
Abstract
Background and objectives
There is an increased burden of mental disorders, including substance use disorders (MSUD) in low- and middle-income countries (LMICs). Digital technology offers a viable avenue to scale up the services for MSUD in such settings. This review aims to synthesize existing evidence from systematic reviews and meta-analyses on the use of mobile applications for mental disorders, including substance use disorders in LMICs.
Methods
A comprehensive search for review articles and meta-analyses was conducted in January 2025 and encompassed all relevant studies published until then using the electronic databases PubMed, Scopus, and Embase. Rayyan software was employed to remove duplicates. Data extraction included information such as publication date, title, author, country, number of participants, study design, data collection procedures, instruments/tools used, the profile of healthcare workers, the profile of patients, name of the mobile application, use of the mobile application and privacy policy. Evaluation of risk of bias and quality assessment for the included studies was carried out using the Cochrane tool for assessing risk of bias RoB 2, ROBINS-I for nonrandomized studies, and the Mixed Methods Appraisal Tool. The quality of the included systematic reviews was assessed using A MeaSurement Tool to Assess systematic Reviews.
Results
Twenty-three individual studies that met the eligibility criteria were included in the review. The effectiveness of mobile applications for mental health in LMICs varied significantly across studies. Despite the high burden of substance use disorders in LMICs, only a few studies evaluated mobile applications targeting substance use disorders. While mobile applications offer numerous advantages, significant barriers to widespread implementation remain.
Conclusions
The findings of this review have significant implications for future research, policy, and practice. Given the potential of mobile applications to improve mental health care in LMICs, efforts should focus on enhancing their cultural relevance, usability, and long-term effectiveness.
Keywords
Introduction
Mobile health applications (mHealth Apps) have shown potential in improving mental health outcomes1,2 by providing remote access to care, which is particularly beneficial in low- and middle-income countries (LMICs) where mental health services delivered through traditional channels are often limited in their reach and availability. 3 Mobile technologies are accessible in LMICs, providing a scalable platform for mental health interventions. They can deliver evidence-based health interventions to a broad audience, including underserved populations.4,5 Studies have highlighted the effectiveness of mobile-based interventions in promoting mental health and psychosocial well-being among young people, offering education, information, and psychosocial counseling through mobile platforms. 6 Additionally, mobile applications have been used to support the management of severe mental disorders, improving medication adherence and reducing relapse rates. 7 The use of mobile applications in addressing tobacco, alcohol, and other substance use disorders has been explored, with features such as self-monitoring, notifications, and peer support being commonly integrated into these Apps. These applications can serve as preventive interventions and additional treatment options. 8 The COVID-19 pandemic has also underscored the need for scalable digital health solutions, highlighting the role of technology in expanding mental health support in LMICs. 9 However, while mobile health solutions offer significant potential, challenges such as data costs, limited internet access, and low personal mobile phone ownership in some regions pose barriers to widespread adoption. 10
Recent literature has indicated that mental health mobile-based applications have the potential to improve the monitoring and management of mental health symptoms and disorders.1,11 Research specific to LMICs has explored the effectiveness of telehealth interventions, 12 digital psychological interventions, 13 and other digital technologies, 5 demonstrating acceptability, feasibility, and effectiveness for the improvement of mental health disorders.
Despite the realization of the need for culturally tailored interventions to ensure relevance and effectiveness, direct comparisons between adapted and original interventions remain limited. 14 There has been a growing emphasis on the cultural adaptation of mobile and internet-based interventions crucial for their success in diverse LMIC settings. The development of mobile applications for mental health screening among adolescents in countries like Zambia and South Africa has shown high acceptability among healthcare workers, despite challenges such as internet connectivity and resource constraints. 15
Mobile applications for mental health and substance use disorders have been widely explored in high-income countries (HICs).8,16,17 However, the data pertaining to the use of mobile applications for mental, including substance use disorders (MSUD) has not been systematically compiled in the published literature. Integrating this body of literature is essential to advancing clinical and research work in this domain. Hence, this review aims to synthesize existing evidence from systematic reviews and meta-analyses on the use of mobile applications for mental disorders, including substance use disorders, in LMICs. By consolidating findings from studies across multiple reviews, this review seeks to synthesize the evidence on the effectiveness, challenges, outcomes, and gaps in the implementation of mobile application-based interventions in LMICs.
The current review aimed to explore the use, development and effectiveness of mobile applications in screening, assessment, diagnosis, treatment, management and referral for MSUD in LMICs. It moreover aimed to discuss the challenges that affect the use of mobile applications for screening, assessment, diagnosis, treatment, management and referral for MSUD in LMICs.
Methods
Protocol
This review was conducted and documented according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020). The protocol for the review was registered with the PROSPERO International Prospective Register of Systematic Reviews (Registration No. CRD42025631819).
Databases and search strategy
A comprehensive search for published review articles and meta-analyses was conducted using the electronic databases of PubMed, Scopus, and Embase. This search was carried out in January 2025 and encompassed all relevant studies published until then within these three databases. The search strategy included a combination of targeted keywords and Boolean operators to ensure a comprehensive retrieval of literature relevant to our research focus, as depicted below. The search terms included:
“mobile app,” “smartphone,” “application,” “mHealth app,” “eHealth,” “mental health app,” “digital app,” “telemedicine,” “technolog*,” “phone,” “mobile,” “iphone,” “android,” “mental disorder,” “mental illness,” “mental health disorder,” “psychiatric illness,” “psychiatric condition,” “psychiatric disorder,” “psychiatric diagnos,” “substance use,” “substance abuse,” “substance related,” “substance dependenc*,” “substance misuse,” “addiction,” “addictive disorder,” “detect*,” “manag*,” “assess*,” “treat,” “screening,” “diagnos*,” “monitor,” “support,” “intervention,” “identif,” “refer,” “systematic review,” “meta-analysis,” “meta analysis,” “review,” “metaanalysis,” “metanalysis.”
