
Abstract
Background
To explore the accuracy of VR technology for strabismus screening.
Methods
In this cross-sectional study, a total of 191 subjects were included. Examinations included VR technology based on infrared, the cover-uncover test, and the prism alternating cover test (PACT) at various gaze positions, specifically at distances of 33 cm and 6 m. The accuracy of VR in diagnosing strabismus and quantifying the degree of strabismus was evaluated by comparing the VR results to the average outcomes of manual examinations conducted by the two physicians, considered the gold standard.
Results
A total of 88 healthy individuals, 81 exotropia patients, 17 esotropia patients, and five vertical strabismus patients were included in this study, and each subject was screened for less than 2 min. The sensitivity of VR for screening strabismus was 80.3% and the specificity was 80%, displaying moderately consistent with the manual results (Kappa = 0.598, p < .001). The sensitivity for diagnosing exotropia was 76.5% and the specificity was 91.8%, also showing strong agreement with the manual results (Kappa = 0.695, p < 0.001). The sensitivity for diagnosing esotropia was 94.1% and the specificity was 95.4%, with strong agreement with the manual results (Kappa = 0.755, p < .001). The sensitivity for diagnosing vertical strabismus was 80% and the specificity was 98.9%, with strong agreement with manual results (Kappa = 0.719, p < .001). For ocular deviation angle calculations, intraclass correlation coefficient (ICC) was used to compare the agreement between VR and manual results. It showed moderately agreement for exotropia in the near mode (ICC = 0.587, range, −0.036–0.826) and less agreement for exotropia in far mode (ICC = 0.349, range, −0.042–0.615). ICC was in good agreement (ICC = 0.701, range, 0.358–0.879) for the esotropic far mode results (6 m) and not statistically significant for the esotropic near mode results (33 cm). ICC was in good agreement (ICC = 0.606, range = −0.143 to 0.946) for the vertical-near-mode results (33 cm) and not statistically significant for the vertical-far-mode results (6 m).
Conclusions
This novel technique for strabismus screening, which utilizes virtual reality technology, enables quick, precise, and straightforward diagnosis of strabismus. It has also shown notable efficacy in accurately measuring the angle of deviation in cases of exotropia.
Introduction
Strabismus is characterized clinically by ocular misalignment, involving inward or outward or, less commonly, an upward or downward deviation. 1 Strabismus has a prevalence of 2–5%2–4 and can develop at any age, most often diagnosed in children. It can cause diplopia, blurred vision, 1 and other symptoms, which can affect visual function and eye development, especially for children. Therefore, it is necessary to differentiate, screen, monitor and diagnose strabismus in a timely manner. The diagnosis of strabismus relies primarily on the cover-uncover test (CUT). The angle of strabismus deviation is commonly measured by the prism alternating cover test (PACT). 5 However, strabismus examination depends on the doctor’s proficiency and subjective judgment. It requires a combination of far and near scenes, patient cooperation, and longer examination times, and the result may not be accurate enough. Combined with the small number of strabismus specialists, the long training cycle, and the inconvenience of real-time retention of imaging data during examinations, early, large-scale screening for strabismus is not clinically feasible.
Humans can see two scenes with two eyes, and the brain integrates the differences between the two scenes (binocular parallax) to create a sense of three-dimensionality. On this basis, virtual reality (VR) technology allows signals to be fed to both eyes to create virtual scenes. Although it is not widely used due to its high cost and maintenance difficulties, its application in both glaucoma and retinal diseases has been reported. 6 In this study, two states of binocular vision under natural conditions, near (33 cm) and far (6 m), were simulated by VR. On this basis, covering can be simulated by closing the screen in front of both eyes, thus simulating manual covering tests. Combined with an infrared camera to capture eye position changes, the output can be quickly obtained so it's possible to diagnose strabismus quickly, accurately, and easily, and to obtain the angle of deviation. This technique offers the possibility of mass screening for strabismus.
Methods
Participants
The study protocols adhered to the Declaration of Helsinki and were approved by the Ethics Committee of the Beijing Tongren Hospital, Capital Medical University (No. TRECKY2020-088). This cross-sectional study took place from October 2022 to February 2023 at Beijing Tongren Hospital. Written informed consent was obtained for this study from the subjects themselves, 18 years of age and older, and from the parents or legal guardians of minors.
