
Abstract
Objective
On the way to a modern digital healthcare system, Germany becomes a driver of innovation by integrating digital health applications (Digitale Gesundheitsanwendungen (DiGAs)) into standard care. Although all insured persons of the statutory health insurance are eligible for a registered DiGA, utilisation has been rather restrained so far. There seems to be a lack of acceptance among healthcare providers. The aim of this study is to analyse the acceptance of DiGAs in non-pharmacological therapies.
Methods
A total of 150 therapists from the fields of physical therapy, occupational therapy, and speech-language pathology participated in an online survey. The questionnaire captured knowledge, intention to use, opinions on advantages and disadvantages of DiGA usage as well as general technology acceptance and commitment.
Results
About 36% of the therapists knew DiGAs, while about 64% had not yet heard of these offers. In addition, 87% of the respondents can imagine integrating DiGAs into their treatment or were already doing so at the time of the survey. Potentials for using DiGAs are seen especially in the quality improvement of therapy, in the increase of the sustainability of the therapy and in promotion of patients’ health literacy. The therapists stated barriers in the lack of technical infrastructure and in the patients’ insufficient digital health literacy.
Conclusion
The results indicate the potential for DiGAs to be further implemented in non-pharmacological therapies. The facilitators and barriers identified allow recommendations to be derived for relevant stakeholders.
Keywords
Background
Digitalisation is increasingly making its way into everyday life. In the course of medical-technical progress, innovative treatment and therapy options are constantly emerging in the healthcare sector. One of these innovations are digital health applications (Digitale Gesundheitsanwendungen (DiGAs)). Patients are assisted by these ‘apps on prescription’ in the detection, monitoring, treatment or alleviation of diseases, injuries or disabilities. A digital health application is defined as a medical device of a low risk class I or IIa, according to the Medical Device Regulation of the European Union. Moreover, the main function of the DiGA must be based on digital technologies and the medical purpose must be achieved through the main digital functions. Those websites, apps and wearables are either used only by the patient or shared between the patient and the healthcare provider. 1
In order to catch up internationally regarding digitalisation, Germany is now taking a pioneering role in the implementation of digital health applications in public healthcare. Therefore, the Digital Healthcare Act (Digitale-Versorgung-Gesetz (DVG)) came into force in Germany in January 2020. The DVG allows insured persons of the statutory health insurance (SHI) access to DiGAs. For this purpose, an innovative procedure, the Fast Track process, was developed, which is particularly attractive for manufacturers, as a decision on reimbursement within the framework of standard care will be carried out within three months. In the course of the Fast Track process, it is assessed whether the digital health application meets certain requirements regarding security, functionality, quality, data protection, data security and interoperability. 1 Additionally, a positive care effect must be proven. Therefore, either a medical benefit or a structural and procedural improvement must be demonstrated. To prove the positive care effect manufacturers must carry out at least one comparative study, demonstrating that implementing the DiGA in standard care is better than not using it. Therefore, an intervention group – using the DiGA – must be compared to another group, which can either be standard care, non-treatment or treatment with another, comparable DiGA, that is already listed in the DiGA directory. The choice of the comparison group must be oriented towards the reality of healthcare. The minimal requirement regarding the study design is a retrospective comparative study, but the manufacturers can always choose to carry out a prospective comparative study with a higher level of evidence. In view of the upcoming price negotiations, 78% of applicants so far carried out a randomised controlled study, thus generating a better negotiating position. 2 The final approval is granted by the Federal Institute for Drugs and Medical Devices (Bundesamt für Arzneimittel und Medizinprodukte (BfArM)). Once the requirements are met and the positive care effect is proven successfully the digital health application will be listed in the DiGA directory (https://diga.bfarm.de/de/verzeichnis) and can therefore be prescribed by physicians and psychotherapists for members of the SHI. If by the time of application, the positive care effect cannot be demonstrated, the DiGA can be provisionally listed for one year, in which the manufacturer must conduct further research to provide the necessary evidence. After this time the DiGA will be reassessed and either will be listed permanently or will be excluded from the directory.
