
Abstract
Background
Virtual reality is a relatively new intervention that has the potential to be used in the treatment of eye and vision problems. This article reviews the use of virtual reality-related interventions in amblyopia, strabismus, and myopia research.
Methods
Sources covered in the review included 48 peer-reviewed research published between January 2000 and January 2023 from five electronic databases (ACM Digital Library, IEEE Xplore, PubMed, ScienceDirect and Web of Science). To prevent any missing relevant articles, the keywords, and terms used in the search included “VR”, “virtual reality”, “amblyopia”, “strabismus,” and “myopia”. Quality assessment and data extraction were performed independently by two authors to form a narrative synthesis to summarize findings from the included research.
Results
Total number of 48 references were reviewed. There were 31 studies published on amblyopia, 18 on strabismus, and 6 on myopia, with 7 studies overlapping amblyopia and strabismus. In terms of technology, smartphone-based virtual reality headset viewers were utilized more often in amblyopia research, but commercial standalone virtual reality headsets were used more frequently in myopia and strabismus-related research. The software and virtual environment were mostly developed based on vision therapy and dichoptic training paradigms.
Conclusion
It has been suggested that virtual reality technology offers a potentially effective tool for amblyopia, strabismus, and myopia studies. Nonetheless, a variety of factors, especially the virtual environment and systems employed in the data presented, must be explored before determining whether virtual reality can be effectively applied in clinical settings. This review is significant as the technology in virtual reality software and application design features have been investigated and considered for future reference.
Introduction
The prevalence rate of amblyopia, strabismus, and myopia has been reported to range from 1.75% to 4.3%,1,2 1.93% to 4.1%,3,4 and 11.7% to 22.9%, respectively.5,6 According to Huang et al., 7 it was found that the prevalence rate of strabismus in amblyopia subjects was 24%. Ocular conditions such as ocular misalignment (strabismus), uncorrected refractive errors including hyperopia, astigmatism, and myopia are of particular concern in children, because without timely detection and intervention, are at risk for developing amblyopia. 8 In general, the critical period during which a child's developmental period is most sensitive to abnormal visual inputs caused by visual deprivation, strabismus, or unequal refractive errors (anisometropia), puts the most vulnerable children in this susceptible group. 9 Therefore, this review has explored studies related to these common childhood ocular disorders.
Initial amblyopia therapy involves prescribing spectacles or contact lenses to optimize vision by correcting for significant refractive errors. Traditional occlusion therapy of the fellow fixating eye is a conventional treatment alongside vision correction. 10 Despite these approaches, there is still a high prevalence of amblyopia due to factors such as the limited availability of proper vision screening programs and/or poor patient compliance, especially for children while undergoing traditional treatment. 11 Therefore, commercialized products that address the aforementioned ocular morbidities offer a promising option for patients. In recent years, virtual reality (VR) technologies have been applied in optometry and ophthalmology where VR-based software programs have been developed to target certain ocular conditions. As mentioned by Coco-Martin et al., 12 VR provides a safe environment and may serve as an effective tool for certain visual target-based training paradigm. However, the potential for VR to supplement or even replace traditional therapies remains controversial. Thus, the advancement of VR technologies should be followed with a parallel critical review of the effectiveness of currently available VR-based applications related to strabismus, amblyopia, and myopia research.
VR is a virtual world in which all visual material and alternate feelings are produced solely by computers. Interactive and dynamic scenarios are provided to users while the physical performance alters the perception of the environmental status.
13
VR, given its true-to-life sense impressed in the virtual world, has been utilized in various research domains as a rather mature technology.
14
Various studies proved the promise of VR in clinical medicine, neuro-rehabilitation, and stroke-rehabilitation applications due to the availability of complex functions such as eye-tracking, haptic feedback, and flexible contents provided by the virtual environment (VE).14–18 Furthermore, multiple sensors to detect various functions of the human body including voice, body motion, heart rate have been used in conjunction with VR, making it possible to measure certain effects of VR on our physiological and neurological systems.19,20 It has been suggested that VR offers a potentially viable option for various ocular training and rehabilitation interventions.
12
The focus of this paper is to look through all available references in the scientific literature relating VR technology with strabismus, amblyopia, and myopia. Additionally, this study covers the following topics, while key research questions are discussed under the related works section.
How were the VR technologies embedded into the research methodology? What were the assessment methods used to evaluate the outcomes? What were the VE design elements and VR application contents considered to achieve the research objectives? What were the treatment and vision training theories employed to develop VR application design?
To date, there has been little review that focuses on VR technologies applied in ocular morbidities, especially in the field of amblyopia, strabismus, and myopia.12,15,21 This review examined how software contents were designed in the VE, which can provide additional insights for the creation of successful VR programs in this field. Moreover, the outcomes measures are vital factors to consider for evaluating the design and implementation of VR training programs that can be applied in the future VR software design for these related vision disorders.
Literature review
Treatment
Amblyopia
Amblyopia, also known as “lazy eye,” can result in certain complications such as abnormal visual information processing, 22 and permanent vision loss, if left untreated. In children, it has been reported that amblyopia prevalence ranges from 1.75% to 4.3%.1,5 Untreated ocular conditions such as congenital cataracts, unequal refractive errors, or strabismus may lead to a reduction of best-corrected visual acuity (BCVA) of the amblyopic eye. 22 The deprived visual experience of the “weaker eye” along with abnormal binocular experience whereby pictures experienced by the amblyopic and fellow sound eyes are mismatched throughout development, which may lead to permanent complications that are more than visual acuity loss alone. 16 Traditional amblyopia treatment involves occlusion therapy by patching the dominant eye or using atropine penalization while training the amblyopic eye.23,24 Although the exact neurophysiological mechanisms underlying amblyopia remains unclear, novel insights on perceptual learning (PL) and dichoptic training offer alternative options to restore certain functional deficiencies evident in the amblyopic system.25–28 The aim of both traditional and novel treatment options including optimizing vision, resolve suppression of the amblyopic eye, developing stereoacuity, and eventually restoring both the neurosensory, oculomotor, and visual concordance of the amblyopic system, to perceive clear, single binocular vision. 11
Strabismus
Strabismus is a vision disorder that may lead to amblyopia. It has a prevalence of 1.93%–4.1%.3,4 Previous reports have shown that strabismus is often perceived with physical biases that can potentially lead to negative self-esteem and interpersonal relationships, especially for young children. 29 The cause of strabismus can be idiopathic or congenital. Late onset may be caused by neurological issues such as stroke, traumatic brain injury, etc. 30 There are different forms of deviations. 3 For example, esotropia is the condition where one eye deviates inwards while exotropia refers to the condition where one eye deviates outwards with respect to the fellow fixating eye. Hypertropia refers to the vertical deviation where one eye deviates upward with respect to the fellow fixating eye. Certain cases of strabismus can be treated with refractive error correction alone while others will need vision therapy and/or surgical intervention depending on the severity of the oculomotor and neurosensory losses. 31 It has been previously reported that PL and/or dichoptic training led to some positive outcomes for strabismic patients concurrently being treated for amblyopia.27,32
Myopia
According to World Health Organization, 33 myopia, also known as “near-sightedness” is a common ocular condition that affects more than 2·6 billion people globally, with a prevalence rate of 11.7%–22.9%.2,6 It is estimated that the myopic population will reach over 3·3 billion by 2030. 6 Eye structures can affect the optical power of the eye include corneal curvature, lens power, and eyeball length. Eyeball elongation during childhood development is a common cause of myopia progression. 34 Proponents of high myopia studies have also noted thinning of the choroidal thickness in high myopes but whether myopia progression is affected by choroidal thinning remains unclear. 35 With normal vision, parallel rays from distant objects are focused on the photoreceptors of the retina, forming clear images. In myopic eyes, however, light rays are concentrated in front of the retina rather than on it. 36 This causes distant objects to appear blurry. Myopia can be corrected by spectacles, contact lens or refractive surgery. More recently, it has been shown that myopia progression may be controlled by specialty lens designs and ocular pharmacological agents such as atropine.37–40 Other indirect methods such as vision training to improve accommodative facility in order to reduce myopia have been proposed with inconclusive evidence. 41
Related works
Several papers have reviewed how VR technology has been applied in vision assessment and training. However, there are no review papers to date that have explored VR technology specifically addressing strabismus.
A review paper published by Rodán et al. 28 examined video game-based PL and dichoptic training for amblyopia. It was concluded that PL and dichoptic training can be effectively applied even without the use of video games as an active therapeutic component in the training process. Only two papers regarding VR has been mentioned in this systematic review. As a result, it remains inconclusive whether VR technology has great potential for amblyopia training based on the information reported. Furthermore, the review was limited to amblyopia only, and the conclusions may not be applicable to other ocular morbidities. Another paper by Coco-Martin et al. 12 also reviewed VR applications in amblyopia studies. The technology applied and eventual results were compared in the review. However, conclusions were still uncertained whether VR can serve as a useful tool in amblyopia studies. Zhao et al. 15 proposed a few factors to consider with respect to VR and myopia studies. It was postulated that VR technology can be applied to accommodation training. While this review did not provide a detailed summary of how VR technologies were applied to control and prevent myopia, a more updated and comprehensive review on this topic is needed. Another review about VR has summarized possible usage of VR in strabismus and amblyopia studies, ocular disease diagnosis and treatment, as well as in surgical procedures. 42 The Interactive Binocular Treatment (I-BiT) system, which is VR-based, was used in the training protocol. Table 1 summarizes the aspects covered in the reviews.
Summary of reviews on VR technologies in amblyopia, strabismus, and myopia.