The detailed search string used across the three databases has been provided in the supplementary file (Supplemental Table S1). The keyword searches covered the fields of title, abstract, and keywords.
Inclusion and exclusion criteria
The selected articles had to meet specific inclusion criteria, i.e. only systematic reviews and meta-analyses that specifically addressed mobile applications used for screening, assessment, diagnosis, treatment, management, or referral for mental disorders, including substance use disorders, were incorporated in this review. Notably, mobile applications aimed at secondary purposes, such as fostering resilience and reducing stigma, were intentionally excluded from consideration. Additionally, this review focused exclusively on individual studies extracted from the included systematic reviews that detailed the development and implementation of mobile applications aimed at the screening, assessment, diagnosis, treatment, management or referral for mental disorders within LMICs.
This review included only systematic reviews and meta-analyses; other types of studies, such as scoping reviews, narrative reviews, and primary studies, were excluded. Additionally, any studies published in languages other than English and full-length articles that the authors could not access were also not considered. In the current review we focused on the previous research from the LMIC settings. This approach also helped as carry out a comparison of the nature of publications form LMIC with the studies form HIC. Such nuanced approach has not been followed in the previous review where the results from the LMIC typically get sidelined.
Study selection
Rayyan software was employed to remove duplicates and document decisions related to including and excluding articles according to the aforementioned criteria. The titles and abstracts of the deduplicated studies obtained from the database searches underwent an initial screening to identify studies that met the inclusion criteria. Two reviewers (RKB and PB) conducted this screening independently, blinded to each other's preliminary decisions. During the initial screening process, a comprehensive full-text review was undertaken for a few studies to address any ambiguities surrounding the criteria for inclusion and exclusion. This thorough examination was carried out in cases where the necessary information was insufficiently detailed in the title and abstract, ensuring that all relevant data were considered for a more accurate assessment. Any discrepancies between the reviewers’ decisions were resolved through discussions with a third reviewer (GS) until an agreement was reached.
The initially identified 192 articles underwent a thorough full-text screening process, which was conducted by one reviewer (RKB). Following this rigorous evaluation, individual studies that met the inclusion criteria were extracted, which then advanced to the data extraction stage in two distinct phases. In the first phase, we identified key characteristics of each selected study, i.e. study design, population and outcome measures. Secondly, we focused on extracting and synthesizing detailed findings from each study such as assessing the quality and validity of the studies followed by quantitative and qualitative findings.
Data extraction
Data extraction from the included studies after evaluating the full-text articles included information such as the publication date, title, author, country, number of participants, study design, data collection procedures, instruments/tools used, the profile of healthcare workers, the profile of patients, name of mobile application, use of the mobile application and privacy policy associated with the mobile application.
The studies were categorized based on disorder domains, including depression and anxiety-related domains, substance use disorder domain and other mental health conditions domain. Other important factors included the application for treatment and intervention, ethical considerations, and potential barriers. Moreover, the origin of application development was noted by the countries where these applications have been used and tested. Additionally, the languages in which the applications were offered, the platforms on which the applications were available (such as Android, iOS, or Windows), and the feasibility and acceptability of these applications across different countries were examined. The target audience for these applications was identified, specifying which cadre of healthcare workers or patients were these applications targeted at, and the focus areas of the applications (screening, brief intervention, assessment, diagnosis, treatment, or referral).
Critical appraisal methods
Additionally, one rater (RKB) evaluated the risk of bias and quality assessment for the included studies. To ensure a systematic approach, the evaluation utilized various established assessment tools. For randomized controlled trials (RCTs), the Cochrane Risk of Bias Tool (RoB 2) was used. 18 Non-randomized studies were evaluated using Risk of Bias In Non-randomized Studies (ROBINS-I)—of Interventions. 19 For mixed methods studies, the Mixed Methods Appraisal Tool (MMAT) was used. 20 Additionally, the quality of the systematic reviews included in this study was appraised using the A MeaSurement Tool to Assess systematic Reviews (AMSTAR-2). 21 The risk of bias ratings was according to the domains specified in each tool's guidelines and were used to support the interpretation of findings reported in studies.
Results
The initial search identified 1025 articles, of which 947 remained after deduplication. These 947 articles underwent a thorough initial screening process, of which 192 articles met the criteria for an in-depth full-text review. Furthermore, the individual studies were extracted from an extensive evaluation of 17 systematic reviews that met the established criteria for inclusion and exclusion. Three of these systematic reviews included meta-analysis as well. Ultimately, 23 individual studies that met the eligibility criteria were included in the review.
Figure 1 illustrates the flow diagram that outlines the review process and the results at each stage.

PRISMA flow chart depicting the study selection process.
The current review included twenty-three studies that met the specified inclusion and exclusion criteria. The geographical location of the studies was diverse across LMICs. Ten studies were conducted in India,22–31 three in Iran32–34 two in South Africa,15,35 one each in Lebanon, 36 Malaysia, 37 Jordan, 38 Kenya, 39 Afghanistan40, Gaza, 40 and Dominican Republic. 41
A total of seven RCTs, which include cluster RCTs, parallel-group RCTs, and single-blind RCTs, were conducted to evaluate the effectiveness of various interventions rigorously. In addition, four feasibility studies assessed the practicality, acceptability, and initial clinical effectiveness of these interventions. Two pre–post evaluations and two quasi-experimental studies were also included. Furthermore, three cross-sectional studies provided insights into specific health conditions and the impact of interventions at a singular point in time. Moreover, five mixed-methods studies integrated quantitative RCTs with qualitative explanatory research to enhance the understanding of outcomes.