Digital health applications still play a minor but growing role in daily healthcare in Germany. Currently, 34 apps and web applications (status: 15 October 2022) are registered in the DiGA directory, which is a requirement for being reimbursable. 3 The apps already listed have so far only been used by a small proportion of those insured by SHI in Germany. A survey, published in February 2021, shows that with the involvement of 18 SHIs funds – referring to 61 million insured – around 3000 DiGA have been reimbursed so far. 4 This development in the primary healthcare market contrasts with the high level of willingness to use and the great interest in digital solutions that can already be observed in the secondary healthcare market. Currently, around half of German smartphone users are interested in and already use comparable digital solutions that did not yet undergo the Fast Track process. 5 However, surveys among physicians authorised to prescribe DiGAs show that there is a great deal of scepticism, especially regarding data protection, the motivation of patients, and the effectiveness and evidence of these products. 6 Thus, only 37% of the physicians state in April/May 2020 their willingness to prescribe was high. 7 In addition, 10% of physicians were not even aware of these products in November 2020. 8 Another online survey of 585 physicians and psychotherapists, conducted from September to November 2021, states that only 7.2% have used a DiGA at least once and only 1.7% regularly. 9 Overall, however, it can be stated that due to the novelty of the Fast Track process and the so far hesitant use of DiGAs in standard care, the evidence situation is deficient.
Besides the physicians and psychotherapists, who are allowed to prescribe DiGAs to their patients, other healthcare professionals such as physical therapists, occupational therapists, and speech-language pathologists are also a relevant stakeholder group, as their activities are supported, supplemented and partially replaced by the applications. So far, the opinions of these therapists regarding the integration of DiGA into non-pharmacological therapy as well as possibly existing barriers have not been surveyed. Also, the manufacturers do not address those professional groups so far with their measures to implement DiGAs into standard care, even if their DiGA is an online physiotherapy. Considering that there are patients who have a close relationship with their therapist, spending more time with the therapist than with the treating physician, the exclusion of these healthcare professionals seems surprising. Particularly in view of the fact that patients with a suitable diagnosis can also receive a DiGA directly from their SHI, without a prescription from their physician, therapists could possibly have an important role in the implementation of DiGAs into standard care.
The objective of this study is to determine the opinion of therapists regarding DiGAs and its use in non-pharmacological therapies. Therefore, physical therapists, occupational therapists, and speech-language pathologists are surveyed. Particular attention is paid to barriers and facilitators of the implementation of DiGAs in order to derive recommendations for key stakeholders.
Methods
A cross-sectional study was conducted as a ten-week online survey between March and June 2021. The target group included physical therapists, occupational therapists, and speech-language pathologists in German inpatient and outpatient settings. Recruitment was conducted primarily via therapist associations, followed by requests for participation in relevant forums, for example, in social media. Prior to the study, participants were informed about the scope of the study, the voluntary nature of the survey, the risks and benefits as well as the procedures to maintain anonymity and confidentiality. An agreement to this consent document was necessary for proceeding with the questionnaire.
The survey consisted of a mixture of self-constructed items, asking for sociodemographic characteristics, knowledge of DiGAs and the intention to use DiGAs, as well as standardised questionnaires. One standardised questionnaire was the short scale of technology commitment. 10 According to this theory, technology commitment is composed of technology acceptance, technology competence and technology control, analogous to the subscales of the questionnaire. A score can be summed up with possible values between 0 (low technology commitment) and 60 (high technology commitment). In addition, participants' technology acceptance was assessed using a questionnaire adapted from Hennemann et al. 11 , which is based on the Unified Theory of Acceptance and Use of Technology. 12 The main element of this theory is the behavioural intention to use a new technology. This behavioural intention is influenced by the subscales of social influence, facilitating conditions, performance expectancy, and effort expectancy. The technology acceptance questionnaire consists of ten statements, for each of which the respondents indicate on a five-point Likert scale how much they agree. A high level of approval means better technology acceptance. In total, the questionnaire comprised 24 to 30 items depending on the answers to the filter questions. The items were operationalised as closed single- or multiple-choice questions. The items of potentials and barriers of DiGA, technology acceptance, and technology commitment were answered on a five-point Likert scale ranging from 1 – ‘totally disagree’, 2 – ‘rather disagree’, 3 – ‘neither’, 4 – ‘rather agree’ to 5 – ‘totally agree’. For the interpretation of the results, scores were dichotomised whereby a conservative approach was taken and ‘neither’ was counted as disagreement.
