
Abstract
Objective
mHealth is increasingly becoming popular and useful for managing chronic diseases. Nurse-led mHealth services offer a patient-centred perspective, but many existing solutions lack a robust empirical foundation. Therefore, this study aimed to address this gap by developing a comprehensive framework to support mHealth implementation through a systematic review and the Delphi method. Specifically, the study sought to create a nurse-led mobile health (mHealth) intervention framework designed for managing patients with chronic diseases.
Methods
We conducted a systematic review of PubMed, Web of Science, Cochrane Library, CNKI, and Wanfang databases to identify existing nurse-led mHealth intervention programs. Items from these articles were compiled into an inclusion list, and the Delphi method was applied to rank their priority. The Delphi process involved 13 nursing specialists and was conducted over two rounds using a Likert priority scale (1–5) to establish consensus.
Results
Based on the systematic review (included 16 articles for full review) and study group contributions, 36 potential framework items were identified. In the initial round of the Delphi study, specialists rejected 7 of the 36 items and recommended merging 6. In the subsequent round, the specialists recommended removing the self-monitoring diet items. The final items were consolidated into a 22-item nurse-led mHealth intervention framework categorized into three domains: pre-hospital evaluation, in-hospital intervention, and post-hospital continuity.
Conclusions
The Delphi-approved items offer a basis for evidence-based nurse-led mHealth intervention frameworks. These findings highlight the need for an intervention framework and its practical integration into the existing mHealth system.
Introduction
Chronic diseases significantly affect populations in both developed and developing countries, contributing to global mortality and disability.1,2 Effective management of chronic diseases is essential for enhancing health outcomes, improving quality of life, and achieving cost efficiency. 3 Managing chronic diseases requires prolonged and continuous monitoring, which has catalyzed the early development of telehealth and telemonitoring technologies. 4 Advances in technology have accelerated the emergence of mobile health (mHealth) services. 5 mHealth interventions have significantly improved chronic disease care by providing access to electronic health records, applications, and patient health portals. 6
Chronic disease depletes a family's financial and emotional resources more rapidly than any other expense. 7 Managing chronic diseases such as cancer, diabetes, cardiovascular, and pulmonary conditions imposes a significant financial burden, frequently necessitates lifelong care, and typically exhibits progressive deterioration over time. 8 In addition to managing various diseases related to diet, exercise, and adherence to prescribed medications, patients navigate intricate communication dynamics with family members and healthcare providers. Thus, intervention frameworks that support long-term health behavior change are essential for preventing further disease progression and improving patients’ quality of life.9,10
MHealth is a significant and efficacious intervention strategy, as defined by the World Health Organization as “applying mobile and wireless technologies to facilitate the attainment of health goals.” 4 mHealth operates in diverse environments and involves various healthcare professionals, with nurses playing a vital role in most mHealth services. 11 As frontline providers, nurses play an important role in managing patients with chronic diseases and helping patients in continuous disease management. 12 Given the increasing demand for mHealth, nurses must be prepared to support mHealth and integrate it into the healthcare system. 11 Studies have found that patients exhibit higher satisfaction and better adherence to treatment protocols when guided by nurse-led interventions compared with management solely by medical professionals.13,14
Several factors influence engagement with mHealth, including access to computers, technological shortcomings, adherence to treatment, and a lack of interest in participating in healthcare delivery.4,15 A systematic review of mHealth for chronic noncommunicable diseases summarizes recent research and highlights the challenges in this rapidly developing field. 16 One major issue is the need for enhancing the methodological quality of mHealth studies. Conducting high-quality, low-bias research can establish the effectiveness of interventions and provide recommendations for research and clinical practice. 17 Incorporating clinical feedback into mHealth interventions is another challenge, which can enhance personalized health services. However, this often requires significant support from health professionals, which may be hindered by organizational constraints. 18 To achieve the best interests of patients with chronic diseases and healthcare systems, developing scientifically grounded, nurse-led mHealth intervention frameworks is important.