PL: perceptual learning; VR: virtual reality.
The aforementioned reviews have focused on possibilities of VR applications in ophthalmic diagnosis, simulation, and surgical guidelines, etc. A comprehensive systematic review of using VR for strabismus, amblyopia, and myopia studies is lacking. As such, the following research questions were addressed under this review (Table 2).
Research questions of this study.

VR: virtual reality; RQ: research question.
Methods
Search strategy and selection criteria
A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was used in this review to identify, select, and examine relevant references with minimum prejudice. 43 The review protocol was registered in the International Prospective Register for Systematic Reviews (PROSPERO) with the registration number CRD42022309851. The digital database Web of Science, IEEE Xplore Digital Library, and ScienceDirect were used to search for related studies from 1 January 2000 up to 1 January 2023. The Boolean operators “AND” and “OR” were used to create a search strategy that was applied to the subject heading, title, and abstract fields. To prevent any missing relevant articles, the keywords and terms used in the search included “VR”, “virtual reality”, “amblyopia”, “strabismus” and “myopia”.
For database searching, the search string was defined for each database as shown in Table 3.
Search strings.

A brief filter was applied in the search string in digital database as mentioned in Table 3. After downloading all references, the reference management software Endnote was utilized for organization and management of data. Then, manual filters were used to identify potential papers. Prospective references downloaded from the database were identified and classified manually. The search was confined exclusively to publications published in peer-reviewed journals and conferences, whereas book chapters and reviewer papers were excluded from consideration. In addition, all articles not written in English were excluded. References with the presentation of any of the exclusion criteria: treatment or training without using VR technologies, use of eyedrops or other medications, and presence of eye surgery were ruled out. Subsequently, each study was screened, extracted, and analyzed. Figures and tables are used in the following sections to convey the findings in a visual format.
Quality assessment
Eligible references were critically appraised using the standardized instruments for critical appraisal, risk of bias (RoB). In Non-randomized Studies - of Interventions (ROBINS-I), by Sterne et al. 44 When designing a thorough research design including healthcare treatments, this tool was created to evaluate the RoB. This increased the amount of knowledge gained into the methodological strengths and flaws of chosen research to the greatest extent possible. Each study was marked and analyzed manually by two members from the research team using the ROBINS-I checklist. Overall, the quality of the references was categorized as low, moderate, serious, critical RoB, and no information according to ROBINS-I. If there was discrepancy, the paper was cross-checked until agreement was obtained. Following the conclusion of the ROBINS-I quality assessment procedure, eligible articles were subjected to further screening before being subjected to the data extraction process.
Data extraction
After screening all eligible studies, a standardized article data extraction method was employed to review the study characteristics of each publication. Characteristics such as research objective, sample size, mean age, outcomes, VR device or systems, intervention type, and VR design elements were extracted and are presented in later sections. Statistical data were visualized and organized using Microsoft Excel. Further information about the relationships among objectives, VR intervention, and VR design elements was evaluated. The homogeneity of the papers included in this systematic review was determined in order to establish the feasibility of subgrouping and meta-analysis within it. For data subgrouping, characteristics were extracted according to RQs. Despite this, no meta-analysis was available due to the significant level of heterogeneity in this article. Since not all studies included control experimental groups and measurable outcomes, conducting a meta-analysis to compare the retrieved data is challenging. Hence, quantitative analysis was used in this review for heterogeneous papers with distinct VR intervention, research objectives, outcomes, and experimental design.
Data synthesis
The findings from the included publications were combined using descriptive analysis to form a narrative synthesis. Regardless of the estimated RoB, the results of each included research are presented. Comparison tables focusing on research objectives, sample size, mean age, study design, outcomes, VR device or systems, intervention type, and VR design elements are presented in Tables 4 and 5. Relationships between research objectives, experimental design, and VR intervention design are presented as a bubble chart shown in Figures 1, 2, and 3.

Relationship between level of immersion and virtual reality (VR) intervention type.

