
Abstract
Objective
Digital health interventions for behaviour change are usually complex interventions, and intervention developers should ‘articulate programme theory’, that is, they should offer detailed descriptions of individual intervention components and their proposed mechanisms of action. However, such detailed descriptions often remain lacking. The objective of this work was to provide a conceptual case study with an applied example of ‘articulating programme theory’ for a newly developed digital health intervention.
Methods
Intervention Mapping methodology was applied to arrive at a detailed description of programme theory for a newly developed digital health intervention that aims to support cardiac rehabilitation patients in establishing heart-healthy physical activity habits. Based on a Predisposing, Reinforcing, and Enabling Constructs in Educational Diagnosis and Evaluation (PRECEDE) logic model of the problem, a logic model of change was developed. The proposed mechanisms of action were visualised in an acyclic behaviour change diagram.
Results
Programme theory for this digital health intervention includes 4 sub-behaviours of the main target behaviour (i.e. habitual heart-healthy physical activity), 8 personal determinants and 12 change objectives (i.e. changes needed at the determinant level to achieve the sub-behaviours). These are linked to 12 distinct features of the digital health intervention and 12 underlying behaviour change methods.
Conclusions
This case study offers a worked example of articulating programme theory for a digital health intervention using Intervention Mapping. Intervention developers and researchers may draw on this example to replicate the method, or to reflect on most suitable approaches for their own behaviour change interventions.
Keywords
Introduction
Ischaemic heart disease is a major cause of mortality and morbidity, accounting for 16% of global deaths1,2 and representing the most frequent cause for disability-adjusted life years in age groups 50 years and older. 3 Regular heart-healthy physical activity (PA) is a crucial behaviour for the primary and secondary prevention of ischaemic heart disease and other cardiovascular diseases (CVDs). For example, a recent study demonstrated that every increase in PA by 500 metabolic equivalent of task minutes per week results in a 14% and 7% risk reduction in mortality in the secondary and primary prevention of CVD, respectively. 4 Therefore, exercise-based cardiac rehabilitation is a central component of secondary CVD prevention. Exercise-based cardiac rehabilitation is a multi-disciplinary programme targeting multi-factorial cardiovascular risk factors with a specific focus on physical inactivity. 5 As a general recommendation, patients with CVD should carry out aerobic PA on at least 3 days per week at moderate to high intensity, and muscle strength training twice per week. PA should provide an energy expenditure of 1000 to 2000kcal/week. 6
Importantly, patients with CVD should establish ongoing (and life-long) PA habits, to reduce their risk of recurring cardiovascular events and death, and to improve their physical functioning and quality of life. However, this remains a major challenge. In the 2017 EUROASPIRE V survey of 8261 patients with CVD who were interviewed at median 1.1 years following an acute coronary event, only 34% of patients reported performing regular PA (i.e. ≥ 30 min on average 5 times a week); only 35% reported performing planned PA to increase physical fitness; 42% of patients did not perform regular PA and had no intention to do so in the next 6 months; and 46% of patients did not recall having received personal advice on PA. 7 Moreover, a systematic review of 26 randomised controlled trials (8593 patients) showed that completion of a cardiac rehabilitation programme did not result in a clear positive impact on sustained heart-healthy PA behaviour compared with patients who did not participate in such a programme. 8 Thus, there is an urgent need to develop effective support for CVD patients’ behaviour change and habit formation for regular heart-healthy PA.
