
Abstract
Objective
WeChat serves as a crucial source of health information, distinguished by its highly personalized nature. Avoidance of such personalized health information has a direct impact on individuals’ health decision-making. This study aims to identify the factors influencing personalized health information avoidance on WeChat and to construct a hierarchical framework illustrating the relationships among these factors.
Methods
A hybrid method was utilized. Semi-structured interviews and grounded theory were used to identify the influencing factors. The interpretive structural modeling (ISM) method was adopted to develop a hierarchical model of the identified factors, followed by matrice d'impacts croises-multiplication appliqué a un classemen (MICMAC) to analyze the dependence and driving power of each factor.
Results
The 20 predictors of personalized health information avoidance were broadly categorized into three groups: personal, informational, and social factors. These factors collectively form a three-tier explanatory framework, consisting of the top, middle and bottom layers. At the root layer, health characteristics and cognition exerted a strong driving force, while negative emotions and affective factors at the top layer showed a high degree of dependence. In contrast, the decision-making cognition, informational factors, and social factors in the middle layer exhibited relatively weaker driving force and dependence power.
Conclusion
This study bridged the research gap of information avoidance by providing new insights targeting the factors influencing personalized health information avoidance behavior on WeChat. It also contributed to enhancing personal health information management and the health information services provided on WeChat.
Introduction
Recently, social media has substantially facilitated the dissemination of health information, 1 with an increasing number of people relying on social media as essential health information sources.1,2 In the United States, nearly 90% of adults turn to social media such as Facebook and Twitter, for a wide array of health-related content, 3 including information on personal health conditions, disease symptoms, treatment experiences, medication recommendations, and wellness tips. 4 The shift toward social media for seeking health information has empowered the general health consumers through informed decision-making and has contributed to greater health literacy.5–7
In China, social media apps such as WeChat and Douyin have similarly become pivotal tools for health information access. According to recent surveys, WeChat is now a primary health information source for 98.35% of the Chinese population, according to recent surveys. 8 Since its launch in 2011, WeChat has evolved from an instant messaging tool into a comprehensive information ecosystem that is deeply integrated with individuals’ health.9,10 Specifically, individuals are able to receive updates on health topics of personal interest through official accounts. 11 In addition, WeChat mini programs are embedded within WeChat in the form of apps, 12 providing users with personal health check-up reports through health monitoring, appointment scheduling, remote consultations, and online diagnosis, while also offering health analysis reports through health tracking and disease prediction.13,14 Furthermore, WeChat groups and moments provide a space for individuals to share their health status with family and friends. It is evident that the above tailored and customized health information on WeChat 15 is directly related to individual health and serves as the primary basis for health decision-making. 16
Despite the accessibility and richness of health information on WeChat, studies have shown that individuals may actively avoid health information.17,18 This behavior, known as health information avoidance, is increasingly prevalent and is a concerning trend.19,20 When individuals avoid health information, they may miss crucial guidance for preventive care, risk management, and timely interventions, which has an impact not only on personal health outcomes, but also on public health on a larger scale. Moreover, the proactive avoidance of general health information may primarily enhance the “filter bubble” and “echo chamber” effects, narrowing users’ perspectives and limiting the breadth of their information access. The avoidance of highly tailored and personalized health information, especially, has a direct impact on individual health decisions and outcomes.
Additionally, from the perspective of cognitive dissonance theory, individuals are more likely to avoid information with a high degree of personal relevance, as they anticipate that such information may challenge or alter their self-concept. 21 If individuals perceive personally relevant information as indicating poor health, 22 or as amplifying their awareness and fear of health risks, 23 they may discontinue their search for information 24 and disengage from information sources, 25 thereby avoiding health information they consider personally relevant. Thus, the personal relevance of health information, which is typically determined by the extent to which a particular topic or issue affects an individual, plays a crucial role in influencing when and why individuals decide to avoid related information. 26
Due to its implications for both public and individual health, health information avoidance has garnered increasing attention from scholars. 27 Existing research primarily focuses on the avoidance of information related to specific diseases such as the COVID-19 pandemic,28,29 breast cancer, 30 colorectal cancer,20,31 and diabetes. 32 In addition, some studies concentrate on analyzing the behavioral characteristics of individuals’ avoidance of unverified,33,34 negative, 17 and erroneous health information, 35 while some research primarily examines health information avoidance behaviors in specific groups, such as Generation Z 36 and the elderly. 37 However, few studies examine how the source and personalized nature of health information influence avoidance behaviors, despite the likelihood that the reasons for avoiding personalized health information differ significantly from those associated with general and average information. Furthermore, most studies assess information avoidance in controlled or experimental settings, where the focus on isolated factors may limit insights into the complex strategies, multidimensional influences, and hierarchical relationships inherent in real-world avoidance behaviors.26,38
Considering WeChat's prominent role in health information engagement in China,
39
this study aimed to explore the behavior and underlying factors of personalized health information avoidance on WeChat to better understand the phenomenon among Chinese social media users. In light of this, the current study explored WeChat to investigate the following research questions:
Q1. What internal and external factors influence the avoidance of personalized health information on WeChat? Q2. What are the interrelationships among these influencing factors? Q3. What are the driving forces and dependence powers of these factors?
The objective of this study was to comprehensively identify the factors influencing personalized health information avoidance on WeChat and their interrelationships. To achieve this, first, in-depth interviews with WeChat users were conducted in real-life contexts, then a grounded theory approach was employed to extract and categorize the relevant factors. Second, the ISM method was applied to analyze the interrelationships among these factors. Third, a MICMAC analysis was performed to evaluate the driving forces and dependence powers of the factors identified.