When conducting the survey 11 to 15 applications had been listed as approved DiGA, out of which one app focused mainly on physical therapy for patients with unspecific back pain and up to five other DiGAs included elements of physical therapy, occupational therapy, or speech-language pathology. It was expected that most participants would be familiar with at least some fitness and lifestyle applications in their profession, as there was a broad offer of comparable medical device apps with business-to-consumer business models already on the secondary healthcare market. While at the same time it was expected that the majority would not yet be familiar with the Fast Track process, the DiGA directory and the specific requirements resulting from this. Therefore, a profession-specific flyer introducing a fictional DiGA was integrated into the survey at the beginning of the questionnaire. The flyer was orientated on DiGAs already listed or, alternatively, on medical device apps that could possibly pass the Fast Track process in the future. The flyer pointed out a description of the exemplary app and in keywords its potential when integrated into non-pharmacological therapy. It was demonstrated when and how the app could be used and three drawings of the fictional user interface were shown in the flyer. Additionally, the framework conditions arising from the Fast Track process that differentiate DiGAs from conventional fitness and lifestyle apps were presented, for example, that the DiGA is a certified medical product and costs will be reimbursed by the SHI. A pretest of the survey was conducted with ten participants from all professional groups as well as tech-savvy and tech-shy individuals. The pretest served to check the plausibility of the questionnaire and the comprehensibility of the items. By programming the questionnaire with the online survey application LimeSurvey, 13 inconsistencies in the data could be avoided.
The analysis was performed using the free programming language R Studio. 14 No imputation of missing values was performed due to the rare occurrence and the partial lack of standardisation of the questionnaire. At first, the characteristics of the study population were examined by reporting absolute and relative frequencies for categorical data, as well as the arithmetic mean and standard deviation for numeric items. In addition, knowledge, usage behaviour and intention to use as well as barriers and facilitators were analysed descriptively. Based on various sociodemographic characteristics, knowledge, usage behaviour, and the intention to use different subgroups were formed. Subsequently, the post hoc subgroups were tested for significant differences by means of a frequency analysis. Depending on the scale level of the item, the distribution between the groups was compared using either a Pearson chi-squared test or the Mann-Whitney U-test. The significance level was set to α = 0.05.
Results
In total, 150 therapists participated in the survey. Of the respondents 46.0% (n = 69) were physical therapists, 38.7% (n = 58) occupational therapists, and 12.0% (n = 18) speech-language pathologists. Most therapists worked in an outpatient setting (62.7%, n = 94) and the average work hours amounted to 32.4 h (SD = 11.0 h) per week (see Table 1). The sample was mainly female 78.7% (n = 118). The average age was 38 years (SD = 11 years), whereby more than half of the participants (59.3%, n = 89) had more than ten years of professional experience.
Sociodemographic characteristics of the study population.

n: amount; %: percentage.
DiGAs were already known by 36.0% (n = 54) of the respondents. This distribution did not differ significantly between professions (χ2 = 1.2863, df = 2, p = 0.526). In addition, 33.3% (n = 18) of those who knew DiGAs were also aware of the DiGA directory. Regarding the usage behaviour of the therapists, it was found that 11 persons (7.3%) had already used DiGAs in therapy. However, when subsequently asked about the app used, only one listed DiGA was named, while the others mentioned additional eHealth tools such as organisational aids, video therapy, and wearables. In the future, 80.0% (n = 120) of the respondents could imagine using DiGAs in their treatment. In summary, a total of 131 healthcare professionals (87.3%) indicated a positive intention to use, as they either stated they already use DiGAs or could imagine doing so in the future (see Table 2).
Therapists’ opinion on integrating DiGAs in non-pharmacological therapy.

DiGA: Digitale Gesundheitsanwendung (digital health application); SHI: statutory health insurance; DVG: Digitale-Versorgung-Gesetz.
*Significant difference α < 0.05.
Potential in the use of digital healthcare solutions was seen particularly in improving the quality of therapy (86.7%, n = 130), in promoting the health literacy of patients (84.0%, n = 126), and in improving the sustainability of therapy (82.7%, n = 124). Likewise, respondents appreciated the apps’ ability to provide therapy regardless of time or location (88.7%, n = 133). In addition, the respondents recognised an advantage in the fact that DiGAs are part of the SHI system and thus costs are reimbursed (85.3%, n = 128). Fewer benefits were seen in improving communication with patients (48.7%, n = 73) or increasing the patient therapy adherence (38.7%, n = 58).