Patients aged 3–71 years were recruited consecutively in the outpatient clinic. They had minimum visual acuity in both eyes (at least 0.1), had normal intelligence and mental status, were able to cooperate with the ophthalmologic examination and the VR examination, had no organic ophthalmologic disease (including nerve palsy and thyroid eye disease) and all agreed to participate in the project. They were measured at a distance (6 m) or near (33 cm) by a concurrent prism covering test and categorized as exotropia or esotropia (10 or more prism diopters horizontally, vertical strabismus (five or more PD vertically), and normal (less than 10 PD horizontally and less than five PD vertically). In addition, patients with no ability to gaze in either eye, who have organic eye disease, mental illness or intellectual problems who are unable to cooperate with the examination, and who did not agree to participate in this study were excluded.
Two specialists in strabismus and pediatric ophthalmology performed alternate cover test (ACT) and CUT on patients in the outpatient clinics, and then guided the patients to undergo strabismus examination with VR. The average of the examination results of the two specialists was used as the gold standard, and the agreement of the four groups of VR results with the gold standard was compared separately.
System description
The strabismus screening technique we explored consists of a head-mounted VR device and a computer. The head-mounted VR device used was the “Qiyou 2S” from Aqiyi corporation, with a resolution of 3840 × 2160, a refresh rate of 75 Hz, 818 pixels per inch which includes an infrared camera mounted on it to provide eye tracking data. The VR device was connected to the computer via a cable. The images captured by the infrared camera were rendered in real-time on the computer screen using Unity 3D. For ease of operation, a menu interface containing all functions for VR scene construction and strabismus diagnosis was created using Python (Picture 1).
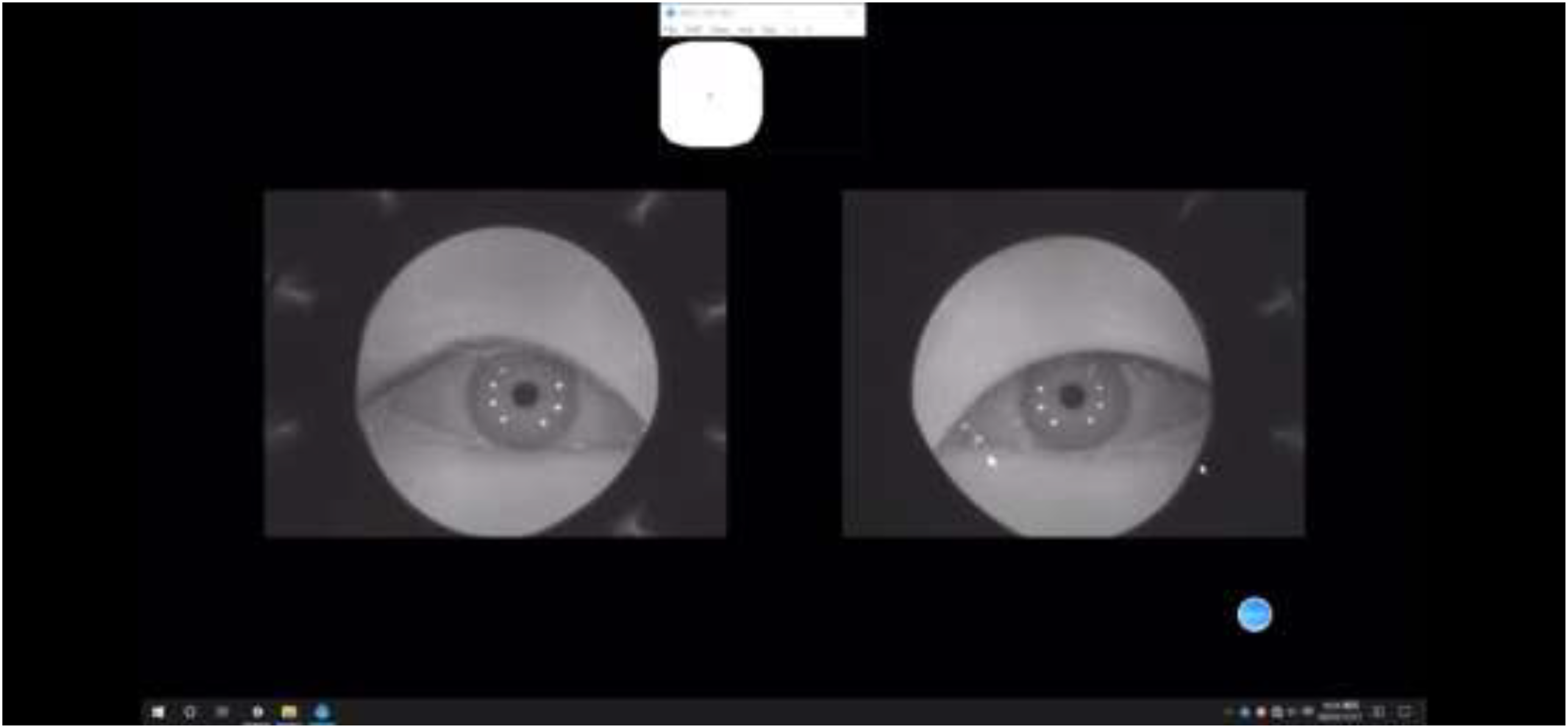
The VR environment was designed with a white background, and the virtual target was a green dot, which both eyes of the patient could see the target on the screen. In the menu screen, the operator can select both near and far modes. Adjusting the size of the reticle simulates both near and far vision, with the distance between the target and both eyes being 33 cm in the near mode and 6 m in the far mode (Picture 2 and Picture 3).
