision. These measures will be implemented to maintain a rigorous and unbiased selection process, minimizing potential bias during the study's selection phase. The plan for study screening and selection, including the process study, will be outlined in Figure 1.
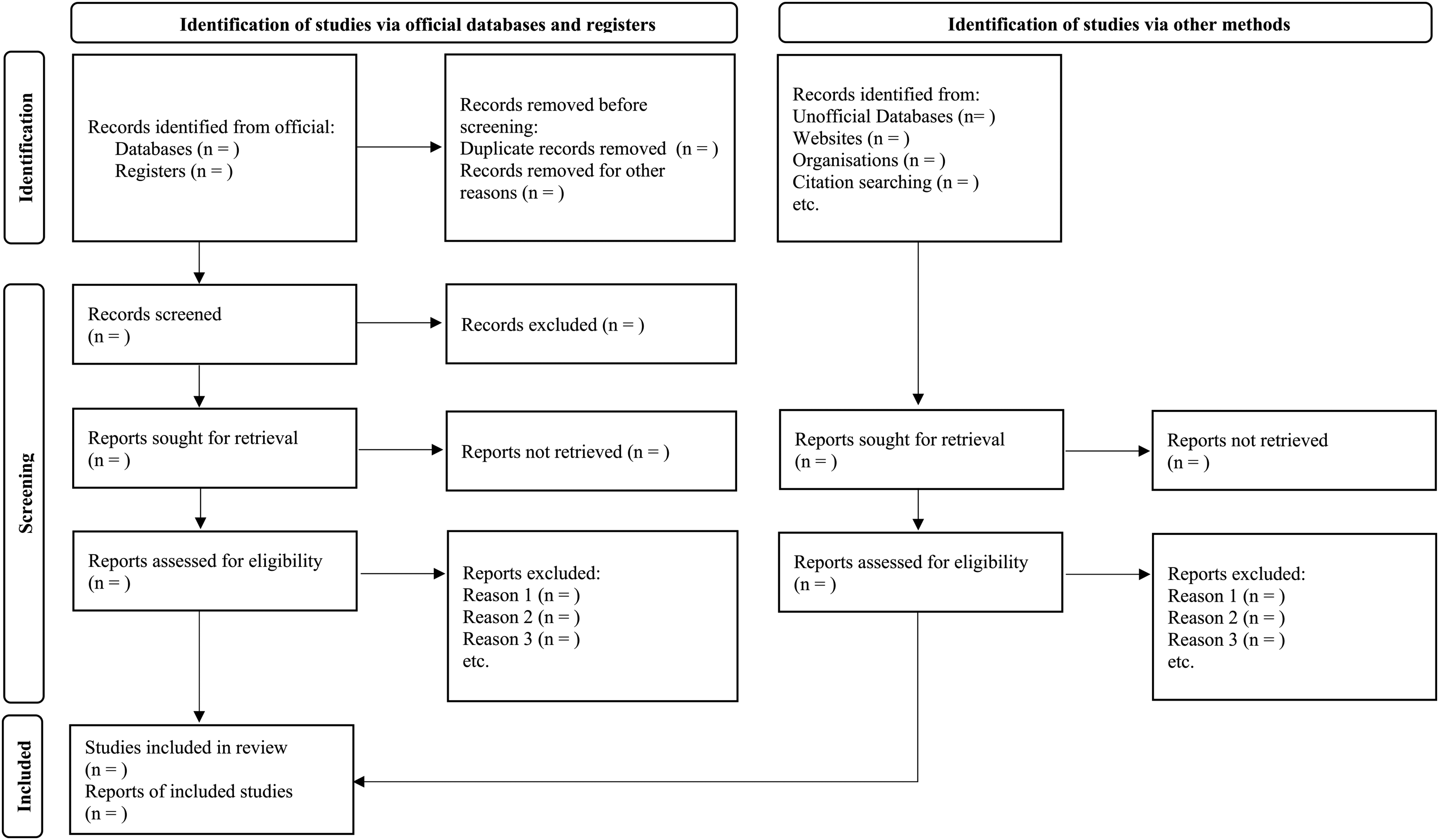
Plan of study screening and selection process.
Assessment of risk of bias
Two authors will independently assess the methodological quality of all full-text manuscripts included in the review, following the current guidelines from the Cochrane Handbook for evaluating the risk of bias in included RCTs.27,35 The quality of RCTs will be assessed across five domains: selection bias, performance bias, detection bias, attrition bias, and reporting bias. In case of any inconsistencies, they will be resolved through consensus between the two reviewers. If a disagreement persists, the opinion of a third expert (LS) will be sought to make a final determination. The risk of bias will be categorized as high, low, or unclear based on the available data and level of certainty.