Relationship between research objectives, level of immersion, and type of virtual reality (VR) intervention.
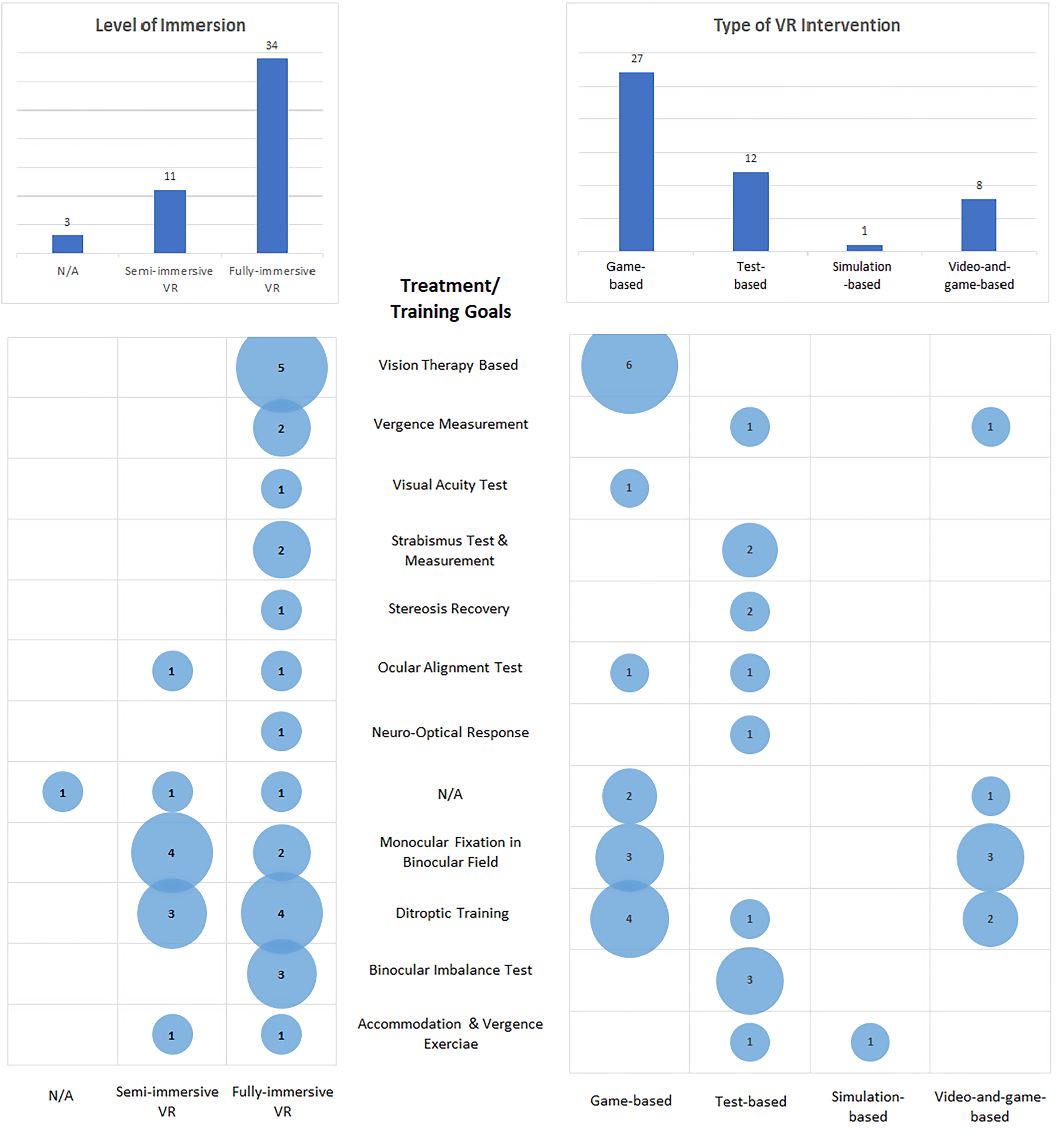
Relationship between treatment or training goals, level of immersion, and type of virtual reality (VR) intervention.
Summary of experimental details, objective, and outcomes of selected.

BCVA: best-corrected visual acuity; VR: virtual reality; CI: convergence insufficiency; PEP: perceptual eye position; DMR: Double Maddox rod; VE: virtual environmentl; VA: visual acuity; IXT: intermittent exotropia; APCT: alternate prism cover test; I-BiT: Interactive Binocular Treatment; HMD: head-mounted display.
Summary of VE design, embedded theory, and VR intervention of selected articles.

VR: virtual reality; VE: virtual environment; MFBF: monocular fixation in binocular field; PEP: perceptual eye position; APCT: alternate prism cover test.
Results
Overview of results
The PRISMA flowchart summarizing the review process is shown in Figure 4. The initial search strategy identified 610 references including duplicates from five electronic databases (ACM Digital Library, IEEE Xplore, PubMed, ScienceDirect and Web of Science). After 100 duplicates were removed, 510 references were further assessed. After reviewing the titles and abstracts, 6 references were excluded because of non-English publication and incomplete citations. The remaining 440 articles were downloaded and one of them was not retrieved. A total of 439 references were reviewed and analyzed with 391 papers excluded as the topics, treatment methodologies, book chapters, and keywords were unrelated to this review. The resultant 48 references were considered relevant with their full texts analyzed.

PRISMA flowchart of reference selection.
The review included references from 20 different countries. Figure 5 depicts the distribution of selected papers. The majority of the research was from the United Kingdom (9/48, 18.75%) and the United States (7/48, 14.58%). There were 5 references each from China and 4 from South Korea, accounting for 10.42% and 8.33% of publications respectively. In general, most publications were from Western countries, followed by Asian countries.

Country of origin.
As shown in Figure 6, the publication year concentrated within the recent 7 years with 85.42% (41/48) of them published in 2016 or later. 7 were published before 2010 and there was only 1 reference published in 2007, 2012, and 2013.

Year of publication.
The references were chosen from 15 topics as shown in Figure 7 in terms of the subject matter of the journals. Ophthalmology covered 20 publications, accounting for 41.67% of the total number of articles. A total of 8 studies were conducted in the field of Computer Science and Engineering, accounting for 16.67%. Another 41.66% were from Optometry, Medical, Industrial Electronics, Engineering, Computing and Communication Technologies, Cognitive Infocommunications, Biological Science, Bioinformatics and Biomedical Engineering, Applied Psychology, and Applied Ergonomics, among others.

Subject area of journal.
The selected papers were organized into three categories: strabismus (n = 19), amblyopia (n = 30), and myopia (n = 6), with 7 studies overlapping amblyopia and strabismus. As for the VR intervention method, it was categorized into game-based, test-based, simulation-based, and video-and-game-based. A summary of selected reference specific to ocular morbidity with their VR intervention methods is shown in Table 6.
References according to amblyopia, strabismus, and myopia with virtual reality (VR) intervention method.

Research objectives (RQ1: what were the research objectives regarding VR for strabismus, amblyopia, and myopia studies?)
Most research objectives were to create novel applications (20/48, 41.67%) and study the effectiveness of VR applications to improve the aforementioned visual disorders (14/48, 29.17%). Another unifying goal was to develop measurement tools (8/48, 16.67%) for amblyopia, strabismus, or myopia. The I-BiT system has been a commonly applied VR tool in strabismus and amblyopia research, with its effectiveness as a training system evaluated in 6/48 (12.50%) papers reviewed (Figure 8).