Primarily, the studies focused on adult populations, with most participants aged between 18 and 50 years. Moreover, some studies specifically focused on younger age groups such as children aged 2–7 years 23 and 5–13 years. 38 Overall, the studies included participants from a wide range of ages, with the most common age groups being young adults (18 to 30 years) and middle-aged adults (30 to 50 years). Ten studies included female participants, whereas one study included only male participants 42 three included adolescents and one included college students. 29
Five studies primarily involved healthcare workers such as Accredited Social Health Activists (ASHA) and Primary or Community Healthcare Doctors as the primary focus.25,27,28,41,43 Most of the studies were published between 2017 and 2024 (Table 1).
Studies included in systematic review of the depression and anxiety-related disorders.

Note: ASHA:Accredited Social Health Activists; IPT: interpersonal therapy; EDSS: Electronic Decision Support System; AUDIT: Alcohol Use Disorder Identification Test; PTSD: posttraumatic stress disorder.
Out of the 23 studies, 1615,22–24,26,28,30–32,34–37 focused on depression and anxiety (Table 2), two29,42 addressed substance use (alcohol) (Table 3), three explored neurodevelopmental conditions such as autism35,38, 57 (Table 3), one addressed insomnia 33 (Table 3) and one focused on schizophrenia 31 (Table 3).
Studies included in systematic review of substance use disorders and other mental health conditions.
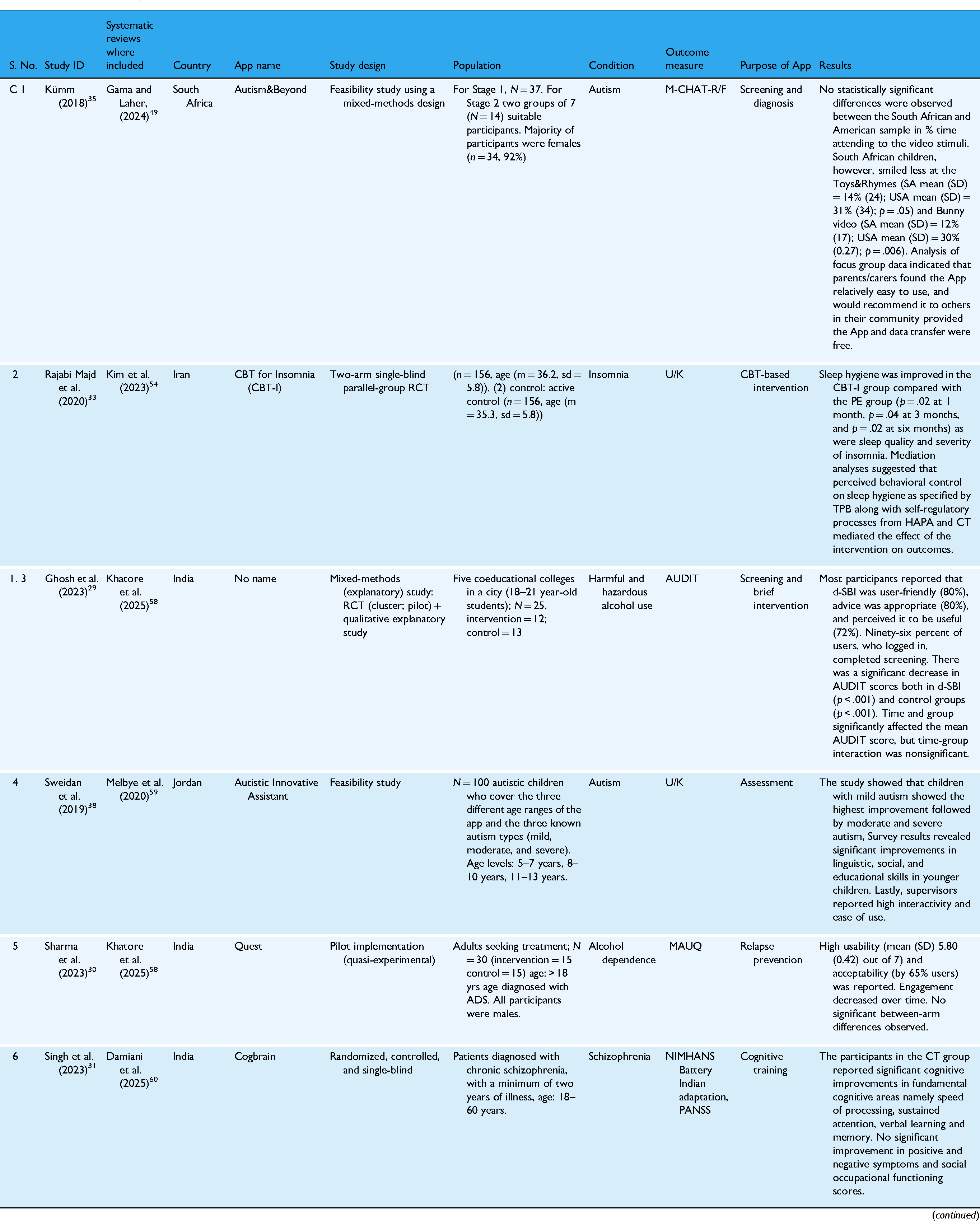
Note: CBT:cognitive-behavioral therapy; ASD: autism spectrum disorder.
Overall quality of systematic reviews included in the current review.

