
Abstract
Objective
The escalating global aging population underscores the need to effectively manage geriatric diseases, constituting a significant public health concern. Community-based rehabilitation has emerged as a crucial and accessible paradigm for the rehabilitation of older adults. In China, however, the practical implementation of community-based rehabilitation faces formidable challenges, including a dearth of specialized rehabilitation therapists, substantial disparities between demand and supply, and suboptimal satisfaction rates. We aimed to develop a community-based rehabilitation management platform for older adults centered around digital health technology, with the plan to conduct a cluster randomized controlled trial to gather more evidence to explore the best practices and service models of community-based rehabilitation based on digital health technology.
Methods
This cluster randomized controlled trial will be conducted in Zunyi City, China. We will recruit 286 adults aged ≥60 years and randomly allocate 20 subdistricts in a 1:1 ratio into either the intervention group, which will use the Rehabilitation Journey application, or the control group, which will be given a Rehabilitation Information Booklet for Older Adults. Both groups will undergo a 12-month rehabilitation management program, encompassing six months of guidance and an additional six months of follow-up through online and offline methods. The evaluation indicators will be assessed at enrollment and at 3 rd , 6 th , and 12 th month.
Discussion
This study endeavors to furnish novel insights to develop a tailored community-based rehabilitation management program for older adults, delivering customized, intelligent, and precise rehabilitation services.
Introduction
Aging results in not only physiological changes and the onset of diseases 1 but also a decline of psychological and social functions of older adults. 2 This phenomenon of disease and functional impairments associated with aging is also known as geriatric disease (usually characterized by chronic disease, with various physiological and psychological dysfunctions). 3 As the life expectancy of people aged 60 and above increases globally, geriatric disease has emerged as a significant public health challenge that cannot be ignored. 4 In China, chronic diseases affect a significant proportion of older adults (69.13%), along with multimorbidity (65.14%), sleep disorders (46.0%), cognitive disorders (22.0%), and depression (20.6%).5–9 These conditions shorten these adults healthy life years (HLYs), leading to dysfunction and impaired quality of life. 10
As a health strategy, rehabilitation can provide older adults with a range of services, including functional exercise, self-management strategies, and assistive device selection. 11 The goal of geriatric rehabilitation is to mitigate or alleviate the impact of geriatric disease while promoting optimal recovery or maintenance of physical, psychological, and social functions among older adults.12–14 However, due to the slow and recurrent nature of geriatric disease progression, older adults often require continuous rehabilitation. Despite this need, due to limitations such as economic constraints, transportation issues, and a shortage of medical resources, older adults are typically advised to continue with community-based rehabilitation (CBR) after passing through the acute phase of their illness. 15 CBR, as an extension of institutional rehabilitation, not only offers economical, sustainable, and effective rehabilitation services but also promotes better social integration by maintaining and improving social networks. In other words, it aims to provide older adults with equal opportunities for development, access to resources, and rights at the community level.16,17 The World Health Organization considers CBR the optimal choice for the provision of rehabilitation services to groups such as older adults and persons with disabilities.
To address the challenges presented by an aging population, the Chinese Government has prioritized CBR as a strategy within public healthcare services. The objective is to provide high-quality CBR services to older adults, thereby extending their HLYs. 18 However, CBR in China confronts several critical issues requiring attention. The first issue is the lack of specialized facilities and professionals. Despite increased government investment in facility construction and personnel training, significant disparities exist in the fund allocation for health service systems and CBR resource distribution due to the imbalanced economic development across different regions of China. 10 For example, Shanghai in the east has much higher levels of CBR services than Chengdu in the west. Such disparity has hindered the progress of CBR.19,20
Second is that CBR services should be tailored to the varying needs of older adults, with both content and formats designed accordingly. 21 As people age, they may encounter a spectrum of geriatric diseases and functional declines, accompanied by fluctuations in their psychological state, such as anxiety, depression, loneliness, and other psychological problems. Concurrently, older adults undergoing such changes also experience significant adjustments in their social roles and functions. These adjustments often result in reduced interaction with family, friends, and society, which can further impact their ability to perform daily activities, their overall quality of life, and their mental health. Rehabilitation strategies for older adults should not be limited to physical rehabilitation alone.22,23 It is important to consider their comprehensive needs, including psychological guidance, support for social participation, and living environment. This guarantees their needs on multiple dimensions, not merely a single aspect. 3 For instance, in addition to physiotherapy, speech therapy, and nutritional therapy, there should also be psychological counseling services, modifications to residential environments, and rehabilitation therapy to encourage social participation among older adults. Such interventions will help improve their functional status and bolster their social connections, ultimately enhancing their overall quality of life. Existing CBR can provide basic rehabilitation services for older adults, however, it is difficult to provide personalized CBR services according to the specific needs, individual abilities and preferences of older adults, resulting in a disconnect between the healthcare needs of older adults and healthcare utilization, 24 which greatly affects the effectiveness of CBR for older adults. Therefore, CBR services should take into account the multidimensional physical, psychological, social, and environmental factors of older adults and provide personalized and accessible rehabilitation services to meet their rehabilitation needs comprehensively.
