
Abstract
Objective
To assess the effects of WeChat platform-based continuing care for arthritis on patients’ self-management, self-efficiency, quality of life (QoL), and medication compliance.
Methods
A study was conducted on arthritis patients recruited between December 2017 and February 2018 and divided into two groups. The intervention group received continuing care from the WeChat platform and regular follow-ups, while the control group only received regular follow-ups. The outcomes in both groups were assessed using questionnaires twice: before the study (T0) and eight weeks after T0 (T1), which consists of the evaluation of self-management, QoL, self-efficacy, and medication compliance.
Results
There were 23 people in each of the intervention and control groups completed two outcome measures. At eight weeks, participants in the intervention group showed an improvement in psychological QoL, cognitive symptom management, and self-efficacy, compared to the control group (QoL scores: mean difference in change between groups was 12.29, 95% CI: 4.51, 20.07, p < 0.001; cognitive symptom management: mean difference in change between groups was 0.65, 95% CI: 0.24, 1.05, p < 0.001; self-efficacy: mean difference in change between groups was 0.69, 95% CI: 0.14, 1.24, p < 0.05). Self-management, self-efficacy, and psychological quality of life were significantly improved in the intervention group before and after the intervention (p < 0.05).
Conclusion
Using the WeChat platform for continuing care is useful in improving the psychological state, self-efficacy, and self-management ability of patients with arthritis. The study is relevant to Clinical Practice.
Keywords
Introduction
Arthritis generally refers to a chronic disease caused by inflammation, infection, degeneration, and trauma in human joints and their surrounding tissues. 1 Some types of it include rheumatoid arthritis (RA), ankylosing spondylitis (AS), and osteoarthritis (OA). Arthritis is a growing public health problem in adults worldwide. 2 It cannot be cured due to the degenerative changes in the joints, which manifest as joint stiffness, swelling, pain, progressive joint destruction, and even disability, all of which significantly affect health-related quality of life (QoL). 3 As a chronic disease, arthritis requires long-term medication and functional exercise at home. For this reason, family continuing care is indispensable and crucial as it contributes to improved medication compliance, self-management ability, and patient QoL.
Arthritis is one of the most common causes of disability, greatly impairing QoL due to pain and joint dyskinesia. 4 Its prevalence is high worldwide, especially in Europe and North America. 5 In China, the overall prevalence of arthritis among middle-aged and older adults was 31.4% in 2014. 6 As the population ages, the prevalence of arthritis is expected to increase. Moreover, its prevalence may worsen poverty if patients fail to manage their arthritis, as it can affect their ability to work and live independently. 7
The incidence of arthritis symptoms and health-related QoL is closely related to the level of self-management. Self-management education includes formulating and implementing scientific and effective rehabilitation plans, changing poor health behaviors, and correcting any misconception about the disease. To improve the self-efficacy of patients and slow the progression of arthritis, more awareness must be raised about its etiology, symptoms, treatment, prognosis, and dos and don'ts during acute and chronic stages.
As a chronic disease, continuous care outside the hospital is crucial. Various health problems caused by arthritis often occur at home, which requires patients to acquire certain knowledge and self-management skills to monitor their condition after discharge and better cope with symptom changes. Continuing care enables patients to receive collaborative and continuous nursing care in different settings, such as hospitals different departments within hospitals, homes, or healthcare facilities. It generally refers to patients accepting the discharge plan drawn up by the hospital, then returning to their homes or communities for continuous follow-up and guidance. 8 The core concept of continuing care is the self-management of patients in the long-term rehabilitation process. By utilizing a series of health education and promotion methods, including discharge planning, home care, and case management, it can enhance patients’ health knowledge and consequently improve their ability, confidence, and enthusiasm in conducting self-management, lower readmission rate, and reduce medical costs, thus enhancing treatment compliance and QoL. Continuing care is believed to be a method that does not require a big investment, but still provides the immediate effects of disease control.
To date, studies have proven that Arthritis Self-Management Programs (ASMPs) can enhance disease-related knowledge and self-care skills, enable patients to self-monitor their physical conditions, improve QoL, reduce healthcare expenditure, and relieve major symptoms. 9 The first organized and implemented program is the ASMP, which was developed by Lorig and his colleagues at Stanford University Medical Centre in the early 1980s. 10 Drawing on the research experience of ASMP, many organizations attempted to carry out the program and explore the practicability effectiveness for the general arthritis population in their region. 11 However, to our knowledge, the results of various studies to date have been inconsistent. Besides, the intervention of ASMP is expensive in terms of human and material resources, making it unsuitable for arthritis patients.
