
Abstract
Objective
Smartphones are being used with increasing frequency to deliver behavioral interventions for depression via apps. However, barriers specific to using an app for depression are poorly defined. The purpose of the current study is to identify barriers to the use of a mobile app to deliver treatment for depression. Secondarily, design implications will be provided based upon identified barriers.
Method
A card sorting task that ranked and grouped barriers to the use of apps for depression was completed. Participants first completed a card sorting task identifying barriers to face-to-face treatment, as a primer to identification of treatment barriers. The sample consisted of those above (n = 9) and below (n = 11) the threshold for a referral to psychotherapy, to capture anticipated barriers for likely end users. Cluster analyses were conducted to analyze the card sorting data. Multiple analyses were conducted to identify: 1) the most important barriers, and 2) how consistently barriers were ranked as important.
Result
The card sorting task identified a number of primary barriers to the use of apps for depression treatment, including concerns over intervention efficacy, app functioning, privacy, cost, and lack of guidance and tailored feedback. The top face-to-face treatment barrier was cost, overlapping with mobile barriers.
Conclusion
This study identified perceived barriers to the use of mobile treatment apps. Identification of barriers implicates design recommendations for apps for depression.
Introduction
Depressive disorders are the leading cause of disability worldwide. 1 While efficacious treatments for depression exist, 2 multiple barriers interfere with the initiation and maintenance of face-to-face (i.e. traditionally delivered) treatments. 3 Therefore, to address this mental health epidemic, significant changes must be made in the strategy with which interventions are delivered. To extend care capacity, technologies are being integrated into multiple health care systems as a mechanism for delivering behavioral health interventions.4–6 The use of web-based delivery platforms has demonstrated efficacy across a broad range of mental health outcomes,7,8 however, barriers to this delivery method, such as needing to be in front of a computer, impact uptake and usage. 9 Consequently, a small, but growing body of research is examining the efficacy of smartphone apps to deliver behavioral interventions,10–14 as they offer the potential to provide a nearly continuous connection between a care system and patients.
As smartphones grow in popularity, their ability to serve as a delivery mechanism for behavioral health interventions with the potential to reach increasingly broad communities increases. Indeed, a growing number of people are becoming smartphone-dependent.15,16 Smartphone-dependency is defined as owning a smartphone, not having broadband internet access at home, and having limited abilities to access the internet outside of a smartphone. 15 Through their instantiation in smartphones, apps are ideally suited to be accessed by users in real-time and in real-world conditions, 17 likely overcoming many previously identified barriers to interventions delivered via face-to-face and computers.3,9 However, multiple issues exist. First, while there are some initial, promising mental health app outcomes,10–14 the efficacy of such apps remains primarily unknown. 18 Second, while apps may address many barriers to more traditional delivery mechanisms, they likely have unique barriers of their own. While barrier identification is secondary to the primary issue of efficacy, the quick turnover of technology and the ubiquity of mental health apps make this an issue worth exploring concurrent with ongoing efficacy trials.18–20 Indeed, identifying these barriers is critical to the success of future iterations of apps in delivering care to those with depression, particularly for those likely to face substantial known barriers to accessing traditionally delivered care.
Identifying barriers will allow us to make changes in the design of mental health treatment apps. For example, if concerns regarding efficacy of an app in addressing psychological symptoms is a barrier, design could shift to include providing specific psychoeducation at download, related to currently established and/or theoretical efficacy. However, without identification of such barriers, app designers must primarily rely on intuition. 21 This promotes a risk that design choices will create a mismatch with the needs or perceptions of the user for this delivery mechanism. Identification of barriers may therefore improve the information available for those who design and develop apps.
The means to identify barriers to the use of apps for depression may include a number of strategies, ranging from self-report questionnaires to moderated focus groups. However, a methodology that has been commonly used to inform multiple design processes and decisions is a card sorting task. 22 Card sorting tasks are designed as a means to categorize and organize variables and ideas. 23 Card sorting therefore enables the identification of potential end users’ perception of barriers to the use and uptake of apps for depression. To our knowledge, card sorting tasks have not been used previously as a means to identify barriers to use of mental health apps.
