
Abstract
Objective
The World Health Organization (WHO) Southeast Asian region, comprising a quarter of the global population, faces significant healthcare challenges influenced by diverse economic and social conditions. The objective of this study is to map the Digital Health Intervention (DHI) functionalities across the nine axes of the healthcare system challenges (HSCs) model; we use WHO's DHIs classification framework and the Health System Challenges model. Our study findings help identify the gaps in the potential of the existing DHIs in addressing health system challenges in low- and middle-income countries.
Methods
Using SCOPUS, EMBASE and PUBMED databases, a scoping review was conducted to identify the existing DHIs in the Southeast Asia region and map the DHIs with the HSCs related to availability, information, utilization, quality, accountability, efficiency, equity, cost and acceptability.
Results
Out of 278 studies, 337 DHI functionalities were identified. A majority of the identified DHIs address challenges related to information (35.6%), availability (34.7%) and utilization, while less than 10% of the DHIs address challenges related to quality (8.9%), accountability (5%) and efficiency (3.9%) in the health system.
Conclusion
Most of the existing DHIs in SEA region address challenges related to availability of services and lack of information, while they fall short in addressing challenges related to quality of services, efficiency, and accountability. Acknowledging the inter-linkages across the health system challenges, this gap identification may well guide future investments and planning in DHIs.
Keywords
Introduction
The Southeast Asian region of the World Health Organization (WHO) constitutes one-quarter of the global population. 1 The disease burden in this region is greater than that of other WHO regions. According to 2019 data, people born in the Southeast Asian region of WHO have the second-highest probability (21.62%) of dying between the ages of 30 and 70 due to cardiovascular diseases, cancer, diabetes or chronic respiratory diseases. Other WHO regions have lower probabilities, such as Europe (16.32%), Western Pacific (15.58%), United States (14.04%) and Africa (20.79%). 2 Furthermore, countries in the region are facing a dual set of challenges: those that have long existed and are predictable, and those that emerge with unexpected and significant impact, as exemplified by the unprecedented effects of the COVID-19 pandemic.3–7 This predictability is underscored by the prevalence of non-communicable diseases such as cancer, diabetes, asthma, hypertension, cardiovascular ailments and other fatal conditions. Such health concerns necessitate ongoing monitoring and medical interventions, both routine and critical situations, because of the recurrent nature of certain challenges within the healthcare landscape.3–7
Coupled with resource-constrained health systems, such high burdens of disease pose a challenge in delivering effective healthcare.8,9 Information and Communications Technology (ICT) in healthcare has the potential to address health system challenges, access barriers and shortage of healthcare workers, especially in low- and middle-income countries. 10 With rapidly advancing technology and the recent pandemic experience, digital health programmes became strategic public health responses to emergency situations, and healthcare delivery via ICT is increasingly becoming the norm.
In 2023, five out of 11 member countries in the region had already prioritized investments in digital health.11–15 However, there is a lack of guidance on prioritizing digital health investments based on the type of digital interventions and the health system challenges that they address according to local contexts.
It is essential to examine the digital health interventions (DHIs) that specifically address challenges in strengthening health systems in the region given the dual burden of diseases coupled with resource-constrained health system in the Southeast Asia region 16 and the Universal Health Coverage vision through strengthening PHC from 2022 to 2030. This examination could guide SEA member countries in targeted investments in DHIs and enhance the potential of DHIs in strengthening health systems. Therefore, this study maps the existing DHIs in the SEA member countries to the health system challenges, using DHI categorization framework given by WHO in the year 2023 and the healthcare system challenges (HSC) framework. 17 The latter is explained in the next section.