The pattern of continuing care has been changing in recent years since the rapid growth of the Internet. In January 2011, WeChat was launched by Tencent as an instant voice communication software where users can chat individually or in groups by sending voice and text messages, videos, and pictures using mobile phones and computers. By December 2016, the monthly number of active WeChat users reached 889 million. The WeChat health management platform may open a new path of continuing care because of its low cost and high efficiency. Moreover, arthritis patients can have access to it anytime and anywhere.
This study aims to develop a continuing care platform for arthritis patients using WeChat based on the ASMP. We then implement an eight-week intervention to evaluate its effectiveness for self-management, self-efficiency, QoL, and medication adherence. To the best of our knowledge, a recent WeChat-based intervention for arthritis patients built on a foundation of solid theory and rigorous experimental design has not yet been carried out.
Conceptual framework
The Roy Adaptation Model and the self-efficacy theory were used to guide the study. The Roy Adaptation Model regards humans as an open system with adaptive ability. There are four parts of the process that interact with the environment: input (stimulus), control process (adaptation mechanism), effect (adaptation mode), and output (adaptation result). The mode of adaptation defined by the Roy Adaptation Model includes physiological, self-concept, role function, and interdependence patterns. 12 Self-efficacy, as a key variable promoting cognitive regulation mechanisms improving adaptation mode and adaptation results, is a belief index that evaluates whether a person can successfully complete a behavioral goal. The self-efficacy theory empowers individuals with chronic disease to live with their illness, allowing them to adapt to the disease. 13
Together with Roy's Adaptation Model and the self-efficacy theory, and based on domestic and foreign studies on arthritis, this study constructs a theory-intervention model of continuing care for individuals with arthritis based on the WeChat platform. The continuous symptom, as a long-term stimulation, significantly bothered individuals with arthritis. Therefore, it is important that they learn how to adapt. Providing continuing care through the WeChat platform can provide disease-related knowledge and guidance on symptoms and life management. Timely and convenient guidance can help improve patients’ coping mechanisms and produce better adaptive outcomes. Meanwhile, functions such as doctor-patient communication and groups for sharing patient experiences on the WeChat platform can have an impact on patients’ self-efficacy, and ultimately improve their self-awareness and QoL.
Through the WeChat public accounts and groups, continuing care based on the WeChat platform for patients with arthritis pushes information on disease knowledge, life, and symptom management. Moreover, it provides other related knowledge, such as building doctor–patient, nurse–patient, and patient–patient communication platforms. It raises patient cognition of diseases and self-efficacy and promotes self-management ability. These can eventually lead to an improved QoL and the relief of chronic symptoms.
Methods
Study design
A controlled before-and-after design was employed in this study, as illustrated in Figure 1. In addition to self-care and regular follow-ups, the WeChat platform-based continuing care was only tested on the intervention group, not the control group. The outcomes in both groups were assessed using questionnaires twice: at baseline (T0), which was before the WeChat platform was applied for the intervention group and eight weeks after T0 (T1). This evaluation consists of self-management, QoL, self-efficacy, and medication compliance. Ultimately, the lasting effects of using the WeChat platform for continuing care were expected to be evident.