In the last decade, digital health technologies, such as artificial intelligence and big data, have shown great potential to enhance global health, especially in low- and middle-income countries.25–27 These technologies facilitate condition monitoring, health management, and the sharing of healthcare resources. Digital health technologies transcend the limitations of time and space. By continuously and dynamically recording changes in the rehabilitation process of older adults in the community, these technologies can improve older adults' health profiles and provide solid data support for multidisciplinary teams to formulate and adjust rehabilitation programs. 28 Simultaneously, sharing health data and synchronizing medical information can facilitate effective coordination and guidance between medical institutions and communities, thereby enhancing access to high-quality medical resources for older adults. 29
Furthermore, a mobile phone support system addresses the challenges faced by older adults unable to access comprehensive and professional rehabilitation service information due to resource scarcity and functional limitations, providing a more convenient channel for continuous rehabilitation management for the older adults. We, therefore, aimed to develop a CBR management platform for older adults centered around digital health technology, with the plan to conduct a cluster randomized controlled trial to gather more evidence to explore the best practices and service models of CBR based on digital health technology.
Methods
Study design
The study will be a cluster randomized controlled trial with subdistricts (a predefined administrative unit consisting of a community health service center) as the unit of randomization. We will randomly select 20 subdistricts in Zunyi, Guizhou province. Ten subdistricts will be randomly assigned to the intervention group, receiving the Rehabilitation Journey, a digital health technology based on CBR management platform for older adults. The remaining 10 subdistricts will be randomly assigned to the control group (the Rehabilitation Information Booklet for Older Adults, an online manual offering routine information and guidance on rehabilitation). A total of 286 participants will be recruited, with an average of 13–15 participants per subdistrict. Cluster randomization is the chosen method of randomization, because CBR is based on the community as the essential subdistrict element. Therefore, individual randomization is not feasible, and participants within the same subdistricts will receive the same measures to minimize contamination and enhance acceptance.
The study will be conducted and reported following the Criteria for the Comprehensive Reporting of Trials of Non-pharmacological Treatments (CONSORT) statement. Figure 1 illustrates the study design and the flow of participants through the study.

Flow diagram for the randomized control trial.
Setting
For this study, we will select Zunyi City in Southwest China, a region with a population exceeding 6.6 million, of which more than 17.05% people are over the age of 60 years. Despite its large elderly population, this region faces the challenges of low social development (with an urbanization rate of 56.69%, below China's average of 65.20%), low income (with GDP per capita at 77.88% of the national average), and a relative shortage of health technicians (with 8.28 per 1000 population) in comparison to the rest of China. Our study in this region aims to concentrate on populations residing in low-income areas and contribute valuable insights applicable to regions grappling with similar developmental challenges.
Sample size
The sample size was determined using GPower3.1 software. Following Gong's indices to calculate mean scores on the EUROPEP, 30 the effect value was calculated to 0.552, with α = 0.01, 1-β = 0.95, resulting in N1 = N2 = 119. Considering a loss of 20% of the sample, 286 (N1 = N2 = 143) participants will be included in this study.
Randomization and blinding
A two-stage random sampling method will be employed to select five county-level administrative districts from the 14 in Zunyi City. This will be followed by selecting four communities within each county-level administrative district, resulting in a total of 20 subdistricts. The sampling process will use the SAS 9.4 software environment and will prohibit researcher substitution. Subsequently, participants will be assigned to either an intervention or a control group based on their subdistrict attribution, with randomization conducted at a 1:1 allocation ratio across the 20 subdistricts. Allocation sequences will be determined using randomly generated optimal sequences. An independent third party will compile and manage a list of allocations for each subdistrict in a password-protected file. Participants will not be informed of their group allocation during the study, and personnel responsible for data analysis will remain blind to the allocation. Third-party personnel will rigorously monitor all recruitment and participant changes, documenting and reporting any potential deviations.
Recruitment
Participants
Participants will be included in this study if they meet the following criteria: permanent residency (≥6 months) in communities within Zunyi City, Guizhou Province, China; aged 60 or older; suffering from geriatric disease requiring rehabilitation; capable of understanding and expressing language; and able to use a smartphone. Participants with severe cognitive impairment; major psychiatric illness; concurrent receipt of various rehabilitation services; undergoing palliative care (life expectancy <6 months); with chronic bedridden status; and those who refuse to participate will be excluded.