Approaches to nurse-led mHealth interventions and the requirements for their implementation are both common and individualized and vary according to disease conditions. Although the acceptability and feasibility of mHealth interventions for chronic diseases, including rare diseases, have been demonstrated, most mHealth interventions designed for chronic diseases are insufficiently supported by empirical evidence.19,20 Therefore, this study aimed to establish a comprehensive, practical, evidence-based, nurse-led mHealth intervention framework for managing patients with chronic diseases. This article is presented in accordance with the PRISMA reporting checklist.
Methods
Study design
This study comprised two main components: (1) a comprehensive literature review on nurse-led mHealth interventions and (2) a Delphi method to evaluate and refine the intervention framework. The literature review was conducted between May 2014 and May 2024, while the Delphi method was employed from October 2024 to March 2025, involving 2 rounds of online anonymous consultation with a panel of nursing specialists. This study was approved by the Ethics Committee of the Affiliated Hospital of Jiangnan University (reference number: LS2024019) and the Evidence-based Medicine Centre of the Fudan University (reference number: ER20230405). Informed consent was obtained from all participants prior to the study initiation.
Systematic review
From May 2014 to May 2024, we conducted a systematic literature search using PubMed, Web of Science, Cochrane Library, CNKI, and Wanfang databases. The English search words included: ‘cardiovascular diseases’ OR ‘myocardial infarction’ OR ‘cerebrovascular disorders’ OR ‘stroke’ OR ‘hypertension’ OR ‘diabetes mellitus’ OR ‘chronic disease’ AND ‘telemedicine’ OR ‘mobile applications’ OR ‘smartphone’ OR ‘mHealth’ OR ‘eHealth’ OR ‘mobile health’ AND ‘nurses’ OR ‘nurse practitioners’ OR ‘nurses, public health’ OR ‘registered nurses’ OR’ nurse-led’ OR ‘personnel, nursing’. The Chinese search words included: ‘chronic disease, mHealth, nurses’. Eligible studies included systematic reviews, meta-analyses, or randomized controlled trials with a clear focus on mHealth in patients with chronic diseases, which were English or Chinese publications. We excluded abstracts, conference proceedings, and incomplete articles.
Delphi process
Participants
Purposive sampling was used to recruit participants for the specialist panel. The following inclusion criteria were applied for specialists: (a) professional background in mHealth, chronic diseases, or nursing; (b) a minimum of 10 years of experience in the relevant field; (c) possession of a senior title; and (d) willingness to voluntarily participate in this study. An online consultation invitation was sent to 15 specialists via email; of whom, 13 agreed to participate. The high participation rate was likely due to the flexibility of asynchronous email communication. The ability to respond at their convenience likely facilitated the specialists’ willingness to participate, as it allowed them to complete the consultation at a time that suited their schedules without requiring real-time interaction.
Data collection
A study group including three graduate nursing students from the hospital drafted consultation letters based on the initial draft of the intervention framework. The consultation letter consisted of four sections: an introduction to the study, informed consent information, a draft of the intervention frameworks, and specialists’ demographic information. A five-point Likert scale was used, in which 5, 4, 3, 2, and 1 points represented ‘strongly agree’, ‘agree’, ‘somewhat agree’, ‘rather disagree’, and ‘disagree’, respectively. A recommendation section was also included in the questionnaire for specialists to share their opinions and reasoning regarding revisions, additions, or deletions. The participants were reminded twice before the conclusion of each Delphi round to engage in the discussion. We conducted two rounds of specialist consultation, as this process enabled the specialists’ opinions to reach a substantial level of consensus. This approach not only enhanced the mHealth framework effectively but also prevented the additional costs associated with conducting further rounds of consultation. The two Delphi rounds were closed after 4 weeks.
Study material
In the first Delphi round, 36 items were presented on the following topics: (1) pre-hospital evaluation, including health profile, health assessment, and admission framework; (2) in-hospital intervention, including dynamic assessment, dynamic interventions, and patient education; and (3) post-hospital continuity, including discharge framework, remote monitoring, and management of follow-up care.