To simulate the cover test, the program can block each screen and observe it through eye tracking to identify whether the eye moved or not and calculate the angle of ocular deviation. We refer to and update the calculations of Yeh and Miao et al.7,8 by setting up a coordinate system that captures the deviation of the pupil in the horizontal and vertical directions and incorporating it into the following equation:

Statistical analysis
VR can diagnose strabismus, determine the type of strabismus, and calculate the arc of ocular deviation by measuring the eye movement angle, which is converted to obtain the strabismus prism degree. The accuracy, specificity, and sensitivity of VR in diagnosing strabismus were assessed using the average of the results of two physicians’ examinations as the gold standard. The agreement of VR with the gold standard in the diagnosis of strabismus was tested by the Kappa consistency test, and P < .05 was considered statistically significant. Kappa takes a value in the range of 0 to 1, where 1 represents complete consistency and 0 represents complete inconsistency. 0–0.2: untrustworthy; 0.21–0.4: low consistency; 0.41–0.60: moderate consistency; 0.61–1: high consistency. The Bland-Altman plot, intraclass correlation coefficient (ICC) and 95% confidence intervals were used to assess the agreement of the strabismus angles obtained by VR with the gold standard based on a two-way random effect, absolute agreement, and single measurement. The Bland-Altman allows a visual assessment of the distribution and bias of the data by graphically displaying the 95% consistency bounds. Good consistency is indicated when the data are evenly distributed around the mean difference and all lie within the 95% consistency boundaries. ICC takes a value in the range of 0 to 1, where 1 represents complete consistency and 0 represents complete inconsistency. 0–0.1: no consistency; 0.11–0.4: low; 0.41–0.60: moderate; 0.61–0.8: high consistency; 0.81–1: very high.
Statistical analyses were performed by SPSS 26.0 and Medcalc 15.2.
Automated VR examination
The operator places the VR device on the patient and asks the patient to gaze at the virtual target in the VR environment with both eyes. The operator independently selects either the ACT or CUT in the menu interface in the near (33 cm) or far (6 m) viewing mode. For ACT, the screen of one eye is covered for 2 s and the screen of the other eye for 2 s, constituting once ACT. Each patient performed ACT 4 times to observe the eye position changes. As for CUT, monocular cover 2 s followed by un-cover 2 s, which counts as once cover un-cover test. Repeated for 4 times for each eye to observe the changes in eye position of both eyes respectively. The operator clicks on the automatic diagnosis, and eye tracking technology automatically captures the distance of the eyeball deviation, which is then inputted into the formula to measure the angle of strabismus. Combining the amount of strabismus and the deviation of the eye position in near and far mode, the system automatically diagnoses strabismus and determines the type of strabismus (Picture 4).
Result
A total of 88 healthy individuals, 81 patients with exotropia, 17 patients with esotropia, and five patients with vertical strabismus were included in this study, and each subject was screened for less than 2 min.
The demographic characteristics of the study subjects are listed in Table 1. The mean age was 16.1 ± 13.2(SD) years (range: 3–63 years); 84 (44.0%) were male and 107 (56.0%) were female. The sensitivity of VR for screening strabismus was 80.3%, the specificity was 80%, and the accuracy was 79.6%, displaying moderate consistency with the manual results (Kappa = 0.598, p < 0.001).
Demographic information of all patients (manual result).