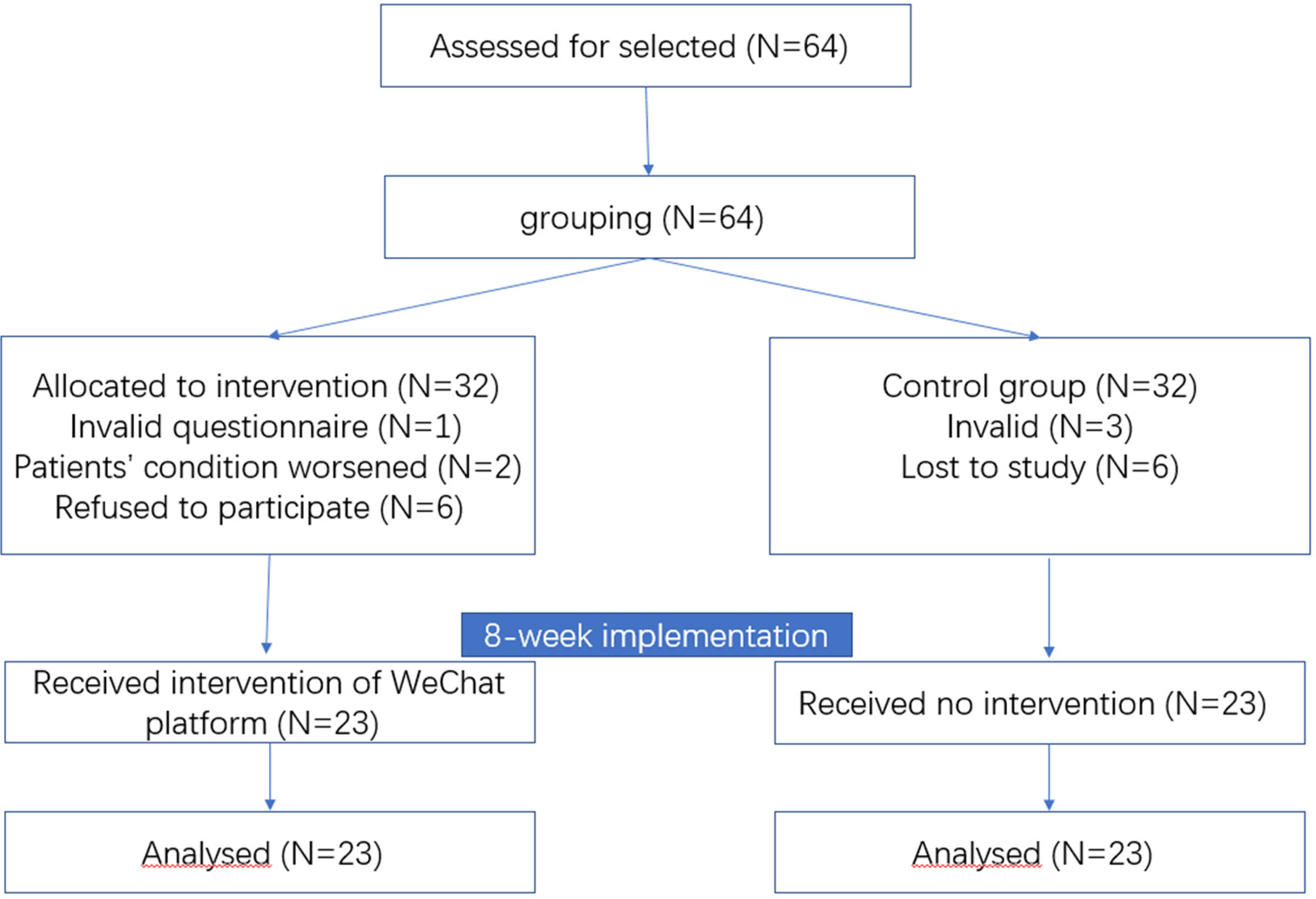
Consort flow diagram of the study.
Participants
Four criteria for patients’ eligibility for the study were established: (a) should have been diagnosed with arthritis with continuous joint pain for more than three months; (b) should be older than 18 years old, conscious, and has independent thinking capability; (c) should have a smartphone, be capable of using WeChat, and be able and willing to complete a questionnaire, and (d) must have voluntarily given informed consent and agreed to participate in eight weeks of interactive learning using the WeChat platform. Patients with severe mental disorders and attention or hearing impairments were excluded.
Data collection
We contacted doctors and nurses in the rheumatology and immunology department of two third-class A hospitals in Xiamen City. Subsequently, we approached patients who met the inclusion criteria and agreed to participate in the study in December 2017. A convenient sampling method was adopted. The sample was estimated using the two-sample mean test formula: setting the significance level at α = 0.05. We calculated the control and experimental groups with 25 people each. Considering an estimated follow-up loss rate of 20%, we determined a sample size of 64 people. Patients were divided into two groups of 32 each, according to the enrolled hospital, to avoid sample contamination, and asked all of them to fill out a baseline questionnaire. The intervention group was included in the WeChat small management and micro-clinic discussion groups. Both the intervention and control groups completed the questionnaires after eight weeks of WeChat platform intervention. Post-intervention data collection was completed in February 2018.