Data analysis
SPSS software version 26 was used for the statistical analyses. Frequency distributions were employed to describe demographic data and questionnaire responses. After two Delphi rounds, means and standard deviations (SD) were calculated for all items that reached consensus. In this study, consensus was defined as “being achieved” when 80% or more of the specialists assigned identical ratings to the items. A recommendation was deemed to have reached consensus when at least 80% of the participants who evaluated the item assigned it a score of 4 (i.e. agree) or 3 (i.e. somewhat agree), for both relevance and feasibility. The objective was to accurately present the responses provided by the specialists. 21 The specialists were provided with feedback following each Delphi round; the subsequent round was adjusted based on the insights gathered from prior feedback.
Results
Systematic review
A total of 887 articles were identified. Among these, 35 duplicates were screened, and 4 articles lacking the full text were excluded. The remaining 848 articles were reviewed in full text for eligibility, of which 832 were excluded because they did not address chronic diseases or report mHealth. Finally, 16 articles were deemed highly relevant to nurse-led mHealth programs in patients with chronic diseases11,22–36 (Figure 1). The included articles consisted of randomized controlled trials, systematic reviews, and meta-analyses. These articles, evaluated by the study group, were closely aligned with the study topic, employed rigorous experimental designs, and were deemed sufficiently rigorous to support development of the intervention framework.
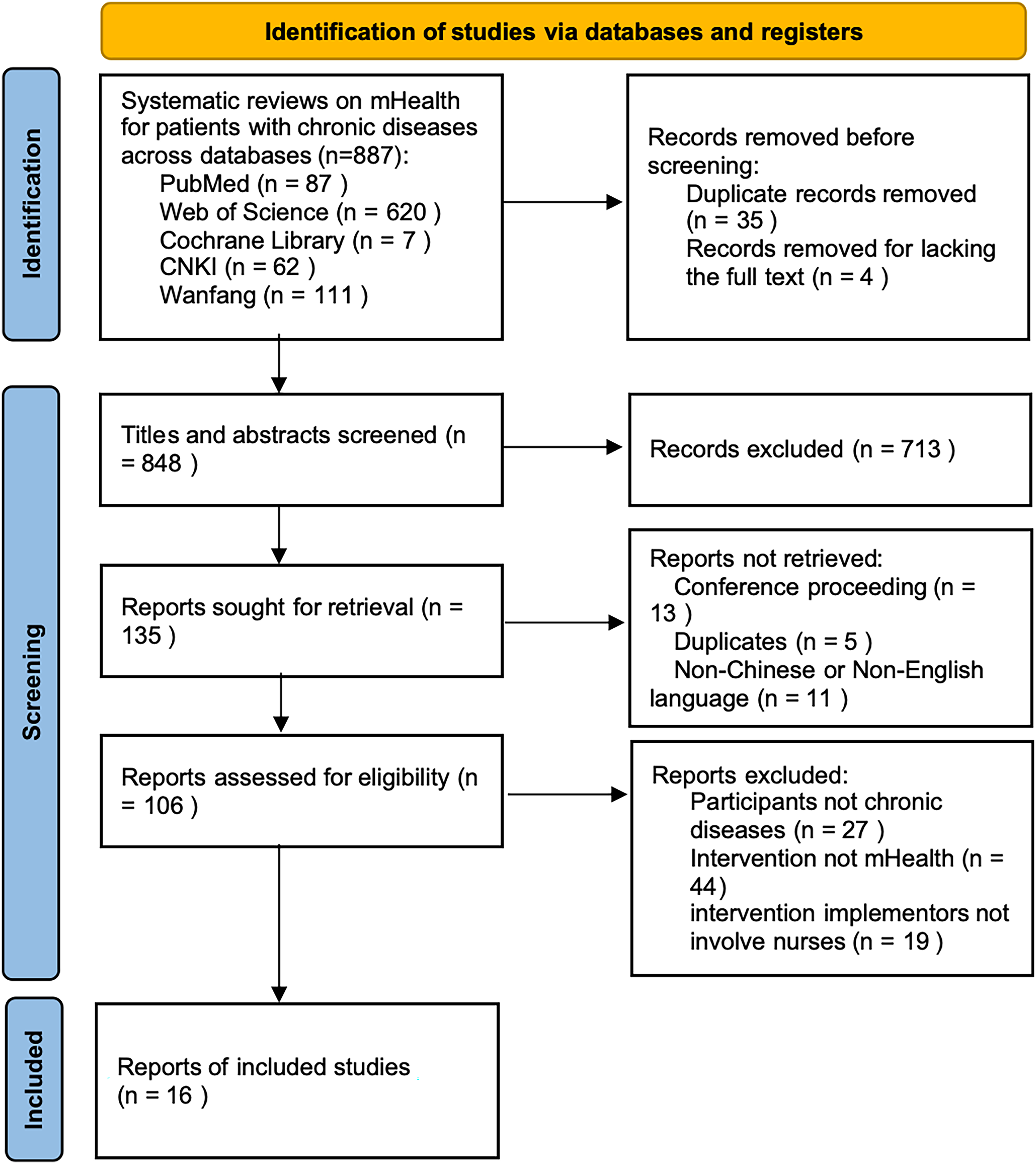
PRISMA flow diagram charting identification of studies.
