
Abstract
Background
Digital and mobile (mHealth) solutions are online or application-based services intended to support individuals with health needs. Despite evidence supporting the use of mHealth for patients with chronic pain, and the increasing desire of these types of solutions by both patients and providers, adoption of mHealth solutions remains limited. Implementation mapping can serve as a practical method to facilitate implementation and adoption of mHealth solutions within healthcare settings.
Methods
Implementation mapping was used to develop implementation strategies based on contextual determinants organized within the Consolidated Framework for Implementation Research (CFIR) for mHealth eLearning solutions across an integrated, multi-site healthcare system. We describe our experience identifying stakeholders, delineating implementation facilitators and barriers, defining implementation outcomes using RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) framework, outlining initial implementation strategies, and iterating on implementation strategies.
Results
A total of 30 implementation strategies were identified and implemented. Over the first year, primary and specialty care providers across all the clinical sites (n = 70) placed 2559 orders for the mHealth solution. Most patients reported receiving the mHealth eLearning module (74%), and most patients felt that the tool improved their knowledge regarding their condition (82%) and their ability to provide self-care related to the condition (73%).
Conclusion
Practical applications of implementation science methods can help enable change within healthcare settings. Implementation mapping is an exercise that can engage stakeholders to facilitate the incorporation of new methods of care delivery, including mHealth solutions.
Keywords
Background
Chronic pain, or pain experienced on most or every day, is reported by more than 20% of the adult population in the United States. 1 Unmanaged chronic pain is associated with multiple aspects of life and health, including increases in distress and disability, as well as decreases in quality of life, cognition, mood, and mental health. 2 From a clinical perspective, patients experiencing chronic pain are best served with multidisciplinary expertise, including those specializing in psychology, neurology, internal medicine, rheumatology, physical therapy, and others. 3 Access to multidisciplinary care is limited, and disparities exist in the management of chronic pain based on patient geographic location, 4 race/ethnicity, 5 and cultural aspects of pain. 6 Within our current structures, healthcare providers report that the needs of patients with chronic pain can be highly burdensome due to the multifactorial medical, social, and mental health aspects that need to be addressed. 7 Additionally, providers report insufficient knowledge about pain physiology and management following revelations of the opioid epidemic.3,8,9
Digital and mobile health (mHealth) solutions have a role in the democratization of clinical expertise to patients experiencing chronic pain by overcoming limitations of geographic location and inherent biases within our medical systems. The advantages of mHealth solutions for patients include consistent and accurate information presentation, geographic independence, and consideration of patient time and availability.10,11 Preliminary data supports improvement in disease-related knowledge and perceived self-efficacy among patients leveraging digitized and interactive disease-specific mHealth tools.12–14 Digitized and interactive mHealth tools may also serve to enhance communication between patients with chronic pain and their healthcare providers, supporting shared decision-making and increasing confidence in clinical judgement. 10 mHealth solutions can be of educational value to patients with chronic pain by providing structured information on the etiology, neurobiology, and treatment of disease, 10 leveraging the expertise of multiple specialties in line with the Institute of Medicine's best practices for the management of patients with chronic pain, 8 but at the scale needed to help the millions of individuals experiencing chronic pain.
Multidisciplinary mHealth solutions addressing the needs of patients with chronic pain have shown small but significant improvements in disability, depression, anxiety, pain intensity, pain-related self-efficacy, and pain catastrophizing. 15 The effects of these mHealth solutions more than double if the solution was guided by clinicians as opposed to self-guided by the patient, 15 demonstrating the role of mHealth solutions to augment and extend the care delivered by our traditional care models. Despite evidence supporting the use of mHealth solutions for patients with chronic pain, 2 and the increasing desire of these types of solutions by both patients and providers, 16 adoption of mHealth solutions remain limited. 17 Implementation mapping, based on intervention mapping, is a practical method for planning implementation strategies that enable change within healthcare settings, extending the reach of effective interventions into the hands of those who could benefit from them. 18 Leveraging the tools of implementation, science can help facilitate integration and spread of new clinical care models, including mHealth solutions.