The therapists expected challenges in the lack of technical equipment in the therapy centres (59.3%, n = 89), which will lead to technical problems (56.7%, n = 85). Both items regarding the technical equipment did not differ significantly between therapists working in rural and urban areas (χ2 = 1.7425, df = 3, p = 0.628 & χ2 = 3.9898, df = 3, p = 0.263). Additionally, therapists anticipated that patients use DiGAs incorrectly and errors will occur while training with the app (62.7%, n = 94). One-third of the respondents expected their patients to be overwhelmed with the DiGA use (28.7%, n = 43). Therapists themselves rarely reported being overwhelmed with using DiGAs (6.0%, n = 9) or not knowing how to use them (14.7%, n = 22).
In the subgroup analyses on barriers and facilitators, it appeared that therapists who know DiGAs were significantly less likely to agree that errors occur during patient training with the DiGA (χ2 = 8.6025, df = 1, p = 0.003). Subgroup analyses between persons who already used a DiGA or plan to do so in the future and persons who declined DiGAs, revealed multiple significant differences in the agreement to given potentials and barriers of DiGAs. Therapists who favour DiGAs generally agreed on most items significantly more with the advantages and significantly less with the disadvantages than therapists who opposed DiGAs. No significant difference could be seen in the statements that DiGA use leads to technical problems (χ2 = 1.4218, df = 1, p = 0.233) that the required technical equipment is not available (χ2 = 0.000, df = 1, p = 1.000), and that the patients' affinity for technology is insufficient (χ2 = 0.000, df = 1, p = 1.000). In addition, proponents and opponents alike indicated uncertainty about the risks and liability associated with DiGA use (χ2 = 0.2320, df = 1, p = 0.630). The only advantage of DiGAs that did not significantly differ between proponents and opponents was the statement that DiGA use can reach new patients (χ2 = 2.1615, df = 1, p = 0.142).
For technology acceptance (see Table 3), the average behavioural intention score was 3.5 (SD: 1.0). Overall, 60.7% (n = 91) of the sample had a score higher than 3.0 ‘neither’, indicating a positive behavioural intention. In particular, the effort expectancy, operationalising the effort required to implement DiGAs into daily therapy, was rated as feasible (4.3 points). This also applied to the benefits derived from using DiGAs, as seen by 4.1 points for the subscale performance expectancy.
Technology acceptance of the sample.
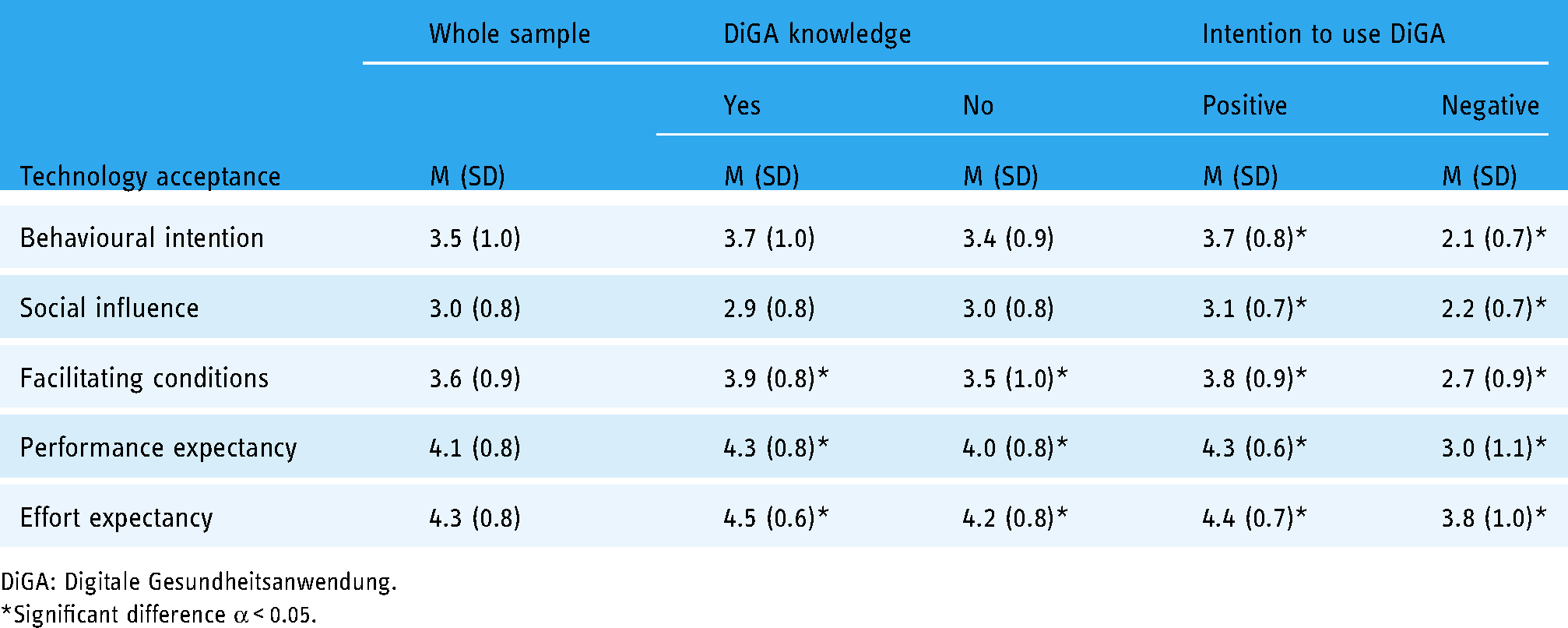
DiGA: Digitale Gesundheitsanwendung.
*Significant difference α < 0.05.
In terms of technology commitment, technology competence was the highest subscale with 17.2 points and the overall score average was 45.8 points out of a possible 60 (see Table 4). Therapists who stated a positive intention to use DiGAs or therapists with DiGA knowledge had a significantly higher technology acceptance than persons who rejected (W = 1537.5, p = 0.036) or did not know about DiGAs (W = 1922.5, p = 0.009).
Technology commitment of the sample.

DiGA: Digitale Gesundheitsanwendung (digital health application).
*Significant difference α < 0.05.
Discussion