Ethical considerations
All participants signed a consent form before participating in the study after being informed of the purpose of the research and their cooperation. Only the researchers of this group have access to all forms of the materials and data used in this study. The data will be used for the overall analysis. The data of a certain research object will not be selected separately for publication and analysis, and the personal information of the research objects will be well protected. Participants will receive health information about the disease without potential harm. This study was approved by the university ethics committee (XDYX2019003).
Intervention
The main intervention modes of the WeChat platform-based continuing care for patients with arthritis are a WeChat public account and WeChat group management. The WeChat public account is presented in a three-level structure consisting of chronic disease classification, self-management, and management tools. The chronic diseases were classified as rheumatism, RA, AS, gout, and OA. Self-management includes the contents of management principles, life management, drug management, and symptom management. Expert consultation, planning, and other secondary directories are listed under management tools.
We expanded the secondary catalog by pushing articles, such as WeChat text and pictures, including the introduction of various diseases, relevant examinations, diet and exercise, misunderstandings, drug effects, dealing with fatigue, pain and sleep disturbance, tips for life management, common knowledge about drugs, and planning.
Various approaches have been applied to the management of WeChat groups. A small-group management system ensures the effectiveness of interventions. The WeChat intervention group was established for every 10–12 patients. The intervention was carried out in batches, but the maximum interval for each batch should not exceed 15 days. The administrator, guided by the WeChat platform theory-intervention model for chronic disease continuous nursing, regularly forwarded the contents of the public account to the WeChat group for patients to learn. Patients punched in when they read and spoke in the group. The administrator recorded the speech, while other staff members simultaneously monitored the page views of the pushed content regularly, and gave reminders to patients who repeatedly failed to read the educational content on time for more than three consecutive occurrences.
A large group communication platform was established to provide a broad doctor–patient, nurse–patient, and patient–patient communication platform, which include administrators, professional doctors, nurses, and target patients. The question-feedback solution mechanism was well implemented in this platform. The manager regularly inquired about the problems existing in the customization of patients and other issues encountered during the intervention process, which professional clinical doctors responded to at 20:00–21:00 every Monday, Wednesday, and Friday. We offered a one-to-one private guide for those who were unwilling to openly discuss their own problems in the WeChat group. We also gave verbal encouragement and praise for members who read articles on time and performed actively in the WeChat group.
Our team considered the medical knowledge and account management experience of the WeChat production and management team members. To ensure visual convenience for elderly people, the font should not be less than size 18, picture color should not be distracting, and the materials should be simple and easy to understand. The materials on the WeChat platform are based on Dr Lorig's research in the field of online intervention for arthritis and authoritative books in this field. They are also supplemented by rheumatoid-related medical books and online resources that ensure the intervention content is as effective as possible. All articles were reviewed by group members and experts before being published online.
Measures
We used a self-administered general questionnaire to assess patients’ baseline characteristics, including age, gender, education, family income, and so on. We used the SF-12 to assess QoL before and after the intervention. SF-12 scale is a simplified version of the SF-36. It is a simple questionnaire developed by the Boston Institute of Health Education of the USA to reduce the burden and time of respondents. 14 Many studies have proven that it has little difference with SF-36 in reliability and has been widely used in many countries to investigate the QoL of the general population or people suffering from special diseases. 15 The scale consists of 12 items and eight dimensions: general health (GH), physical function (PF), role physical (RP), bodily pain (BP), vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH). The GH, PF, RP, and BP were calculated to obtain the physical component summary (PCS), while SF, RE, MH, and VT were calculated to obtain the mental component summary (MCS). The scale uses a hundred-mark system to score points. The higher the total score, the higher the QoL. The Cronbach's α value of the total scale was 0.862, the split reliability was 0.841, and the subscale coefficients were all above 0.7, which indicates that the reliability of the questionnaire is good. The content validity of the scale between PCS items was above 0.6, that of MCS items was above 0.7, while it was 0.19 between PCS and MCS; confirmatory factor analysis was used to extract eight factors with a cumulative contribution of more than 90% for rotation. The extracted common factors were consistent with the eight dimensions of the scale, indicating good validity.