The goal of our overall project was to create, implement, and evaluate novel mHealth eLearning solutions for patients experiencing centrally sensitized chronic pain. We intended for our mHealth solutions to be (1) accessible by any patient and provider across our multi-site, integrated healthcare delivery system, and (2) to fit within existing clinical and technological workflows to create a seamless experience for care team members. Contextual determinants for implementation of our mHealth solutions were delineated using the Consolidated Framework for Implementation Research (CFIR), and here we describe our process of implementation mapping to develop our implementation strategies. We assessed the implementation outcomes of the deployment using the RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) framework. In the current study, we share our implementation experiences to help inform further research and application of mHealth solutions to meet the needs of patients experiencing chronic pain.
Methods
Setting
Mayo Clinic is a large, integrated healthcare delivery organization with more than 70 hospitals and facilities, and 7000 physicians serving more than 1.3 million patients a year across all 50 U.S. states and more than 130 nations around the world. Healthcare providers and patients are supported by enterprise support services deploying digital support patient care tools, creating patient education materials, and maintaining the electronic medical record. Ethical approval for this investigation was provided by the Mayo Clinic Institutional Review Board, and patient consent for enrollment was waived. Patients across our healthcare system were eligible to receive the mHealth eLearning solutions if they had an active digital connection to our electronic health record (EHR) and diagnosed with an applicable chronic pain condition by any practicing clinician at Mayo Clinic.
Overall implementation approach and the role of implementation mapping
Prior to the initiation of this work, project leaders reviewed a recent publication by Gordon et al. 19 (2020) describing the determinants of integration of mHealth solutions into clinical care, and then utilized the Consolidated Framework for Implementation Research (CFIR) to discuss and delineate the barriers and facilitators to the design, development, deployment, and sustainment of a digitized education program for patients experiencing chronic pain (Figure 1). The process of implementation mapping was used to develop implementation strategies that would enable the adoption, implementation, and maintenance of these solutions (Figure 2). 18

Implementation framework deployed within a multi-site, integrated healthcare delivery system for mHealth eLearning solutions for chronic pain, Consolidated Framework for Implementation Research (CFIR).
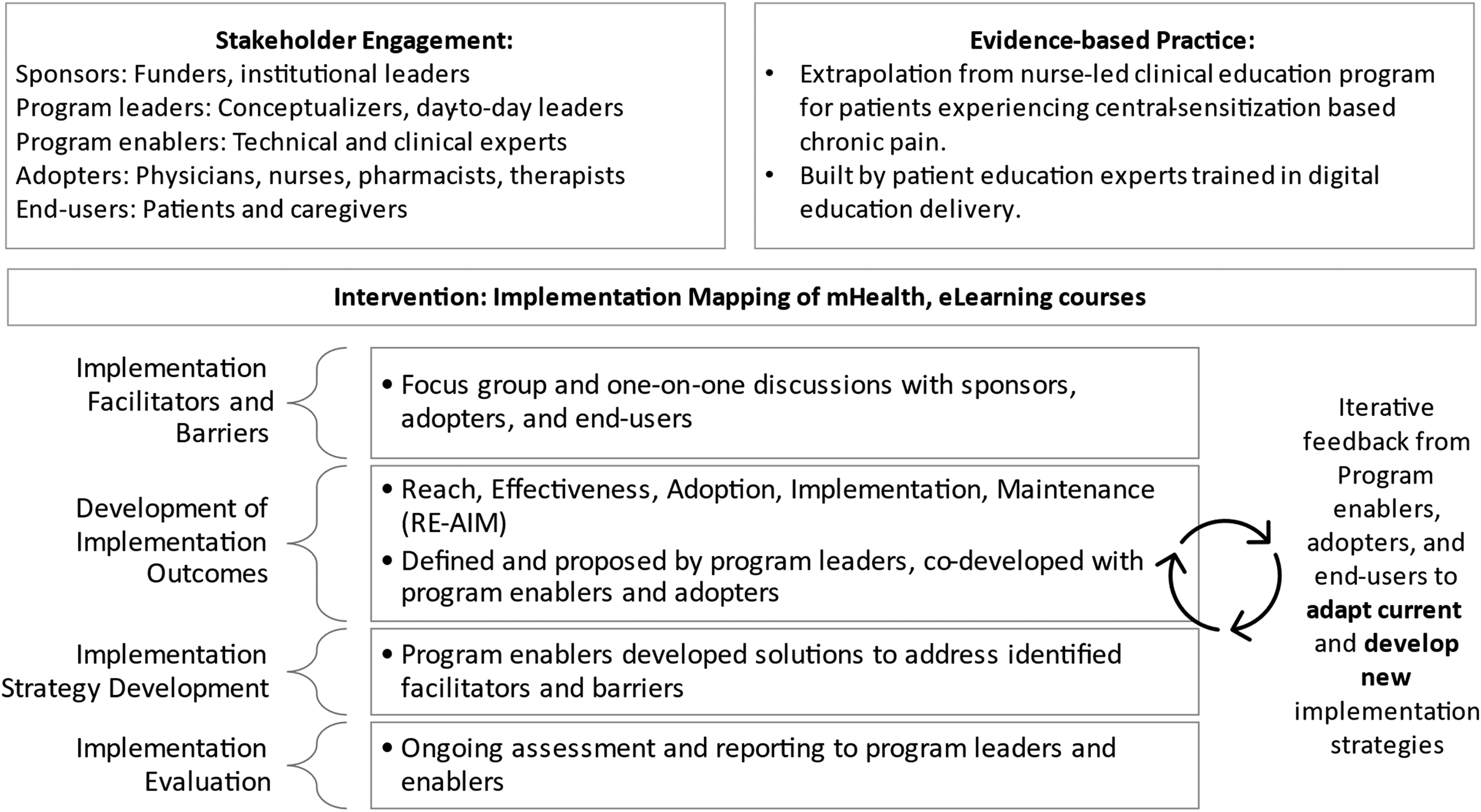
Implementation mapping process used to deploy mHealth eLearning courses for patients experiencing centrally sensitized chronic pain conditions across an integrated healthcare system.