Research objectives of selected references.
Several researchers aimed to develop new VR applications and systems for amblyopia, strabismus, and myopia studies. Applications were either re-designed, deploying existing VR products, or new systems were created afresh including the Viston-VRTM system, 85 NeuroDotVR, 70 and a VR-based experimental protype. 91 Novel applications to measure myopia and ocular deviation were proposed by Nesaratnam et al., 75 Maiello et al., 81 Mehringer et al., 78 Miao et al., 76 and Yeh et al. 77 The traditional methodology was re-designed and applied in VR, where promising results were reported. Studies by Eastgate et al., 83 Waddingham et al., 84 Cleary et al., 86 Herbison et al., 87 Herbison et al., 88 and Rajavi et al. 49 used existing systems such as the I-BiT system with new applications developed and deployed to study its compatibility with the I-BiT system.
Among the 20 papers with major objectives regarding investigation of the effectiveness of I-BiT system and VR, the results were analyzed and presented in Table 7 and 8, respectively.
Effectiveness of Interactive Binocular Treatment (I-BiT) system.

Effectiveness of VR.

BCVA: best-corrected visual acuity; VR: virtual reality; HMD: head-mounted display.
VR technologies were utilized in various studies involving amblyopia, strabismus, and myopia. I-BiT system was used in the treatment of amblyopia and strabismus. It has been shown to be an effective therapy for amblyopia and strabismus (Table 7). Other than I-BiT system, positive effects of VR was recorded in treatment of amblyopia, strabismus, and myopia.13,65–67,82 The binocular status of some patients showed moderate improvement following VR therapy for myopia,13,65–67,82 but the effectiveness still needs to be investigated further as there were reports of mild to no effect of VR in myopia treatment.13,65–67,82,83
Assessment methods and measurements (RQ2: what were the assessment methods used to evaluate outcomes?)
Research relating to amblyopia, strabismus, and myopia have recognized protocols and outcomes measures. After analyzation and examination of all references, major experimental outcomes were extracted. The efficacy of VR treatment and training was revealed. While not all selected papers reviewed have followed standard protocols, the experimental design, objectives, and relevant outcomes are summarized in Table 4.
VR-based applications and headsets have been developed to offer a new method in treating patients with amblyopia. Performance ease of participants has shown that the headsets achieved acceptable compliance when used as a training tool.46,47,56,58,71 As reported by Waddingham et al., 84 Cleary et al., 86 Herbison et al., 87 Herbison et al., 88 Vedamurthy et al., 45 Hurd et al., 53 Halička et al., 55 Jhangian et al., 58 Tan et al., 60 and Xiao et al., 89 VA outcomes have shown comparable improvements through training using VR applications. Likewise, Rajavi et al., 49 Žiak et al., 16 Elhusseiny et al., 69 and Rajavi et al. 50 have also made VA improvements, which reflected a promising application value for further research on this topic. Research regarding VR and observed changes in accommodative status and ocular structures have been reported by Turnbull & Phillips, 82 Elias et al., 13 Munsamy et al., 66 Yoon et al., 67 and Panfili et al. 65 According to Turnbull & Phillips, 82 after a brief duration of VR usage, there was a considerable change in choroidal thickness. Elias et al. 13 reported some related changes as a result of exposure to the VR environment, inducing changes in accommodative and convergence systems. Munsamy et al. 66 assured that binocular accommodative and vergence facilities increased after 25 min of VR usage. Yet, there were insignificant reports of VA worsening as a result of VR exposure. 65 Several game-based treatment methods45–48,61,62,64,84,90 and virtual ocular testing applications68,74 were applied in various strabismus studies. The reported results showed a positive potential for implementing novel systems and applications in treating strabismus, which was reflected by some improvement in deviation magnitude74,75,77,90 and VA.45,69 Kim & Oh proposed new applications for strabismus training but there were no data on its efficacy, which warrants further investigation 62 while reported by Tan et al. 79 and Bindiganavale et al., 80 positive results were shown in strabismus treatment using VR interventions.
Most studies relied on the logarithm of the minimum angle of resolution (logMAR) VA improvement as amblyopia outcomes measures.45,53,84–88 The optimum goals in treating amblyopia are to improve VA, restore neurosensory and oculomotor visual functions such as anti-suppression, 73 oculomotor, accommodative and vergence training. 92 Further VR designs should focus on these outcome measures such as improvement in contrast sensitivity, stereopsis, accommodation, and suppression in addition to solely logMAR VA comparisons. Strabismus is the condition of misalignment of eye sight. From the systematic review, it was noted that stereoacuity and degree of strabismus were mostly reported as the outcomes measure for strabismus studies.45,48,68,74,75,77,90 These parameters should be considered in future VR experimental designs. Whether the VR viewing environment is a negative or positive drive to myopia progression remains unclear. As such, changes in factors such as axial length, cycloplegic refractive error, choroidal thickness should be closely monitored.13,65,82,93,94
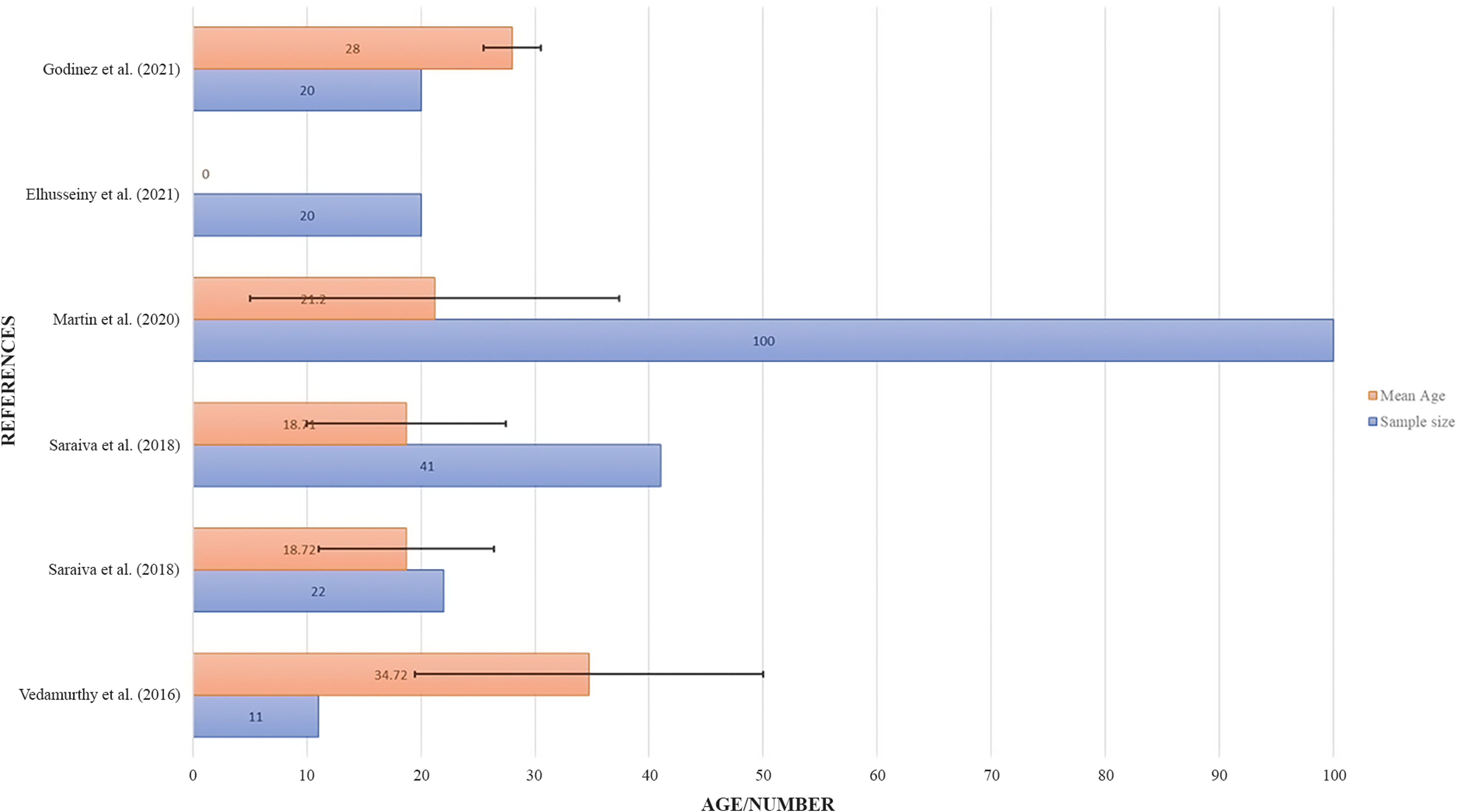
The sample size and age of the experimental groups varied in different amblyopia, strabismus, mixed (strabismus and amblyopia), and myopia studies. Their demographics summaries are presented in Figures 9, 10, 11, and 12 respectively. There were no obvious patterns in the number of participants. For the mean age, only adults above 18-year old were included in the myopia group and combination of amblyopia and strabismus group. There were seven research studies that reported participants under the age of ten for amblyopia references. The strabismus group, with a mean age of over 45 years old, were the oldest. It reflected that current amblyopia-based VR treatment are more often offered for children. While for myopia, strabismus, and combination of amblyopia and strabismus, VR-related research was limited to adult subjects only.