The recruitment program is scheduled to take place from April 2024 to March 2025 and will be conducted in randomly selected subdistricts through recruitment posters appearing on both online and offline communities. Our target group consists of older adults who are in need of and interested in CBR. The recruitment posters will provide an initial understanding of the study, and potential participants can utilize the contact information displayed on the poster to communicate with our researchers and gather more information thereon. The personal information of interested participants will be registered. Individuals who obtain information offline will be directed to their local community health center, where trained community staff will provide information on the study and assist with registration. Our study will apply inclusion and exclusion criteria to screen both online and offline registrants to compile a list of potential participants. Invitation letters will be sent to all potential participants to confirm the meeting location (either face-to-face or remote) and time. At these meetings, potential participants will be informed in detail about the study and their rights, including privacy protection and the right to withdraw at any time without any obligation. After confirming, participants will sign an informed consent form to officially join the study. For those who choose not to participate, we pledge to provide necessary support as needed.
Professional volunteers
Forty professional volunteers will be recruited. The inclusion criteria are as follows: (1) students majoring in rehabilitation therapy at medical universities in Zunyi City, Guizhou Province, at the junior or senior level; (2) those who have completed systematic theoretical studies related to rehabilitation medicine; (3) those who have a desire or are already engaged in CBR volunteer activities; and (4) those who choose to voluntarily participate. Exclusion criteria will be as follows: (1) participants who withdraw from the study; (2) those under 18 years of age; (3) those who failed the final assessment at the end of the training period; and (4) individuals with psychiatric disorders or who recently suffered a significant event. All eligible volunteers will undergo a four-week professional training program covering rehabilitation assessment, functional rehabilitation exercises, and rehabilitation knowledge, followed by an objective structured assessment with standardized patients. Those who pass will be certified as professional volunteers and will be included in this study.
Platform development and functional modules
In adherence to the IDEAS framework and through collaboration with a specialized software corporation, 31 we created an interactive digital health management platform focusing on CBR for older adults based on their rehabilitation behaviors and viewpoints. 32 The rapid advancement of information technology has significantly improved the storage and computing capabilities of cloud computing, thereby enhancing the sharing and processing of health information resources. This has dramatically improved the platform's capacity to store, compute, and share data, thus increasing efficiency and innovation in the field. As part of our methodology, we adopted standard cloud computing system construction procedures, entailing the establishment of a distributed cluster system. This process encompasses the creation of a Hadoop cluster, deploying the zookeeper, and building an Hbse cluster. This meticulously crafted system provides robust storage and arithmetic support for our interactive digital health management platform, which is segregated into a web-based administration and a mobile application (Figure 2).