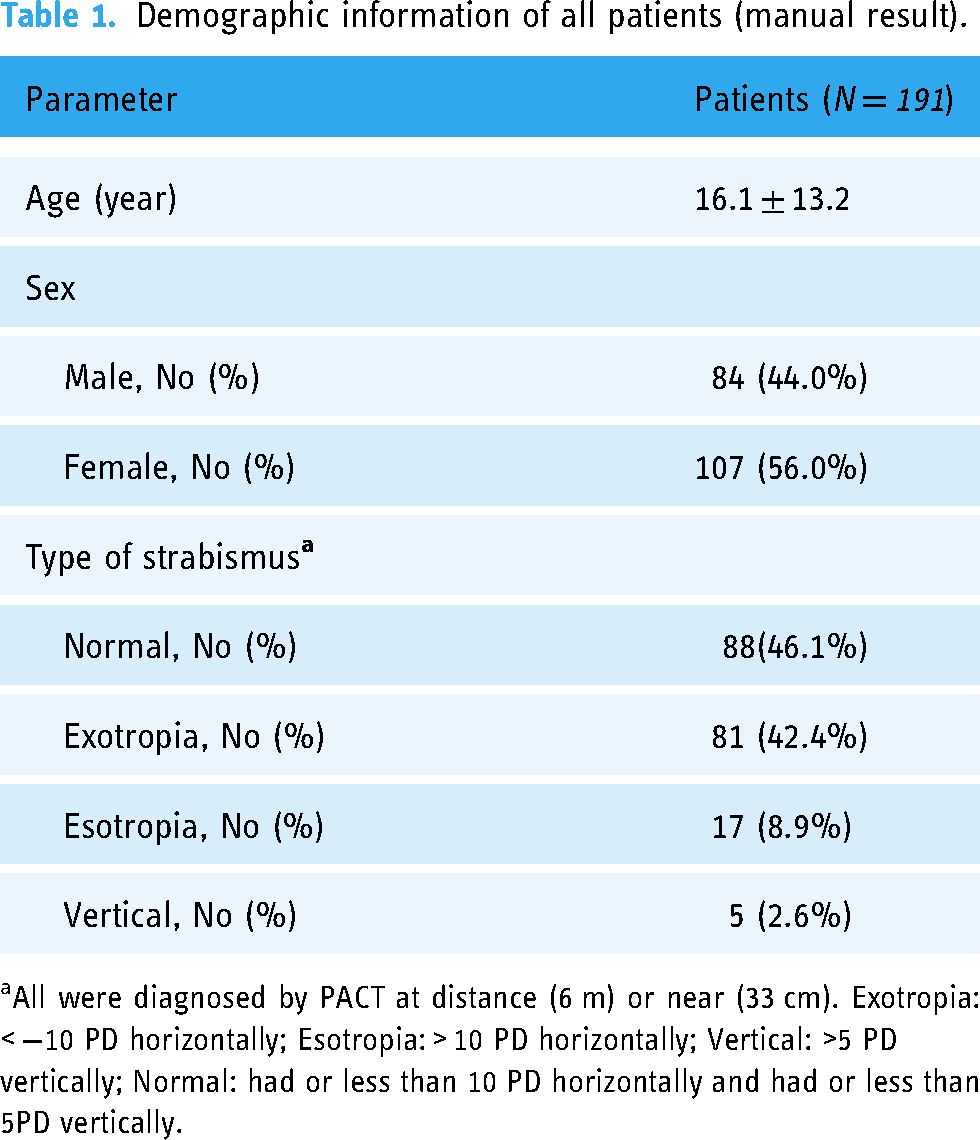
All were diagnosed by PACT at distance (6 m) or near (33 cm). Exotropia: < −10 PD horizontally; Esotropia: > 10 PD horizontally; Vertical: >5 PD vertically; Normal: had or less than 10 PD horizontally and had or less than 5PD vertically.
According to Figures 1 and 2, the agreement between VR and manual results was good in looking near and far. The mean values of the differences between the manual and VR results are −18.0 PD in 33 cm and −17.7 PD in 6 m. This data indicates that there is still a systematic error of about 18 PD between the manual and VR results, suggesting that VR is still not a complete substitute for manual measurement of ocular deviation angle.