Sample size and mean age of experimental groups in amblyopia references.

Sample size and mean age of experimental groups in strabismus references.

Sample size and mean age of experimental groups in myopia references.
Sample size and mean age of experimental groups using Interactive Binocular Treatment (I-BiT) TM system.
Compared to other methods, the target age group in treatment using the I-BiT™ system were mainly young subjects with a mean age below nine years old (Figure 13). Based on the number of studies included the I-BiT™ system have shown a strong acceptance potential for the pediatric age group.
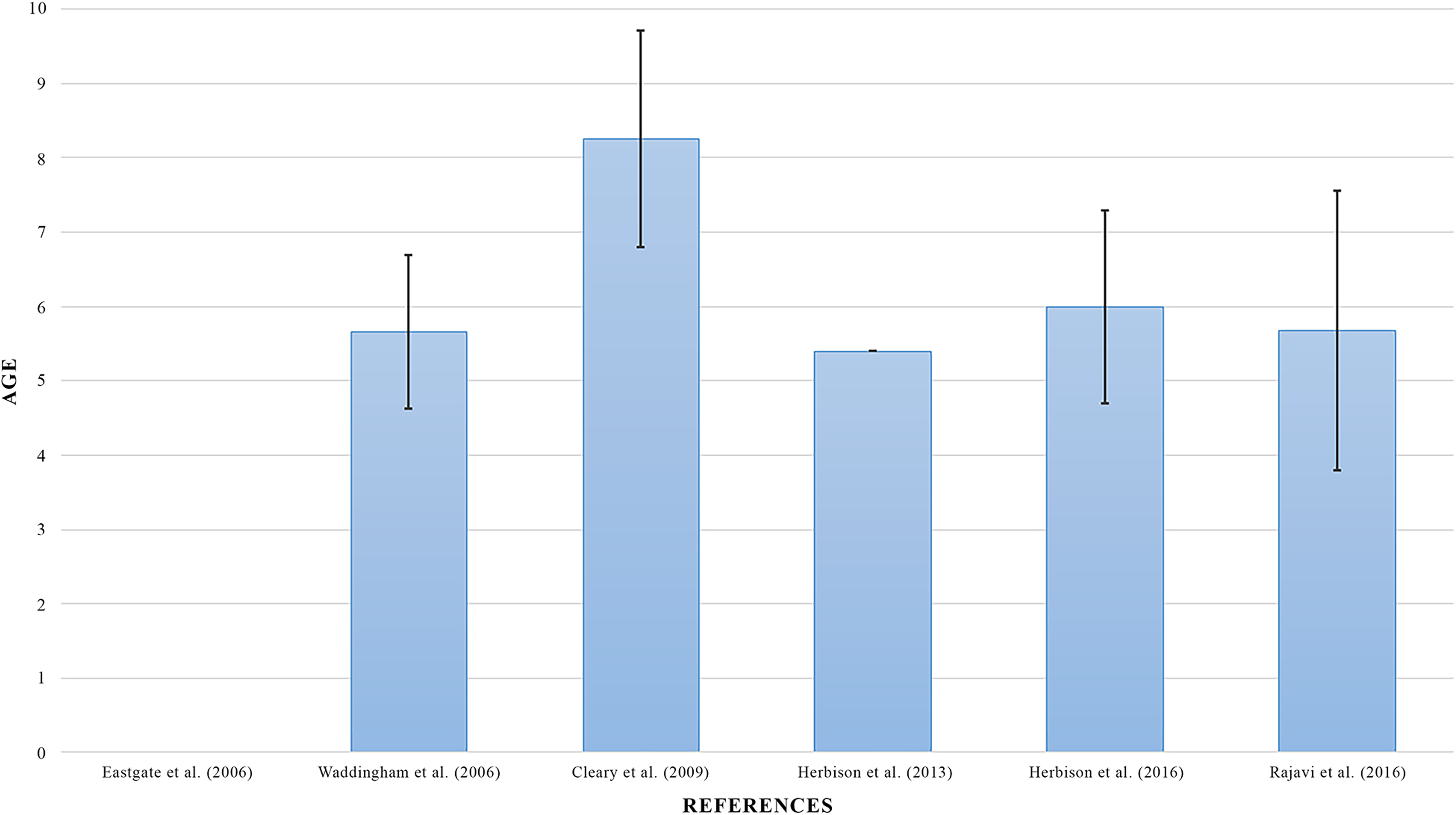
Mean age of experiment subjects in treatment using Interactive Binocular Treatment (I-BiT) TM system.
As for study design, majority (22/48, 45.83%) of the reference were experimenting on uncontrolled groups of experiment subjects. Only in 17/48 (35.42%) clinical findings were obtained with controlled, randomized, double masked, and/ or cross-in method. This made meta-analysis impossible in this for the experiments with distinct experimental design and VR systems (Figure 14).