The Chinese version of the Arthritis Self-efficacy Scale-8 (ASES-8) was used for the assessment of patients’ self-efficacy. It was translated by Gao Lei and developed on the basis of the ASES compiled by Lorig. 16 It includes two items from the ASES pain dimension, four items from the ASES other symptom dimensions, and two newly added items used for the evaluation of treatment in patients with pain and fatigue symptoms. Each item uses the 1–10 scoring method; the higher the score, the higher the level of self-efficacy. The Cronbach's α coefficient for the original scale was 0.89. The Cronbach's α coefficient of the Chinese version was 0.920, and the retest reliability was 0.986, which is good. After a principal component analysis, one common factor was extracted. The factor load of each item was above 0.652, the cumulative variance contribution rate was 66.24%, and the structural validity was good.
We used the Chronic Disease Self-Management Behaviour Scale (CDSMS) to assess patients’ self-management levels. The CDSMS was developed by the Center for Chronic Disease Education and Research at Stanford University and mainly includes three subscales (15 items in total): exercise, cognitive symptom management, and communication with doctors. This scale has been widely used in studies on the self-management of patients with chronic diseases. 17 The Cronbach's α coefficient of the scale is 0.72–0.75, indicating good reliability. The exploratory factor analysis extracted three common factors, which had high factor load and cumulative variance contribution rates of 70.62%, 75.35%, and 79.74%, respectively, indicating good structural validity.
Medication adherence was assessed using the MMAS-8. The MMAS-8 was compiled by Morisky in 2008 includes a total of eight questions to examine the medication compliance of patients with chronic diseases. 18 An answer of “yes” would be given 0 points, while “no” would be given 1 point, while five items are in the opposite direction. A total score of 8 indicates good compliance, 6–8 indicates medium compliance and less than 6 indicates poor compliance. The reliability analysis of the Chinese version of the MMAS-8 showed that Cronbach's α coefficient of internal consistency was 0.65, and the intragroup correlation coefficient was 0.8.
Data analysis
The data were analyzed using SPSS version 22, which included both statistical description and analysis. The data encompassed quantitative and qualitative data. The former included scores for QoL, self-management, self-efficacy, and medication compliance, and the latter included demographic information such as gender, education level, work status, family monthly income, marriage, and family residence. We also calculated the differences in QoL, self-efficacy, self-management, and medication adherence before and after intervention, which were also quantitative data in both groups. For quantitative data, the statistical description was presented as mean (standard deviation), while qualitative data were presented as N (percentage). Statistical analysis of quantitative data was carried out using t-tests (including two independent sample t-tests and paired samples t-test), while Chi-square tests were used for qualitative data.
Results
In the experimental group, one person failed to fill in the baseline questionnaire, two exited due to worsening physical condition, six quit the process, and 23 participants finally completed the intervention. In the control group, three participants failed to complete the questionnaire, and six did not report back for a follow-up during the control period. There were a total of 23 participants in the control group who completed the intervention (Figure 1).
The demographic data of the 46 subjects showed that the age of the subjects ranged from 23 to 68 (42.52 ± 11.53) years old. Among them, 91.3% were married, and 89.1% were employed. The overall education level and income were moderately high, 17 were in junior college or above, 20 were in senior high school, and 9 were in junior high school or below. Monthly household income was above average, with four cases earning less than 3000 RMB, 16 cases earning 3000–6000 RMB, 14 cases earning 6000–10,000 RMB, 8 cases earning 10,000–20,000 RMB, and four cases earning 20,000 RMB or more. Nine cases (19.6%) lived in rural areas, 16 (34.8%) lived in towns, and 21 (45.7%) lived in urban areas. Among them, 38 (82.6%) paid medical expenses by medical insurance or public expenses. The primary caregivers of 29 patients (63.0%) were the patients themselves, and those of 16 patients (34.8%) were spouses or children. Only a small number of people had morning stiffness lasting longer than 30 min, and 84.8% did not have morning stiffness or only experienced it for less than 30 min. There was no statistically significant difference in the demographic data analysis of the patients (p > 0.05), indicating high comparability (Table 1).
Baseline characteristics of the intervention group and control group.

Table 1 also presents the initial scores for psychological and physiological QoL, self-management behavior, self-efficacy, and medication compliance, which were not significantly different between the intervention and control groups (p > 0.05). This indicates that the two groups were comparable at the outset.