Digital health interventions have the potential to offer suitable solutions that contribute to addressing this problem. For example, in a recent systematic review of 14 randomised controlled trials (1497 patients), digital health interventions showed positive effects for promoting PA following completion of a cardiac rehabilitation programme (pooled effect size assessed as standardised mean difference (SMD) = 0.35; 95% confidence interval (CI) 0.02–0.70; p = 0.04). 9 Moreover, several systematic reviews support patient safety of digital health interventions in cardiac rehabilitation, for example the studies by Wongvibulsin et al. 10 and Antoniou et al. 11 However, it is notable that digital health interventions for CVD secondary prevention are typically very heterogeneous – including building blocks such as websites, text messages, wearable sensing devices, smartphone apps and virtual reality programmes – and little information is available on their underlying programme theory; that is, what intervention components are expected to lead to which changes. 9 This runs contrary to methodological recommendations and reporting guidelines for behaviour change interventions, such as the United Kingdom Medical Research Council's framework for developing and evaluating complex interventions, 12 the Template for Intervention Description and Replication (TIDieR) checklist, 13 the Workgroup for Intervention Development and Evaluation Research (WIDER) 14 and others.15,16
Digital health interventions that aim to support behaviour change are often complex interventions, in the sense that they may combine a number of components and target a number of behaviours. 12 Developers of complex interventions should ‘articulate programme theory’ 17 ; that is, they should describe all individual intervention components (‘active ingredients’) and their proposed mechanisms of action, and they should make transparent the rationale(s) for intervention components and proposed mechanisms of action, including underpinning theories and/or empirical evidence. Such an explicit description of the complex intervention and its (proposed) workings can be helpful to communicate the importance and function of intervention components to others, 13 and to select appropriate evaluation designs that capture the relevant processes and outcomes. 12 At a wider scientific and societal level, detailed intervention descriptions support transparency, reproducibility and the reduction of waste in research.18,19 However, despite available guidance, the articulation of programme theory for complex behaviour change interventions remains lacking.20,21 It may be presumed that the reasons for this include lack of time and resources, lack of awareness, and lack of methodological knowledge, but there is little data to explain why this problem persists. However, one contributing factor may be the limited availability of applied (‘worked’) examples that demonstrate how this can be realised in practice. Such applied examples can arguably raise awareness, offer methodological guidance, and possibly reduce the cost and effort required for intervention descriptions, by providing practical examples to relate to.
In this article, we therefore describe a conceptual case study with an applied example of ‘articulating programme theory’ for our newly developed digital health intervention