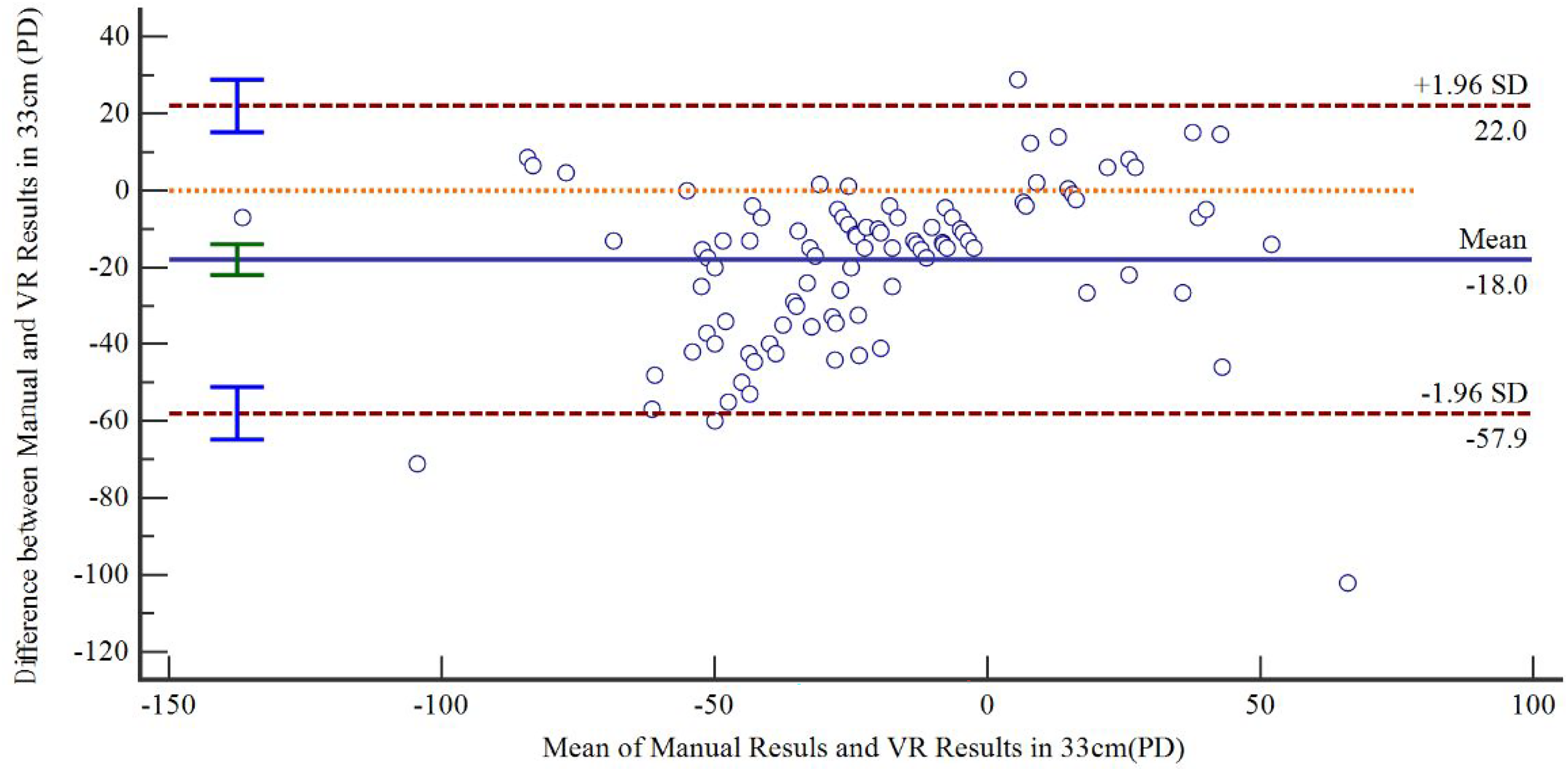
Bland-Altman plot of the difference between manual results and VR results in 33 cm versus the mean of the manual results and VR results in 33 cm. Upper and lower dotted lines represent the 95% limits of agreement. The solid line represents the mean difference, which was −18 PD. VR, virtual reality; PD, prism diopter.

Bland-Altman plot of the difference between manual results and VR results in 6 m versus the mean of the manual results and VR results in 6 m. Upper and lower dotted lines represent the 95% limits of agreement. The solid line represents the mean difference, which was −17.7 PD. VR, virtual reality; PD, prism diopter.

Vr device (Aqiyi Qiyou 2S).

Vr performing ACT in near mode (33 cm).

Vr performing ACT in VR far mode (6 m).
Vr performing ACT in near mode (33 cm) for normal people.