Following eight weeks of intervention, significant differences were observed between the groups in terms of total psychological QoL scores, cognitive symptom management scores, and self-efficacy scores (p < 0.05). The mean difference in changes in psychological QoL scores between the two groups was 12.29 (95% CI: 4.51, 20.07; p < 0.001), while for cognitive symptom management and self-efficacy, the mean differences were 0.65 (95% CI: 0.24, 1.05; p < 0.001) and 0.69 (95% CI: 0.14, 1.24; p < 0.05), respectively. The intervention group showed increase scores in self-management (exercise) and self-management (communication with doctors) scores, while the control group showed a decreasing trend without intervention. The intervention group showed statistically significant improvements in these measures (p < 0.05), but the improvements were not statistically significant when compared to the control group (p > 0.05). More detailed information can be found in Table 2.
Between-group and within-group differenced of outcomes (n = 46).

95% CI: 95% confidence interval.
*p < 0.05; **p < 0.01.
Discussion
Quality of life measurement is a practical method that provides healthcare professionals with a better understanding of the effectiveness of the management plan for arthritis patients. 19 Continuing WeChat nursing interventions are effective in promoting the QoL of such patients. This study focused on developing a continuous care model for arthritis patients based on WeChat platform and investigated its impact on enhancing their QoL, self-efficacy, and self-management abilities. The results showed a significant improvement in patients’ psychological well-being, cognitive symptom management, and self-efficacy following an eight-week intervention period.
It is well known that patients with arthritis have poor QoL and are prone to fatigue.20,21 Our research findings demonstrate that the continuity of care provided through the WeChat platform can enhance the psychological and physiological QoL for arthritis patients. While the latter did not attain statistical significance, this may be attributed to the small sample size used in our study. Nevertheless, our research suggests that the WeChat platform has enormous potential in improving the overall QoL for arthritis patients, similar to the positive outcomes achieved by Trudeau et al.'s four-week web-based intervention and follow-up survey on RA or OA patients. 22 This study's results were also in line with those of Chitkar et al., who found that a two-month instruction period using a mobile app-based program improved specific aspects of PF and quality of life in knee OA patients, including fatigue/energy, PF, and pain. 23 Through careful nursing intervention, arthritis patients can benefit from improved diet, medication management, and joint exercise, which can effectively alleviate joint pain and promote their physical and mental well-being. 24 The WeChat platform for chronic disease continuity provides a myriad of benefits, including the dissemination of disease knowledge and symptom management skills via public account push notifications, as well as facilitating communication between patients and healthcare providers, nurses, and fellow patients through WeChat groups. This enhances arthritis patients’ understanding of the disease and its treatment, allowing them to make more informed decisions about medication, exercise, and diet. Ultimately, this results in better cooperation with doctors’ treatment plans, improved treatment effectiveness, reduced arthritis reactions, relief from joint pain, enhanced PF, and better MH outcomes.
Studies showed that patients with arthritis expect more knowledge and home-care skills. 25 Patients also seek to improve their understanding of arthritis through formal health education. 26 In addition to sending management skills and knowledge through a public account, the WeChat platform provides a medical communication platform for patients, doctors, and nurses. Studies have shown that utilizing the WeChat platform for health education has led to increased self-management levels among hemodialysis patients. 27 This internet-based remote health education program offers unique advantages. In this study, it was found that the cognitive symptom management of arthritis patients in the intervention group improved following the WeChat platform intervention. Patients’ self-management ability in facing pressure, managing symptoms, setting goals, and learning to relax among other aspects could be enhanced. 28 One participant in this study reported feeling pain after taking a bath in a hot spring joint, suspecting the hot spring aggravated the joint pain. The doctors gave the right analysis: the join was not protected from the warm waters. Through the WeChat group, patients can not only ask questions about their own problems and receive advice from a professional but they can do so in a collective environment as well. They are willing to share their experiences and even remind each other to implement management plan properly, which greatly improves their symptom management ability. However, there was no significant difference in the level of exercise between the intervention and control group after the intervention with WeChat, which may be related to the living conditions of patients and the restriction of the duration of intervention. Most patients were on the job, and it was difficult to significantly change their living habits and time planning in a short period of time.