Literature review
Information avoidance, defined as any behavior aimed at preventing or delaying the acquisition of available but potentially unwanted information, is driven by individuals’ desire to protect cognitive resources and reduce uncertainty.21,23,26,40 Under this concept, the content of the information being avoided must be unknown and the avoidance should not include ignoring information due to a lack of interest, time, or energy. 26 While both information avoidance and information seeking are strategies for sense-making and coping with uncertainty, they are fundamentally distinct.26,36 Information seeking involves individuals recognizing information needs and actively striving to satisfy these needs, which is often characterized by effortful behavior with a high expectation of rewards, 41 whereas information avoidance aims to avoid information that threatens how individuals wish to think, feel, or behave. 42 Furthermore, several concepts are related to, albeit distinct from, information avoidance, including information non-seeking, information ignoring, and selective exposure. Specifically, information non-seeking refers to the absence of proactive information-seeking behavior, whereas information avoidance involves a deliberate effort to avoid attending to or engaging with certain information,21,43 and it occurs less frequently than information non-seeking.41,44 Unlike information ignoring, which is an unconscious behavior of disregarding information, information avoidance is an intentional choice.45–47 Additionally, the distinction between information avoidance and selective exposure lies in the nature of the information encounter, that is, information avoidance typically occurs when individuals actively choose to avoid information due to uncertainty or lack of knowledge about its content, while selective exposure involves the intentionally selecting information that aligns with existing beliefs or attitudes and intentionally avoiding contradictory information.21,48–50
Information avoidance can be categorized into active and passive forms. 51 Active information avoidance refers to deliberate actions taken by individuals to actively prevent exposure to certain information, such as uninstalling software. In contrast, passive information avoidance involves ignoring received information or failing to take further actions to address it, such as neglecting to review a health check-up report.26,52 Moreover, information avoidance typically manifests as behaviors such as selectively obtaining information from certain sources and channels, 53 diverting attention, 54 interpreting information in a biased manner, and engaging in selective forgetting. 55 On many occasions, researchers have observed people's tendency to avoid information. For example, individuals may avoid putting social information in their goal-pursuit journal to circumvent potentially negative comparisons, 56 consumers may avoid digital ads due to perceived goal impediments and prior negative experiences, 57 and researchers may avoid academic information under time pressure. 58 Despite the prevalence of the general phenomenon of information avoidance, it seems to be more prominent in healthcare than in other contexts. For instance, a survey conducted with a nationally representative sample in the United States revealed that 31.1% of adults preferred not to know the likelihood of their developing cancer. 59 Similarly, research by McCloud et al. 60 indicated that about one in three cancer survivors intentionally avoided seeking information on cancer.
The phenomenon of health information avoidance draws much research interest because it seemingly contradicts with some of the traditional assumptions of the information-seeking literature, as Kuhlthau (1993) noted that people are inclined to seek information to alleviate uncertainty. 61 However, a recent meta-analysis 62 revealed that the average observed association between illness uncertainty and health information seeking is nonsignificant, while the correlation between illness uncertainty and health information avoidance is more statistically significant. For example, studies have revealed that cancer patients’ fears contribute to their avoidance of cancer-related information, which manifests as avoidance of cancer discussions and a refusal to seek out relevant information.
In addition to illness, the information overload caused by the explosive growth of health information on social media, 52 the proliferation of low-quality health content, 63 and the heightened perception of health risks 36 can lead to stress and discomfort. Moreover, public health crises confront individuals with significant uncertainty, and thus, uncertainty-related information avoidance is especially apparent in such risk contexts. During the COVID-19 pandemic, researchers spontaneously reported that people worldwide deliberately avoided health misinformation.52,64 Public health crises seem to create a dilemma in which people possess a dual inclination: they aspire to access more valuable health information to mitigate risk, yet they lack the necessary resources to cope with numerous challenges such as information overload, anxiety, and fears. 65 Consequently, they are confused about whether to seek or avoid certain health information.
However, uncertainty is not the sole predictor of health information avoidance. Previous research indicates that feelings of discomfort triggered by health information are key factors driving consumers to steer clear of it. Studies suggested that individuals tend to avoid health information that might challenge their established beliefs, preferences, and habits, to reduce negative reactions and conflicts in health-related decisions makings.66,67 For example, McCloud et al. discovered that smokers intentionally avoid health warnings on cigarette packaging to alleviate their perception of health risks, especially prevalent among individuals with lower socioeconomic status. 68 Some other motives can be found in the literature as well, such as cognitive fatigue stemming from the proliferation of false health information, mitigation of anxiety caused by information overload,69,70 and negative emotions like the fear and disappointment associated with confronting undesirable health-related contents.71,72 Moreover, significant differences in health information avoidance behavior are evident among individuals, depending on their age, gender, education,73,74 health literacy, 75 and their ability and willingness to access information.17,76
Despite the recent proliferation of health information research, studies on health information avoidance remain relatively sparse, especially in comparison to studies on health information seeking, and significant gaps in the literature still exist. First, the prior studies were mostly conducted in disease- or risk-specific contexts and paid little to people's everyday life information practices. We argue that these two areas are inherently different. In day-to-day life settings (e.g., surfing social media), the external stimuli that trigger personalized health information avoidance may not be as apparent as those in disease- or risk-specific contexts. Therefore, we became interested in what motivates people to avoid personalized health information on social media, taking WeChat as an example. Second, it is seemingly clear that health information avoidance involves complex dynamics that stem from various factors, however, it remains relatively unclear how these factors are related to and influence each other, and thus, a further, finer-grained investigation is needed to uncover the structural relationships among the predictors. Motivated by these gaps, this study employed semi-structured interviews, the grounded theory, and ISM and MICMAC approach to examine health information avoidance behavior on a typical social media app WeChat and aimed to explore the influencing factors and underlying mechanisms of health information avoidance among the general population.
Research design
Research methods
This study applied a hybrid approach that integrated semi-structured interviews, grounded theory, ISM, and MICMAC to comprehensively identify the determinants of health information avoidance behavior on WeChat and to elucidate their hierarchical structural relationships. Figure 1 shows the roles of the four methods in the steps of the procedure, which were: (1) identifying the factors that contribute to health information avoidance behavior on WeChat through semi-structured interviews and grounded theory (2) constructing a hierarchical model based on ISM, and (3) analyzing key factors using the MICMAC approach.

Research framework.