Methods
We present a conceptual (descriptive) case study with an applied example, describing the retrospective application of IM to articulate programme theory for an existing digital health intervention. This work was conducted in spring 2023 at the Ludwig Boltzmann Institute for Digital Health and Prevention in Salzburg, Austria.
The aktivplan digital health intervention
The
A digital planning calendar for regular heart-healthy PA and exercise is a central component of the

The healthcare professional's view of the
In clinical practice, the
Patients can view the planning calendar via the

The patient's view of the
Further functions of the
Intervention Mapping
IM is a six-stepped approach (Figure 3) for the systematic development, implementation and evaluation of health promotion programmes. 26 The six steps are each broken up into smaller tasks. Upon completion, these smaller tasks provide a basis from which the subsequent step is started.
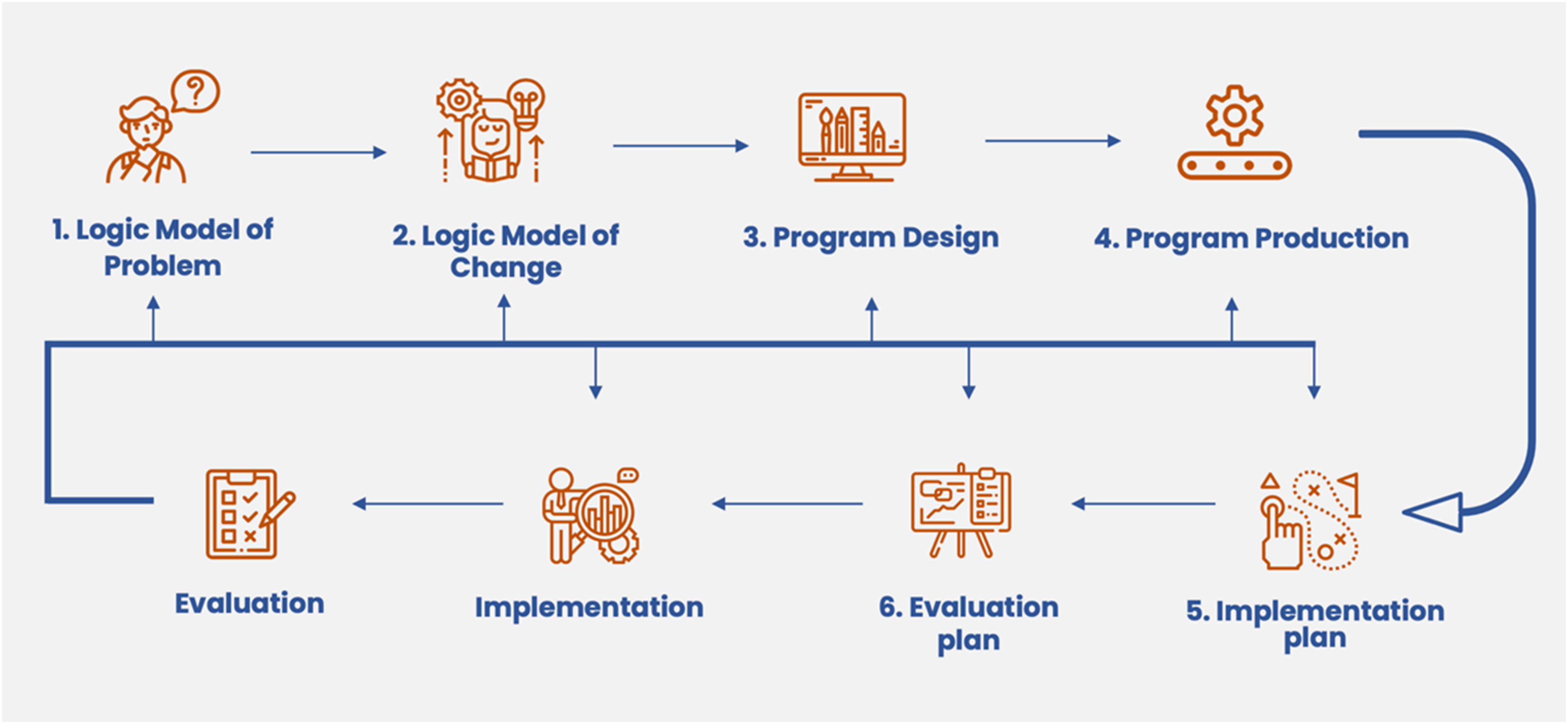
The six steps of Intervention Mapping.
The first step of IM starts by forming a planning group that consists of the programme planners, community members and programme beneficiaries among others. This mirrors the group of contributors in a user-centred design process, for example, patients and experts from different disciplines in our development of the
The second step comprises of stating behavioural and environmental outcomes, specifying performance objectives (POs) and change objectives (COs), selecting determinants for the behavioural and environmental outcomes, and constructing matrices of change. POs are the sub-behaviours necessary to perform a desired target behaviour, and COs are specific changes needed at the determinant level to achieve those sub-behaviours. These COs result from crossing POs with their related personal determinants. The final product of the second step is a logic model of change.
The third step consists of generating programme themes, components, scope and sequence. Matching the previously generated COs with theory-based and evidence-based behaviour change methods and selecting or designing practical applications to deliver the change methods conclude the third step.
The fourth step starts off by refining programme structure and organisation, whereafter plans for programme materials are drafted. Programme messages, materials and protocols are developed in collaboration with designers. The final task of the fourth step is to pre-test, refine and produce programme material. After the fourth step, the development of the intervention programme is finalised.
Step 5 relates to the implementation of the programme. It is a repetition of the first three steps of IM and starts off by identifying programme adopters, implementers and maintainers, for whom outcomes, POs and COs are developed in terms of programme use. This step is finalised by constructing matrices of change and designing implementation interventions.
The sixth and final step of IM concerns the evaluation of the programme. The evaluation is split into effect and process evaluation. First, questions in regard to the evaluation are formed. Then, indicators and measures for assessment are developed, the evaluation design is specified and finally, the evaluation plan is completed.