The Tables 1 and 2 report the selected studies’ characteristics including, application name, country, study design, outcome measure, population and results based on various domains for studies included in the review.
Mobile applications for screening and assessment
Three mobile applications were specifically designed for screening, allowing patients or healthcare workers to identify potential mental health issues.15,39 Two applications also incorporated assessment, diagnosis and management alongside screening.28,35 One application focused solely on assessment. 38
Mobile applications for treatment
Eight apps were specifically designed for cognitive-behavioral therapy (CBT)-based interventions involving behavioral activation, structured therapeutic exercises, mindfulness, and relaxation-based support.25,26,30–34,37 Two applications facilitated referrals to mental health professionals.25,43 Additionally, one application used game-based interventions, incorporating interactive elements and gamification. 22 One application included cognitive training–based intervention delivered via mobile or tablet. 31
Mobile applications for management of comorbid conditions
One application addressed the management of comorbid depression, alcohol, and tobacco use along with other chronic conditions. 28 Two others focused on helping users track their progress and maintain well-being.24,26
Mobile applications for depression and comorbid MSUD conditions such as anxiety and posttraumatic stress disorder
Most of the studies specifically addressed the use of mobile applications for depressive and anxiety disorders. One study explored postpartum depression in women. 32 A study in Iran reported a significant decrease in postpartum depression symptoms after two months of mobile-based CBT intervention. 32
Three studies examined combinations of depression, posttraumatic stress disorder (PTSD), substance use, anxiety, and self-harm. In Zambia and South Africa, 15 Groen et al. (2022) assessed a mobile app for screening depression, PTSD, anxiety, and substance abuse among female nurses. The app was deemed feasible and high-quality, though engagement strategies and visual design were lacking. 15 A study in Gaza found a mobile app effective in screening for depression and PTSD in children, identifying symptoms such as hyperarousal and somatic concerns. 40
The evaluation of the effectiveness of a CBT-based mobile intervention among adults residing in Lebanon explaining its effectiveness in significantly reducing the symptoms of depression, anxiety and posttraumatic stress along with improving overall well-being and functioning. 36
Six studies focused exclusively on depression. One piloted a behavioral activation intervention in Brazil and Peru, showing success among women aged 41–60. 50 Another study conducted in India investigated the feasibility or clinical effectiveness of a mobile application for screening depression indicating a high sensitivity of the screening tool and overall satisfactory performance of the screening measure in facilitating further assessment and diagnosis. 24
Mehrotra et al. (2018) tested a self-help app PUSH-D for the management of depressive symptoms and incorporated CBT and interpersonal therapy-based intervention. It was found to be effective in decreasing depressive symptoms and increasing well-being significantly. 26 Caplan et al. (2018) evaluated the feasibility of a CBT-based intervention using a mobile app among primary healthcare workers. They found it to be useful but identified several barriers including issues related to digital literacy, connectivity concerns and cultural considerations. 41 Another study explored the acceptability and practicality of a mobile application specifically designed for ASHAs to deliver screening and counseling services. The findings revealed that despite facing challenges due to limited digital literacy, the ASHAs reported a notably positive and transformative experience while engaging with digital technology. 27 Prabhakaran et al. (2019) evaluated a mobile application-based intervention aimed at managing comorbid conditions such as depression, alcohol use, and tobacco use among patients with hypertension and diabetes. The study found that the mWellcare application did not have a significant impact on these comorbid conditions when compared to usual care. 28
In Malaysia, a mobile intervention led to a significant reduction in depression, though not in anxiety. 37 A study in Iran evaluating the Yara mindfulness app found significant improvements in anxiety and sleep quality, but not in suicidal thoughts. 34
A WHO mental health Gap Action Programme Intervention Guide (mhGAP)-based app in Kenya demonstrated feasibility for screening depression. 39 Maulik et al. (2020) evaluated the feasibility of a mobile-based Electronic Decision Support System for healthcare workers in India, designed for screening and referral of depression and anxiety, highlighting its role in the significant reduction of depression and anxiety symptoms. 25
Khoja et al. (2016) evaluated a mhGAP-based mobile app for screening and referral in Afghanistan, finding it acceptable and feasible. 43 Another study used a game-based intervention to address anxiety, depression, and conduct problems, showing effectiveness and cultural adaptability. 22
Mobile applications for substance use disorders
Two studies focused on alcohol dependence. One app was piloted for relapse prevention, with no significant group differences, though usability and acceptability were high (65%). 30 Additionally, Ghosh et al. (2023) piloted a screening and brief intervention app for hazardous alcohol use among Indian college students, showing significant Alcohol Use Disorder Identification Test score reductions and positive user feedback. 29 One application specifically targeted relapse prevention for alcohol use disorders. 30
Mobile applications for neurodevelopmental disorders
Three studies addressed autism. One tested a mobile screening tool for autism, intellectual disability, and typical development. 23 Kümm et al. (2017) evaluated the “Autism & Beyond” mobile-based application for screening and diagnosis through interactive video stimuli, reporting no significant difference between American and South African children in terms of the percentage of time spent attending to the video stimuli. However, South African children smiled less during the “Toys & Rhymes” and “Bunny” videos compared to American children. Additionally, the application was reported to be feasible and easy to use by the users. 35 Sweidan et al. (2022) assessed the feasibility of a mobile application for screening autism in adolescents, reporting it to be highly interactive and easy to use. 38
Mobile applications for other disorders
One of the studies evaluated a CBT-based intervention delivered via a mobile application, finding it significantly effective in improving sleep quality, sleep hygiene, and symptom severity in patients suffering from insomnia. 33
Additionally, a study from India evaluated the use of an application-based intervention for providing cognitive remediation to patients with schizophrenia. It reported significant improvements in fundamental cognitive areas—namely, speed of processing, sustained attention, and verbal learning and memory. However, no improvement was observed in positive and negative symptoms or social-occupational functioning scores. 31
Operating system
Most of the smartphone applications were available on Android devices only, and only two were available on the iOS platform.36,37
Access and implementation barriers
Across multiple studies, several common barriers to access and implementation were identified, significantly affecting the effectiveness of interventions. These included limited digital literacy, poor internet connectivity, high dropout rates, and logistical constraints such as time, transportation, and cost. Many interventions required smartphone proficiency, thereby excluding individuals with low technical skills or illiteracy, particularly in LMICs.34,39,50 In these remote regions, connectivity issues affected not only data transfer but also the real-time usability of mobile health (mHealth) applications and services.39,40
Furthermore, several studies highlighted issues with user engagement and adherence to sessions.34,36,50 To overcome this issue, strategies such as timely reminders 32 or phone-based monitoring 26 were introduced to encourage ongoing participation. Recruitment difficulties were also reported—particularly when targeting marginalized populations such as refugees, who were often overlooked in outreach efforts.34,39 Lastly, some interventions excluded persons who lacked adequate digital access or technological proficiency.31,33,50
Nevertheless, despite these barriers, many studies employed innovative solutions, demonstrating feasibility through adaptive delivery models and effective task-shifting approaches. These strategies successfully integrated interventions into existing healthcare systems, enabling scalable delivery in LMIC settings.