Grounded theory is a widely adopted qualitative research method designed to generate theories closely rooted in phenomena, events, or issues through the continuous interplay between data collection and analysis. 77 Based on different philosophical assumptions, grounded theory has been categorized into three main strands: classic Glaserian grounded theory, 78 straussian grounded theory, 79 and constructivist grounded theory. 80 These strands differ in their approaches to induction, deduction, and verification. 81 Among them, straussian grounded theory that is seen by scholars to have more reach and influence.77,82 Building on the foundation of classic grounded theory, straussian grounded theory introduces a systematic and procedural approach, defining the coding process into three distinct steps: open coding, axial coding, and selective coding. 77 Straussian grounded theory is particularly well suited for developing more refined and structured theories directly from data, without relying on prior assumptions. 83 Therefore, we utilized straussian grounded theory to explore the multiple factors influencing personalized health information avoidance behavior on WeChat, examine the intricate interrelationships among these factors, and address the limitations of prior research in terms of analytical depth. Despite its approachable and flexible nature, grounded theory adheres to a structured sequence of well-defined methods for formulating a theory, model, or detailed description. Thus, this study focused on the phenomenon of health information avoidance on WeChat, with the goal of developing a theoretical framework for personalized health information avoidance on the app by arriving at comprehensive explanations through the systematic application of sort encoding, analysis, comparison, and reanalysis.
ISM was employed to unravel the complex interrelationships among the factors that impacted the behavior. This approach, proposed by Warfield, enables the researcher to construct a multilevel hierarchical structural model, which facilitates the transition from a qualitative to a quantitative assessment of these relationships and of any mitigating subjective influences. 84 Additionally, to enhance objectivity and precision in characterizing the interrelations among these factors, we complemented ISM with the MICMAC method, which assisted with the hierarchical categorization and clarified the degrees of interdependency and influence among the factors. 85 The hybrid method has been widely adopted in various fields, including eHealth. 86 technology application, 87 and mobile wallet. 88 We also applied this mixed ISM-MICMAC method to establish the relationships and the degrees of association among the factors influencing personalized health information avoidance behavior. 89
Data collection
Considering the intricate nature of the psychological states involved in avoidance behavior,53,72 we conducted semi-structured interviews to gather qualitative data for the grounded theory analysis. Semi-structured interviews allow for dynamic interactions between interviewers and participants, such that interviewers can extemporize follow-up questions guided by participants’ responses and emotional states. This approach provides participants with the space to articulate their perspectives during the interview process. 90 The flexibility inherent in semi-structured interviews, as emphasized by Barriball and While, 91 proved invaluable for the comprehensive exploration of WeChat health information avoidance.
This study set out to explore the avoidance of personalized health information on WeChat in everyday contexts, targeting interviewees who considered WeChat as a source of health information, had experiences of avoiding personalized health information, and possessed a level of perceptions and understanding of these avoidance behaviors. This selection criterion ensured that the data collected were aligned with the study's research objectives. Purposive sampling and snowball sampling were employed to select the interviewees, which ensured the suitability and sufficiency of the sample. The interviews were organized iteratively, with a pre-test of the initial outline involving three participants (two aged 20–35 and one aged 45–60), which was conducted before the formal start of the interviewing to ensure content validity and practicality. We gathered feedback from the participants to assess the interview's effectiveness and refine the outline. The main interview questions were formulated based on the research objectives, relevant literature, and participant feedback. A detailed outline of the interview questions is provided in Appendix 1. The formal data collection involved conducting in-depth qualitative interviews with a total of 34 participants. To ensure data saturation, an additional 6 interviews were conducted, bringing the total number to 40, each identified by “I + sequence number,” for example, “1–40.” The interviews were conducted in participants’ homes, community activity rooms, and community parks. For those unable to meet face-to-face, supplementary online methods, such as WeChat videos or voice calls, were employed. Each interview lasted between 30 and 50 minutes, with an average duration of 35 minutes, resulting in a total interview time of 1411 minutes.
The interview sample consisted of 40 WeChat users, aged 18–70, from diverse regions, including Guangdong, Sichuan, Jiangxi, Jiangsu, Yunnan, Chongqing and Guangxi. Notably, the group comprised 14 males and 26 females, as detailed in Table 1. The interview sample was well-balanced, encompassing various age groups and educational backgrounds. Moreover, participants exhibited varied patterns of WeChat usage: 6 used it occasionally, 16 frequently, and 18 daily. Most interviewees displayed a high level of familiarity with WeChat. Thus, the sample satisfied the requirements of our research. The recordings were transcribed verbatim by carefully listening to each audio file and cross-referencing with the interview notes, resulting in a total of approximately 110,000 words, with an average of over 2900 words per transcript.
Sample characteristics.

Data analysis
Identification of factors affecting personalized health information avoidance
According to grounded theory, the primary data analysis strategy involves coding the data to develop a theory through three stages: open coding, axial coding, and selective coding.92,93 During the process of coding analysis, it is essential to fix one's attention only on the original data, relinquishing prior experiences, viewpoints, speculations, and assumptions. 94 Concurrently, the investigators remain cognizant of theory, in this case utilizing NVivo software to continually refine and summarize the data for theory development.
Open coding
Open coding is a methodical process that entails a meticulous line-by-line analysis of the original data. Through the refinement and integration of original statements, it gives rise to new concepts that closely approximate the nature of the original data. 95 By systematically coding the interview text, and through an iterative comparative analysis of key statements, we formulated initial concepts, which were then categorized based on their characteristics and connotations. During the open-coding stage, we obtained 63 initial concepts and then generalized the features of these concepts to yield 22 basic categories. Examples of the initial concepts and dimensions formed by the open coding and their representative original statements are shown in Table 2.
Examples of the initial concepts and dimensions formed through open coding.

Note: The “I + sequence number” denotes the respondent.