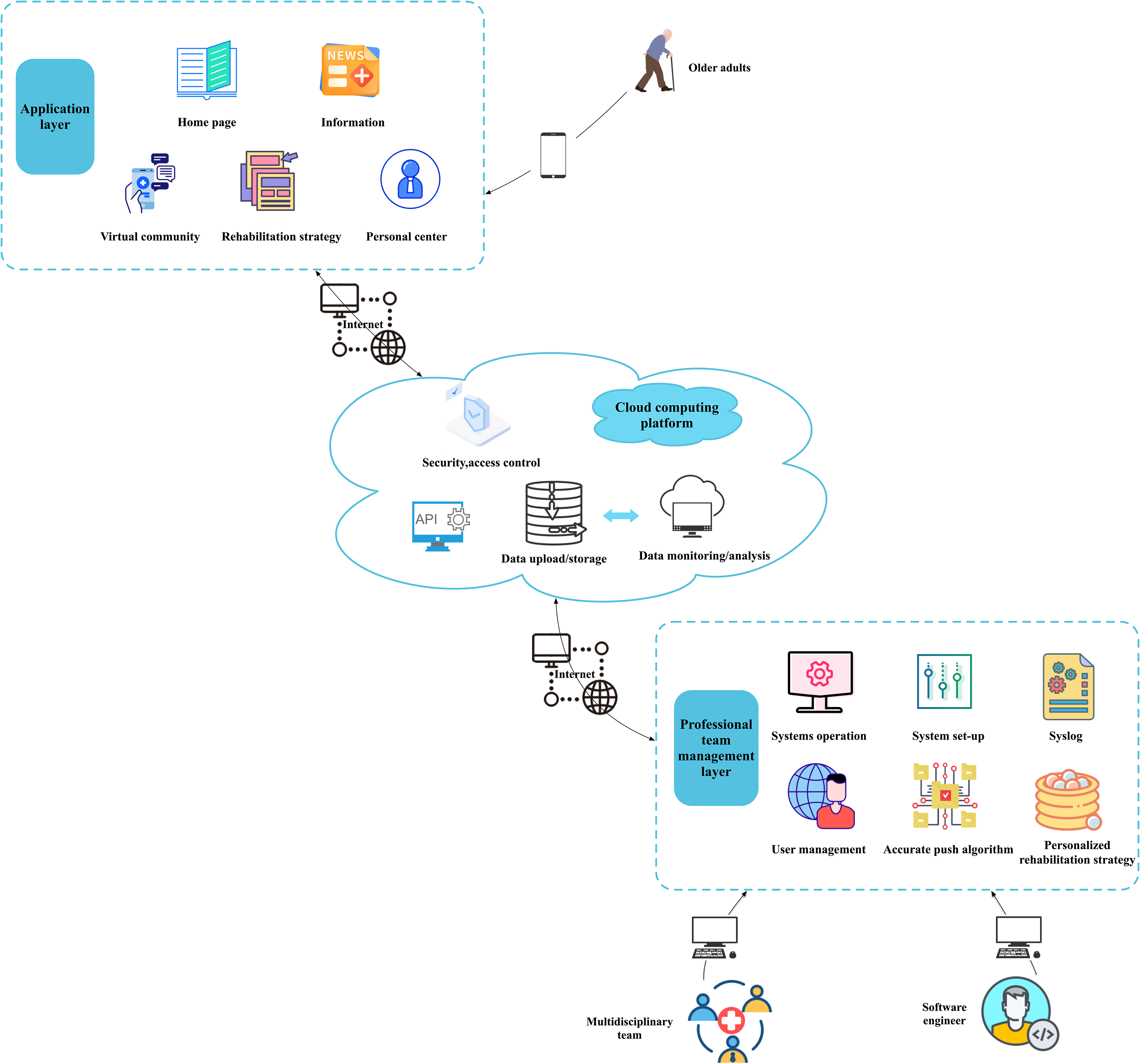
Community-based rehabilitation management platform for older adults utilizing digital health technology (cloud computing platform).
The research team, leveraging administrative accounts, utilizes the web administration for various management functions, including system supervision, configuration settings, user management, message dissemination, and strategy adjustments. The mobile application, Rehabilitation Journey, tailored for older adults, interfaces with the system platform through a web service interface using the HTTPS protocol. All information is stored and retrieved by the Hadoop Distributed File System. The study will employ optimized algorithms to compute the data and assess the user's health metrics and needs. With its secure web administration and user-friendly mobile application, this platform structure ensures a comprehensive and accessible solution for CBR management. The main app functions are listed in Figure 3.

Functions of the rehabilitation journey and key characteristics.
Intervention
Control group
Participants in the control group will receive existing offline CBR services, which include basic functional training (activities of daily living [ADL], walking training, etc.) and health education lectures. Additionally, we have developed an online version of the Rehabilitation Information Booklet for Older Adults based on Hyper Text Markup Language 5 (HTML5) technology. This digital resource provides comprehensive information on standard rehabilitation practices, health literacy, the locations and contacts of rehabilitation organizations, and details about our research team. To enhance user experience, a voice interaction enables participants to access information via voice commands and reducing operational complexities. Our overarching goal is to provide older adults with a user-friendly and visually intuitive guidance platform through the HTML5 interface. Furthermore, the booklet will be regularly updated by our research team to reflect the latest advancements in medical knowledge and rehabilitation practices, assisting them in better managing their health.
Intervention group
Based on the training program of the control group, we will establish a multidisciplinary joint CBR management team. This team will comprise a rehabilitation physician, a geriatrician, a rehabilitation therapist, a nursing PhD, two clinical nurse specialists, a platform maintenance staff member, and a graduate nursing student. This team will oversee program safety evaluation, with the rehabilitation therapist monitoring the quality of rehabilitation training and adjusting the program accordingly. Clinical nurses will actively participate, assessing and aiding in program execution to monitor participant progress. The nursing PhD will coordinate the intervention process, while the graduate student will handle study recruitment, implement intervention measures, and manage data collection and analysis. The platform maintenance staff will maintain the older adult CBR management platform.