Cultural considerations
Most studies included basic cultural adaptations, such as translations into local languages like Arabic, Persian, Hindi, Kamba, and Spanish, along with simplified language and visuals for accessibility.24,36,39,50 Some studies incorporated locally relevant examples and stigma-sensitive narratives to connect more effectively with target populations.29,32,34,36 For example, Ghosh et al. (2023) tailored their intervention for urban Indian college students by using culturally aligned norms and peer language to enhance engagement. Additionally, for low-literacy populations, several interventions included audio illustrations and video guidance to improve usability and comprehension.34,39,40
Similarly, collaborations with local service providers or community health workers were shown to enhance cultural relevance and program acceptance.24,39,50 However, a few studies lacked deeper cultural adaptations—such as consideration for religious beliefs, geographic region, or gender norms. For instance, Singh et al. (2023) implemented a cognitive training app for patients with schizophrenia without incorporating any such cultural tailoring. 31
Overall, studies that incorporated cultural customization reported better intervention outcomes, increased user satisfaction, and greater trust and engagement from participants.
Risk of bias and quality assessment
The risk of bias assessment of RCTs was evaluated using the RoB 2 tool. It was found that two studies reported a high risk of bias primarily due to bias in randomization, deviation from intended intervention and bias in the measurement of outcome, whereas two studies reported a low risk of bias exhibiting high methodological quality and rigor in their research design and execution. In contrast, the other three studies reported some concern due to a lack of information regarding the randomization process which could potentially impact the validity and reliability of the conclusions drawn from these studies.