Within each IM step, many planning questions will be raised. These are answered using the core processes of IM. Core processes are a helpful and systematic way to answer planning questions during intervention development, supporting a complete understanding of the problem, which is imperative for finding effective and appropriate solutions.26,28 The six core processes need to be conducted in order and are as follows: (1) posing questions, (2) brainstorming potential answers, (3) reviewing findings from empirical literature, (4) reviewing theories, (5) assessing and addressing needs for new data, and (6) developing a working list of answers. 26
Applying Intervention Mapping to articulate programme theory for aktivplan
The six steps of IM as described in section Intervention Mapping lay out the entire sequence of developing and evaluating a health promotion programme (or behaviour change intervention) anew, from initial conceptualisation to intervention development, implementation planning, and formative and summative evaluation. Orienting ourselves on this IM sequence, our
First, the target population and main behavioural outcome were defined. Because user-centred design methodology includes a thorough needs assessment and close involvement of intended users (cardiac patients and rehabilitation professionals), we had rich data to inform the PRECEDE model and to devise the logic model of the problem (IM step 1).
Before moving on to IM step 2, we sought to ascertain all psychological determinants addressed in
We then completed the tasks of IM step 2. Based on the different
Lastly, we combined all these aspects in an acyclic behaviour change diagram (ABCD) matrix. ABCD matrices assist in more clear and transparent communication of processes in intervention development.
29
The ABCD matrix provides a complete overview and enables the creation of a graphical representation of the ‘logic chain’ between any single
Results
The logic model of the problem
Figure 4 shows the logic model of the problem which the

Logic model of the problem.
Based on the logic model of the problem, we define the main programme goal (the main behavioural outcome) as ‘following discharge from a cardiac rehabilitation programme, cardiac patients independently and regularly carry out the recommended amount of heart-healthy PA over months and years’.
aktivplan features mapped to behaviour change methods
The
aktivplan features mapped to behaviour change methods, determinants and theories.

Of note, the intervention does not aim to change readiness for behaviour change, but rather the intervention is purposively timed to coincide with a moment when patients are likely to be receptive to behaviour change.
HCP, healthcare professional.
As one important aspect of the application,
Within this collaborative relationship between HCP and patient,
Additionally, the
Goal setting is another major factor of the
Furthermore,
In terms of its implementation in the cardiac rehabilitation patient pathway,
In addition to the individual effectiveness of these behaviour change methods, in their systematic review on lifestyle modification programmes for patients with coronary heart disease, Janssen et al.
70
reported on the synergetic effects of behaviour change methods, including goal setting, self-monitoring, planning and feedback, in changing lifestyle behaviours. All these methods are effectively incorporated into the
The logic model of change for aktivplan
We defined four POs for the target population. In sum, these four sub-behaviours contribute to the main behavioural outcome of the target population:
PO.1 Patients plan their weekly PA sessions in the PO.2 Patients complete their minimum recommended amount of weekly PA; PO.3 Patients monitor their PA using the PO.4 Patients adapt PA plans according to their own capabilities in collaboration with their HCP.
61
After defining these POs, we conducted literature searches on the personal determinants associated with these behaviours. Thereafter, we conducted a comparative analysis between the identified determinants and those addressed by the
The acyclic behaviour change diagram for aktivplan
The ABCD in Figure 5 gives a complete overview of all POs, COs, determinants, behaviour change methods, and practical applications (i.e. the corresponding features of

Acyclic behaviour change diagram (ABCD) for the
For example, the
The ABCD matrix in the online supplemental file (tab ‘ABCD – patients’) gives a tabular presentation of the content in Figure 5.