Stakeholder identification
A group of stakeholders were identified iteratively throughout the development process and included individuals within five categories: sponsors, program leaders, program enablers (implementers), adopters, and end-users. Sponsors included those who funded and sponsored the initiative throughout the design, build, implementation, and evaluation process. Program leaders conceptualized and led the day-to-day operations of the program. Program enablers included technical experts in patient education, digital learning, program management, health systems engineering, data analysis, communications, revenue cycle/patient billing, legal/compliance, information technology, and our electronic medical record environment. Adopters included physicians, nurses, nurse educators, clinical pharmacists, and desk operations staff. Patients with centrally sensitized chronic pain conditions were the end-users.
Evidence-based practice
One of the three care delivery models included within the mHealth umbrella is eLearning, a model consisting of digitally static and interactive patient education material intended to provide general information about a condition including symptom identification and insights into treatment planning. 2 We developed eLearning content based on pain neuroscience education programming created for patients with fibromyalgia, 20 and was created as an extension of the multidisciplinary clinical effort described previously. 21 Five mHealth eLearning courses were created by multidisciplinary teams to focus on five centrally sensitized-based chronic pain conditions: fibromyalgia, post-COVID syndrome, chronic fatigue, irritable bowel syndrome, and chronic migraine. The in-person, virtual, and traditional paper-based patient education materials were digitized to include videos by multi-specialty providers, 8 animations, pictures, and interactive content, which incorporated neurobiology-based education that has been shown to improve symptom severity, pain catastrophizing, depression and anxiety.22,23
Intervention
Implementation mapping was deployed to work collaboratively with stakeholders to facilitate implementation of the mHealth eLearning solutions across our healthcare system.24–26 As described by Fernandez et al. (2019), implementation mapping is comprised of six components: (1) identification of problems/concerns and an outline of how to address them, (2) creation of change objectives through the overlay of performance objectives with determinants, (3) selection of theory-based intervention methods matched to determinants, and translation of these determinants into strategies, (4) integration of implementation strategies into a program, (5) identification of program users and supporters to co-develop plans for adoption, implementation, and sustainment, and (6) creation of process and effect evaluation plans to measure program effectiveness. Here we describe the implementation mapping process used by our teams.