Study design if the references.
Type of VR technologies (RQ3: what were the types of VR technologies used to achieve the research objectives?)
Different types of VR headset and technologies were used by researchers (Figure 15). Among total references, the majority (16/48, 33.33%) used commercial standalone VR headset in their studies due to specific functions provided by the headsets. Oculus Rift was used by Nesaratnam et al., 75 Turnbull & Phillips, 82 Žiak et al., 16 Halička et al., 55 Jiménez-Rodríguez et al., 56 Jhangian et al., 58 and Godinez et al. 80 This kind of headset provided VR experience without considering space constraints as the headset was a wireless type. HTC Vive was used by Hurd et al., 53 Martín et al., 68 Mehringer et al., 78 Lin & Chou 57 and Panfili et al., 65 while HTC Vive Pro Eye was used by Yeh et al. 77 Although the HTC Vive series headsets were wire-connected, they provided high-resolution images while eye tracking functions were found with the Pro Eye model. FOVE was used by Esfahlani et al., 52 Miao et al., 76 and Chung et al. 90 It provided eye tracking functions with a wireless google. Meanwhile, development of smartphone applications with VR viewers were common approaches, and were also used in 16 research studies (16/48, 33.33%). Google Cardboard was used by Vichitvejpaisal & Chotine, 51 and the research team of Saraiva,46,47 while VR viewers from Samsung, Shinecon, Oculus, and Zeiss were used in several other research studies.13,50,59,60,62,63,66,67,69,71,72,80,89 I- BiT™ system was frequently used (6/48, 12.50%) in the treatment of amblyopia and strabismus. Eastgate et al., 83 Waddingham et al., 84 Cleary et al., 86 Herbison et al., 87 Herbison et al., 88 and Rajavi et al. 49 employed I-BiT™ system in amblyopic and strabismic therapy and found the approach effective in the treatment.

Types of VR Headset and Technologies.
In addition, three novel systems (2/48, 4.17%), including the Viston-VRTM system, 47 and NeuroDotVR system 70 were developed to treat myopia, amblyopia, and strabismus, while 3D display screens together with 3D polarized glasses were used (5/48, 10.42%) in a few studies.45,51,61–63,72,74,79,81 Furthermore, Cepeda-Zapata et al. 64 did not mention the device or system used in the research in which a VR game theory was proposed by Tan et al. 54
Design elements (RQ4: what were the design elements included in VR applications?)
As numerous VR headset were utilized, distinct VE and functions were designed based on major goals of the study. The VR applications were categorized into four types, including game-based, video-and-game-based, test-based, and simulation-based. Game-based design focused on playing a VR game for treatment, while video-and-game-based design was the treatment of video clip viewing followed by VR game play. Test-based applications were designated for measurement of the ocular status of specific ocular morbidities. Last but not least, the simulation-based program was a facsimile VE of the actual environment. In addition, stereoscopic visualization is provided in VR and interaction of virtual objects and environment, with haptic feedback are available. 95 Further categorizing VR systems, there are fully immersive VR systems, semi-immersive VR systems, and non-immersive VR. Bamodu and Ye defined type of VR by their features. 96 With head-mounted displays (HMD) and tracking sensors, fully immersive VR achieves the maximum degree of immersion. Semi-immersive VR achieves a high degree of immersion while being technologically basic. The immersion level for non-immersive VR is the lowest with simple system monitor or TV systems.
To in cooperate the VR design elements, training or treatment targets should be addressed. Common treatment targets included monocular fixation in binocular field (MFBF), Ocular alignment test, dichoptic training, VA test, vision therapy based treatment, and vergence and accommodation exercises. MFBF was first introduced in 1981, which calls for both eyes to be open at the same time. Thus, the work done is in a binocular field. 97 And as is described in a recent study, both eyes are shown the cursor but only the amblyopic eye is shown the target. Thus, the amblyopic eye must guide the eyes to the target, a process called supervised PL. 98 However, in the dichoptic training, the image shown to the amblyopic eye should be of a higher contrast than the fellow eye, but with the same content. 99 Most differently, vision therapy-based training only provides a single stimulation to only one or both eyes of the patient simultaneously.
Summarized information regarding VE design, embedded theories, treatment targets and VR intervention of selected articles is presented in Table 5.
With a fully immersive VR system, game-based design was used in most studies while shooting games were commonly programed in the VR game design (20/48, 41.67%). Žiak et al., 16 Elias et al., 13 Esfahlani et al., 52 Hurd et al., 53 Kim and Oh, 62 Godinez et al., 48 Halička et al., 55 Khaleghi et al., 59 and Rajavi et al. 50 developed VR shooting games with different scenarios for amblyopia, strabismus, and myopia studies. Other non-shooting games for amblyopia included photo hunt games, 51 escape room games, 63 response games,71,72 and matching games.58,65 The VE design varied from each other. Most treatment paradigm incorporated basic vision therapy MFBF concept or dichoptic viewing in the program design. A few studies included simulation (1/48, 2.01%) and tests (14/48, 29.17%) as the application content. Saraiva et al. 46 developed VR software to encourage sensory and motor eye muscle controls for amblyopic patients. VR simulation of indoor and outdoor scenes was developed by Turnbull and Phillips for myopia studies. 82 Furthermore, some tests were designed for amblyopia and strabismus as assessment and training.68,69,75–78 They include deviation assessment, dichoptic nonius target alignment, with an alternate prism cover test (APCT) redesigned in VR context. The results were tabulated and can be used in assisting further clinical diagnosis.
Semi-immersive VR systems with 3D stereo viewers were used in several studies. A system with crystal Eyes shutter goggles, CyberDome1400, and a system with polarized 3D monitor and 3D polarized glasses were employed by Handa et al., 61 Vedamurthy et al., 45 and Li et al. 74 respectively for treatment. These semi-immersive VR systems offer a promising tool for future amblyopia and strabismus studies. The video-and-game-based method mainly utilized the I-BiT™ system. A total of seven studies among all (8/48, 16.67%) used video-and-game-based experiments, and five of those were application of the I-BiT™ system. Eastgate et al., 83 Waddingham et al., 84 Cleary et al., 86 Herbison et al., 87 and Herbison et al. 88 designed treatments with a video-watching part followed by interactive gaming part with I-BiT™ system. Rajavi et al. 49 proposed experiments using videos or games only with I-BiT™ system. Several videos and games were available in the treatment and basic strategy was similar with other studies in which cooperation with both eyes are needed. The results by Herbison et al. 88 showed that there was a modest VA improvement after the experiment among all groups. BCVA of the amblyopic eye improved significantly offering a promising value of the I-BiT™ system for amblyopia therapy. 49
In addition, only a few research studies developed new systems/games for treating eye conditions. The Viston-VRTM and NeuroDotVR systems were developed by Qiu et al. 85 and Versek et al. 70 respectively for amblyopia studies. The Viston-VRTM system presented interactive videos and games in a VE. On the other hand, the NeuroDotVR system aimed to collect EEG signals by presenting alternating light and dark square stimuli in a VE in order to analyze brain activities for assessment. Tan et al. 54 initiated a game theory that involves hardware and software feedback by analyzing eye tracking and biometric data to adjust the VR game difficulty according to the participant competency level during VR therapy.
Figure 1 shows a bubble chart that describes how level of immersion and VR intervention types were used in the research. Fully immersive VR was commonly used in 34 studies (70.83%) while game-based intervention was deployed in most of the studies (25/48, 52.08%). It can be concluded that game-based fully immersive VR was utilized in most of the studies in the design of VR headsets for amblyopia, strabismus and myopia studies.
Treatment and training goals (RQ5: what were the underlying theories embedded in VR interventions?)
The VR interventions were designed according to several training goals (Figure 16).