Discussion
We applied the IM approach to ‘articulate programme theory’ for our digital health intervention
Practical use of the logic model
As already stated, at a wider scientific and societal level, detailed intervention descriptions support transparency, reproducibility and the reduction of waste in research.18,19 At a more immediate level, one practical use of the
Another practical use for our logic model is to support our communication about
With regard to the evaluation of the
Possible disadvantages of developing a detailed logic model
There are some considerations which might preclude developing such a detailed logic model as presented in this article. The required expertise in the IM methodology or the required time resources might not be available. From a design perspective, such an analytic dissection of the intervention as presented in this example might take away from the more creative ‘designerly intuition’ and ‘abductive reasoning’ that is characteristic for co-design approaches. 79 In the retrospective development of the logic model, initial design intentions might be misrepresented, and intervention components mapped inappropriately. Similarly, one could get lost in the details of the logic model and lose sight of a clear design focus and vision. In any case, intervention developers should work up a type of logic model for their digital health intervention, and approaches that require less detailed description and justification of psychological mechanisms and theories than in the example presented here are available (see section Other approaches for the retrospective development of a logic model). 17
User-centred iterative co-design meets Intervention Mapping
As demonstrated in this work, user-centred design and IM can both be integrated in the development of digital health interventions for behaviour change, building on the strengths of both methodologies, each underpinned by complementary principles. User-centred design, with stakeholder involvement and iteration as key tenets, emphasises the involvement of end-users at every stage of the design process, fostering a deep understanding of user needs and preferences. 80 This approach aligns closely – and is often used in conjunction – with co-design, which involves stakeholders, including users, in the creative process to ensure that the outcomes are both usable and meaningful. 81 IM, a systematic approach for health promotion programme planning, encompasses six iterative steps as detailed above: needs assessment, formulation of change objectives, selection of theory-based methods and practical strategies, programme design, adoption and implementation planning, and evaluation planning. 22 Similarities between user-centred design/co-design and IM are their iterative nature and shared commitment to a systematic, user- (or human-)focused approach. Both methodologies highlight the understanding of user context and needs, albeit with different emphasis – user-centred design/co-design through direct user involvement and iterative testing, and IM through a structured analysis of the problem and possible solutions together with the target population and other relevant stakeholders. Both approaches complement each other in their theoretical underpinnings and scope. While user-centred design and co-design are grounded in design theory and primarily focus on product usability and satisfaction, IM initiated from the field of health promotion and encompasses a broader range of considerations, including the effectiveness of interventions in changing (health) behaviours. This is critical in the context of digital health interventions, where the convergence of these approaches can leverage the strengths of each – user-centred design/co-design enhancing user engagement and adherence in close interplay with digital health intervention feature design, and IM ensuring the intervention's theoretical robustness and practical effectiveness in behaviour change.82, 83
Other approaches for the retrospective development of a logic model
As stated above, there are approaches to constructing a logic model for a complex intervention that require less detailed description and justification of psychological mechanisms and theories than in the example presented here. O'Cathain et al. 17 describe a more basic structure for a logic model of a complex intervention, which starts from ‘principles’ and links sequentially to ‘actions to consider’, ‘intervention’, ‘outputs’, ‘short term effects’ and ‘long term effects’. A similarly basic logic model structure is described in the frequently cited ‘Logic Model Development Guide’ by the Kellogg Foundation 84 which takes ‘resources/inputs’ as a starting point and links sequentially to ‘activities’, ‘outputs’, ‘outcomes’ and ‘impact’. Diagrammatic representations of such logic models are often seen in scientific publications of complex interventions, for example, in Cook et al. 85 Nevertheless, for a digital behaviour change intervention even such a basic logic model will need to include reference to behaviour change methods and/or theory. 13 To achieve this in retrospect, an approach applied in the systematic review by Patterson et al. 86 can be appropriate, by which descriptions of digital health interventions according to the TIDieR checklist were mapped against a comprehensive classification of behaviour change methods and theories – in this case the behaviour change technique taxonomy developed by Michie et al. 87 As described in section Practical use of the logic model, an ABCD may also be developed as a ‘stand alone’ tool, to offer a visual representation in support of a logic model that has been developed via a framework other than IM. 29