Implementation facilitators and barriers
Engagement with stakeholders was iterative. To help drive our conversations with stakeholders, we structured conversations around a modified version of the framework described by Gordon et al. to include the following considerations: clinical value and validation of the mHealth eLearning courses, provider communication, awareness and support, the legal, privacy, and security measures needed to ensure the safe delivery of the mHealth eLearning courses to patients, the workflow and electronic medical record integration needs to incorporate a new mHealth eLearning solution into routine clinical care, the payment models needed to support mHealth eLearning for patients, and the patient and provider end-user support needed to adopt and maintain this new outlet of patient-facing mHealth solution. 19 Initial engagement discussions consisted of varying stakeholders, and two-way communication was facilitated through the project's senior project manager.
Definition of implementation outcomes
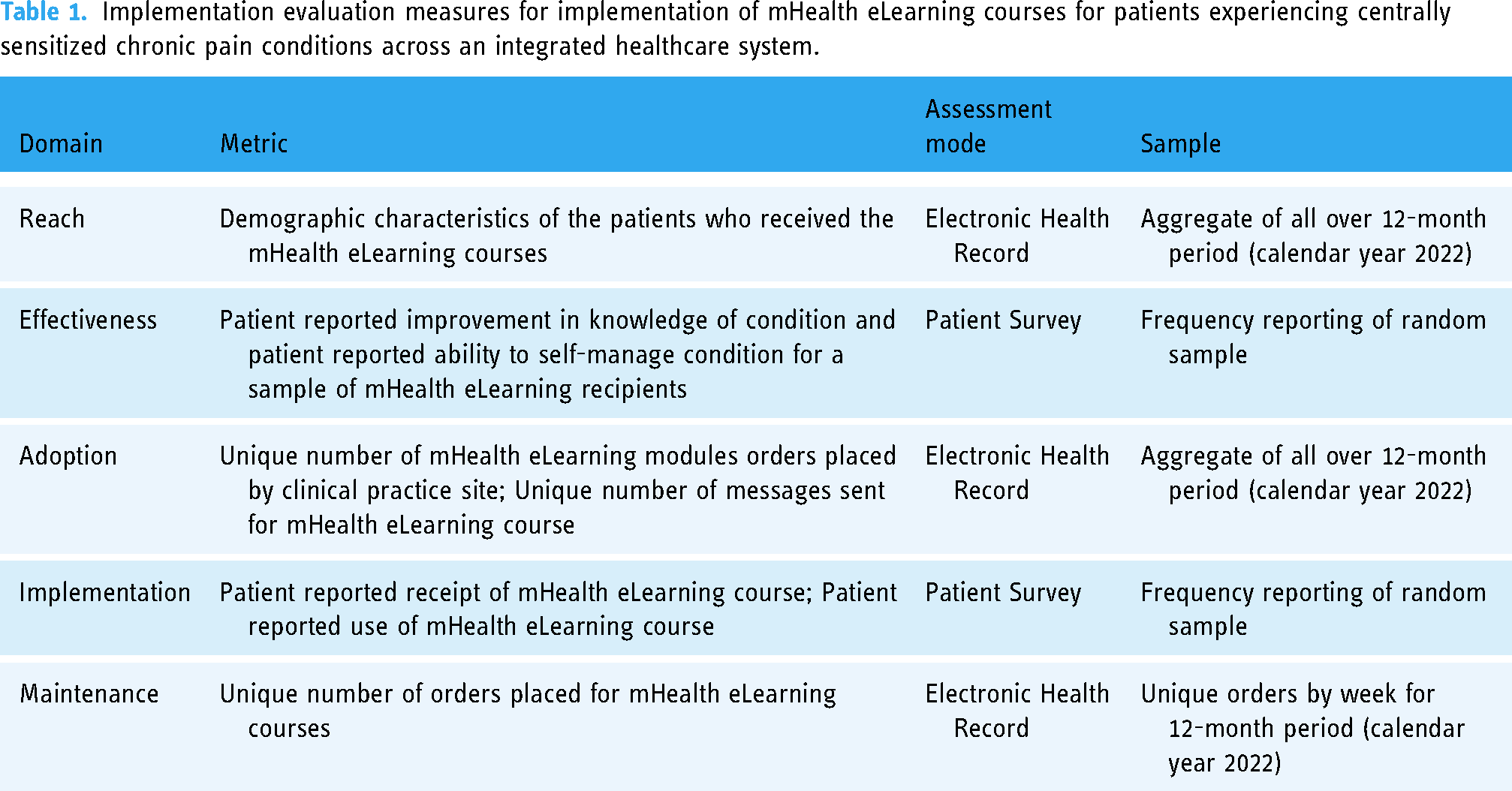
To structure the development of implementation outcomes that facilitated generalizability and dissemination of the program we utilized the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework.27,28
Implementation evaluation measures for implementation of mHealth eLearning courses for patients experiencing centrally sensitized chronic pain conditions across an integrated healthcare system.
Implementation strategy development
Once the major barriers and facilitators of implementation of the mHealth eLearning courses were identified, we worked collaboratively with leaders and subject matter experts within our clinical practice and shared service groups to outline implementation strategies. Implementation strategies were often iterated upon from an ideal solution or set of solutions, to those that were achievable.
Implementation evaluation
To ensure measurement of the implementation outcomes, we deployed two data gathering tactics. First, data was gathered passively from the EHR, to include the demographic characteristics of the patients who received the mHealth eLearning courses (Reach), the number of unique orders placed for the mHealth eLearning courses (Adoption, Maintenance), and the number of unique messages sent from the EHR order to the patient portal (Adoption). Demographic information included age, gender, race/ethnicity, and marital status. Age is reported as mean ± standard deviation, and all other