Axial coding
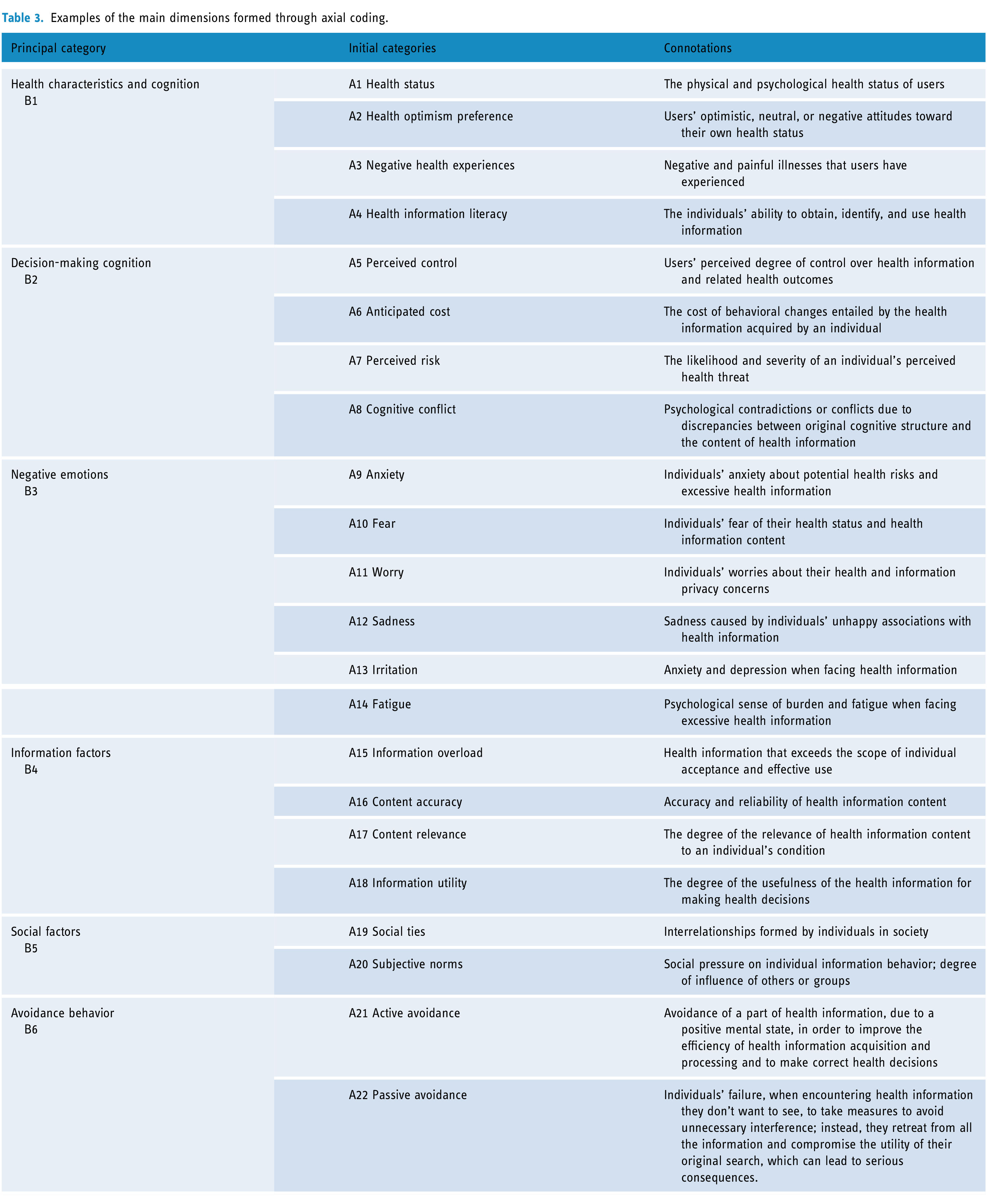
The purpose of axial coding is to systematically classify, abstract, and synthesize the most predominant and crucial factors referred to by users, establishing potential logical connections between categories and concepts, and distinguishing between main categories and subcategories. Simultaneously, it verifies the associative relationships utilizing raw data. 96 We reorganized the factors influencing the avoidance of personalized health information, consolidated the redundant factors, summarized the conceptual categories, and ultimately constructed six principal categories: health characteristics and cognition, decision-making cognition, negative emotions, information factors, social factors, and avoidance behavior, as shown in Table 3. Clearly, most of these factors are closely related to the personalized characteristics of health information on WeChat.
Examples of the main dimensions formed through axial coding.
Selective coding
Selective coding involves refining categories and discovering relationships among concepts. During selective coding, core categories can be extracted from major categories, along with the influential relationships between them. 97 By repeatedly comparing categories, carefully considering the original statements, and thoughtfully examining the relationships among categories, it became evident that avoiding personalized health information was the core category. This avoidance behavior was influenced by six principal categories (the sixth of which marked the distinction between active and passive factors), which were further subdivided into 20 subcategories.
As presented in Table 4, the factors influencing personalized health information avoidance can be broadly categorized into three groups: personal, informational, and social factors. Personal factors, which are internal drivers, include health characteristics and cognition, decision-making cognition, and negative emotions. Specifically, health characteristics and cognition encompass health status, health optimism preference, negative health experiences, and health information literacy. Decision-making cognition includes the four factors of perceived control, anticipated cost, perceived risk, and cognitive dissonance. Emotional factors have a significant impact and include anxiety, fear, worry, sadness, and irritation, as well as fatigue. Informational factors are important external drivers of avoidance, consisting of information overload, content accuracy, content relevance, and information utility. Social factors, also external drivers, come from the social environment; they include social ties and subjective norms.
Summary of the data coding.

Results of the level partitions.

This study sequentially employed open coding, axial coding, and selective coding of the original interview texts to extract the initial concepts and construct the principal and core categories. A detailed summary of the data coding is presented in Table 4.
Theoretical saturation test
Theoretical saturation is an evaluation of the accuracy and reasonability of the concepts and categories formed by researchers through concept extraction and category delineation. 98 It is the stage when no new categories or relationships can be discerned in the data.91,92 To verify whether theoretical saturation was achieved, an additional six participants were interviewed, but no new concept categories or relationships were identified. Therefore, it was concluded that the coding results had reached theoretical saturation.
Construction of ISM model
Based on Moughari’s research, the interpretive structural modeling approach includes four steps: constructing the adjacency matrix, constructing the reachable matrix, dividing the hierarchical relationship, and developing the ISM model. 99
Constructing the adjacency matrix
An adjacency matrix reflects the logical relationships among influencing factors. The twenty subcategories identified through grounded theory were entered into the adjacency matrix as influencing factors. Within the matrix, each value represents the impact of a factor in a given row, 
Furthermore, the adjacency matrix registers only direct relationships among the influencing factors, as extracted from terms such as “resulted in,” “generated,” “helped to,” and “increased” in the interview transcripts, without accounting for indirect impactful relationships.