The purpose of the current study is to identify user perceived barriers to the initiation and maintenance of apps for depression. The aims of completing the card sorting tasks therefore are to: 1) identify perceived barriers to depression interventions delivered via apps and 2) identify overlap in primary barriers for intervention delivery via apps with traditional delivery methods (i.e. face-to-face) barriers. Implications for design changes and improvements that better align with the identified needs of the users will also be noted.
Method
Procedure
Recruitment of participants occurred from July to August 2015 from online postings in Chicago and nearby areas, resulting in the participation of 20 adults. Current recommendations for a card sorting task sample size is 15, 23 making the sample of 20 sufficient for the present study. Inclusion criteria were: being at least 18 years of age, the ability to attend an in-lab session, and ability to speak and read in English. Equal numbers of participants currently above and below the criteria for a referral for psychotherapy were recruited. 24 This sampling ensured that perceived barriers were being measured with likely end users, ranging from those with no or mild depressive symptoms to those with moderate or severe depressive symptoms. 25 Participants who completed the card sorting task, as well as an in-lab usability testing session were compensated $20 in petty cash for their time and participation. In compliance with the University’s Institutional Review Board (IRB), participants completed an online screening consent prior to the collection of any data and were consented in-person for the card sorting and usability testing session.
Card Sorting
To identify barriers to use and engagement with apps that are specific to users with depression, two separate card sorting tasks using open sort methods were employed. Open card sorting refers to providing participants topics and asking them to sort them into groups that make sense to them, as opposed to a closed card sorting in which the topics would be organized into predefined groups. 22 The first card sort was related to barriers to face-to-face delivery of interventions for depression, and the second was related to barriers to app delivery of interventions for depression. This order was chosen, as a concern was that if participants were asked to consider barriers to an app, they might not be familiar with the concept of an intervention app. If so, participants might identify barriers solely related to phone functionality (e.g. battery) or commonly used apps (e.g. Facebook). However, people are generally able to identify barriers to face-to-face interventions, and having participants first consider these barriers promotes consideration of intervention barriers. Barriers listed for both tasks were informed by findings from the literature and polls from content experts at the Center for Behavioral Intervention Technologies (CBITs).3,26 Barriers included issues related to typical depression intervention (e.g. concerns about stigma), technology-mediated delivery of care (e.g. data privacy), and app-specific (e.g. data plan) issues.
Prior to each card sorting task, participants were read the following prompt: I’m providing you with a stack of cards that have reasons that people might not want to or be able to (card sort 1: attend face-to-face therapy/card sort 2: use a mobile app for treatment) when feeling down. I would like you to go through the cards and choose the ones you think are barriers to (card sort 1: attending face-to-face therapy/card sort 2: using a mobile app for treatment). Once you choose them, please decide which ones are the biggest barriers. As you can see, the table is labeled to help you put ideas down from biggest barriers to smallest. You might notice that some overlap into groups in your mind; feel free to put them into groups. If there are cards you think do not apply, feel free to put them over here to be discarded. If there are cards with reasons missing, we can add more (indicate blank cards and marker). Please feel free to think aloud as you go through the cards.
Measures
Study data were collected and managed using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Northwestern University. 27 REDCap is a secure, web-based application designed to support data capture for research studies, providing 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources.