The demographic characteristics of the total 81 exotropia subjects are listed in Table 2. Mean age was 14.9 ± 11.8 (standard deviation) years (range = 4–59 years); 35 (43.2%) were male and 46 (56.8%) were female. The sensitivity for diagnosing exotropia was 76.5%, the specificity was 91.8% and the accuracy was 85.3%, with strong agreement with the manual results (Kappa = 0.695, p < .001). The mean strabismus prism degree is −44.5 ± 27.2 (SD) PD in 33 cm and −37.6 ± 26.5 (SD) PD in 6 m (range = −10∼−140 PD). For ocular deviation angle calculations, intraclass correlation coefficient (ICC) was used to compare the agreement between VR and manual results. It showed moderate agreement (ICC = 0.587, range = −0.036, 0.826) for the exotropic near mode results (33 cm). However, the consistency was poor (ICC = 0.349, range = −0.042, 0.615) for the exotropic far mode results (6 m).
Basic information of VR results.
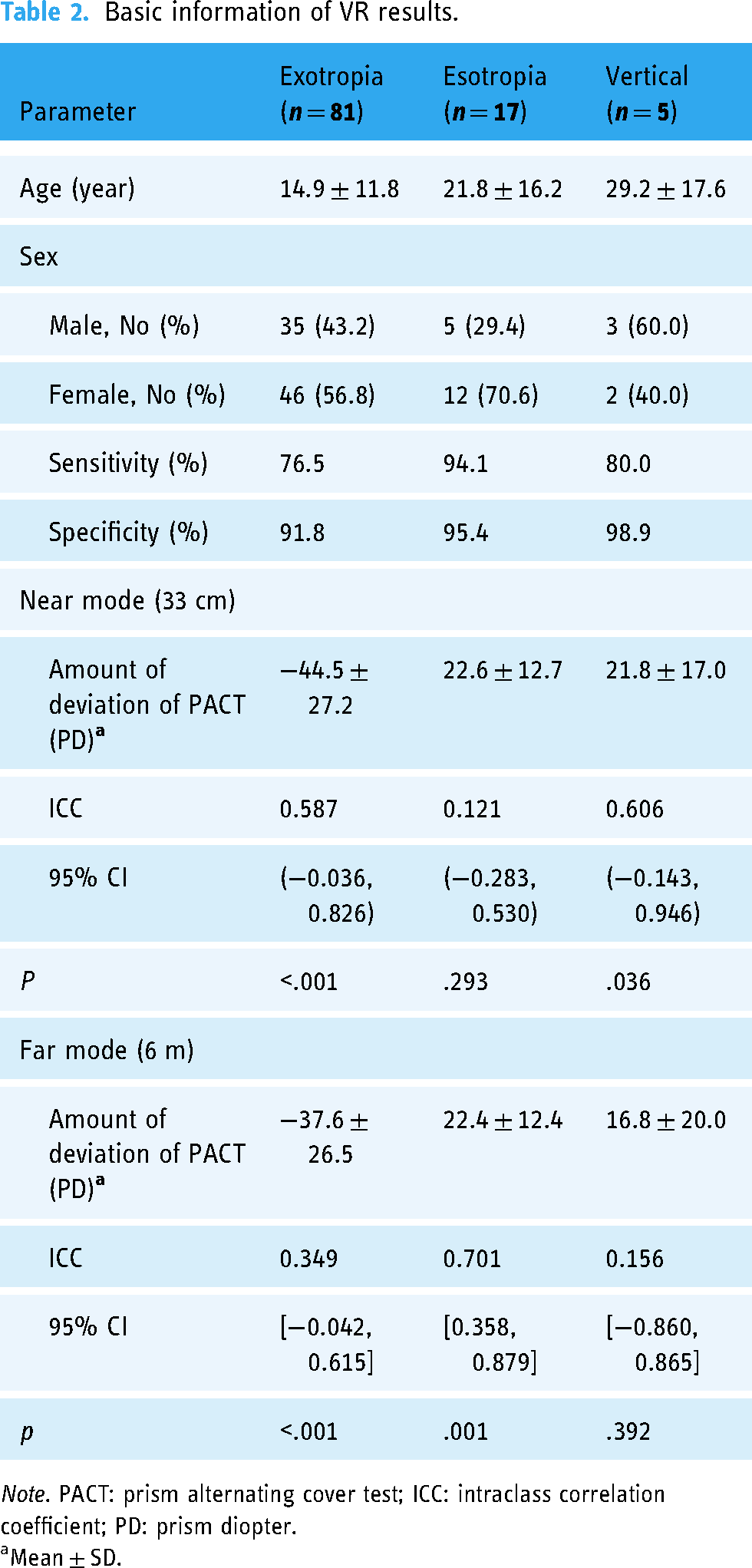
Note. PACT: prism alternating cover test; ICC: intraclass correlation coefficient; PD: prism diopter.
Mean ± SD.