Constructing the reachable matrix
To further capture indirect relationships among the influencing factors, the transitivity principle was employed to construct the reachable matrix M. That is, if the first factor relates to the second factor, and the second factor relates to the third factor, then the first factor is transitively related to the third factor. The transitivity check continues until the transitivity of all factors in the matrix has been examined. The reachable matrix can be calculated according to the following Boolean rules:
M = the final calculated reachable matrix I = unit matrix
Since there are 20 factors influencing personalized health information avoidance behavior, MATLAB R2020b was utilized to perform several power operations to obtain the reachable matrix M. (The operation code is attached in the last Appendix). In the reachable matrix, 1 indicates the existence of a reachable path between corresponding factors, while 0 shows the absence of both direct and indirect connections between the corresponding row and column factors.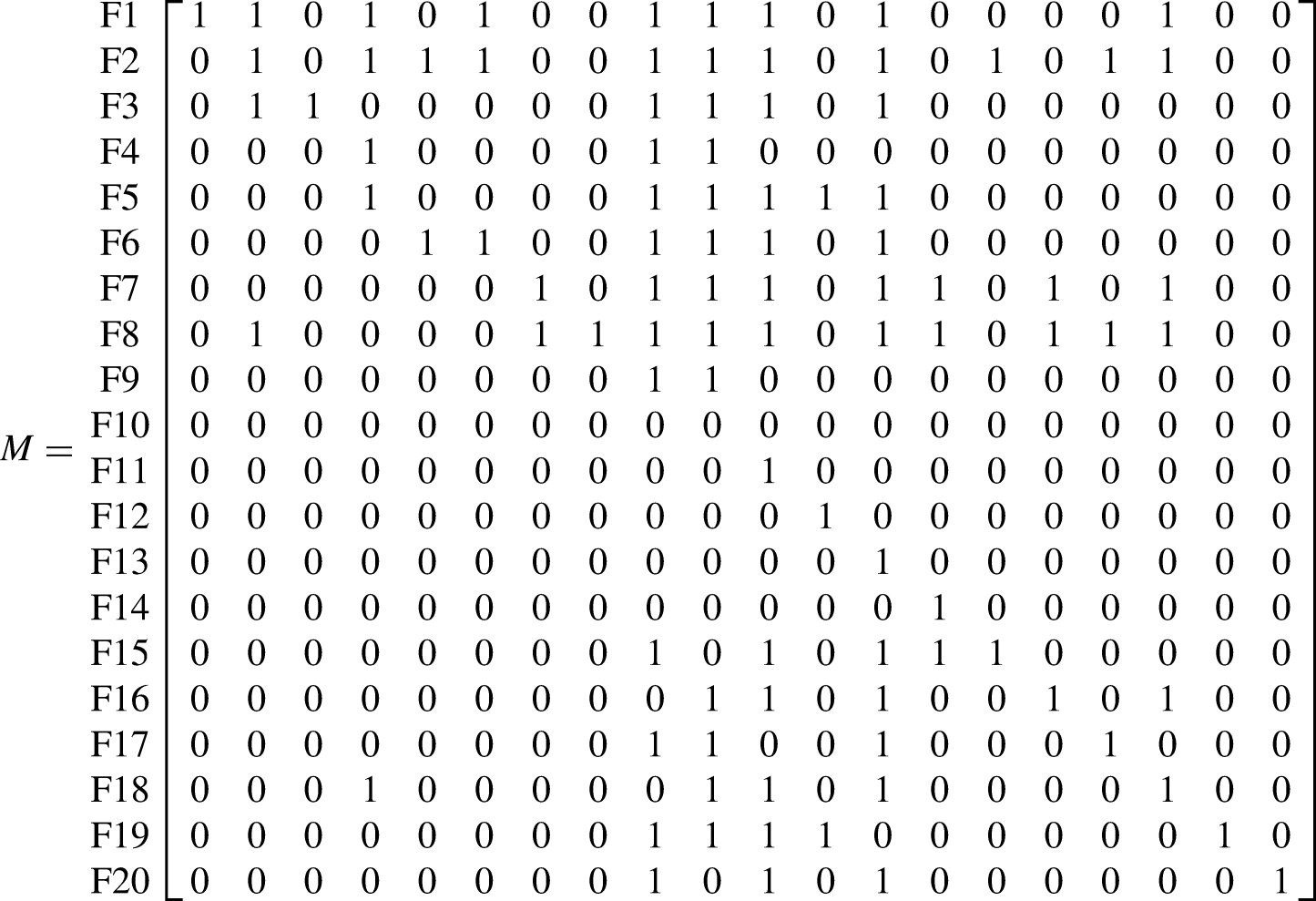
Dividing the hierarchical relationship of influencing factors
According to the reachable matrix M, we obtained the antecedent set 


A top-level factor is a factor achieved with the assistance of all other factors, but one that does not contribute to any factor beyond those at the same level.
101
A top-level factor is identified when
Developing the ISM model
A four-level ISM model of the factors that influence personalized health information avoidance behavior was developed, as displayed in Figure 2, which is based on the hierarchical division and the interactions involving each influencing factor in matrix M. The model illustrates the hierarchical relationships of the twenty influencing factors from the bottom to the top. Levels 3 and 4 consist of fundamental factors that directly affect the factors at level 2 (anticipated cost, perceived control, perceived risk, cognitive conflict, content accuracy, information utility, content relevance, information overload, social ties, and subjective norms). Level 2, in turn, directly affects level 1. Additionally, the four levels can be divided into three layers: a top layer (level 1), a middle layer (level 2), and a bottom layer (levels 3 and 4). Direct and indirect influences operate between layers, ultimately forming chains of factors that contribute to personalized health information avoidance behavior.

ISM model diagram of influencing factors.
MICMAC analysis
A MICMAC analysis was conducted to understand and identify critical factors, based on their driving power and dependence power. According to Mohapatra's method, 102 the former was calculated by summing the value of each row, namely, the values of the influencing factors in the reachable matrix M, while the dependence power was derived by adding the values in each column of factors. Then, all 20 factors were divided into autonomous, independent, linkage, and dependent factors to form a four-quadrant, dependency/driving force classification diagram (see Figure 3).