Treatment or Training Goals Using VR Interventions.
For amblyopia and strabismus treatment, the majority of the VR games design were based on MFBF (11/48, 22.91%), followed by dichoptic training theory (10/48, 20.83%) and vision therapy-based training (7/48, 14.58%). Under these kinds of training, different images were presented to each eye in the VR headsets, the dominant eye and amblyopic eye. 45 Some of the treatments were designed with fixed background objects presented to the dominant eye, while the amblyopic eye follows a dynamic target. Under this training, both eyes were forced to cooperate with each other in order to properly align the target and background. For several measurement and test-based VR applications,68,75–78 binocular imbalance test (3/48, 6.25%), vergence measurement (2/48, 4.17%), ocular alignment test (2/48, 4.17%), strabismus test and measure (3/4, 6.25%), and stereopsis recovery (1/48, 2.08%) were applied.
For myopia studies related to VR, accommodation and vergence responses were measured (4/48, 8.33%). The accommodative-Convergence to Accommodation (AC/A) ratio was also recorded in the process.13,81,82 VA testing was adopted in other research studies (1/48, 1.25%), in which VA was measured during the tasks. 65
Relationship between research objectives and design elements (RQ6: what were the relationships between research objectives and design elements of VR applications?)
Level of immersion and type of VR intervention are used to study how the research objectives were achieved in selected references (Figure 2).
Concerning the research objective and design elements of the selected 48 articles, fully immersive VR was most popular in 34 articles (70.83%) while semi-immersive VR was used in 12 articles (25.00%). Game-based intervention was used in 27 articles (56.25%), followed by test-based intervention (12/48, 25.00%) and video-and-game-based intervention (8/48, 16.67%). As presented in Figure 2, the relationship between research objective, level of immersion, and type of VR intervention can be investigated. It is noticed that in order to achieve the objective of the development of new systems among a total number of 19 articles, fully immersive VR (17/19, 89.47%) and game-based intervention (14/19, 73.68%) were commonly used. To investigate the effectiveness of I-BiT system in six articles, semi-immersive VR was used by all researchers, and video-and-game-based intervention was used in all of the articles. Among eight articles regarding the objective of development of measurement tools, the majority used fully immersive VR (5/8, 62.5%) and test-based intervention (6/8, 75%) in their research. To achieve the objective of investigation of the effectiveness of VR in 14 articles, fully immersive VR (12/14, 85.71%) and game-based intervention (11/14, 78.57%) were generally used.
It can be observed that apart from the I-BiT system, fully immersive VR was used to achieve all other objectives. On the other hand, game-based intervention was used in the majority of the new systems. Test-based intervention was applied in measurement tools while video-and-game-based intervention was mainly used with I-BiT system.
Relationship between design elements and goals (RQ7: what were the relationships between VR intervention design elements and theories employed?)
With the intention of investigate how VR application and systems were designed in treatment and vision training of amblyopia, myopia, and strabismus, the relationship between design element and treatment or training goals was analyzed.
As presented in Figure 3, studies regarding amblyopia are dominant, and the treatment and training method related to amblyopia was the most popular among all studies. Fully immersive (six articles) vision therapy-based training games (five articles) were commonly utilized, as well as fully immersive dichoptic training (six articles) games (five articles). For strabismus test and measurement, fully immersive test-based intervention was applied by researchers in three articles. The VR test design was based on conventional theory of the strabismus test and measurement methods. While for myopia, the accommodation and vergence exercise and visual acuity test were used as the basic of VR application design. Among the six references, different design elements were considered. Fully immersive VR was used in four studies while semi-immersive VR was used in two articles. Game-based intervention was developed by two research groups while test-based and simulation-based interventions were deployed in one study each.
Discussion
This systematic review is the first to specifically focus on evaluating how VR technologies were utilized regarding treatment and vision training of amblyopia, strabismus, and myopia. An increasing trend using VR technologies in the ophthalmology/optometry field have been observed in recent years. To understand how VR has been implemented and their contribution to the ocular field, this systematic review provided a qualitative analysis of available information on the experiment details including experimental targets with their age, objective of the study, major outcomes of the study, VR device or system used, and how VE was designed and set up. While the objective of this review was to investigate how VR technologies were employed in amblyopia, strabismus, and myopia, detailed assessment of the references was separated based on the research questions in the previous section.
Despite the necessity for a practical research objective, additional components such as design elements, VR intervention, and embedded theories must be considered when proposing a new VR application or system for treatment and vision training of amblyopia, myopia, and strabismus. From the results obtained after analyzation of the selected articles, fully-immersive game-based VR was the most popular. Commercial standalone VR headset and smartphone Apps with VR viewers were common experiment equipment. To treat or train amblyopia and strabismus, VR applications could be designed following the rule of dichoptic training, vision therapy-based training, and/or monocular fixation in the binocular field. Whereas for treatment or training of myopia, theories of accommodation and vergence exercise can be considered. There was no optimal age range or obvious age limits for the treatment or training. Yet, from the selected studies, there are no concrete conclusions on whether VR is an effective tool in the treatment and vision training of amblyopia, myopia, and strabismus. Several studies have proven the potential of VR in the field, while further experiments are needed to recognize the importance of VR in ocular treatment and training.
In spite of the development of new VR applications and systems in a number of research studies, the effectiveness of VR in the treatment and training of amblyopia, strabismus, and myopia remains unknown. Research studies regarding myopia is limited. The effectiveness cannot be addressed by reviewing the papers with only vergence and accommodation as the major research focus. For amblyopia and strabismus, I-BiT system and VR treatment have existed for several years, the potential effectiveness of them were addressed with limitation of specification of VR systems. It is concluded by Lynn e al. (2020) 100 that average resolution of some VR goggles is only 0.55 logMAR. Some of the VR devices are incapable of providing high-quality images for logMAR improvement, leading to little effects of VR in treatment of amblyopia. While for strabismus, mean field of view of some headsets was 67.1 ± 18 degrees (Lynn et al., 2020), which may not provide sufficient room for vergence training. 100 Although VR technologies are still under rapid development, there are hardware restrictions that limit the effectiveness of amblyopia and strabismus treatments.
Implications