The CBR management platform, Rehabilitation Journey, will be developed specifically for older adults utilizing cloud computing technology. This platform is designed to administer rehabilitation management for participants in the intervention group over 12 months, which encompasses six months of personalized intelligent rehabilitation guidance and a follow-up of six months. The platform's main objective is to offer personalized rehabilitation strategies and targeted guidance by tracking and analyzing participants’ rehabilitation needs and processes. Initially, participants will register and provide their personal information through Rehabilitation Journey, including their demographic details, medical history, and rehabilitation service utilization experience. Simultaneously, the platform will conduct the initial data collection and automatically generate electronic rehabilitation files for participants based on their personal information and the collected data. Subsequently, the platform will send out data collection questionnaires once at each of the 3rd, 6th, and 12th month of the study, which is in order to continuously monitor participants’ rehabilitation progress and evolving needs at different points in time. The data will primarily consist of satisfaction with CBR, as well as improvements in participants’ ability to perform activities in daily life, physiological functional status, quality of life, and health status. Following each data collection, Rehabilitation Journey will automatically analyzes the information and generates intelligent rehabilitation management strategies based on the results of the analysis. The multidisciplinary team will then review and adjust this strategy based on participant's progress, culminating in a personalized and scientifically grounded rehabilitation strategy presented in the Rehabilitation Strategy module (Figure 4). The Rehabilitation Strategy encompasses three core components: Rehabilitation goals, outlining general objectives and milestones (0–3 months, 4–6 months); Rehabilitation programs, including physical, speech, occupational, and nutritional therapies to promote the recovery of physical function, as well as psychosocial support to promote the recovery of psychological and social function; and Rehabilitation recommendations, addressing home environment adaptations and assistive device implementation.

Flowchart of accurate rehabilitation strategy based on cloud computing platform.
The Rehabilitation Journey will automatically generate a daily rehabilitation program using the above strategy. The platform will send a reminder message for each upcoming day's rehabilitation program at 6:00 p.m. The Information module will be refreshed and pushed daily with relevant rehabilitation program content. Moreover, the platform will notify participants to schedule a rehabilitation appointment in My Appointment by 9:00 p.m, providing details about the rehabilitation program, including the specific time and location of the rehabilitation (whether in-home, community-based, or online). If the participant fails to attend a scheduled appointment, we will contact them to find out the reason and reschedule the appointment. In addition, the platform will send a reminder message 1 h before the rehabilitation training on the same day, allowing the participant to prepare for the training.
Each trial subdistrict will be assigned two professional volunteers, each responsible for guiding and providing full rehabilitation training for approximately 6–8 participants. The volunteers will provide personalized rehabilitation training based on participants’ rehabilitation program and appointments and are accountable for safety assessments and rehabilitation guidance. Rehabilitation training will occur approximately 3–5 times a week, for 30–60 min/session. The frequency and duration of rehabilitation will depend on the participant's program and progress. The rehabilitation therapists and nurses in the study team will monitor the overall quality of the rehabilitation training.
Furthermore, participants can consult medical professionals regarding relevant rehabilitation topics through the Virtual Community. They can also join various communities to communicate and interact with other participants, share rehabilitation experiences, and offer mutual support based on their disease characteristics, rehabilitation needs, interests, and lifestyle, enhancing social support for participants.
Additionally, during a designated period, participants can document the fulfillment of every rehabilitation task on the Rehabilitation Journey, which will automatically verify the fulfillment status and allocate points. These points will be ranked with the participant's informed consent, showcased on the Homepage, and can subsequently be converted to prizes based on the point value.
Data collection methods
As previously stated, all participants will complete data collection questionnaires at the initial data collection point when the rehabilitation profile is created and subsequently at 3 rd , 6 th , and 12 th month. To ensure smooth data collection, participants will receive a notification of the upcoming assessment task one day before each data collection and will be asked to complete the data collection questionnaire within 24 hours of receiving the notification. These notifications will provide detailed instructions, requirements, and questionnaires for the assessment tasks at different points in time. Each data collection is expected to take approximately 10–15 min. The assessment and data collection will be conducted online, with the intervention group receiving notifications and completing the data collection via the Rehabilitation Journey, and the control group receiving notifications and completing the data collection via cell phone text messages. This standardized approach ensures consistent timing and uniform delivery of assessment-related information to both groups, mitigating potential bias. The concise period for completion promotes participant engagement and adherence to the assessment protocol. The instruments used are as follows.
Community-based rehabilitation needs questionnaire
The research team has developed an older adult CBR needs questionnaire based on the International Classification of Functioning, Disability and Health and the Guidelines for Community-Based Rehabilitation design. 32 It consists of six dimensions and a total of 29 items, covering physiological function needs (13 items, such as defecation and muscle power functions), cognitive function needs (three items, such as cognitive function), individual activity needs (three items, such as self-care functions), social participation needs (two items, such as community life participation), environmental needs (four items, such as cultural and entertainment needs), and informational needs (two items, such as social security and public service information). To evaluate each item, the questionnaire uses a five-point Likert scale ranging from 0 (not needed) to 4 (very needed) to measure the necessity level for each aspect of rehabilitation. A significant need within any given dimension is identified when the average score for an item exceeds 3 points, indicating a substantial requirement for support in that area.