Additionally, the nonrandomized studies were evaluated using the ROBINS-I tool where it was found that three studies had a high risk of bias primarily due to bias in confounding, selection of participants, missing data and measurement of outcome. On the contrary, seven studies displayed a moderate risk of bias arising due to minor faults in the selection of participants, deviations from the intended deviations and unclear information in a few domains. Only one study was found to have a low risk of bias exhibiting high methodological quality and rigor in their research execution. Overall, the nonrandomized studies reported a moderate risk of bias (Figures 2–6).
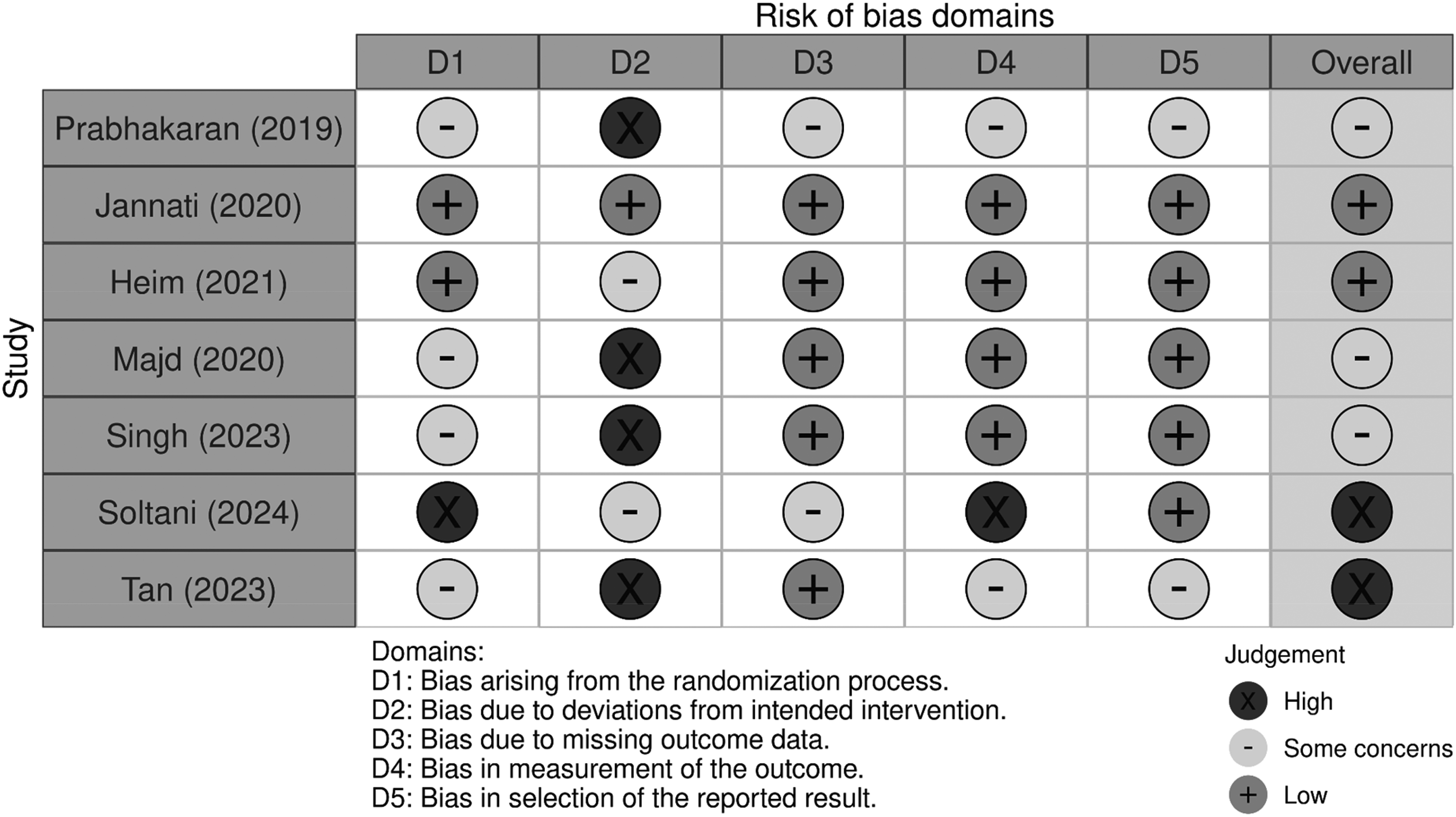
Risk of bias in randomized control trials.

Overall risk of bias in randomized control trials.

Risk of bias in nonrandomized studies.

Overall risk of bias in nonrandomized studies.

Overall risk of bias in mixed-method study.
The studies using a mixed-method design were evaluated with MMAT, and four studies exhibited high methodological quality, whereas one study exhibited moderate methodological quality. The only concerns were the insufficient data regarding the integration of qualitative and quantitative approaches and failure to address inconsistencies between findings.
The overall quality of the included systematic reviews and meta-analyses was assessed using the AMSTAR-2 tool. In total, eight review articles were rated as having moderate quality. This was mainly due to several issues, including the lack of a description of the excluded studies, insufficient information about funding sources, the absence of registered study protocols, lack of search strategy and the inability to conduct a risk of bias assessment in the studies. Similarly, eight studies reported low quality due to critical assessment flaws, including the absence of registered study protocols and a lack of description of excluded studies. This made it challenging to evaluate the comprehensiveness and rigor of the review process. In contrast, a single study emerged with a high-quality rating, highlighting its excellence among the others assessed (Figure 7).
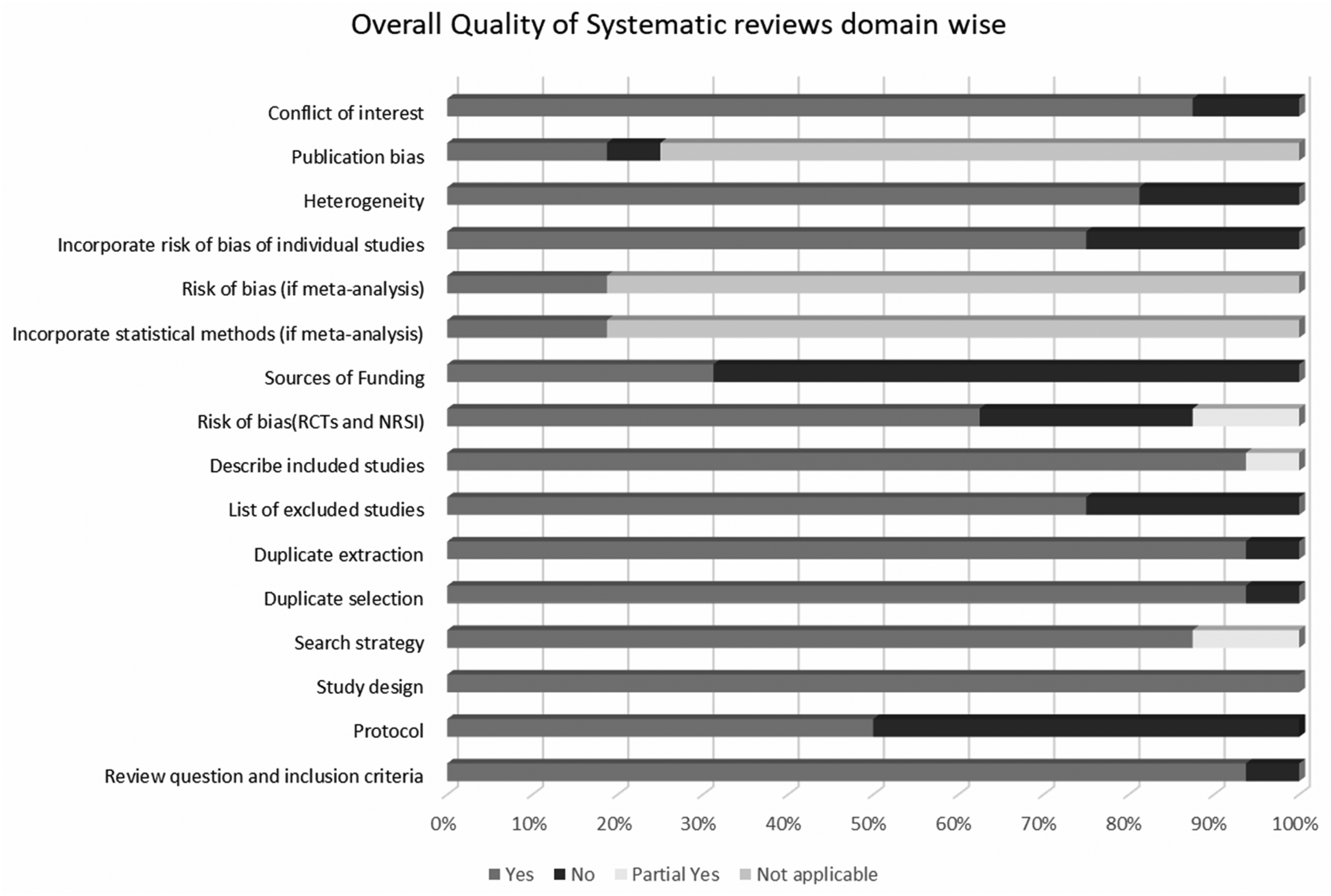
Quality of systematic reviews.