To identify the nurse-led mHealth interventions described in these studies, two researchers independently reviewed all included articles. Based on the literature review, the study group developed an initial draft of the intervention framework comprising 36 items across three topics. This preliminary draft was evaluated for readability and feasibility by four nursing specialists with extensive experience in mHealth. The framework items from all studies were gathered into one consultation letter for review by Delphi panelists.
Delphi process
Participants
Fifteen eligible nursing specialists, experienced in the field of mental health, were invited to participate in the first round. Thirteen (12 female and 1 male specialists) agreed to participate in two rounds of Delphi. Ten participants have rich clinical experience in managing patients with chronic diseases; however, this was not an eligibility requirement. Table 1 presents detailed demographic information.
Demographics of the Delphi panel.

Round 1
Among the initial 36 items, the specialists deleted 7 items without consensus (consensus level < 80%), and suggested that 6 items could be merged; 23 items finally remained. Regarding individualized interventions, specialists suggested that elements with commonalities could be integrated. Additionally, no consensus existed among specialists on items that significantly increased nursing workload, prompting the study team to consider their exclusion.
Round 2
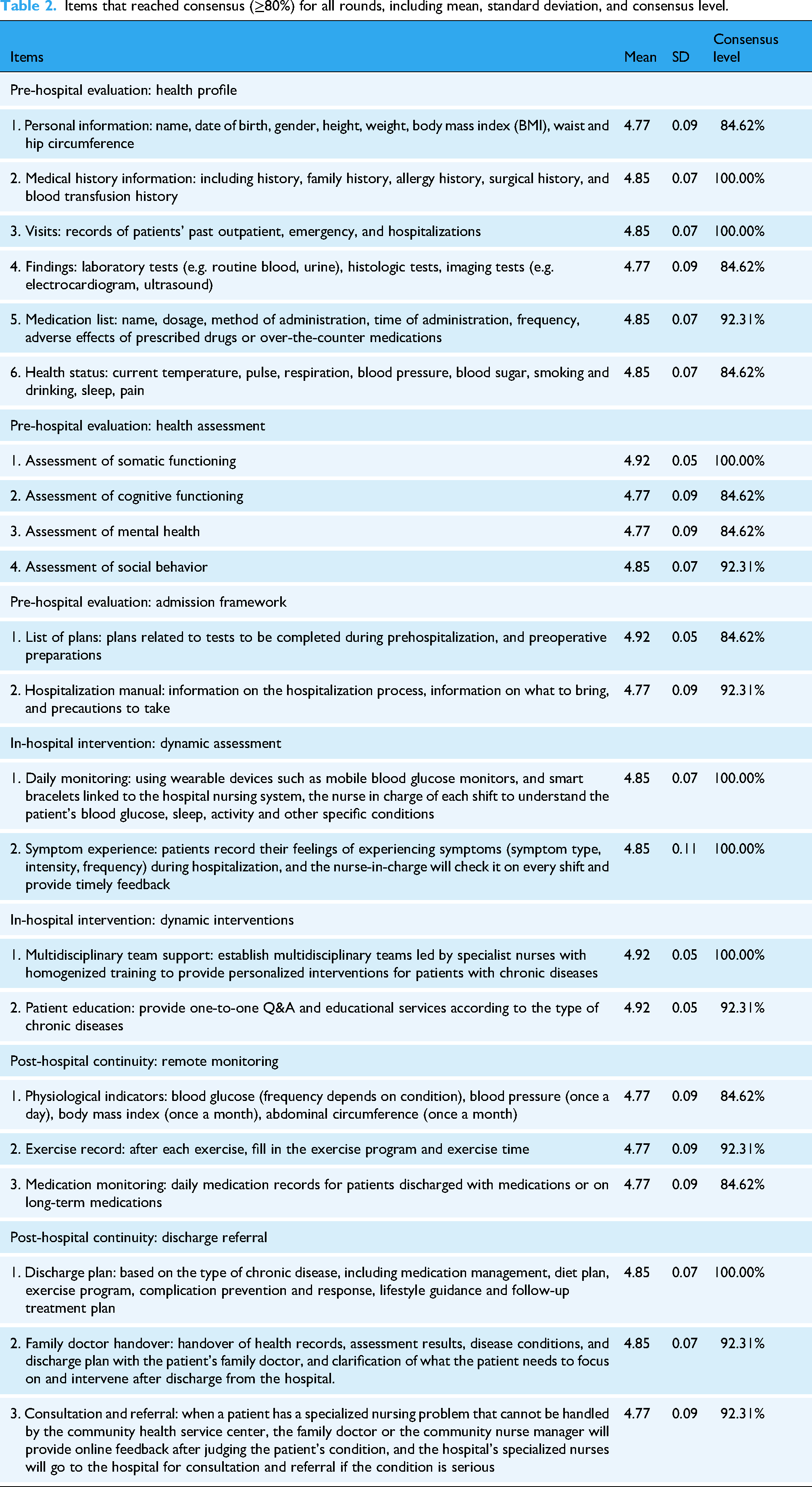
After the first round of revisions, a second round of Delphi analysis was conducted on the remaining 23 items. A total of three recommendations were suggested by the specialists, one of which—removing the “diet plan” from self-monitoring—was agreed upon. The other two recommendations were ultimately rejected because the participants continued to suggest that they were not feasible due to the limited resources available for hospital intelligence. Hence, 22 out of 36 items reached consensus after 2 rounds, with a mean of 4.77–4.92 (SD, 0.05–0.11), as listed in Table 2.