The demographic characteristics of the total 17 esotropia subjects are listed in Table 2. Mean age was 21.8 ± 16.2 (standard deviation) years (range = 5–56 years); 5 (29.4%) were male and 12 (70.6%) were female. The sensitivity for diagnosing esotropia was 94.1%, the specificity was 95.4% and the accuracy was 95.2%, with strong agreement with the manual results (Kappa = 0.755, p < .001). The mean strabismus prism degree is 22.6 ± 12.7 (SD) PD in 33 cm and 22.4 ± 12.4 (SD) PD in 6 m (range = 10–45PD). ICC was in good agreement (ICC = 0.701, range = 0.358–0.879) for the esotropic far mode results (6 m) and not statistically significant for the esotropic near mode results (33 cm).
The demographic characteristics of the total five vertical strabismus subjects are listed in Table 2. Mean age was 29.2 ± 17.6 (SD) years (range = 3–52 years); 3 (60%) were male and 2 (40%) were female. The sensitivity for diagnosing vertical strabismus was 80%, the specificity was 98.9% and the accuracy was 98.4%, with strong agreement with manual results (Kappa = 0.719, p < .001). The mean strabismus prism degree is 21.8 ± 17.0 (SD) PD in 33 cm and 16.8 ± 20.0 (SD) PD in 6 m (range = 5–50PD). ICC was in good agreement (ICC = 0.606, range = −0.143–0.946) for the vertical-near-mode results (33 cm) and not statistically significant for the vertical-far-mode results (6 m).
VR technology has demonstrated excellent performance in the diagnosis and deviation measurement of esotropia in far mode. It was further categorized into two groups, children and adults, and the results are shown in Table 3. Mean age was 8.8 ± 3.4 (SD) years (range = 5–15 years) in children's group and 36.55 ± 11.0 (SD) years (range = 22–56 years) in adults’ group. Compared with the adults ‘group, the children's group had higher sensitivity. The mean strabismus prism degree is 25.0 ± 12.0 (SD) PD in 6 m (range = 5–45PD). ICC was in good agreement (ICC = 0.776, range = 0.301–0.944) for the children's group in far mode results (6 m) and moderately agreement (ICC = 0.661, range = 0.011–0.921) for the adults’ group in far mode results (6 m).
Information for children and adults of VR results in Esotropia.

Discussion
In this study, we found that VR combined with eye tracking can rapidly, accurately, and conveniently diagnose and classify strabismus. The accuracy of VR technology in diagnosing strabismus was 79.5%, with 85.3% accuracy for exotropia and the highest accuracy of 95.2% for esotropia. Although the accuracy of the technique in diagnosing vertical strabismus was up to 98.4%, the sample size in this group was small and the results may still need to be further explored. VR is accurate in all determinations of the type of strabismus, but it is less accurate in diagnosing whether a condition is strabismus or not. In this study, we performed a covering test by simulating a manual looking far and looking near. Patients who had more than 10 PD horizontally or more than five PD vertically in either mode were diagnosed as strabismus However, diagnosing strabismus in clinical practice involves more than looking at the degree of strabismus, but also considering the patient's fusion and accommodation functions, and whether the eye position can be controlled on its own. Due to the large proportion of children with strabismus, there are significant individual differences. Clinicians need to fully break the fusion when performing the covering test, and the covering time of the covering test may be different from the 2 s in this system, in addition to the patient's ability to control the eye position and adjustment, etc., which cannot be improved in this system now.
The intraclass coefficient shows increased agreement for exotropia at near and esotropia at far. It is well known that most of the esotropia is related to accommodation, and for isotropic patients, there is no accommodation stimulus, and no accommodation change in the case of distance viewing, so their esotropia is more stable when they are looking at a distance, so the VR performance in this study is more consistent with the manual results. In the case of near vision, the adjustment function is involved, such as refractive error, eye overuse and inappropriate prescription, etc., which can be excluded from the manual test, while VR is still affected by this part of the test. Similarly, exotropia is also affected by accommodation. In the near mode, the collection ratio of exotropia patients is weaker, the strabismus is more obvious, and the eye position deviation is more likely to occur than in the far viewing condition, so the VR in this study was more consistent in this mode. This study, while exploring a new technique for strabismus screening, obtained conclusions consistent with the pathogenesis of strabismus, and demonstrated laterally that it is possible for this technique to replace manual diagnosis of strabismus and measurement of ocular deviation.