This systematic review focused on the design and implementation of VR in the treatment and training of the aforementioned ocular morbidities, but other reviews have looked into the conventional treatment method of a sole disorder.12,15,28,42 Due to the fact that a systematic review of VR used in treatment and training of ocular morbidity was lacking, this paper serves as a foundation for future researchers to understand how VR was utilized in the treatment and training of amblyopia, myopia, and strabismus. To utilize VR in this field, it is crucial to evaluate the cost, convenience, and feasibility of VR equipment and intervention design. As VR device or systems, VR experiment design, and design elements of VE were concluded in this review, references can be taken from this review in future experiments.
One strength of this paper was the extensive search strategy including three digital databases and searching other reviews on the same topic that met the required criteria. As VR was the main focus of the study, other treatment and training methods were excluded. The increased importance of VR with the advancement of technologies, a trend of using VR to treatment or training in ophthalmology/optometry field was observed. 12 From this systematic review, an increasing number of papers was published regarding the treatment and vision training of amblyopia, myopia, and strabismus. While previous papers regarding VR were included in this paper, there are hopes for a breakthrough in further experimentation or investigation on VR technology.
Recommendations
This review emphasizes the importance of high-quality randomized clinical trials in VR in this discipline. With corresponding experimental groups and results, meta-analysis can be carried out for further comparison. It is recommended that researchers can evaluate the dosage of VR exposure compared to other treatment and training methods, including spectacles wearing, dichoptic training, and usage of eyedrops, in the long term. Moreover, the adverse effects of VR in ocular fields should be investigated in advance so that the experiment design can be optimized to achieve maximum treatment or training effects.
In addition, a standard definition of VR-related terms and VR intervention is still lacking. For instance, the level of immersion was defined by Bamodu and Ye according to their features. 96 Fully immersive VR achieves the maximum degree of immersion with HMD and tracking sensors, and semi-immersive gives a high level of immersion while using a simple technology. However, most of the studies did not define the level of immersion in their research. Immersive level can be defined only with the VR device or system used in the experiment. The level of immersive is closely related to the quality of the VR experiment. 101 It is important to consider which type of VR headset and intervention to be used when designing a new system for treatment and vison training of amblyopia, myopia, and strabismus.
One additional recommendation is the standardization of the definitions in the effects and progress of treatment and vision training of the specific ocular morbidity. Presently, multiple parameters were considered as the binocular status. For the assessment of ocular morbidity, several variables are taken into account. In this systematic review, several research studies consider VA improvement as an indicator of effectiveness in amblyopia treatment; whereas others may also include stereoacuity as an index. For myopia, VA, accommodation response, and choroidal thickness were considered by separate researchers. On the other hand, there was no standard in training duration defined making it difficult to compare the outcomes across different experiments.
Limitations and future work
Some limitations of this review were addressed. Firstly, only publications in English were considered, eliminating eligible results in other languages. In addition, the quality assessment of included references suggested a high risk of biased results from the experiments. Some of them were randomized trials, some were controlled studies and some were pilot studies. Some included studies agreed that VR was effective in treating amblyopia, myopia, and strabismus from experimental results while some just proved the results by user experiment questionnaire. The sample size of the references varied from the tens to the hundreds, making the results less united and it is hard to draw a concrete conclusion. Moreover, the type of VR technology was not specified in this review. Effect of non-immersive may provide a distinct result and usability compared to immersive VR. The varied nature of the VR headsets and systems used across these studies made the analysis incomparable.
Due to heterogeneity, it is not possible to perform meta-analysis for the experiments with distinct designs and VR systems. Since the focus of this paper is to review VR application in treatment and vision training of amblyopia, myopia, and strabismus, the efficacy and effectiveness of VR were not determined. In the future, it is expected that the effectiveness of VR in the same field can be concluded by meta-analysis. With comparable results, the software content and VE elements can be referenced in designing applications for treatment and vision training of amblyopia, myopia, and strabismus.
Conclusions
This review paper examined the use of VR in amblyopia, strabismus, and myopia studies. A total of 48 references were included and analyzed of which 31, 18, and 6 of them were related to amblyopia, strabismus, and myopia respectively. The main objectives of the references included the development of a novel VR application or system for treatment and to investigate their effectiveness. Based on major outcomes of the studies, VR may serve as a promising tool for amblyopia and strabismus treatment. In addition, myopia studies related to the use of VR warrants room for further investigation. Regarding technologies used in the references, smartphones with VR headset viewers were most commonly used in amblyopic studies while commercial standalone VR headsets were utilized most frequently in strabismus and myopia studies. Software and VE design were based on vision therapy based training and dichoptic training. Binocular vision was rebalanced after therapy treatments for amblyopia, myopia and strabismus.
This study provides the basis for future research so as to evaluate how VR technologies can be applied in the aforementioned ocular morbidities using the standardized PRISMA method. Exemplifications of VR systems acquired from diverse sources might give insights for future VE content creation and development. According to the quality evaluation completed as a consequence of this review, there is inadequate information regarding the experimental outcomes of VR's efficiency in the treatment and ocular rehabilitation of ocular morbidity. Future research should focus on the VR technology used in the treatment and ocular rehabilitation of strabismus, amblyopia, and myopia. Last but not least, clinical experiments should be conducted to test the efficacy of VR as a therapeutic tool.
Footnotes
Acknowledgements
The authors would like to acknowledge the support from the Department of Industrial and Systems Engineering and the School of Optometry, The Hong Kong Polytechnic University for this research.
Contributorship
The authors confirm contribution to the paper as follows: Study conception and design were handled by Yuk Ming Tang and Chi Wai Do; data collection was done by Hoi Sze Chan, Horace Wong and Lily YL Chan; analysis and interpretation of results were done by Hoi Sze Chan, Yuk Ming Tang, Chi Wai Do, Horace Wong, and Lily YL Chan; draft manuscript preparation was done by Hoi Sze Chan, Yuk Ming Tang, Chi Wai Do, Horace Wong, Lily YL Chan and Suet To. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is supported the Department of Industrial and Systems Engineering, and this project is funded by the PPK Holdings Limited and the Innovation and Technology Fund (ITF) of the Hong Kong Special Administrative Region, China (Project Ref.: PRP/071/20FX), for the research, authorship and/or publication of this article.
Ethical approval
Research ethics approval and participant consent are not required to collect data from publicly available information (i.e., this systematic review).
Guarantor
Y.M. Tang.