Items that reached consensus (≥80%) for all rounds, including mean, standard deviation, and consensus level.
Discussion
The Delphi process effectively established consensus on key items for the nurse-led mHealth framework. A majority of the initial 36 items reached consensus (22/36, 61.1%). The approved items are designed to support the nurse-led mHealth intervention framework and to ensure its meaningful integration into existing healthcare structures. Although previous studies have suggested that mHealth can be effective in delivering high-quality healthcare, the overall evidence remains mixed. 37 The objective of our study was to provide evidence by (1) conducting a systematic review of the literature to identify a detailed list of items present in published mHealth intervention frameworks and (2) reaching a clinical agreement among specialists through the Delphi method. Our findings indicated that combining these methods was effective in developing a detailed mHealth intervention framework.
Despite the increasing adoption of mHealth, limited evidence supporting frameworks exists. 38 Positive outcomes have been observed in chronic disease management, including reduced mortality and hospitalization, enhanced quality of life, and improved glycemic control in patients with diabetes. However, additional issues related to applying study findings to actual healthcare settings and organizational obstacles were observed. 39 Several questions, such as identifying the most suitable action frameworks, remain unanswered. 38 Thus, the current study created an evidence-based mHealth intervention framework and obtained a high level of confidence that nurses can use the framework. The final version of the framework serves as a reliable guide for prehospital evaluation, in-hospital intervention, and posthospital continuity.