Discussion
This review provides a comprehensive synthesis of evidence from the systematic reviews on the use of mobile applications for mental disorders, including substance use disorders, in LMICs. The findings highlight the potential of mobile-based interventions in improving mental health care, including substance use disorder treatment due to their accessibility, effectiveness, and feasibility. However, key challenges and limitations in the implementation of mobile applications have also been highlighted in this review. To the best of our knowledge, this is the first compilation of evidence on the use of mobile applications for screening, assessment, diagnosis, treatment, management, and referral of mental disorders, including substance use disorders, in LMICs.
The effectiveness of mobile applications for mental health in LMICs varied significantly across studies, with some demonstrating strong positive outcomes while others showed limited or no significant effects. Several interventions, particularly those based on CBT and behavioral activation, were found to be highly effective in reducing symptoms of depression, anxiety, and PTSD.32,33 Game-based interventions also showed promising results, particularly among adolescents and children, with studies reporting high feasibility and engagement. 22 However, other studies found mixed or limited effectiveness. For example, some screening applications were highly sensitive in detecting mental health conditions but did not necessarily lead to improved mental health outcomes. 24 Furthermore, a cognitive remediation app for schizophrenia showed improvements in cognitive functions but did not translate into better social or occupational functioning. 31 The variability in results suggests that while mobile applications have the potential to bridge the mental health treatment gap in LMICs, their effectiveness depends on factors such as intervention type, user engagement, and population-specific needs.
Despite the high burden of substance use disorders in LMICs, only two studies evaluated mobile applications targeting SUDs. The introduction emphasized the importance of technology-driven interventions in addressing alcohol and substance use disorder 8 ; however, the findings indicate mixed results, hence future research could better explain it further. While mobile interventions for alcohol use among college students showed promise in reducing hazardous drinking behavior, 29 relapse prevention apps for substance dependence did not yield significant differences between intervention and control groups. 42 These findings highlight the need for further research into the efficacy and long-term impact of mobile interventions in addressing SUDs.
Mobile applications have been increasingly utilized for neurodevelopmental disorders such as autism spectrum disorder (ASD), with studies assessing their feasibility for screening and diagnosis. As emphasized in the introduction, digital tools have the potential to enhance early detection in LMICs where specialist availability is scarce. 63 The review found that mobile-based ASD screening tools were generally well-accepted and feasible, with applications such as “Autism & Beyond” demonstrating high usability and cross-cultural applicability.23,35 These findings suggest that mobile screening tools may serve as valuable adjuncts in early diagnosis and intervention, though further validation is necessary to establish their reliability and cultural adaptability.
While mobile applications offer numerous advantages, significant barriers to widespread implementation remain. As discussed earlier, digital health solutions in LMICs are often constrained by issues such as limited internet access, data costs, and low mobile phone ownership. 10 These challenges were reflected in the review findings, where several studies highlighted difficulties in sustaining user engagement, ensuring technological accessibility, and addressing privacy concerns.15,25
Mobile health application based interventions have the potential to address the existing gaps persisting in mental health care in LMICs. However, existing literature indicates that accessibility to these interventions is inconsistent and full of challenges. Although many interventions showcased feasibility in controlled or pilot settings, barriers such as inadequate technological infrastructure, limited access and availability of devices or data, and low digital literacy posed significant challenges, particularly in remote areas. Even among populations which were more digitally connected, such as college students residing in urban settings, 29 maintaining engagement has proven difficult. The exclusion of individuals who could benefit from mental health support and may lack digital competence or access raises serious equity concerns.31,34 Use of strategies like regular reminders and frequent phone check-ins have improved adherence and exhibited low dropout rates in some cases. On the other hand, the reliance on external support posed questions about their long-term sustainability.
Moreover, the quality assessment revealed methodological limitations in many of the included studies, with over half rated as having a moderate or high risk of bias due to small sample sizes, lack of control groups, and inadequate follow-up periods. These issues raise concerns regarding the generalizability of findings and underscore the need for more rigorous, high-quality research in this domain.