demographics are reported as frequency (proportion). Second, a simple random sample of patients receiving the mHealth eLearning courses received an electronic survey. Patients were asked whether they had received a link to our mHealth eLearning course (Implementation). Patients were also asked if they opened the mHealth eLearning course (Implementation), whether it improved their knowledge (Effectiveness), and whether it helped them to manage their condition more effectively (Effectiveness). Survey responses are reported as frequency (proportion). Survey assessments were sent electronically to patient-provided Email addresses using Qualtrics Survey Software (Provo, UT). A copy of the survey assessment is included as a supplemental appendix. All data management and analyses were performed using Statistical Analysis Software (SAS) Version 4.2 (Cary, NC).
Results
Implementation mapping and implementation strategies
Beginning in January of 2021, the program leads began the implementation mapping process. Over the course of 2021, while the mHealth eLearning courses were built, the program leads met with the stakeholders listed above to identify, build, and execute on the implementation strategies listed in Table 2. Initial implementation strategies are listed in the third column, and included those implementation strategies that were decided upon prior to the go-live of the first mHealth eLearning course in October of 2021. The remaining courses and workflows were completed through the end of the 2021 calendar year, with all five mHealth eLearning courses live and orderable by any healthcare provider across the healthcare enterprise on 5 January 2022. The strategies listed in the fourth column include those that were identified and added during the pilot launch of the mHealth eLearning course in October 2021.
Products of implementation mapping exercise outlining the change objectives, agents, and implementation strategies (at onset of implementation and those added during implementation) experienced during implementation of mHealth eLearning courses across an integrated healthcare delivery system.

Note. Individual implementation strategies are mapped to domain target within the Consolidated Framework for Implementation Research (CFIR). CFIR, Consolidated Framework for Implementation Research (IV = Innovation, IN = Individual, IS = Inner Setting, OS = Outer Setting); EHR, electronic health record. Clinicians include physicians, advanced practice providers, and nurses.