Digital health intervention, digital health functionality and health system challenges
In 2023, the WHO 17 released comprehensive guidelines that categorize various DHIs according to their functionalities in an easy-to-understand fashion for the benefit of stakeholders regardless of their technical backgrounds. Further, the guidelines proposed a HSC framework which is useful to map the DHIs with the HSCs, which in turn facilitates understanding the potential of DHIs to address HSCs. In this study, we utilize the HSC framework and DHI classification framework 17 to gauge the potential of existing DHIs in addressing the HSCs. The HSC framework guides stakeholders by outlining the needs and issues that hinder optimal performance in health systems. 17 In this framework, the health system challenges are classified across nine axes: information, availability, quality, acceptability, utilization, efficiency, cost, accountability and equity (see Figure 1). Health system challenges related to information involve lack of access to data, delayed reporting of events, the lack of unique identifiers, and reliable data. Health system challenges related to availability include insufficient supply of commodities, services, equipment and skilled health workers. Health system challenges relating to quality include insufficient health worker competence, low-quality commodities, poor adherence to guidelines, standards and protocols, inadequate identification and management of risks. Similarly, health system challenges classified under acceptability include health interventions not being tailored to the local norms of the community and when individual beliefs are not addressed. 17 Utilization challenges are primarily concerned with inability to access healthcare due to geographical barriers, low demand for services and loss to follow up. Efficiency challenges could occur due to lack of guidelines, priority setting, inadequate workflow management, manual processes and inappropriate referrals. 17 Cost challenges deal with out-of-pocket expenditures and the lack of financial protection, coordinated payer mechanisms. Equity challenges are concerned with inadequate representation of the community members, illiteracy, disabilities or any other unfair or avoidable differences among people on various dimensions of inequality such as sex, gender and sexual orientation. 17

Conceptual Framework adapted from the WHO 17 report.
According to the WHO framework (2023), ‘a DHI represents a discrete capability of digital technology to address health sector objectives’. The DHIs are categorized into four overarching categories based on the primary target user, namely, provider, client or person, health system manager and data services. Each DHI has unique functionalities that have the potential to address health system challenges. Utilizing the HSC framework and DHI classification framework given by WHO (2023), we map the HSCs with the DHI and the corresponding DHI functionalities.
As shown in Figure 1, the HSC framework includes nine axes. We map the identified DHIs across the nine axes of the HSCs. Figure 2 provides an example of the mapping exercise. The identified HSC axis is ‘Quality’, specifically quality of care. So, the DHI that could potentially address quality of care is the ‘Decision Support System’ for healthcare providers. The functionality identified provides prompts and alerts to healthcare providers based on the protocol and suggests a detailed checklist to the healthcare provider based on the protocol. The DHI functionality specifically addresses the challenge of poor adherence to clinical guidelines and thus, poor quality of care.

Linkages across health system challenge of quality and digital health functionalities https://www.who.int/publications/i/item/9789240081949) This is in reference to the figure on page 3 of the WHO document.
The WHO classification of DHIs as a framework is valuable for understanding how technology can applied practically to health system challenges. So, following from this, utilizing the strategy outlined in the WHO classification guide builds connections between DHIs and the health system challenges they address, respectively, as illustrated in Figure 2. For each of the HSCs (across the nine axes outlined in Figure 1), we identified a DHI that addresses the given HSC. Considering the extensive range of digital health initiatives, from telemedicine to various others, and acknowledging the immense challenges in the healthcare system, it is important to identify and map the precise health system challenges addressed by each DHI. This will facilitate targeted investments in specific DHIs based on the regional context.
Given this, we mapped the existing DHIs into nine broad categories (the nine axes of health system challenges) and then, within each broad category the sub-category of the DHI functionality was identified. This mapping exercise helps us to gauge the potential of existing DHIs in addressing the health system challenges and also identify the gaps for designing future DHIs in SEA region.
Methodology
A scoping review was conducted using the Arksey & O’Malley framework (Arksey and O’Malley, 2005). Arksey & O’Malley framework includes five stages: (1) defining the research question or research objective, which is typically broad in scope; (2) identifying relevant studies using a systematic method, preferably following PRISMA guidelines (3) selecting studies, with the establishment of inclusion/exclusion criteria; (4) charting the data and identifying key themes, and (5) compiling, summarizing and reporting the results. Our research objective was to scope the potential of existing DHIs in the SEA region in addressing health system challenges. The research objective guided our search strategy. We systematically searched peer-reviewed literature in PubMed, Scopus and EMBASE(Ovid) electronic databases. A search was performed using keywords, Medical Subject Headings and database-specific subject headings. Our search terms were derived from three core concepts and their related terms:
Digital health (e.g., m-health, mobile applications, telemedicine, telerehabilitation) Non-communicable and infectious disease categories (e.g., cardiovascular disease, COPD, tuberculosis, HIV, malaria). The selection of the disease categories was guided by the WHO-SEA regional disease priorities. SEA regional countries (e.g., Southeast Asia, India, Bangladesh, Nepal, Myanmar, DPR Korea, Bhutan, Indonesia, Timor-Leste, Thailand, Sri Lanka).