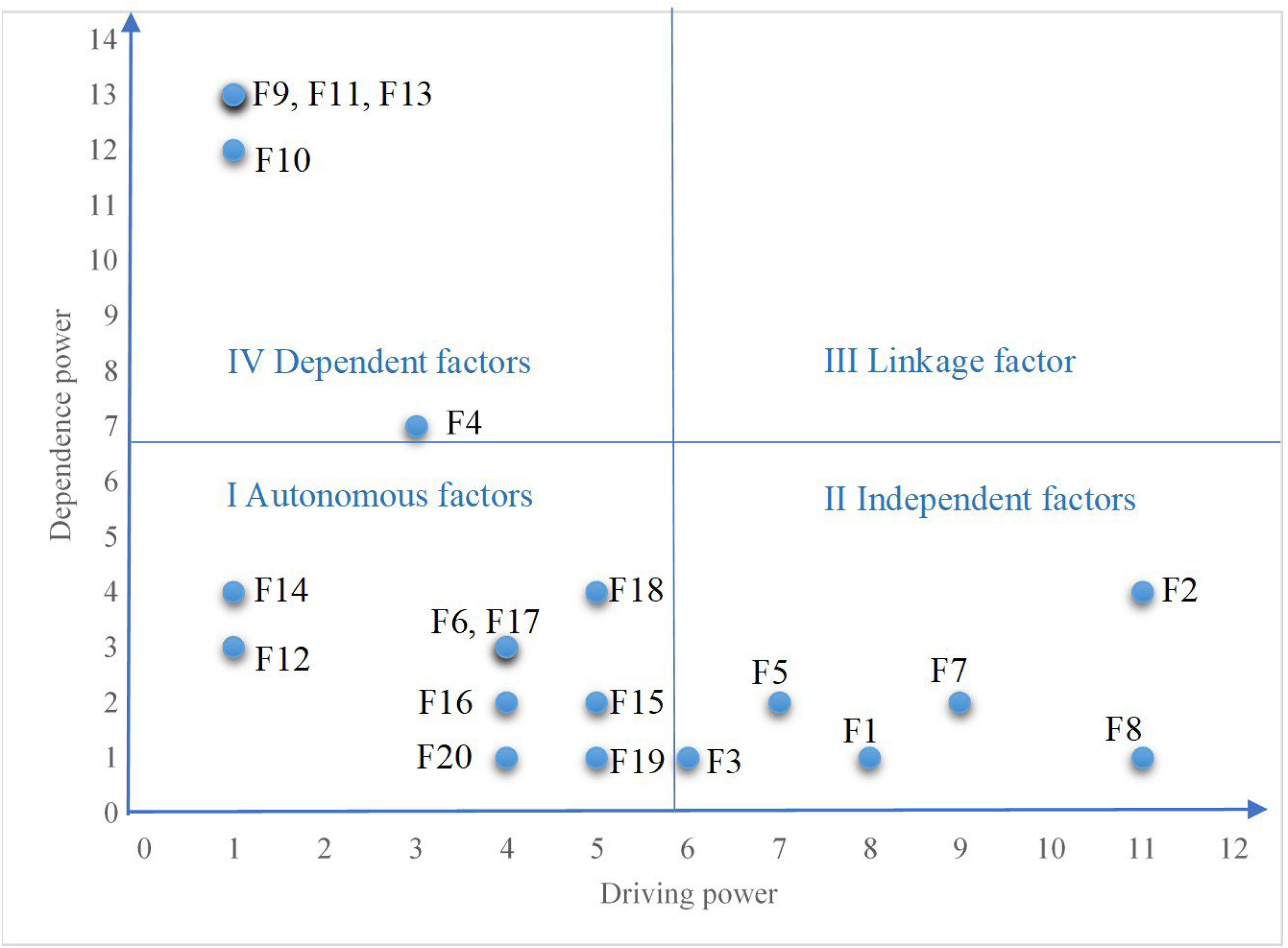
Dependence-driving force classification diagram.
Quadrant I contains the autonomous factors, (F6, F12, F14, F15, F16, F17, F18, F19, and F20), which usually have low dependence and driving power, with minimal influence on WeChat health information avoidance behavior. Most of these are located in the middle layer of the ISM model, including most cognitive factors, information factors, and social factors, which are indirect influencing factors. Autonomous factors are generally relatively stable. The impact of lower-level factors on them usually takes a while to appear, although changes in autonomous factors can lead to more direct and rapid impacts on upper-level factors.103,104
Quadrant II displays the independent factors (F1, F2, F3, F5, F7, and F8), which are critical factors with low dependence and high driving power. The results of the ISM show that most of the independent factors are distributed in levels 3 and 4, likely eliminating or weakening the impact of factors at other levels. 105
Quadrant III typically holds linkage factors, which have both high dependence and driving force; however, no influencing factors fall into this quadrant. This is highly likely attributable to the high instability of linkage factors, as they easily impact other factors and are impacted in turn. 106
Quadrant IV displays the dependent factors (F4, F9, F10, F11, F13), which generally have high dependence and low driving power. These mainly consist of negative affective and emotional factors found at level 1 in the ISM model, and they are easily influenced by other factors and require the support of other factors in the current scenario. 107
To sum up, the classifications arrived at through the MICMAC analysis are generally in line with the ISM model, where the driving power of direct factors in the surface layer is weak and their dependence is high, whereas the driving power and dependence of indirect factors in the middle layer are relatively low. What's more, the dependence of basic factors in the root layer is weak, but these factors exert a strong driving power on WeChat health information avoidance behavior.
Results and discussion
This study identifies and prioritizes twenty predictors classified into four levels, each of which has a different impact on health information avoidance.