At screening, participants were asked to provide demographic information (i.e. gender, race/ethnicity, age, education and employment status). Further, they completed the Patient Health Questionnaire-9 (PHQ-9), a 9-item self-report instrument measuring depressive symptomology with scores ranging from 0–27. 25 Participants below the criteria for a referral to psychotherapy were defined as having a PHQ-9 score as below 10 (i.e. with no to mild depressive symptoms), whereas those meeting criteria for a referral to psychotherapy were defined as having a score of 10 or greater (i.e. with moderate to severe depressive symptoms). This criterion reflects the MacArthur recommendations for referrals to psychotherapy at the cutoff for mild depressive symptoms. 24
Data analysis
The card sorting task was analyzed via quantitative data; each card was assigned a number and then the mean rank for each card was determined for each participant. Consistent with past card sorting methodology, cluster analyses, a commonly used statistical method for grouping complex data, were conducted to analyze the card sorting data.28,29 For both the face-to-face and the app barrier cards, a hierarchical cluster analysis was conducted to determine the number of clusters appearing in the data set. This number was used to then conduct K-means cluster analysis to determine membership of cards within the different clusters. These analyses were conducted for the ranked means of the cards for both groups, as well as for the ranked means with the standard deviations for both card sets. Two analyses were conducted to: 1) identify the most important barriers (ranked means only to provide an indication of the average ranking of barriers); and 2) how consistently barriers were ranked as important (ranked means and standard deviations to provide an indication in the variance of ranked barriers).
Result
Participants
Card sorting sample characteristics.

Note. M = mean, SD = standard deviation, PHQ-9 = Patient Health Questionnaire-9.
Face-to-face delivery barriers
Face-to-face delivery barriers.
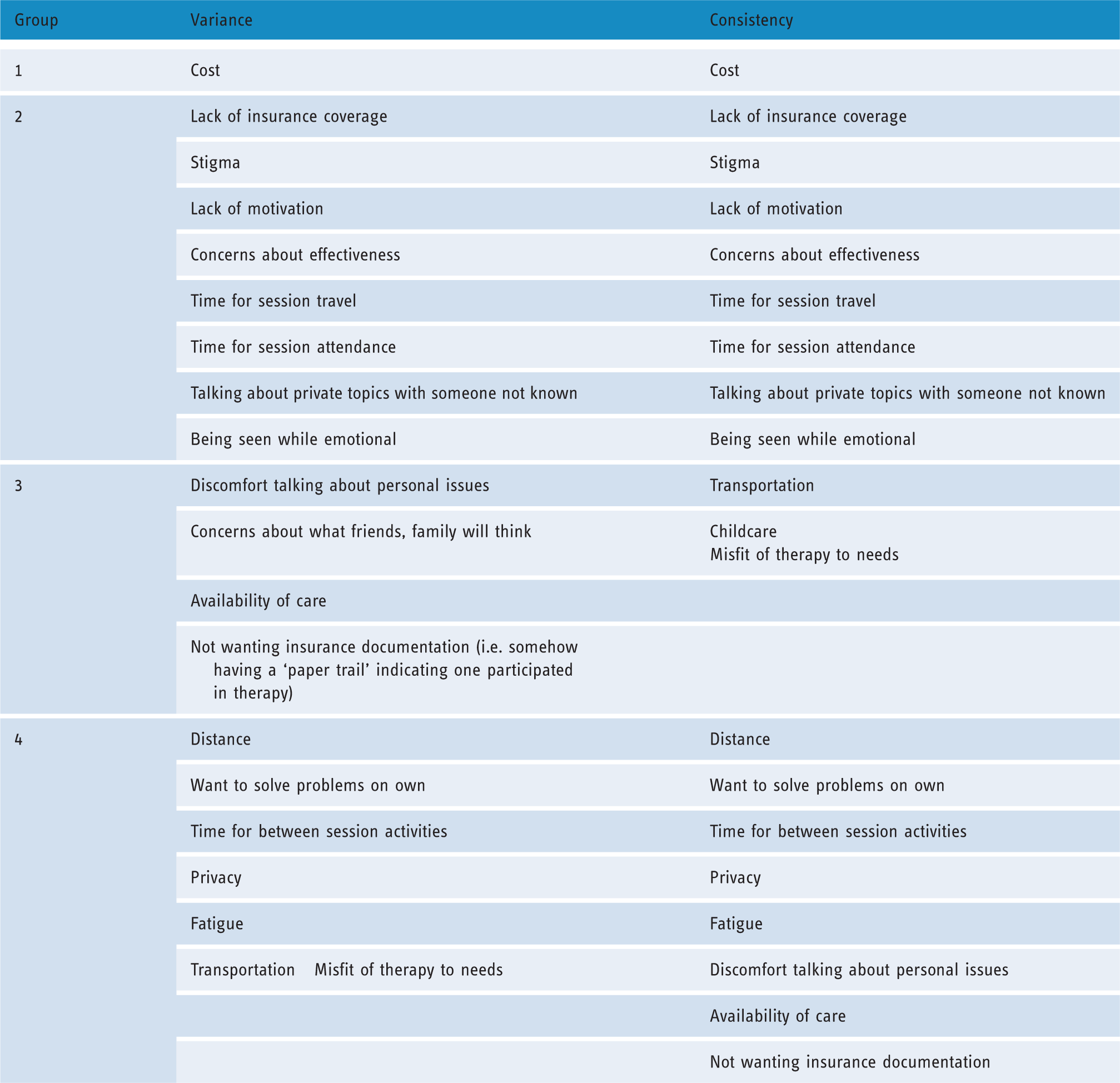
Note. Wording in table is identical to the wording the participants viewed on the cards. Groups are listed in order of greatest (1) to smallest (4) barriers. Variance represents clusters formed using mean ranks only (to indicate overall importance); Consistency represents clusters formed using mean ranks and standard deviations (to indicate consistency of importance).
App delivery barriers
App delivery barriers.

Note. Wording in table is identical to the wording the participants viewed on the cards. Groups are listed in order of greatest (1) to smallest (4) barriers. Variance represents clusters formed using mean ranks only (to indicate overall importance); Consistency represents clusters formed using mean ranks and standard deviations (to indicate consistency of importance).
Discussion