To our knowledge, this online survey is the first research project to examine the publicity of and opinion about DiGAs out of the perspective of therapists in non-pharmacological therapies. Results show that most participants are not aware of DiGAs. In general, the willingness to implement digital health applications in therapy in the future is high. By using DiGAs, therapists mainly expect benefits, for example, quality improvements of therapy. Nevertheless, the survey identified current barriers that hinder a broad implementation of DiGAs in standard care, such as the lack of technical infrastructure or the insufficient digital health literacy of the German population.
According to official statistics, nearly 333,000 therapists were working in non-pharmacological therapies in 2018, of which 60.7% were employed in an outpatient setting. 15 The proportion of therapists in an outpatient setting in this study is 62.7% and therefore matches the official statistics. With 72.1% the majority of healthcare providers in 2018 were physical therapists, followed by occupational therapists with 18.9% and speech-language pathologists with 9.0%. 15 This distribution is also reflected in the current survey. Furthermore, predominantly women (84.3%) work in these professions. 15 The majority of respondents in the online survey are women too (78.7%). Therefore, certain characteristics of the sample are comparable with data from official statistics of the German healthcare system, so that the study population appears to be representative for the target population.
One important result of the survey is that there is a lack of information among therapists regarding DiGAs as well as new DVG regulations. For example, only 36.0% of respondents are aware of DiGAs and only 12.0% know the DiGA directory. This information deficit does not differ significantly between professions, suggesting that regardless of the existence of digital health applications for specific therapy, there is a lack of awareness of DiGAs amongst therapists. Accordingly, it is up to relevant stakeholders to provide therapists with information about DiGAs and DVG in order to reduce the information deficit. However, the responsibilities between SHIs, medical associations and DiGA manufacturers do not seem to be clear at this point, which is why no one has fulfilled this obligation so far. 16
Compared to physicians, therapists are less likely to have knowledge of DiGAs. A survey of 528 physicians of all specialities in inpatient and outpatient settings carried out in November 2020 found that one in ten physicians does not know what a DiGA is, 8 while in this survey six out of ten therapists do not know what a DiGA is. This result is not really surprising, because physicians are allowed to prescribe DiGAs and are therefore more likely to be confronted with these offers than therapists, who have so far had a rather accompanying role. In addition, the hesitation of physicians to prescribe DiGAs does not contribute to other health professionals' awareness of digital health applications. The first reports of the SHIs 4 can be confirmed, as this survey showed that only one therapist has used a DiGA in therapy so far. DiGAs have not yet arrived in daily care and certainly not as an adjunct in non-pharmacological therapies.