Outcomes
The study's outcomes will be comprehensively evaluated through three dimensions: effectiveness, feasibility, and usability. Firstly, to assess effectiveness, we will use a standardized test instrument to quantify the participant's progress in rehabilitation. The test will contain both subjective and objective indicators. The subjective indicators include EUROPEP scale, ADL, EQ-5D-5L, and health promotion lifestyle profile-II, which will reflect participants’ satisfaction, ability to perform daily life, quality of life, and health status, respectively. The objective indicator is assessed through the Assessment of rehabilitation set for classification of functioning, disability, and health (ICF-RS), which will reflect the specific functional status of participants. Secondly, feasibility is measured in this study through two main factors: engagement rate and attrition rate. Thirdly, to assess participants’ convenience and interactive experiences with the technologies, we will apply the System Usability Scale (SUS). The primary and secondary outcomes measures for this study will be determined using the test instruments described above. We will also include sociodemographic measures as additional outcomes. Through this multidimensional assessment approach to provide a comprehensive understanding of the effectiveness and value of digital health interventions targeting CBR for older adults.
Primary outcomes
With the growing importance of community healthcare services, prioritizing patient satisfaction surveys is crucial. Satisfaction with CBR represents not only the older adults' experience with the quality of the services but is also an important indicator for service providers to enhance their offerings and the effectiveness of rehabilitation. Furthermore, it influences their willingness to participate and their trust in the rehabilitation team. To assess this, we will use the EUROPEP scale, which consists of five dimensions and a total of 23 items. 33 These dimensions include the doctor–patient relationship (six items), health care (five items), information acquisition and support (four items), continuity and cooperation of medical service (three items), and service organization (five items). Respondents will employ a five-point Likert scale, assigning scores from 1 to 5 for “very dissatisfied,” “dissatisfied,” “average,” “satisfied,” and “very satisfied,” respectively. The scale's total score will be computed as the sum of individual item scores, with higher scores indicating increased satisfaction with community healthcare services. The EUROPEP scale has been used in health service satisfaction studies across 16 countries, involving 24,016 patients who have received community-based general medical service, with sufficient technical quality assurance, and indicating a favorable reference for our regional CBR service satisfaction study. It has confirmed consistency, with a Cronbach's α of 0.961, 34 adding credibility and validity to our use of the EUROPEP scale in quantifying participant satisfaction within our study's context.
Secondary outcomes
Activities of daily living: The ADL scale, developed by Lawton et al. in 1969 and later adapted by Yanling et al. 35 for Chinese populations, includes both physical ADL and instrumental ADL, totaling 20 items. The scale is scored on a four-point Likert scale, from “can do it all by myself,” “some difficulty,” “need help,” to “can’t do it at all,” with scores from 20 to 80. A total score of >26 indicates varying degrees of functional decline.
International Classification of Functioning, Disability, and Health-Rehabilitation Set (ICF-RS): The questionnaire used in this study was the ICF-RS developed by Yan Tiebin et al. 36 It comprises 30 entries, with nine for physical functioning and 21 for activity and participation. Each entry is categorized into grades 0–4 based on the severity of the patient's dysfunction as follows: no dysfunction (grade 0), mild dysfunction (grade 1), moderate dysfunction (grade 2), severe dysfunction (grade 3), and complete dysfunction (grade 4). Additionally, ratings that do not provide enough information to describe the severity of the problem are indicated by an 8, while entries that are not relevant to the assessment subject are indicated by a 9. A study has confirmed that the Cronbach's α values for physical functioning activity and participation on the ICF-RS are 0.69 and 0.87, respectively. 37
EQ-5D-5L: Developed by the EuroQoL Group, 38 the scale includes five dimensions of health status and a visual analog scale (VAS), including mobility, self-care, usual activity, pain/discomfort, and anxiety/depression. Each dimension has five levels of difficulty, including “no difficulty,” “mild difficulty,” “moderate difficulty,” “severe difficulty,” and “highly severe difficulty.” The VAS represents a patient's self-assessment of their overall health, measured from 0 to 100, with 0 indicating the poorest state of health and 100 indicating the best. A study verified the scale's consistent reliability, with a Cronbach's α of 0.78. 39
Health promotion lifestyle profile-II: This scale, translated from English to Chinese with cultural validations, 40 comprises six dimensions and 52 items, covering nine items each for health responsibility, nutrition, spiritual growth, and interpersonal relationships, and eight items each for physical activity and stress management. The scale is based on a four-point Likert scale, with options including “Never,” “Occasionally,” “Often,” and “Always.” The scale's total score ranged from 52 to 208 points, and participants were classified into four groups according to their scores: poor, 52–90 points; fair, 91–129 points; good, 130–168 points; and excellent: 169–208 points. There is a positive correlation between the level of a patient's health-promoting lifestyle and their scores. In the reported study, the split-half reliabilities for each dimension ranged from 0.64 to 0.78, the Cronbach's α coefficients ranged from 0.63 to 0.81, and the retest reliability of the scale was 0.69.