A senior information specialist validated the search strategy. The search included studies published since 2010, and the final search was performed in February 2022.
Eligibility criteria
The inclusion criteria for full-text review were peer-reviewed articles published in English that described the use of a DHI for managing diseases in SEA member countries. We included publications examining any aspect of digital health intended for the general population, patients and caregivers, healthcare providers, health system managers and data services.
We excluded publications in any language other than English, those for which the full text was not available, pilot interventions, conference proceedings and DHIs outside SEA member countries.
Data extraction
Articles identified by our search strategy were imported into Rayyan, the online systematic review software and duplicates were removed. Two researchers independently assessed the titles and abstracts of search results against the inclusion criteria. Any uncertainties or differences in opinion were discussed, and if unresolved by discussion the full article was taken forward to full-text review. Subsequently, both researchers independently conducted a full-text screening of the articles excluding publications that did not meet the eligibility criteria or where full text was unavailable. Standardized template for data extraction to tabulate specific information from the included studies, such as journal title, article title, publication type and date, country of focus, disease or condition in focus, target population, description of DHI and its purpose, was developed.
Summarizing results: Using the WHO DHI classification (‘Classification of Digital Health Interventions v 1.0,’ n.d.), the identified DHIs were appropriately characterized. Based on the target user and the functionality of the DHI, the DHIs were mapped with the HSC. For example, if a DHI is ‘Decision Support System’ for a ‘healthcare provider’ (target user) with the functionality of prompts and alerts based on medical/clinical protocols. This DHI has the potential to improve quality of care, specifically due to lack of skilled manpower.
Results
Study selection
The initial search yielded 3439 articles. After eliminating duplicates and reviewing title and abstract, 512 articles were considered for full-text review. Upon full-text review, 232 articles were excluded, and 278 papers were eligible for inclusion. This process is shown in Figure 3. Within the 278 included articles, 337 DHIs were identified and each of the DHIs was analysed in terms of its target user, functionality and the health system challenge being addressed.

PRISMA flow diagram for the scoping review. *DHIs outside SEA region, study protocols, pilot interventions, perspectives, editorials, conference proceedings were excluded.**. DHI: Digital Health Intervention.
Geographic distribution of DHIs
As shown in Figure 4, 66.9% (n = 186) of the identified study records were reported from India; 10.1% of the identified study records were identified by Thailand (n = 28). Indonesia and Bangladesh each constituted 8.6% (n = 24) of the total study records; 2.5% of the studies were reported from Nepal (n = 7). Myanmar and Sri Lanka each constituted 1.1% (n = 3) of the studies. In addition, there were three mixed-country study records that had at least one of the countries from the SEA region of the WHO.