The lack of knowledge among therapists may also be related to the limited DiGA offer, as only a few applications were listed in the DiGA directory at the time of the survey. One of the reasons for the slow start of the DiGAs is the extensive requirements a digital health application must meet in order to be reimbursed via the Fast Track process. Many manufacturers withdraw their applications to revise them, as they otherwise expect rejection by the BfArM. At the moment (status: 12 October 2022), 83 out of 151 applications have been withdrawn. 3 However, with increasing experience in the Fast Track, a broad expansion of the offer can be expected. A survey of approximately 300 drug and medical device manufacturers found that more than half of these companies have already developed or plan to develop digital healthcare applications. 17
Despite the knowledge gap the willingness to use DiGAs is 87.3% clearly higher. This suggests that therapists, even without being enabled to prescribe DiGAs themselves, are nevertheless a relevant target group. They can play a key role in encouraging patients to use DiGAs. In particular, considering the possibility that patients with a relevant diagnosis are able to receive access to a DiGA directly from their SHI without a prescription from a physician. Consequently, involving other healthcare professionals, such as therapists or nurses, in promoting a digital health app can be successful.
The great interest of the therapists in using DiGAs is reflected in the participants’ perceptions of the facilitation and benefits of DiGA implementation. Thus, on average, the respondents agree significantly more with statements about facilitators than with statements about barriers. However, respondents do not assume that all patients will equally benefit from the use of DiGAs. For example, therapists expect greater benefits from the DiGA use for specific patients in terms of improving treatment quality and improving treatment adherence than for the whole patient cohort, for example, persons of a certain age group or with a certain severity level. To ensure an efficient implementation, it is important to provide DiGAs only to those patients who are likely to benefit from them and who will actually use them. Thus, three factors can be defined for the long-term success of DiGAs in standard care 18 : (1) There must be a wide range of patients for whom medical benefit can be expected from the use of DiGAs. (2) DiGAs need to achieve a high level of user acceptance, which requires good usability. (3) The cost-effectiveness ratio of DiGAs should be continuously reviewed in the future, especially through real-world evidence studies.
Another major advantage of DiGAs is seen in the statement that they promote patients’ health literacy, as 84.0% of the sample agree with this statement. In the German population, 58.8% have low health literacy, especially persons over 65 years of age and those with chronic, sometimes multimorbid diseases. 19 For this reason, experts recommend strengthening the digital sovereignty of older people and adapting the development of digital technologies to the competencies, needs and requirements of older people. 20 This results in a need for action by policymakers to promote and improve the digital health literacy of the population, especially for vulnerable groups. With the DVG coming into force, policymakers have transferred this task over to the SHIs, which are now obliged to offer programs to promote the digital health literacy of the insured (§20k SGB V).
Besides the inadequate digital health literacy of the patients, 61.3% of the respondents assume that the patients' affinity for technology is insufficient for DiGA use. Therapists’ own technology competence is estimated better. Additionally, therapists perceive the greatest disadvantage of DiGA use to be the potential for errors to occur during patient training (62.7% agreement). However, errors that occur when patients train on their own can never be completely ruled out, even without digital assistants, which is why regular monitoring by the therapist is important. It is therefore necessary to consider to what extent DiGAs can replace an in-person therapy, or whether a supplementary or partial replacing use is preferable.
In the aspect of whether the therapists are relieved in their daily treatment routine by the DiGA use, the sample is divided into opinions. This shows that the implementation of newer technologies is often initially associated with hurdles and additional effort before these technologies provide meaningful support and facilitate daily business. According to the indications in the technology acceptance questionnaire, where the effort expectancy subscale is rated the highest with an average of 4.3 points out of 5 points, therapists expect the implementation of DiGAs into therapy as feasible.