Another approach for ‘reverse-engineering’ a logic model for an existing intervention has been described by Walker et al. 16 Termed ‘Evidence-Based Intervention (EBI) Mapping’, this approach is similar to our example, as it also applies IM methodology retrospectively. However, the primary motivation for EBI Mapping is to support uptake of interventions with proven efficacy or effectiveness (EBIs) in practice, whereas our approach prioritises systematically analysing existing interventions regardless of their evidence base to understand their components and logic, offering necessary insights for their evaluation, potential adaptation or enhancement. In EBI Mapping, the suggestion is that a detailed description of an EBI's goals, components and theory of change will help potential adopters judge and decide whether the EBI could be suitable for their particular population and context. Walker et al. define four stepwise tasks – identifying the who, what, why and how of an EBI – to arrive at a logic model that lists practical applications, change methods, determinants, health behaviour, health outcome and health problem. In contrast to our example, EBI Mapping does not include an ABCD with its detailed specification of POs and COs and its depicted (proposed) causal linkage between individual behaviour change methods, applications, COs, determinants and POs; and the suggested use of EBI Mapping is mainly to inform potential adopters of an EBI about suitability of the intervention and adaptation needs for their particular setting. 16
Strengths and limitations
A strength of our work is the comprehensive and practical description of the retrospective application of IM to ‘articulate programme theory’, providing readers with sufficient detail to replicate the approach. Moreover, because IM is a well-established and actively taught methodology, readers seeking further guidance on the application of IM may draw on current scientific publications and educational resources about IM. Another strength of our approach is its compatibility with user-centred design/co-design, enabling synergies between this prevalent paradigm in modern design thinking and the psychologically and theoretically informed underpinning logic of a behaviour change intervention that is generated through IM.
We acknowledge limitations to our work. The approach may be limited by lack of access to intervention contents and materials, especially when the development of the logic model is conducted by persons who are outside the intervention development team and who may rely on scientific publications and other publicly accessible information about the intervention. Differing conceptual understandings and definitions of terms may add to this difficulty. Another limitation concerns the possibility that the delineation of intervention features, determinants, behaviour change methods and theories may not be obvious or straightforward, and decisions may to some extent require judgement calls or group consensus. We recommend that an attempt is made to create a suitable stakeholder group, ideally including representatives from the intervention development team, so that access to intervention contents and materials is granted and accounts of the ‘history’ of intervention development can be provided. This stakeholder group may then constitute the forum in which concepts, definitions and decisions are discussed and agreed upon.
While the example presented in this article only addressed the behaviour of the at-risk populations (i.e. patients who had an acute cardiac event), a logic model may also extend to include various environmental agents. However, the roles of environmental agents can sometimes overlap with those of implementers (i.e. the persons involved in the adoption, implementation and maintenance of an intervention), 26 creating potential for lack of conceptual clarity in this respect. 16
Recent literature calls for introducing more flexible and dynamic logic models to incorporate elements of interaction between an intervention and the context within which it is deployed15, 88 including considerations of potential intervention harms and their mechanisms of action. 89 We acknowledge that this is not accounted for in our example.
Conclusion
It is important to make transparent the indented – or hypothesised – workings of digital health interventions, by ‘articulating programme theory’. This article offers a conceptual case study and a worked example, applying IM to retrospectively develop a detailed logic model of an existing, co-designed digital behaviour change intervention for physical activity in cardiac rehabilitation. Intervention developers and researchers may draw on this example to replicate the method, or to reflect on most suitable approaches for ‘articulating programme theory’ for their own interventions. Publications of similar case studies and worked examples from other clinical use cases can enrich and support researchers’ practice of articulating programme theory.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076241260974 - Supplemental material for Making it transparent: A worked example of articulating programme theory for a digital health application using Intervention Mapping
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076241260974 for Making it transparent: A worked example of articulating programme theory for a digital health application using Intervention Mapping by Tamika A. Marcos, Rik Crutzen, Veronika Leitner, Jan D. Smeddinck, Eva-Maria Strumegger, Daniela Wurhofer and Stefan T. Kulnik in DIGITAL HEALTH
Footnotes
Contributorship
STK and RC conceived the work. TAM developed the logic model with support from STK and RC. VL, JDS, E-MS and DW peer reviewed and validated the logic model. TAM and STK wrote the first draft of the manuscript; and E-MS, RC and JDS contributed to the manuscript draft. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
STK
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.