Rehospitalization rates: A comparison of unplanned rehospitalization during management in two participants groups.
System Usability Scale: This scale was proposed by Brooke et al. in 1986. Wang et al. later translated and validated the score into a Chinese version for localized use based on the cultural characteristics. 41 System Usability Scale is a widely utilized tool to evaluate the usability of software systems and mobile applications. It consists of 10 items and employs a five-point Likert scale, with 1–5 indicating “completely disagree,” “disagree,” “generally agree,” “agree,” and “completely agree,” respectively. To calculate the score, the contribution of each item is first determined, with a range of 0–4. The scale's rating criteria are as follows: the base value for questions 1, 3, 5, 7, and 9 is 1 point, while the base value for questions 2, 4, 6, 8, and 10 is 5 points. Finally, the sum of all entry scores is multiplied by 2.5, resulting in a total score range of 0–100 for SUS scores. A study has indicated that a mean SUS score of over 70 implies good usability of the mobile application, 42 and the consistency reliability of the scale was a Cronbach's α of 0.84.
Engagement rate: Engagement will be assessed by the engagement frequency, use duration, and engagement level of participants in the Rehabilitation Journey or Rehabilitation Information Booklet for Older Adults. Participation data for the intervention group will be logged automatically through the platform, while participation data for the control group will be logged based on click-through tracking frequency as follows: (i) the engagement frequency will be determined by the total number of logins (the number of times a participant accesses the platform or online manual); (ii) the duration of use will be calculated based on the total number of minutes that a participant spends on the platform or online manual; and (iii) the engagement level will be defined as the number of visits to different pages in the platform or online manual.
Attrition rate: A comparison of the proportion of participants who withdraw from the study during management in two participant groups.
Additional outcomes
Sociodemographic measures
At the beginning of the study, participants will undergo an evaluation of sociodemographic factors through an information form carefully designed by the research team. This form encompasses essential sociodemographic variables, including sex, age, ethnicity, marital status, education, health insurance enrollment, monthly household income, number of chronic diseases, educational acceptance, medical record-keeping practices, and ease of access to CBR services when unwell. This comprehensive sociodemographic assessment ensures a nuanced understanding of participants’ backgrounds and contexts, contributing to the robustness and depth of the study's sociodemographic analysis.
Quality control
Quality control of the intervention
Before intervention implementation, a comprehensive training session and assessment will be conducted for all the study's professionals, community workers, and volunteers. This training will cover aspects such as timing, assessment, intervention methods, and precautions in executing the rehabilitation program to ensure program implementation homogeneity. Enrollment of the intervention and control groups will be based on inclusion and exclusion criteria, followed by a baseline survey and group balance assessment to ensure comparability. To foster participant engagement and compensate for their time and effort, all participants will receive RMB 50 in cash for every completed assessment round, with a total of RMB 200 upon concluding assessments at baseline, 3 rd , 6 th , and 12 th month, to reduce the shedding rate, enhance participant activation, and compensate for the assessment time. Upon submission of the assessment questionnaire, the research team will receive an automatic notification from the platform in cases of any abnormality with the outcome indicators (such as a significant decrease in the total score). When necessary, the participant will be removed from the study and referred to face-to-face services, as appropriate. However, if the assessment questionnaire is not received from the participant, the researcher will send a follow-up message. If the participant does not respond within five days, the researcher will attempt to contact the participant by phone. The participant will be considered a sample dropout if they cannot be reached after two consecutive attempts.
Quality control of platform use
Before intervention commencement, the platform maintenance staff will provide uniform training to research team members on utilizing the CBR management platform, minimizing implementation bias. Standardized training guidance will instruct participants on module usage, ensuring a comprehensive understanding of the platform's features. The research team will create and rigorously vet functional rehabilitation videos and images for this platform. The materials will feature standardized and straightforward content to support participant needs. Additionally, we will respond promptly to participant messages and inquiries.
Platform management and data protection
Regular maintenance by platform staff will ensure the smooth operation of the CBR management platform, with built-in filters for sensitive words and friendly reminders for potentially problematic content. Participants will sign a user agreement and privacy policy, activating privacy settings for enhanced user security. Data privacy and confidentiality will be maintained through unique participant IDs, authorization protocols, and HTTPS technology for secure communications. For risk management purposes, the assessment data will undergo reidentification. The separate storage of de-identified master lists and data will be accessible only to select research team members. HTTPS technology will secure confidential communications, and all data will be stored on a secure server in the People's Republic of China. Participants can request data deletion or withdraw from the study, ensuring their control over personal information.