Numerous studies have reported nurse-led approaches to mHealth, including the facilitation of remote consultations, organizing video conferences with participants, and management of extended communications via phone calls and emails. 11 However, the content construction processes have rarely been reported. Nurses primarily acted as mHealth evaluators, with subject matter specialists playing the secondary most common role. Their involvement in mHealth development or planning is limited, and they rarely serve as patient advocates, research specialists, or nurse informaticists. 40 The integration of nurses into mHealth development teams adds a patient-focused perspective to the developmental processes. This can generate frameworks that include evidence-based contemporary health-related information important to end users. 41 In this study, nurses served as the primary personnel responsible for the mHealth framework, ensuring the content was aligned with patient needs.
The nurse-led mHealth intervention framework could present a distinctive methodology for assessing and managing patients with chronic diseases in real-world clinical environments. 42 Its significance lies in the integration of digital health technologies to improve patient care and self-management capabilities. Previous studies demonstrated that nurse-led digital health interventions effectively enhance self-management behaviors, clinical outcomes, and overall patient satisfaction among individuals with chronic conditions.33,43,44 Developing such a framework is essential for guiding nurses through the systematic implementation of mHealth interventions. It provides a structured and evidence-based approach to intervention design and execution. Furthermore, the three major themes of the framework can be designed as the three core modules of the mHealth application, with specific functions integrated into each module. Nurses can utilize the application to conduct scientific and standardized prehospital assessments in patients with chronic diseases and establish individualized health records. The application also supports in-hospital symptom monitoring and patient education, while ensuring the continuity of nursing and medical services after hospital discharge.
The major strengths of our study were the use of validated methodologies, such as the systematic review and Delphi method, to create a mHealth framework and the involvement of nursing specialists from several medical centers. The effectiveness of this framework has not yet been formally assessed among nurses; thus, leaving its clinical usefulness undetermined. With the framework structured and portable design, a future study assessing its effectiveness among nurses would be a logical, subsequent step. The implementation of frameworks within mHealth applications holds significant potential for optimizing clinical nursing for managing patients with chronic diseases, as these frameworks comprehensively encompass the full spectrum of patient care from prehospital to posthospital stages.
This study has some limitations. First, the quality of evidence varied greatly owing to differences in study objectives, designs, and outcomes. Another limitation pertains to the regional concentration of the nursing specialists. Although efforts were made to recruit participants from various regions across China, all participating specialists were located in Jiangsu Province, primarily due to time constraints in data collection and regional variations in willingness to participate. This geographic homogeneity may restrict the generalizability of the findings to other settings with differing healthcare systems and cultural contexts. To address this limitation, the study team prioritized the inclusion of specialists with diverse educational backgrounds and substantial clinical experience. Additionally, considerations regarding cultural adaptability and operational feasibility were systematically addressed during the development of the framework. Future studies should seek to validate and refine this framework through multicenter investigations involving broader national and international representation of healthcare professionals.
Conclusions
We used a systematic review of the literature and the Delphi method to develop a nurse-led mHealth intervention framework. Based on an analysis of 16 published articles and inputs from our study group, we developed an initial framework comprising 36 items. This framework was refined to 22 items using the Delphi method. Our nurse-led mHealth intervention framework achieves both brevity and breadth of content and is highly suitable for designing mHealth applications or conducting mobile care for chronic disease management.
Footnotes
Acknowledgement
The authors want to thank every specialist who offered us valuable suggestions in this research.
Ethics approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of the Affiliated Hospital of Jiangnan University (reference number: LS2024019).
Informed consent
We confirm that all participants provided informed consent to participate in the study based on a written privacy notice. Written informed consent was required before participating in each round of the Delphi.
Contributorship
JH, DG, and LZ were involved in conception and design; HW in administrative support; JC, GF, and QZ in provision of study materials or patients; NH and DS in collection and assembly of data; and DS in data analysis and interpretation. All the authors contributed to manuscript writing and final approval of manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovative research projects of Jiangsu Hospital Association (top-level guidance program): JSYGY-3-2023-125 and the 2024 Wuxi Youth Science and Technology Talents Promotion Action: TJXD-2024-211 and the Chinese Medical Association Journal of Nursing Research 2022-2023-Development Program: CMAPH-NRD2022003.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.