The top-layer enablers of health information avoidance
The top-layer factors are related to negative emotions, including anxiety, fear, worry, irritation, sadness, and fatigue. This suggests that emotional discomfort is a direct cause of personalized health information avoidance behavior, which is consistent with Kleiber's point of view toward stress and coping theory, namely, that information avoidance is an emotional management coping style in stressful situations. 108 The RPA model posits that people, in order to alleviate discomfort, 75 tend to avoid information that can increase negative emotions or diminish positive emotions; in other words, information avoidance is expressly a way to regulate negative emotions, such as anxiety, fear, and worry. For instance, when confronted with unfavorable information regarding an increased risk of breast cancer and the associated anxiety, 26 people may resist breast cancer screening and avoid corresponding information. Similarly, fear and anger associated with COVID-19 can induce information avoidance. 109 However, other individuals, driven by sadness and the fear of illness, actively seek out health information rather than try to protect themselves against negative emotions by avoiding it. 52 The decision of individuals to avoid health information primarily depends on the perception of emotional effects before and after acquiring such information. 26 When individuals perceive that the emotional gains from not knowing are greater than those from being informed, they are more likely to exhibit avoidance. Hence, it is evident that the impact of emotions on the avoidance of health information is complex and conditional.
The middle-layer enablers of health information avoidance
The middle-layer factors, found in the second tier of the ISM model, can be divided into three dimensions: (1) decision-making cognitive factors (perceived control, anticipated cost, perceived risk, and cognitive conflict), (2) informational factors (information overload, content accuracy, content relevance, and information utility), and (3) social factors (social ties and subjective norms), which have been confirmed by previous research to be antecedents that contribute to information avoidance. 110 A study by Melnyk and Shepperd 111 revealed that individuals are more likely to engage in information avoidance when the processing of irrelevant health information requires more resources; for instance, information overload was a known reason that people avoided seeking information about COVID-19 during the 2020 pandemic. Individuals who perceive injunctive and descriptive avoidance norms are more inclined to avoid health information. 65 However, our results indicate that cognitive, informational, and social factors at the middle level do not exert a direct impact on information-avoidance behavior. Instead, they contribute to heightened information uncertainty, which might be a proximal cause of negative emotions that directly trigger information avoidance. 26 This also explains nicely why certain studies have found that social norms and cognitive factors have no impact on information avoidance.112,113 Additionally, anticipated cost (F5) and cognitive conflict (F7) fall into the quadrant of driving factors, and these are the key determinants of information avoidance. This finding aligns with the literature, indicating that individuals often tend to avoid information that conflicts with their knowledge and beliefs66,67 and content of low quality and value. 114
The bottom-layer enablers of health information avoidance
The bottom-layer enablers, involving level 3 and level 4 factors in the ISM model, have strong driving power. These factors include health status, negative health experience, health information literacy, and health optimism preference, all of which are not influenced by other factors in the system but have indirect or direct effects on middle-level personal cognitive and informational factors. Specifically, health status directly influences perceived control, perceived risk, and health optimism preference. This is supported by the findings of Elliot et al., who proposed bidirectional associations among perceived control, health risk, and positive/negative emotions. 115 Moreover, health information literacy has been associated with content accuracy, content relevance, and health optimism preference, which means that individuals with higher information literacy find health information easier to comprehend,60,73,116 possess greater health self-efficacy, and have a more optimistic perception of their own health status. Also, our study supports the idea that patients’ negative health experiences (F3), such as bad prior experiences with serious illness or with doctors’ not examining them thoroughly,20,117 tend to lower their level of health optimism, thereby increasing the likelihood that they will avoid health information. 19
Types and results of WeChat health information avoidance
From the results of the interviews, it can be observed that many people engage in information avoidance to some extent, but their situations and their reasons for doing so vary. 118 Moreover, avoidance behavior is regarded as a way to manage information uncertainty and involves active and passive strategies. 119 Active avoidance, typically rooted in high health-information literacy, develops as a response to false, unreliable, or useless information. Exercised with a high level of self-control and self-efficacy, it enhances efficiency in seeking and utilizing health information.120,121 In contrast, passive avoidance, often associated with negative emotions, involves health information that might bring about cognitive conflicts, cognitive overload, comprehension difficulties, or social pressures. 122 Passive avoidance is merely a temporary emotional comfort; it not only diminishes the utility of information but also can lead to adverse consequences such as delays in diagnosing a disease. This, in turn, further intensifies negative emotions like anxiety and fear; therefore, it is necessary to reduce unreasonable and irrational information avoidance. 19
Conclusion
Theoretical implications
This study makes two important theoretical contributions. First, despite the considerable amount of research on health information avoidance,18,123,124 there is still a gap in studies conducted on everyday encounters with personalized health information on social media. Health information avoidance is a diverse and complex phenomenon shaped by a combination of individual, informational, and social factors.26,118 Moreover, the avoidance of personalized health information differs significantly from general or average patterns of health information avoidance; the driving factors of personalized health information avoidance are highly individualized. Among the 20 factors identified, 14 are personal factors and only 4 relate to information characteristics and 2 to social contexts. These personal factors fall into three categories: health status and cognition, decision-making cognition, and emotional responses. Personalization contrasts not only with generality, in terms of greater relevance to the individual and deeper personal engagement, 26 but also with the average patterns of other avoidance behaviors. For example, compared to average disease prevalence rates, personal health examination results have a more pronounced influence on individual health assessments and decision making. 16 Consequently, personal factors play a critical role in shaping personalized information avoidance behaviors.
Second, this study used in-depth interviews and grounded theory analysis to explore the avoidance of personalized health information in everyday life contexts, overcoming the limitations of controlled experiments and predefined hypotheses. The findings comprehensively summarize the multidimensional influencing factors and enrich the literature on information-avoidance behavior. Moreover, the paper stands as a pioneering attempt to introduce the ISM-MICMAC method to construct a four-level hierarchical structure of the factors that influence health information avoidance behavior on social media and to investigate the interdependence of these factors and their impacts on health information avoidance. The causal relationships revealed by the structural framework, grounded in driving power and dependence power, are in keeping with the stimulus-organism-response (SOR) model,125–127 which describes how health characteristics and cognition can act as stimuli to arouse an organism (through decision-making cognition, negative emotions, informational factors, and social factors) and lead to health information avoidance. Thus, the findings clarify the logical relationships among the factors that influence health information avoidance on social media and serve as a valuable guide for further research and practical applications.