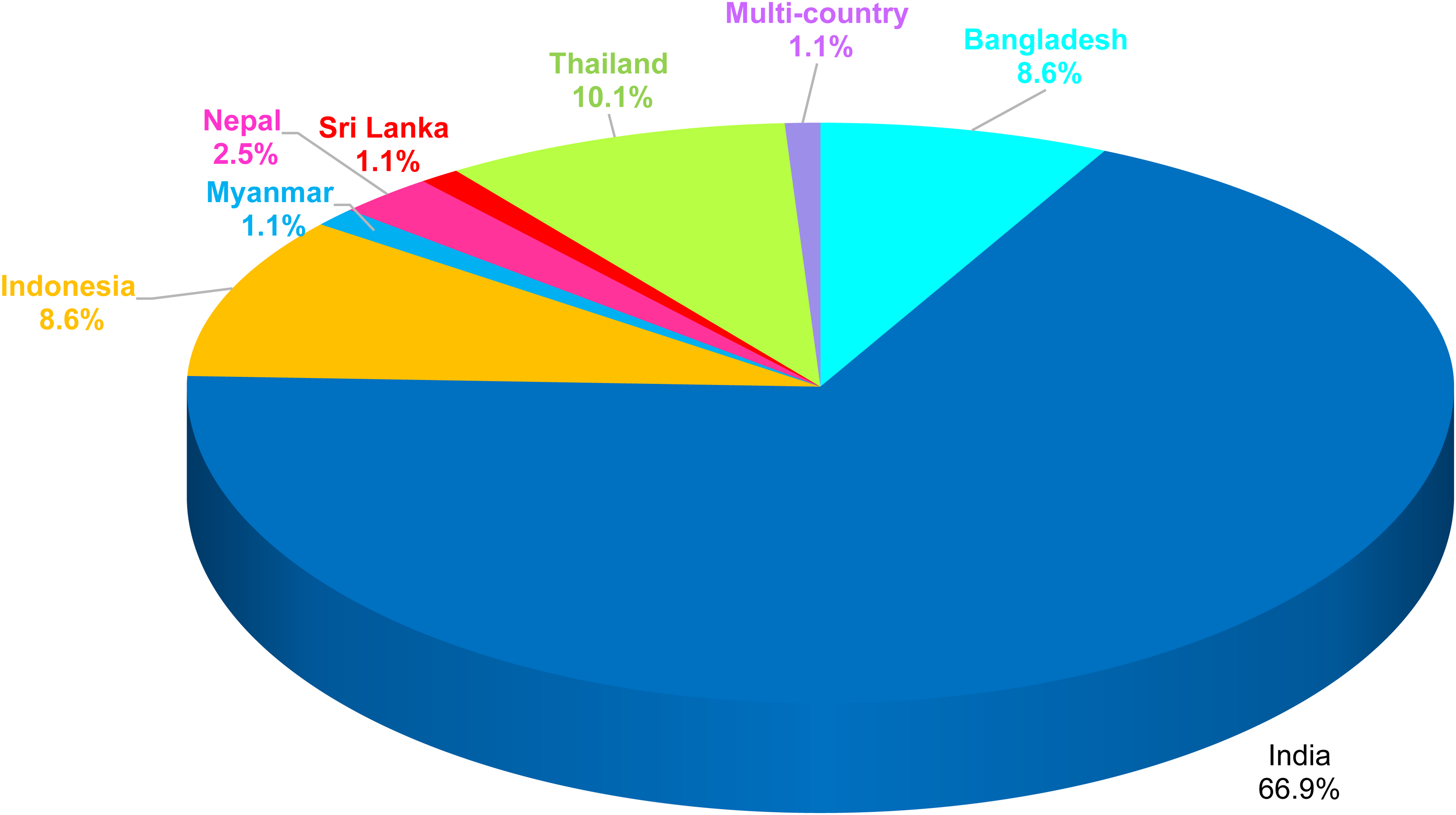
Geographic distribution of included studies (n = 278).
Figure 5 displays the distribution of DHIs across the Health system Challenges axes from 2010 to 2021. It is evident that the focus of DHIs in terms of addressing the health system challenge has been on information-, utilization-, and availability-related challenges. During the COVID-19 pandemic, there was a significant surge in the overall number of DHIs and a visible surge in DHIs addressing availability challenges, such as geographical inaccessibility. The DHIs addressing quality concerns, such as non-adherence to protocols and incompetent healthcare providers, started appearing in the SEA region only in 2015 and remained low in the overall proportion of DHIs. There was also a surge in identified interventions related to health system challenges of efficiency, quality and accountability during the first wave of the pandemic. During the same time, a DHI addressing cost-related challenges was also present.

Trend analysis of DHIs addressing health system challenges from 2010 to 2021. DHI: Digital Health Intervention.
Digital Health Interventions and health system challenges
As seen in Figure 6, out of the n = 278 study records, about 337 DHI functionalities were identified that addressed one or more challenges of the health system; 35.6% (n = 120) of the DHIs functionalities addressed the health system challenge of information; 34.7% (n = 117) of the DHIs functionalities addressed the health system challenge of availability; 8.9% (n = 30) of the DHIs functionalities addressed the health system challenge of quality. Utilization challenges were addressed by 7.1% (n = 24) of the DHIs. While 6.2% (n = 21) of the DHIs addressed the challenges of both Information and Utilization; 3.9% (n = 13) of the DHIs addressed the challenge of efficiency. The health system challenge of cost was addressed by only one DHI. We could not identify any DHIs that addressed the health system challenges of acceptability and equity.