Adapted from Gordon et al. (2020).
Clinical value and validation
Both patients and clinicians indicated that clinical value of an mHealth eLearning intervention was most needed for patients experiencing centrally sensitized chronic pain conditions. Additionally, clinical teams indicated that building upon clinical programs that were developed by recognized experts in the field of central sensitization would increase trust in the content. Therefore, we engaged with clinical experts (physician, nurse, nurse educator) in the diagnosis and treatment of patients with chronic pain and fibromyalgia to serve as the core content for our mHealth eLearning courses. We then partnered with subject matter experts specializing in chronic fatigue, post-COVID syndrome, irritable bowel syndrome, and chronic migraine for condition-specific content. The creation of eLearning content that leveraged best practices of patient education and adult learning was identified as a requirement for the clinical value of the program. Gaining input on the content, layout, and the process of receiving the mHealth eLearning tool was identified as a need to ensure clinical value of the courses, and patients were engaged during the pilot launch to provide feedback as an implementation strategy. Based on patient feedback, modifications were made to the length and intent of the clinical content provided.
Provider communication, awareness, and support
To facilitate knowledge about and awareness of the mHealth eLearning solutions, multiple communication pathways were identified by our stakeholders. Our initial implementation strategies focused on traditional routes of institutional messaging, including presentations at standing committees and lectures, and provider-directed practice update newsletters. Through additional feedback, additional implementation strategies emerged, including the creation of patient stories of their experiences with the mHealth eLearning solutions, and increased communications and presentations with nursing staff, who often participate in the care planning for patients across our clinical settings. Due to time constraints of our clinical leaders and the volume of requests for demonstrations and presentations, next steps include the creation of short videos intended for clinical audiences that can be included within electronic communications or played during standing clinical meetings.
Legal, patient privacy, and security measures
As digital tools and mHealth solutions continue to grow in volume and relevance, the landscape of data privacy and security evolves to ensure that both patients and providers are safe. 29 Our stakeholder group requested that the project team explore the legal, patient privacy, and security measures necessary to ensure the safe referral to and use of our mHealth eLearning tools. Initial implementation strategies included the identification and vetting of web-hosted solutions, the secure routing of patient orders to secure message delivery, and the security processes needed from our internal patient portal system to the mHealth eLearning hosting website. Agents internal to Mayo Clinic with expertise in legal, compliance, information technology, and our electronic medical record system were close partners to ensure the safety of referral to our mHealth eLearning tools.
Workflow and EHR integration
To facilitate ease of referral to our mHealth eLearning solutions, our stakeholder group encouraged the team to assess clinical workflows for our outpatient practices and identify workflow enablers. Workflow assessments identified several opportunities within the enterprise electronic health record system that would enable seamless ordering and delivery of our mHealth eLearning solution by any provider with ordering privileges across our enterprise (physician, nursing, pharmacy, therapy, and other clinical roles). Specific implementation strategies that enabled clinical workflows via electronic health record integration at the program onset, as well as those that were developed during solution roll-out are outlined in Table 2
Payment
To enable as many patients as possible in need of our mHealth eLearning solutions to have access to them, our stakeholder group identified the need for the project team to explore the payment needs and options related to our mHealth eLearning solutions. Experts internal to Mayo Clinic were able to assess the role, content, and proposed function of our tools, and proposed these solutions be treated as traditional patient education materials and provided at no charge to patients. Via patient feedback loops (as part of the operationalization of our eLearning program), we learned that patients benefitted from reassurance of the no-cost structure of the mHealth eLearning solutions, so patient-facing communication was updated to include this clarification.
Patient and provider end-user support
As patients and providers transition to new models of care, including digital health solutions, our stakeholder group suggested we investigate the types of end-user support that could enable our mHealth eLearning solutions. Members of our information technology, electronic health record, patient education, and clinical teams were the primary agents to define and develop implementations strategies to address this need. Quick reference guides were created to enable our care teams in locating and ordering the mHealth eLearning tools. During the early phase of our implementation, patients were contacting members of our clinical care teams for support in the use of these tools, which was not sustainable for the success of digital tools broadly across the clinical practice. Patients were subsequently connected to technical support personnel within the digital health department.