Mobile applications for mental health and substance use disorders have been widely explored in HICs, where they offer functionalities such as self-monitoring, notifications, peer support, and expert guidance.8,16,17 These applications are often integrated into existing healthcare infrastructures, supplementing traditional mental health services to enhance accessibility and effectiveness.8,16,17 However, despite their widespread availability, a major concern in HICs is the lack of clinically validated evidence supporting their efficacy, with many commercially available apps lacking rigorous scientific evaluation.11,17,64 Systematic reviews have highlighted the need for more robust research to establish the efficacy and safety of these digital interventions.11,17,64 In contrast, findings from our review study indicate that mobile applications in LMICs, while serving similar functions, often operate as the primary mode of mental health service delivery due to a lack of trained professionals and formal healthcare infrastructure. 25 Additionally, while HICs struggle with ensuring clinical validation of commercial apps, LMICs face additional challenges related to cultural adaptation, internet access, smartphone affordability, and digital literacy. 10
The integration of mobile applications into health systems in HICs has been facilitated by established digital infrastructure and regulatory frameworks that ensure their safe and effective use.16,17 In contrast, LMICs often lack structured policies for app-based mental health interventions, leading to inconsistencies in adoption and implementation. While HICs emphasize usability, engagement, and adherence to privacy regulations such as GDPR and HIPAA5, LMICs struggle with basic infrastructural issues and the absence of digital governance.15,25 The COVID-19 pandemic highlighted the growing importance of digital mental health solutions globally, but while HICs leveraged telemedicine and mobile interventions to expand service delivery, LMICs faced considerable barriers in scaling up these solutions due to limitations in funding, internet coverage, and local language adaptability. 14
Limitations
The current review has certain limitations. First, while we included all the relevant systematic reviews and meta-analyses, the included studies varied in methodological rigor, with many displaying a risk of bias due to small sample sizes and lack of control groups. Second, the generalizability of findings may be limited by the heterogeneity of study populations, intervention types, and outcome measures across LMICs. Third, this review included only articles published in English, which may have resulted in the exclusion of relevant studies published in languages other than English. The data regarding use of mobile applications specifically in LMIC was not assessed. Lastly, 20 likely eligible studies were excluded due to the unavailability of full texts, which could have impacted the comprehensiveness of the review.
Future directions and policy implications
The findings of this review have significant implications for future research, policy, and practice. Given the potential of mobile applications to improve mental health care in LMICs, efforts should focus on enhancing their cultural relevance, usability, and long-term effectiveness. There is a need to develop comprehensive mobile-based Clinical Decision Support Systems targeted at common MSUD that integrate screening, diagnostic and management algorithms. Future studies should aim to conduct large-scale RCTs and implementation research to establish efficacy and effectiveness across diverse LMIC settings, explore adaptive and personalized interventions to enhance user engagement and adherence, address barriers related to infrastructure, digital literacy, and affordability to promote equitable access and develop robust data security and privacy protocols to increase trust and adoption of digital interventions. Additionally, policymakers should consider integrating mobile applications into national mental health programs, aligning with recommendations for digital mental health expansion. 9 Collaborations between clinicians, researchers, technology developers and policy and program experts are essential to ensure the rapid development, effectiveness testing, adoption and up-scaling of mobile application-based interventions in LMICs.
Conclusion
The findings of the current review emphasize the emerging interest and growing potential of mobile application-based interventions to support mental health. While studies have demonstrated promising results for use of mobile applications mainly for depression and anxiety; their effectiveness for managing substance use disorders remains limited. It is difficult to draw consistent conclusions because the studies included use different designs, methods, and ways of measuring outcomes. Furthermore, contextual factors such as digital literacy, internet access, cultural adaptation, and policy frameworks significantly influence the feasibility, acceptability, and scalability of such interventions in LMICs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251387056 - Supplemental material for A review of systematic reviews for evidence on use of mobile applications for mental disorders, including substance use disorders, in low and middle-income countries
Supplemental material, sj-docx-1-dhj-10.1177_20552076251387056 for A review of systematic reviews for evidence on use of mobile applications for mental disorders, including substance use disorders, in low and middle-income countries by Riya Kaur Bhatia, Parag Bhardwaj, Anshika Chaudhry, Abhishek Ghosh, Arpit Parmar, Yashita Ahluwalia, Gunjan Singh, Deepshikha Prasad, Pulkit Verma, Neha Dahiya, Ashoo Grover, Siddharth Sarkar and Yatan Pal Singh Balhara in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251387056 - Supplemental material for A review of systematic reviews for evidence on use of mobile applications for mental disorders, including substance use disorders, in low and middle-income countries
Supplemental material, sj-docx-2-dhj-10.1177_20552076251387056 for A review of systematic reviews for evidence on use of mobile applications for mental disorders, including substance use disorders, in low and middle-income countries by Riya Kaur Bhatia, Parag Bhardwaj, Anshika Chaudhry, Abhishek Ghosh, Arpit Parmar, Yashita Ahluwalia, Gunjan Singh, Deepshikha Prasad, Pulkit Verma, Neha Dahiya, Ashoo Grover, Siddharth Sarkar and Yatan Pal Singh Balhara in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors wish to acknowledge the support of the ICMR-MINDS project group.
Ethical approval
The article did not require any data to be collected from human/animal participants and hence did not require ethics committee approval.
Contributorship
YPSB, PV, and ND conceptualized the article; YPSB, PV, ND, AG, AP, RKB, and YA developed the methodology; PB, AC, GS, DP, and AG contributed to the finalization of the methodology; RKB, PB, and GS collected the data and carried out the analysis; RKB, PB, AC, and YPSB prepared the first draft of the manuscript. All the authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Indian Council of Medical Research (ICMR), India via the grant letter NHRP-IST/MH-2/2023-NCD-II.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Yatan Pal Singh Balhara, Professor of Psychiatry, National Drug Dependence Treatment Centre (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi, ypsbalhara@gmail.com, + 919868976365.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.