Distribution of health system challenges that were addressed by (n = 337) DHIs. DHI: Digital Health Intervention.
Functionality of DHIs – current focus
The treemap (see Figure 7) displays the distribution of the identified DHIs across the nine axes of HSC framework, and further, within each axis the digital health functionality is identified. As highlighted above, about 36% DHIs had the potential to address HSC of ‘information’. Within these, majority of the functionalities were pertaining to the category of targeted client information which represents 17% of the total DHIs as opposed to the category of untargeted client information – a mere 1% of the total DHI functionalities. The other major functionalities that were associated with information include data collection and management (n = 21) and the category of On-demand information services to clients (n = 14). Many of the functionalities in the following interventions were under-used, such as Client-to-client communication, Personal Health tracking, Citizen-based reporting, Client ID and registration, Client health records and HCP communication.

Distribution of DHI functionalities across health system challenge axes (n = 337). DHI: Digital Health Intervention.
Among the DHIs addressing HSC of ‘availability’, a majority of the identified functionalities were associated with ‘Telemedicine’ that accounted for a significant 23% of the total DHIs identified in our review, followed by ‘Lab and Diagnostic imaging management’ that accounted for about 10% of the total DHIs.
The next major health system challenge that was identified to be addressed by a good number of DHI functionalities was utilization (13%). Within these, the major focus was on ‘Targeted Client information’ which was about 12% and the remaining under-used functionalities identified with the potential to address utilization were related to DHIs namely, ‘Prescription/Med management’ (n = 2) and ‘telemedicine’ (n = 2).
Health system challenges of quality, accountability and efficiency were addressed by very few digital health functionalities. About 8% of the DHI functionalities, categorized as, namely, ‘HCP decision support’ and ‘health worker training’ addressed quality challenges.
Digital Health Interventions related to efficiency and accountability were less than 5%. The DHIs addressing efficiency included functionalities such as referral coordination, scheduling for healthcare providers and human resource management. We could not identify any DHIs that addressed the health system challenges of acceptability and equity. Overall, the existing DHIs in the Southeast Asia overwhelmingly addressed the health system challenges related to information, followed by availability, and utilization.
Discussion
This review may well be the first one to assess the potential of DHIs to address the health system challenges based on the WHO framework in the Southeast Asia region.17,18 The number of studies has increased over the years, a finding consistent with other reviews on DHIs.19,20
This review identified 337 DHIs and the identified DHIs were then mapped across the nine axes of the health system challenges framework. A majority of the identified DHIs address challenges related to information (35.6%), availability (34.7%) and utilization, while less than 10% of the DHIs address challenges related to quality (8.9%), accountability (5%) and efficiency (3.9%) in the health system. Digital Health Interventions addressing challenges related to cost, equity and acceptability were lacking.
This review study found that majority of the interventions that were implemented addressed the health system challenge of ‘Availability’ via Telemedicine that caters to the ‘insufficient supply of commodities, services, equipment, and health care workers in addition to the health system challenge of ‘Information’ that pertains to the lack of access to information and inadequate utilization of data, communication roadblocks and delayed reporting of events’. As seen in another review, 21 telemedicine was more often implemented as the intervention followed by targeted client communication. Interventions in targeted client communication addressed multiple health system challenges of utilization, information and availability as identified in our review. However, there is not much evidence of the effectiveness of these interventions although there may be some improvements in some health outcomes with low certainty. 22
On the other hand, there were no interventions identified in our review that addressed the health system challenge of acceptability. These include interventions that are designed to tackle challenges arising from a ‘lack of alignment with local norms and culture and adapted to cater to individual beliefs and traditional practices prevalent in the community’. 18 Studies measuring whether an intervention was perceived as acceptable by the users are lacking – a clear evidence gap. 23 Admittedly, limited data exists regarding the extent to which the population actively engages with DHIs since the distinction between genuine utilization and mere persuasion remains unclear.24,25 So, more research is needed to explore the barriers that hamper vulnerable communities from using DHIs. Governments need to ensure that the challenges in the health system are addressed such that it is inclusive and meets the needs of every population group. 26 In addition to the health system challenge of acceptability, there were no interventions identified that addressed the health system challenge of equity in our review. This contrasts starkly with the research findings in other WHO regions of the globe. 27 Notably, a report from the WHO regional office of Europe reported that half the countries in the Region have implemented a digital inclusion strategy. 27 Populations in this part of the world (Southeast Asia region of the WHO) are diverse. Following this, indigenous communities are often neglected, and the healthcare challenges they face are unique compared to non-tribal and global health issues. 28 These challenges include financial barriers, long distances to healthcare centres and discrimination by healthcare providers.29–31 These are objective factors that are not very difficult to empirically measure.