In addition, the agreement between the quantitative results of the strabismus angle from the VR technology and the manual results was good. The high consistency of the near mode results in the exotropia group indicates that it is feasible to build a near-looking scene to simulate the covering test manually. In the esotropia group, the consistency of VR results was the highest among all strabismus types. Considering that there are more adult patients with clinical esotropia, to investigate whether there is a difference in its application between the pediatric and adult groups, it was divided into two groups according to the age of the children and the adults, and the results showed that the consistency of the VR technique was higher for esotropic angles in the children's group, which suggests that it has a good prospect for its application to ophthalmologic disease screening in children.
As of today, there are many AI algorithms that can diagnose strabismus from images with up to 98.89% accuracy, 93.3% sensitivity, and 96.17 specificity, 9 and retaining the image information allows the algorithm to diagnose strabismus. It has also been stated that AI technology can now simulate the masking test, and its results have a high correlation compared to manual results 10 (horizontal deviation R = .90, vertical deviation R = .91, p < .001). Therefore, it is possible to build a scene, perform the covering test through AI, and retain the image data for the automatic diagnosis of strabismus. VR technology gives the human eye a sense of three-dimensionality through binocular parallax, which allows the construction of a scene for looking near and far, 11 combined with an infrared camera to capture the eye movement data, an AI simulation of the covering test, and finally, the use of an AI image processing algorithm for diagnosing strabismus and calculating strabismic angle, which solves the problem of the shortage of clinical strabismus specialist and the problem of long examination time.
Compared to previous studies, this study has the advantage of being quick, easy, and qualitatively accurate, and all patients were diagnosed within 2 min. In addition to this, the VR in this study can screen for large-angle strabismus, independent of the display and spectral technology limitations of the VR device. Miao et al. 12 created a virtual target via VR and converted the position of the virtual target at which the deviating eye was gazing while performing ACT into a strabismus angle. This was limited by the display technology and spectral technology of the VR device, which prevented the examination of large-angle strabismus. However, in this study, eye movement images were captured directly from an infrared camera, and AI technology was used to analyze and calculate the eye position strabismus angle, which can directly screen patients with strabismus of 0–140 degrees with a wider range. However, the consistency of VR in measuring strabismus angle was not high, with the highest only in the esotropia group (ICC = 0.701), while in the exotropia group, it showed an ICC of 0.587. In Yeh et al.'s study, 7 the consistency of VR for quantification of strabismus was above 0.8 and the highest was up to 0.962. The following possible reasons were hypothesized: (1) The effect of the kappa angle was not taken into account, and the change in eye position was not clear enough; (2) During the examination, some patients were younger children, and their inattention led to irregular eye movements, which affected the examination results; (3) VR uses binocular parallax to form a stereoscopic sense, but the patients did not undergo a stereoscopic examination in this study, and it is possible that the stereoscopic function of some of the patients was incomplete, which affected the examination results; (4) In this study, the conversion of radian and trigonometry was carried out by formulae after capturing the angular deviation of the eye position. 13 However, the conversion is not a linear relationship, which may lead to errors.
There are some limitations to the study. Firstly, the sample size of patients in the vertical strabismus group was too small to be used as a clinical conclusion and further studies are still needed. Second, this study did not ensure that all patients were in a state of refractive correction, which would affect the magnitude of strabismus in patients with intermittent exotropia and esotropia. Third, the clinical diagnosis of strabismus requires consideration of the patient's fusion function and accommodation ability, especially in patients with intermittent esotropia, and the patient's ability to independently control eye alignment, which is not reflected in the VR examination. The aim of this study was to investigate techniques that would allow mass screening for strabismus, and subsequent updates to the criteria for strabismus diagnosis are needed.
This article focuses on the clinical feasibility of a new technique for strabismus screening that incorporates virtual reality, and the results show good prospects. As strabismus is a common pediatric eye disease, we will update the artificial intelligence algorithms based on this study in the future and explore the accuracy of this technique in screening children for strabismus.
Conclusion
This study reports on new technology for strabismus screening combined with virtual reality that allows rapid qualitative diagnosis of strabismus type and quantification of ocular deviation angle. This technology provides feasibility for large-scale screening of children's eye diseases in China and aims to protect children's eye health. Although the accuracy of this technology has yet to reach its full potential, it holds promising prospects for further development.
Footnotes
Acknowledgments
We thank the Aqiyi Corporation for providing the Qiyu 2S headset.
Author contributions
JF contributed to study design and protocol draft. WWC contributed to study protocol draft. YMW contributed to research design, research execution, data manipulation, and manuscript preparation. MXJ and JWC contributed to data acquisition and research execution. All the authors reviewed the study protocol and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by Beijing Hospitals Authority Clinical Medicine Development of special funding support, code: XMLX202103.