This study revealed that the WeChat platform management application offers an opportunity to effectively improve the self-efficacy of patients with arthritis. When patients recognize their own health problems and have the skills to deal with them, their self-efficacy can be enhanced, and they are more likely to make behavioral changes and improve their QoL. A study found that self-efficacy is an important factor affecting joint dysfunction. 29 A higher level of self-efficacy is conducive to promoting self-management, thereby reducing disease symptoms and joint dysfunction. Interventions should gather feedback from arthritis patients and be tailored to provide adherence support when necessary. 30 Intervention through WeChat can ensure the accessibility and feasibility of support for patients. 31
Implications
Combined with the Roy Adaptation Model and self-efficacy theory, this study takes self-efficacy as a key variable to produce adaptive ways and results through a cognitive adjustment mechanism. Disease and symptom management were conducted through a WeChat public account and WeChat group communication, which provided a platform for communication between doctors, nurses, and patients. Self-efficacy in patients with arthritis must be promoted to develop their self-management ability, alleviate chronic symptoms, and ultimately improve their QoL.
The WeChat platform, as a means of providing continuous care, is an invaluable resource for enhancing the psychological well-being of patients and bolstering their cognitive capacity to manage symptoms associated with arthritis. Simultaneously, it has the potential to elevate patients’ sense of self-efficacy. These endeavors hold promise in augmenting patient quality of life, alleviating the burdensome responsibilities and complexities faced by medical personnel. If the WeChat platform intervention mode of continuous care for chronic diseases is effective and widely used, it can promote the cognitive level of family members about the disease and its related symptoms. It would enable patients and their families to properly manage the disease and its medical treatment. In addition, it can also reduce the number of treatments, lower medical costs, and improve the medical treatment effect. For hospitals, the reduction in medical treatments can lighten the workload and ease the difficulty of medical staff, as well as rationalize the allocation of medical resources. The improvement in these functions is also very important for cancer care. By strengthening self-management strategies and self-efficacy, patients are empowered to better attend to their health, and concurrently, an improvement in their psychological well-being engenders confidence in confronting the adversities posed by the disease, fostering greater cooperation with medical professionals.
Limitations
The intervention was only conducted for eight weeks; whether an extension can achieve a better effect needs to be further verified. After the intervention, the patients needed to be supplemented. During the study, there were nine cases of sample loss in each group. The reasons for the high loss rate may be related to the long questionnaire; some patients lacked patience due to illness, resulting in the questionnaire not being carefully filled in. In addition, the loss of patients in the control group may be related to being aware of not accepting WeChat intervention. We suggest that future studies extend the intervention time and maintain the tracking time to obtain a more obvious effect. The sample size could be expanded based on this study to improve the credibility of the WeChat platform on patients with arthritis and draw more reliable conclusions.
The sample size was also too small, which may affect the statistical power. However, this trial could be a reference for future RCTs with a large number of participants. Also, other drugs or comorbidities may have affected the results, especially in terms of physical symptoms. The lack of randomisation also limits the scientific validity of our conclusions, and we will carry out high-quality randomised controlled trials in the future.
Conclusion
The WeChat platform-based continuing care is a useful tool for improving patients’ psychological state and their cognitive symptom management ability with arthritis. At the same time, it can improve the self-efficacy level of patients. This can contribute to improving patient QoL and reducing the workload and difficulty of medical staff.
Footnotes
Acknowledgements
The authors would like to thank Wang Qingqing, Xu Xiaoguang, Zhou Lihua, Bao Shuying, Xue Yuan, all nurses from the Department of Rheumatology and Immunology, Zhongshan Hospital Affiliated to Xiamen University; and all nurses from the Department of Rheumatology and Immunology, the First Affiliated Hospital of Xiamen University for their support and assistance during recruitment and data collection period. The authors would also like to thank all participants for their participation in this study.
Contributorship
CJ and XQ researched literature and conceived the study. SQ, XQ, PJ, LS, and YG were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. CJ, HY, JY, and PJ wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the university ethics committee (XDYX2019003).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been supported by Humanities and Social Sciences Research Planning Fund of the Ministry of Education (21YJAZH071), with the recipient of the funds being Shen Qu.
Guarantor
SQ.
Patient consent statement
All the patients who met the inclusion criteria and agreed to participate in the study.