Practical implications
The data analysis results show that six negative emotional factors directly impacted avoidance behavior, while another six influencing factors (health status, health optimism preference, negative health experiences, anticipated costs, cognitive conflicts, and health information literacy) exerted strong driving forces, followed by information overload, information utility, and social ties. Therefore, the article puts forward noteworthy practical implications.
First, health information avoidance, as an adaptive strategy for dealing with uncertainty, may enhance the efficiency of information seeking, but it may also lead individuals to overlook health information that is beneficial to them.26,117 Hence, it is imperative to guide user behavior toward rational avoidance. To counteract or alleviate negative emotions such as anxiety and fear, individuals might start by mitigating their perceptions of threat.128,129 Introducing elements of music, games, and entertainment into health information can foster curiosity 130 and induce positive emotions—for instance, offering emotionally engaging, interesting, and persuasive videos rather than explanatory text, or developing entertaining mini-games on WeChat to disseminate health knowledge. Additionally, self-regulation techniques can be considered, 131 such as using the psychological contrast between negative future outcomes and positive present realities to effectively alleviate the information avoidance related to specific diseases.
Second, individuals need to recognize the crucial roles of health status, negative health experiences, and health literacy in health information avoidance. On one hand, people need to actively monitor their physical condition, assess and control their health status objectively and in a timely manner, understand the costs associated with the behavioral changes prompted by health information, and act to prevent information avoidance due to excessive optimism or pessimism. On the other hand, to enhance the health-information literacy of WeChat users, governments could collaborate with communities, schools, libraries, hospitals, and health commissions to regularly organize activities to disseminate health knowledge. 28 For example, they could set up dedicated public accounts or video channels on WeChat that offer regular courses on health-information literacy and provide targeted training for information-poor groups such as the elderly, low-income individuals, farmers, and people with low education levels. 27
Third, the abundance of health information on the WeChat platform may lead to information overload and reduce information utility,121,132 which is not conducive to effective health-information seeking. 65 The dissemination of a large amount of misinformation and disinformation can cause information overload; therefore, WeChat should provide users with health information that is clearly sourced 133 and matches their needs. Specifically, the platform could require information senders to cite sources to enhance the credibility of health information and use human-AI collaboration methods to identify fake or misleading information, semantically and contextually, while also promptly debunking information through official accounts and removing false information. These measures would strengthen users’ perception of the utility of health information available on WeChat. Additionally, governments could enact and enforce stricter policies to reduce the dissemination of health misinformation and disinformation on social media. 134
Limitations and future research
Although this study involved a fairly comprehensive analysis of the factors that influence people's health information avoidance on WeChat, it had certain limitations. First, it should be noted that grounded theory relies on small-scale data that primarily capture subjective user experiences. Therefore, the conclusions drawn from this study have not been validated with a large-scale dataset. Future research could integrate large datasets and machine-learning methods to conduct a more in-depth investigation. Second, the interview sample encompasses a variety of groups, however, the limited number of participants from each group may result in insufficient representation of certain populations, potentially limiting the generalizability of the research findings. Future studies could optimize the conclusions by expanding the sample size or integrating quantitative methods. Third, despite that our theoretical model passed the saturation test, there is still the possibility that certain factors were missed. Future research could benefit from expanding the scope of the study to encompass a broader population to extend the findings currently found in the literature. Fourth, this study did not account for the dynamic adaptability of information-avoidance behavior, nor did it categorize different types of health information. Future research could integrate experimental and survey methods to meticulously investigate the adaptive strategies of information avoidance adopted by WeChat users in various contexts.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251314277 - Supplemental material for A model for predicting factors affecting health information avoidance on WeChat
Supplemental material, sj-docx-1-dhj-10.1177_20552076251314277 for A model for predicting factors affecting health information avoidance on WeChat by Minghong Chen, Xiumei Huang, Yinger Wu, Shijie Song and Xianjun Qi in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251314277 - Supplemental material for A model for predicting factors affecting health information avoidance on WeChat
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251314277 for A model for predicting factors affecting health information avoidance on WeChat by Minghong Chen, Xiumei Huang, Yinger Wu, Shijie Song and Xianjun Qi in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251314277 - Supplemental material for A model for predicting factors affecting health information avoidance on WeChat
Supplemental material, sj-docx-3-dhj-10.1177_20552076251314277 for A model for predicting factors affecting health information avoidance on WeChat by Minghong Chen, Xiumei Huang, Yinger Wu, Shijie Song and Xianjun Qi in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to acknowledge and thank all the volunteers who participated in the interviews.
Contributorship
MC wrote the article and oversaw the study; XH contributed to the article review and revised the article; YW collected and analyzed the data for the study; SS contributed to the article review; XQ, the corresponding author, headed the study, including putting it forward and carrying it out. All the authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
We obtained electronic consent from the participants during recruitment through social media. Additionally, since the study did not involve biomedical issues, it was exempt from the requirement to obtain written consent according to the institutional review policy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Office for Philosophy and Social Sciences, Guangdong Province Philosophy and Social Science Project (grant number 24BTQ032, no. GD24CTS05).
Guarantors
MC and YW.
Supplemental material
Supplemental material for this article is available online.
Appendix
Interview outline.

| Index | Key elements | Themes |
|---|---|---|
| 1 | Demographic characteristics of the participants: gender, age, educational background, frequency of and proficiency with WeChat use. |
Participants’ experiences related to WeChat health information avoidance behavior Factors that influence WeChat health information avoidance behavior |
| 2 | Have you ever experienced information-avoidance behavior when faced with various types of health information on WeChat? Please give specific examples. | |
| 3 | Under what circumstances do you usually choose to avoid health information on WeChat? What are your reasons for avoiding health information on WeChat in this situation? What motivates you to avoid health information? Under what circumstances would you not normally choose to avoid health information on WeChat? What are the reasons for not avoiding at this time? |
|
| 4 | How would you rate your previous health information avoidance behavior on WeChat? Do you think this avoidance behavior has had the desired effect on you? What impact did it have on your health perceptions and health behaviors? | |
| 5 | In what ways do you avoid health messages on WeChat? | |
| 6 | Apart from the reasons mentioned above, do you think there are any other factors that cause you to avoid health messages on WeChat? |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.