Evaluation
Over the course of the first full year of implementation of our mHealth eLearning modules for patients with chronic pain, there were 2559 patients who received an order from a Mayo Clinic provider. Of these, 2488 (97.2%) received a portal message containing patient information and the electronic link for the mHealth eLearning tool. The primary cause for attrition within this step was patient lack of an active patient portal account at the time of order batch processing. The average age of recipients was 45 years (±16), the majority were female (80.0%), white race (92.7%), not Hispanic or Latino (93.2%), and identified as married or within a life partnership (59.4%) (Table 3). Orders were placed for patients residing in all 50 U.S. states, with the majority residing in Minnesota (35.4%), Florida (11.1%), Wisconsin (7.9%), Illinois (5.9%), and Iowa (5.4%).
Characteristics of patients who received an order for one of five mHealth eLearning modules for chronic pain in 2022 (n = 2559).

Most orders placed for the mHealth eLearning solutions were placed from our primary clinical practice location (Rochester, Minnesota, 75%), followed by our Florida campus (16%), Mayo Clinic Health System (5.5%), and Arizona campus (3.5%). The most ordered mHealth eLearning module was for fibromyalgia (40.6%), followed by chronic abdominal pain / irritable bowel syndrome (23.4%), post-COVID syndrome (14.9%), chronic fatigue (14.0%), and chronic migraine (7.1%). On average, there were 213 unique orders per month (±32) or 48 orders per week in 2022. Volumes of orders increased for the first 3 months of the implementation timeframe, then varied within one standard deviation of the average number of orders per month (Figure 3).

Volume of unique orders placed for mHealth eLearning modules by month during 2022.
Among our small sample of patients surveyed regarding experiences with the mHealth eLearning tool, 23 (74%) reported receiving the mHealth eLearning module, and 22 (71%) reported interacting with the module. Of patients who reported interacting with the mHealth eLearning modules for chronic pain, most patients felt that the tool improved their knowledge regarding their condition (8, 36.4% “Probably Yes”; 10, 45.5% “Definitely Yes”), and improved their ability to provide self-care related to the condition (12, 54.6% “Probably Yes”; 4, 18.2% “Definitely Yes”).
Discussion
In this study, we describe the implementation mapping process taken by our team to support the implementation of mHealth eLearning solutions for patients experiencing centrally sensitized chronic pain across a multi-site, integrated healthcare delivery system. We describe the types of stakeholders we engaged with, the change objectives that were outlined by stakeholders, our engagement with experts to develop discrete implementation strategies, and how our implementation strategies evolved and expanded during implementation. Through the use of our implementation mapping process, our mHealth eLearning modules are now ordered for 50 new patients each week across our clinical practice locations. Most patients surveyed reported that the mHealth eLearning modules increased knowledge of their condition and improved their ability to manage their symptoms.
The translation of effective interventions into routine clinical care, including mHealth solutions, is challenging due to a multitude of social, cultural, economic, and organizational factors resulting in the slow adoption of new treatments and tools. The traditional trajectory of discovery science into routine clinical practice includes the development of clinical interventions, the testing of clinical intervention effectiveness, then the eventual adoption, implementation, and ongoing maintenance of new interventions. 18 The field of implementation science has emerged to provide rigorous study and recommendations of methods, models, and frameworks to condense this traditional discovery trajectory and support the adoption of new clinical interventions within complex healthcare environments.