Data extraction
Two authors (RHS and MD) will perform data extraction using a pre-designed form that outlines the relevant information about the study, including its objectives, primary and secondary outcomes (fatigue and depression, if they were assessed in the included studies), sample characteristics, intervention details, follow-up duration, analysis methods, critical appraisal information, intervention effectiveness, and study limitations. Any discrepancies during the data extraction process will be resolved using the consensus-based approach mentioned earlier.
If the required data is not available in the included studies, attempts will be made to collect the data using tools like Webplotdigitizer or by contacting the corresponding authors for the missing information. If the authors do not respond after three attempts, the study will be excluded from the review.
Missing data management
Missing or unclear data will be addressed by attempting to contact the authors via email to obtain the necessary information. The available data will be analyzed, and sensitivity analysis will be performed to assess the robustness of the results. This analysis will help evaluate the impact of the missing or uncertain data on the overall findings of the study.
Strategy for data synthesis and statistical software
Descriptive statistics will be computed using SPSS 16 (IBM Company, Chicago, IL, USA) to present the characteristics of the included references, such as information on the authors, publication year, population, interventions, and settings. Due to the variability in study design, methods, and outcome measures, the primary approach for data synthesis will be narrative or descriptive.
The meta-analysis will be based on the mean differences and their standard deviations of QoL. Effect sizes will be calculated using Cohen's d statistic, 36 In cases where the standard deviation is not reported directly, the method proposed by Hozo et al.37,38 will be employed to estimate the standard deviation based on the available results from the articles. A meta-analysis will be conducted using random-effects models if applicable to calculate the overall effect size while accounting for heterogeneity between studies. This approach considers variations across the included studies and provides a robust estimation of the treatment effect. 39 Heterogeneity will be assessed using the I2 statistic, with values higher than 50% indicating high heterogeneity, and the Q-test, with values less than 0.05 indicating significant heterogeneity. 40 Publication bias will be assessed using statistical tests such as Egger's and Begg's tests which will visualize in a funnel plot. 41 Sensitivity analysis will be performed using the leave-one-out method to examine the influence of individual studies on the overall results. 42 All statistical analyses will be conducted using STATA software (StataCorp) version 14.2.
The Robvis (Risk-of-Bias Visualization) package will be employed to generate Risk-of-Bias figures, providing a visual representation of the assessment of bias in the included studies. 43
Validity, reliability, and rigor
We will strive to utilize the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach to generate a summary of findings. Additionally, our SRMA will adhere to the reporting and design criteria outlined in the Cochrane Handbook, 27 and the protocol was developed following the PRISMA-P guidelines28,29 to ensure the integrity, validity, and reliability of the study.
Discussion
The field of telehealth has experienced significant growth due to technological advancements and offers promising opportunities for healthcare. 44 Given that MS often occurs at a young age and individuals with MS are familiar with technology, studying TIs in this population is crucial to understanding their effectiveness in meeting the specific needs of these patients and improving their healthcare outcomes. 45 Although various TIs have been explored in recent studies, there is a lack of systematic research on their value in the context of MS. A previous review conducted in 2018 discussed the potential and utility of telemedicine for individuals with MS, their families, and caregivers. However, this research was not systematic and did not focus on interventions in this field. Therefore, to the best of our knowledge, this SRMA will be the first of its kind, aiming to fill this gap and provide valuable insights into TIs for individuals with MS.8,46,47
Despite the widespread implementation of TIs targeting well-being and QoL in MS clinical trials, their overall effectiveness remains uncertain. Therefore, this review seeks to provide evidence-based insights into whether TIs can lead to positive outcomes for individuals with MS. By synthesizing and combining data from various research studies, this SRMA will contribute to the existing body of knowledge on TIs in MS. The comprehensive analysis of reliable data will offer valuable insights to professionals in health services, public health, and public policy. Such evidence will not only contribute to the development of efficient guidelines but also aid in the adoption of appropriate strategies for educational programs. Also, it will assist researchers, nurses, and clinicians in making informed decisions regarding the selection of efficient TIs tailored to individual MS outcomes.
Footnotes
List of abbreviations
Consent for publication
Not applicable.
Data Availability
No data sharing is required for this study as it is an SRMA that relies on existing data from clinical trials rather than generating new data.
Contributorship
RHS, MD, LS, TM, and RN made substantial contributions to the conception and design of the study, or acquisition of data, or analysis and interpretation of data. All authors were involved in drafting the manuscript or revising it critically for important intellectual content and gave final approval of the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content. RHS, MD, LS, TM, and RN agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
As this study is based on SRMA methods using existing clinical trial data, ethical approval was not required for this research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was part of a research supported by Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran (Grant No: 1401-4-160-63983).
Guarantor
LS.
Informed Consent
As this study is based on SRMA methods using existing clinical trial data, participant consent was not required for this research.