Our review identified that 35% of the DHIs have the potential to address health system challenges of availability and information each, the adoption of these interventions is questionable because mere availability of a DHI does not necessarily translate to its adoption.32,33 A number of factors have been associated with a lower intention to use DHI, including demographics,34,35 lack of digital literacy skills,32,33 privacy concerns, perceived value 21 and app design and content. 21 These factors need attention of stakeholders responsible for creating, managing and implementing DHIs for effective healthcare delivery.
Although DHIs have been acknowledged for their effectiveness in alleviating financial burdens, 36 our review did not reveal sufficient interventions specifically examining the aspect of cost savings. Only one DHI addressed the health system challenge of cost by using a cohort-based budget impact model to calculate the incremental cost of generic medicines for diabetes by means of mobile health application. 37 The lack of interventions in this area is a grave concern considering that this challenge is linked to the other health system challenges involving logistics and operations in the health system.
It is also important to note that our study included only those studies that were reported from the Southeast Asia region. We did not include studies that had Southeast Asian populations residing in other regions of WHO. Also, we have not assessed the effectiveness of these interventions to address the health system challenges. That is something that needs to be investigated ahead as confirmed in research findings from other WHO global regions.27,38 In addition, technological advancements are always subject to change in a rapidly advancing field. 39 It will be important to also take into consideration these aspects in future reviews on how effectively a particular DHI can address health system challenges. Based on our research findings, we believe there needs to be more research on factors that have an impact on adoption of DHIs for different population groups. In addition, research on digital health needs to insist on an equity lens while designing the interventions. There also need to be experimental studies to know the effectiveness of different DHIs for addressing various health system challenges in different contexts such as wars, pandemics and disasters in addition to everyday health system challenges.
Limitations: We acknowledge certain limitations of this review study. The first and foremost is that it is a scoping review and thus quality checks of the included studies were not done. Secondly, this review included only published literature in English. Therefore, there is a possibility that digital health applications from several countries such as Myanmar, DPR Korea and Maldives exist but were not identified in our review. Furthermore, it is understood and known that many industrial digital health applications do exist in the SEA region that fail to document their progress in the scholarly literature, and thus, we accept the limitation of reporting (publication) bias in our results.
Conclusion
Our review highlights a growing number of studies on DHIs, predominantly from India, addressing health system challenges. However, there is a notable gap in interventions targeting acceptability, cost, efficiency and accountability. The absence of interventions targeting acceptability raises concerns about the alignment of digital health services with local norms, cultural practices and individual beliefs within communities. Similarly, the dearth of interventions addressing equity underscores the need for inclusive approaches that cater to the diverse needs of different population groups. While our study focused on the Southeast Asia region, these findings emphasize the importance of exploring and implementing strategies to enhance acceptability and promote equity in DHIs on a global scale. The effectiveness of DHIs and their inclusivity across diverse populations needs further exploration.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241311062 - Supplemental material for The potential of digital health interventions to address health system challenges in Southeast Asia: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241311062 for The potential of digital health interventions to address health system challenges in Southeast Asia: A scoping review by Vanita Singh, Rosemol Johnson K, Anil G. Jacob and Oommen John in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank the George Institute for Global Health and University of New South Wales for the resources and access to databases.
Contributorship
VS and OJ conceptualized the study objectives and research design. VS performed data acquisition, data analysis and report writing. RJK performed data analysis and report writing. AGJ reviewed the manuscript and finalized the same.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our study did not require an ethical board approval because it did not contain human or animal trials.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
VS.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.