Another challenge in the use of DiGAs is seen by the therapists in the comprehensive, technical implementation. Thus, 59.3% of respondents agree that the required technical infrastructure is not available. Similarly, 56.7% anticipate technical problems with DiGA use. These items, unlike most of the other statements, do not differ significantly from each other in any of the subgroup analyses, which indicates that the challenge of technology is seen equally by the therapists. Technical challenges are expected independent of whether therapists approve or disapprove DiGAs. Particularly in rural areas, the nationwide availability of broadband in Germany remains problematic, resulting in the need to expand the infrastructure. 21 By the end of 2020, only 80.9% of the 4.4 million households in rural areas in Germany had broadband availability of more than 50 Mbit/s. 22 Policymakers have recognised this need and are therefore promoting the expansion of broadband, especially in rural regions. In the present survey, however, therapists in rural and urban areas alike state that there are technical challenges.
Regarding the technology acceptance of the sample, the results of the opinion survey on facilitators and barriers to DiGA use are confirmed, which is shown by the high score in the performance expectancy subscale. The high score in the effort expectancy subscale implies a sufficient digital competence of the therapists to implement DiGAs. The fact that DiGA knowledge is still insufficient is confirmed indirectly by the comparatively low score in the subscale social influence, since therapists state to not feel pressured by colleagues or patients to start using DiGAs. This indicates that most patients do not know about DiGAs either. Still, in the future, DiGAs are expected to be increasingly requested by patients as this is a typical development for digital innovations. For the majority of the German population, it is now normal to use online banking, to buy transportation tickets via app and to shop online. These applications, analogous to the DiGAs, took some time to integrate into the daily life of people. The growing interest in DiGAs can also be observed in a recent report by the German National Association of Statutory Health Insurance Funds (Spitzenverband der Gesetzlichen Krankenkassen (GKV-SV)), which indicates that the use of DiGAs increased steadily in the first half of the year 2021. By September, a total of 50,112 DiGAs had been prescribed by physicians and psychotherapists or approved by the health insurance companies, of which 78.5% were redeemed during this period. 23
The results of the technology commitment scale show once again that a generally high technology acceptance is a predictor of DiGA knowledge and a positive intention to use DiGAs. This is confirmed by the significant differences in the subgroup analyses. Therefore, tech-savvy persons are likely to be the first users of DiGAs and by doing so they will become role models for their colleagues and patients.
Generally, there are some limitations in this survey that should be considered when interpreting the results. (1) As standardised and validated, DiGA-specific measurement instruments have not been developed so far, often self-developed questions had to be used in the questionnaire, which may have led to restrictions on the reliability and validity of the results. (2) In order to address the expected lack of knowledge regarding DiGAs, a profession-specific flyer introducing a fictional DiGA and the most important regulations resulting from the DVG was included in the survey. On the one hand, this was necessary to ensure that the answers of the participants are valid. On the other hand, this could have influenced the respondents’ perceptions, as possible advantages of DiGAs and the accessibility via the Fast Track procedure were presented. (3) Additionally, the division of the sample into different subgroups resulted in small sample sizes in some cases. Therefore, these results have to be evaluated rather exploratively. (4) Due to the cross-sectional design only a snapshot of the knowledge, the intention to use and the therapists’ opinion on DiGAs could be recorded. In the future, it is therefore advisable to conduct further surveys in order to gather more experience and to monitor the development over time in the context of a broader DiGA offer and increasing implementation of DiGA in everyday non-pharmacological therapy.
Conclusion
The results of the study indicate that an increased implementation of DiGAs in non-pharmacological therapies is possible. The interest of the therapists is high, and they tend to expect more benefits in the DiGAs use than barriers. Nevertheless, the prerequisites must first be improved, such as the technical infrastructure or the level of information about DiGAs among healthcare providers and patients alike. A more diverse range of products is also likely to promote the implementation of DiGAs in standard care.
Footnotes
Acknowledgements
The authors like to thank all participants of the survey.
Contributorship
SF and LK researched literature and conceived the study. SF carried out the programming of the questionnaire, and the data analysis and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
According to the guidelines of the German Research Foundation (Deutsche Forschungsgemeinschaft) no ethical approval was necessary, because no patients or vulnerable groups were involved in the study. Participation in the anonymised survey was voluntary and informed consent was a necessary requirement.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Informed consent
The informed consent was given online preliminary to the survey.
Trial registration
Not applicable, because this study does not contain any clinical trials.
Guarantor
SF.