Our team utilized the implementation mapping method described by Fernandez et al. 18 to work with stakeholders, experts, and change agents to implement mHealth eLearning solutions for patients with chronic pain across our multi-site, multi-specialty healthcare system. The benefits of implementation mapping within complex healthcare delivery systems include the ability to leverage the institutional and historic knowledge of stakeholders in the identification of change objectives and implementation strategies, 18 the ability to foster transparency in the selection of implementation strategies, 24 and the ability to share the strategies deployed with medical communities who may be interested in executing on similar initiatives. 18 In addition to these recognized benefits of implementation mapping, we also felt that this method enhanced our ability to foster collaboration with internal experts as change agents when coordinating changes such as modified clinical workflows or enhancements to electronic medical record systems; these are fundamental components of overall change management. 30
mHealth solutions offer the potential to extend the care provided by healthcare professionals into the daily lives of those experiencing chronic conditions, including chronic pain. Digitized expertise, such as mHealth eLearning solutions, offer insight into the pain experience, including in depth review of the physiological, psychological, and social constructs associated with pain that have been demonstrated to help improve the pain experience.22,23 mHealth eLearning solutions can provide information that is easily accessible, accurate, and interactive to those patients interested in and able to use them. 10 Hypothesized additional benefits include patients’ enhanced ability to communicate with healthcare providers and family members, as well as the ability for rural and/or remote patients to have increased access to medical expertise. 10 However, patients will not be able to experience these benefits should we not enable our provider teams to deliver interventions in a seamless manner. Beyond mHealth eLearning solutions, patients with chronic pain may be further helped through advanced behavior change interventions supported by mHealth and via digital therapeutics such as augmented and virtual reality-based psychology and mindfulness training.31,32 Despite growing evidence of the helpfulness of mHealth solutions for clinical care, and the growing interests on behalf of both patients and providers, little guidance exists into how to best incorporate this new class of tools into routine clinical care.
Although we were able to utilize a robust method for implementation mapping of our mHealth eLearning solutions for patients experiencing chronic pain, our experience had several limitations. We were unable to comprehensively assess the effectiveness of our mHealth eLearning implementation. We did gain insight into the perceived improvement in knowledge and ability to self-manage among a small sample of our end-users, but a more robust study should include a control group to assess for effectiveness of the mHealth eLearning intervention and associated learning objectives. Further assessment would be warranted into engagement with the mHealth eLearning intervention, and the individual tasks completed within the solution. We also appreciate that static, digital education via eLearning will likely not serve all patients in the knowledge retention and behavior changes needed to support them in their experiences with chronic pain. As a result, we are working to build new, interactive experiences utilizing the properties of facilitated self-care as the next iteration of the presented work. The evolving work also engages with end-users (patients) to enhance end-user experience.
Conclusion
Implementation mapping can enable change within healthcare settings, extending the reach of effective interventions into the hands of those who could benefit from them. Leveraging implementation science can facilitate integration and dissemination practical mHealth solutions for patients with chronic health conditions.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231216404 - Supplemental material for Implementation of eLearning solutions for patients with chronic pain conditions
Supplemental material, sj-docx-1-dhj-10.1177_20552076231216404 for Implementation of eLearning solutions for patients with chronic pain conditions by Lindsey M. Philpot, Desiree J. Ahrens, Ryan J. Eastman, Arya B. Mohabbat, Elton A. Mosman, Priya Ramar, Karen J. Reinschmidt, Daniel L. Roellinger and Jon O. Ebbert in DIGITAL HEALTH
Footnotes
Contributorship
Conceptualization (LMP, DJA, RJE, ABM, PR, DLR, JOE); data curation (LMP, PR, DLR); formal analysis (LMP, PR, DLJ); funding acquisition (LMP, RJE, EAM, JOE); investigation (LMP, DJA, RJE, ABM, PR, KJR, JOE); methodology (LMP, PR, JOE); project administration (RJE, EAM); resources (LMP, DLR, KJR); supervision (JOE); visualization (LMP, PR, DLR); writing – original draft (LMP, PR, DLR, JOE); writing – review and editing (LMP, DJA, RJE, EAM, ABM, PR, KJR, DLR, JOE).
Declaration of Conflicting Interests
JOE serves on a scientific advisory board for Applied Aerosol Technologies and a consultant to Exact Sciences not related to the current work. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this investigation was provided by the Mayo Clinic Institutional Review Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Mayo Clinic Midwest Clinical Practice Committee, Mayo Clinic Foundation.
Guarantor
LMP
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.