The present study identified user perceived barriers to face-to-face and app-based delivery of depression interventions via two card sorting tasks. Cost was consistently rated as the top barrier to face-to-face delivery, and top app barriers included concerns over intervention efficacy, app functioning, privacy, cost, and lack of guidance and tailored feedback. The common top barrier between the two delivery methods was cost, suggesting that this is a cumbersome barrier for users with depression, regardless of delivery mechanism.
Cost was identified as a top barrier for both delivery mechanisms, but it is unclear if the same meaning was associated with both mechanisms. Cost of therapy (i.e. cost of service) has previously been detailed as a primary barrier to initiation and maintenance of face-to-face delivered treatment. 3 Ancillary costs, such as paying for transportation and childcare have also been noted. 3 Qualitative feedback indicated that participants generally interpreted ‘cost’ as meaning the cost of service for face-to-face therapy. In apps, cost of apps (i.e. cost of service) has previously been suggested as an inhibiting factor in adaptation of mobile technologies in community health settings and across general health app consumers.30,31 Cost of apps has also been cited as a top user criticism in app user reviews. 32 However, participants identified the cost of data package (i.e. ancillary costs) as a primary barrier. This suggests that ancillary costs, which are possibly hidden or unclear to a user, are of greater concern than the cost of service. This shift in concern over cost is a difference between face-to-face and app delivery of interventions for depression. As apps are being designed and disseminated with an aim to overcome barriers to traditional intervention delivery mechanisms, overlaps in barriers with face-to-face interventions are particularly problematic. Cost appears to be a consistent concern across delivery mechanisms, however the focus appears to shift towards ancillary costs as opposed to service costs.
After cost, barriers to apps are related to user uncertainties around use of them as a delivery mechanism, such as data access and privacy, app functioning, guidance and efficacy. These findings are not surprising, given previous reports indicating that information about app privacy and theoretical efficacy are frequently not communicated to users. Indeed, the majority of privacy policies for currently available apps are missing, not focused on the app itself, or require college-level literacy for comprehension. 33 Additionally, a majority of health apps have been found to pose a threat to the security and privacy of user data.34,35 While current users of health apps generally report trust in their accuracy, 31 efficacy related to cultural and symptom-specific factors have also been cited as potential barriers or concerns about smartphone intervention uptake.36–38 Further, app functionality issues, such as errors and app crashes, have previously been identified as primary criticisms from general app users.32,39 The barriers identified through card sorting are consistent with previously raised issues and concerns from app users.