Data analysis
Data analysis will be conducted using SPSS 29.0 statistical software. Descriptive statistics will be applied to count data, presenting frequency counts and composition ratios. For measured data adhering to a normal distribution, mean and standard deviation (x̄ ± s) will be employed, while non-normally distributed data will be described using the median and interquartile range. Baseline data comparison between the two groups will employ the two independent samples t-test for normal distribution, the chi-square (χ2) test for qualitative data, and the rank-sum test for both. Between-group differences will be examined using the Mann–Whitney U and Kruskal–Wallis tests. To assess trends in satisfaction with CBR services, older adults’ ADL, functional status, quality of life, health status, rehospitalization rates, system availability, engagement rates, and attrition rates at four time points (baseline, 3 rd , 6 th , and 12 th month), repeated measures analysis of variance or generalized linear mixed models will be applied. To minimize the influence of confounding factors, we will use statistical methods employing multivariate analysis techniques. This will control for the influence of confounding factors and ensure that the assessment of intervention effects is as free as possible from the influence of unmeasured variables. Statistical significance for all tests mentioned above will be considered at p < 0.05.
Ethical approval
This study was approved by the Medical Ethics Committee of the Affiliated Hospital of Zunyi Medical University in Guizhou, China (KLL-2023-228). All respondent participants will be informed of the study's purpose, their voluntary participation, their right to withdraw from the study, and their anonymity guarantee. Once participants fully understand the study's purpose, procedures, and methods, they will sign a written informed consent before participating. The study will be conducted in accordance with the Declaration of Helsinki, and all procedures will adhere to the pertinent guidelines.
Dissemination
The study findings will be disseminated through open-access, peer-reviewed journal publications, and participation in research conferences. The study protocol will be presented at local meetings targeting public health managers, specialists in geriatric and rehabilitation medicine, representatives from the voluntary sector, and community health centers. A summarized report of the study results will be provided to interested participants. In cases where the efficacy of this study on older adults is established, the intervention will be duplicated through online portals and healthcare institutions, emphasizing CBR management platforms utilizing digital health technology. The goal is to facilitate community and social reintegration of older adults.
Additionally, as our study was funded by the Guizhou Provincial Department of Science and Technology, we will provide policy recommendations based on our findings. This policy proposal focuses on the potential benefits and data presentation of CBR that utilizes digital health technology to improve satisfaction for the older adults, increase service efficiency, and expand service coverage. At the same time, we will identify the necessary infrastructure, technology, and training support required to implement the process by digital health technology. We aim to promote and apply this proposal in relatively underdeveloped areas such as Guizhou province.
Discussion
This paper describes a protocol for a study aiming to test and evaluate the effectiveness and feasibility of a digital management platform for CBR services for older adults. By using digital health technologies, this platform aims at providing scientifically sound, effective and precise CBR services for older adults, based on a comprehensive assessment of their health characteristics, medical conditions and rehabilitation needs; addressing their comprehensive physical, psychological, social, and environmental needs; facilitating information sharing between doctors and patients; and encouraging older adults as active participants in rehabilitation. This represents a crucial step toward establishing a more comprehensive CBR service system.
Considering the prevailing deficiencies in China's CBR services regarding resource allocation, service coverage, participation of older adults, and the alignment of supply and demand, the study's successful completion will introduce a new tool and a perspective for these services. By effectively integrating the rehabilitation needs of older adults, community-based healthcare providers, and extant rehabilitation resources via digital health technology, the quality and satisfaction of rehabilitation for older adults can be enhanced. This can improve their physical functioning, quality of life, and health status; reduce the risk of rehospitalization; and enhance their social participation ability, ultimately promoting their overall development in the community. Additionally, given its geographic relevance and potential societal impact, the study program and its findings may serve as a valuable blueprint for developing countries and regions grappling with similar challenges.
However, the study has some limitations. First, despite the implementation of robust measures, the sample size is relatively small, potentially leading to unavoidable systematic errors. Second, the study did not assess economic and cost-effectiveness factors, limiting extrapolation of the results. In subsequent studies, there is an intention to augment this research through a more extensive randomized controlled trial and a cost–benefit analysis. This will enable the identification of the best practice and model of CBR services based on digital health technology.
Footnotes
Acknowledgements
The authors would like to thank all community workers and older adults who are participating in this study.
Contributorship
CX contributed to writing the protocol, editing the manuscript, conducting the trial, and collecting the data. LX, KY, JW, XX, WZ, QL, and RD aided in test design, data analysis, and interpretation. LW conceived and designed the research, gave final approval of the manuscript, and ensured the accuracy and integrity of all aspects of the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Medical Ethics Committee of the Affiliated Hospital of Zunyi Medical University in Guizhou, China (KLL-2023-228).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zunyi city science and technology plan project, Guizhou Provincial Science and Technology Projects, (grant number Zun Shi Ke He HZ Zi (2021) No.157, Guizhou Composite Support [2023] General 263).