Among other barriers identified for apps, concerns emerged regarding a potential lack of guidance and feedback. This issue may overlap with a less primary barrier identified via the card sorting task: lack of human interaction. Integration of human support in health interventions delivered via technology has been recommended, and included in apps and other technologies, for the purposes of improving adherence, communication with care teams, and improving quality of tool use.40–42 However, the majority of currently available apps for depression do not include connection to human support, nor provide personalized guidance or feedback. 43 These findings highlight implications for design changes and improvements that better align with the needs and concerns of users.
Implications for design
Implications for the design of future apps for depression based on user perceived barriers.
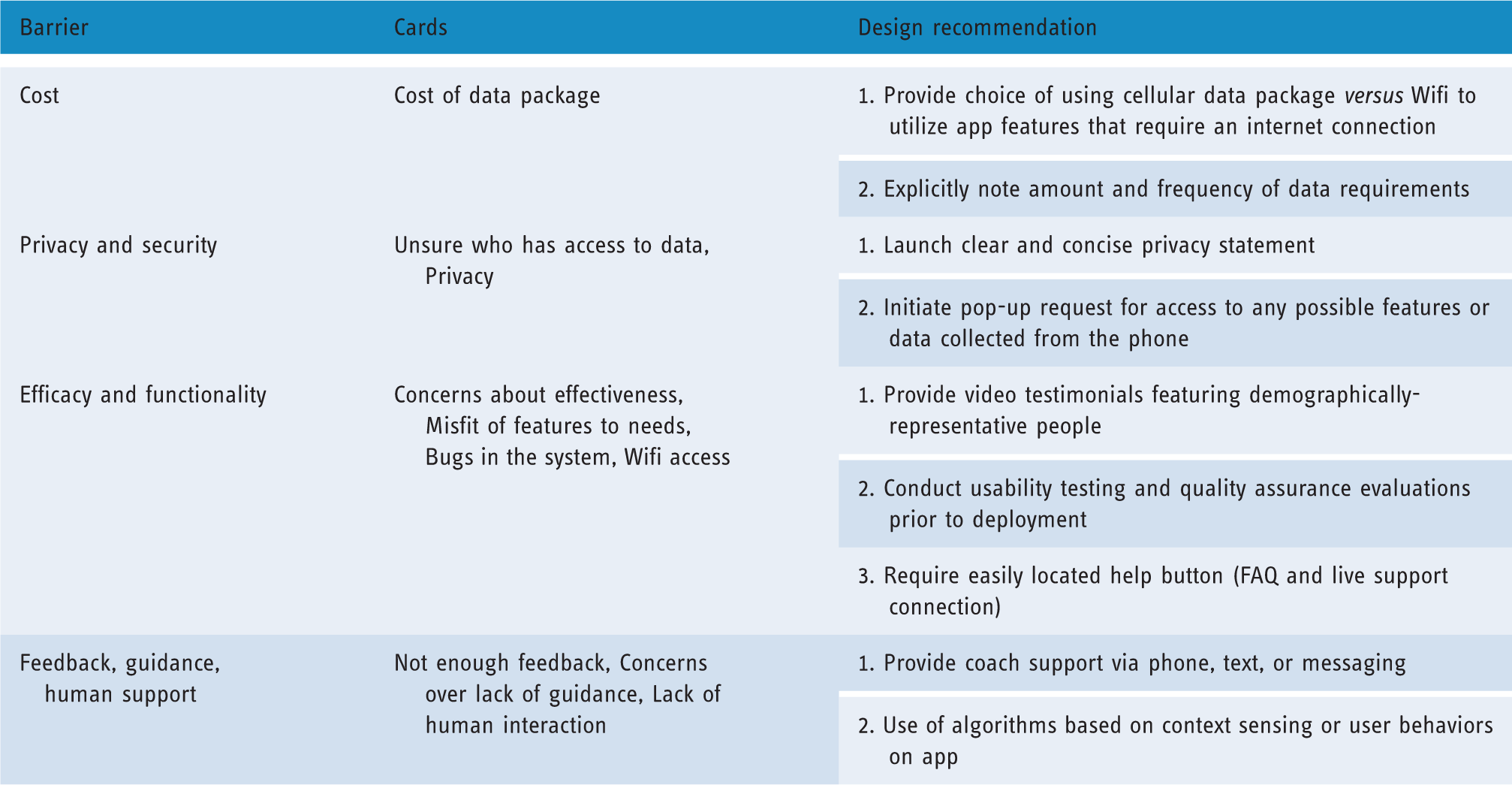
Note. FAQ = Frequently Asked Questions.
Limitations
Limitations and caveats should be considered in the interpretation of these findings. First, while the sample size was sufficient for a card sorting task, 23 the sample was comprised of urban and primarily younger, non-Hispanic Caucasian users. This is despite efforts to recruit a diverse, urban sample. It is unclear how well these findings extend to users in differing geographical locations and demographic groups. Future research might consider implementing purposive sampling methods to insure more diverse samples and may consider exploring barriers based upon other demographic features, such as age (i.e. younger users might face different barriers than older users). However, the process of identifying barriers with participants in an in-person setting was established as feasible. Second, the sample was a mixed group of those with no depressive symptoms to those with severe depression, with the majority in the mild symptom range. It is unclear if similar groupings of barriers would be identified with a more severely depressed sample, or those with comorbid psychiatric or health conditions. Despite concerns of generalizability to more severe samples, this sample represents the diversity of symptoms experienced across the typically relapsing and remitting course of depression.60–62 Third, it is possible that the participants inferred different meanings for the barriers listed on the cards. For example, the cards ‘Unsure who has access to data’ and ‘Privacy’ were typically ranked differently despite having similar meanings. While qualitative feedback was utilized to better understand rankings and groupings of the cards, future research utilizing card sorting to identify barriers would benefit from uniform definitions for each card. Additionally, as many barriers overlapped with typical concerns relating to technology broadly as a delivery mechanism, future research might explore barriers targeted specifically to apps. Indeed, the present study included barriers associated with depression treatment (e.g. stigma) and issues associated with broad use of technology as a delivery mechanism. 63
Conclusion
To the best of our knowledge, this is the first identification of user-perceived barriers to apps via a card sorting task. Smartphones stand as a promising delivery mechanism for overcoming barriers to traditional delivery of depression interventions. However, while there is some promising initial evidence for the efficacy of apps as a behavioral intervention delivery mechanism,10–14 a larger evidence base is required. In terms of barriers to uptake and use, cost remains a consistent barrier across face-to-face and app delivery of interventions. Other barriers to the use of apps for the delivery of depression interventions relate to uncertainties around apps as a technology mediated delivery mechanism. Implications for design to address these barriers include: limiting wireless data usage; clearly stating possible costs and privacy/access options at download, including demographically-representative video testimonials; conducting usability testing and quality assurance evaluations; and including human support. Future research should evaluate the impact of changes in design and marketing of mental health apps on perceptions of barriers for users with depression.
Footnotes
Contributorship
CSS researched the literature and conceived the study. CSS and EGL executed the research sessions. CSS wrote the first draft of the manuscript and EM, EGL, MJK, and DCM contributed to later drafts. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This research was approved by Northwestern University’s Institutional Review Board (IRB STU00099556).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health (F31 MH106321). This project was also supported by NIH/NCRR Colorado CTSI Grant Number UL1 RR025780. Its contents are the authors sole responsibility and do not necessarily represent official NIH views.
Peer review
This manuscript was reviewed by Anne Moen, University of Oslo and Vivek Furtado, University of Warwick.
Guarantor
CSS