
Abstract
Objective
The widespread penetration of the internet and digital technology have profoundly impacted the global economy and people's lives. Although the impact of digital skills on social development and personal lifestyles is well-documented, their influence on health and health inequalities remains underexplored. This study aims to analyze the impact of digital skills on health and health inequalities and to investigate the underlying mechanisms.
Methods
This study utilized cross-sectional data from the 2017 China General Social Survey (N = 2195). We employed the Ordered Probit (O-Probit) model and ordinary least squares regression to examine the impact of digital skills on health and explore the underlying mechanisms. Health inequalities across different groups were measured using the health concentration index.
Results
Enhancing digital skills enhances population health by boosting economic status, increasing social participation, and improving access to information. However, the impact varies by age and residence. Digital skills have a stronger effect on the health of young and middle-aged individuals, as well as urban residents, compared to older adults and rural populations. Furthermore, digital skills exacerbate health inequalities, benefiting high-income groups and widening the gap between income levels.
Conclusions
Widespread promotion and continuous improvement of digital skills are key to enhancing public health. We need to focus on the popularization of digital skills and the construction of digital infrastructure for low-income disadvantaged groups and rural areas, as well as use various means to reduce group and regional differences in the impact of digital skills on health conditions.
Introduction
The rapid advancement of information technology and its integration with socioeconomic systems have positioned digital technology as a key driver of global economic and societal progress. Recent data reveal that over 66% of the global population now uses the internet. 1 The widespread adoption of the internet and digital technologies has profoundly impacted human life by revolutionizing the ways information is exchanged and acquired, significantly influencing people's lifestyles, behavioral habits, and thought processes. Notably, according to PwC's data analysis, the impact index of digital technologies and artificial intelligence on residents’ health reaches as high as 3.4. 2 Two countries stand out in terms of capacity to engage in and benefit from digital technology: the United States and China. 3 As the largest developing country, China has formed the world's largest digital society with 1.092 billion internet users by December 2023, according to statistics from the China Internet Network Information Center. From the standpoint of China, scrutinizing individual digital skills and their implications for health emerges as pivotal in elucidating strategies for enhancing adaptation to the global digital shift. This examination is crucial for enabling nations and regions to bolster their digital economy's competitiveness, elevate the populace's quality of life, and fortify social welfare.
Previous research mainly focused on the impact of internet use on medical care and health, including medical costs,4,5 doctor–patient relationship,6–8 medical security model,5,9 health policy,10–12 health information search,10,13 medical information sharing,14,15 medical resource rationing, 16 mental health intervention,17–19 and many other aspects. Some studies focus on the impact of internet use on different groups. For example, Huan et al. 20 pointed out that internet use significantly reduced the level of depression in older people but also found that stopping using the internet was associated with depression or life satisfaction. There was no significant relationship with improvement. Yeunhee et al. 21 investigated the relationship between Korean adolescents’ internet use and health. In terms of health, subjective health, stress, feelings of sadness, and suicidal thoughts were also associated with time spent on the internet. Khodabakhsh et al. 22 studied the impact of internet use by three different levels of users (internet addicts, excessive users, and ordinary users) on health anxiety among Malaysian young people in the context of the COVID-19 epidemic. The results showed that compared with ordinary users and excessive users, internet-addicted users scored higher on overall health anxiety and health anxiety factors (possibility of illness and negative consequences) than internet-addicted users. High internet use appears to be associated with high health anxiety. People may search the internet for more information related to COVID-19 and symptoms, which may increase their health anxiety. In addition, some studies have focused on the impact of internet use on the health status of people in different regions.23–25 However, while the effects of internet use on health have garnered growing attention, the role of digital skill disparities in influencing the health of different groups has largely been overlooked. Therefore, this study not only examines the impact of digital skills on health but also analyzes how differences in digital skills affect the health of individuals across different regions, age groups, and income levels.
Based on the aforementioned issues, this study utilizes data from the 2017 China General Social Survey (CGSS) to empirically examine the impact of digital skills on health. It explores the mediating roles of income status, social participation, and information acquisition and investigates how differences in digital skills contribute to health inequalities across different regions and age groups. The contributions and innovations of this study can be summarized in three key aspects: (a) The construction of multidimensional indicators: Unlike previous studies that simply analyzed residents’ internet use, the CGSS systematically investigates Chinese residents’ digital skills and health outcomes. It employs six distinct questions to measure digital skills at multiple levels by summarizing and quantifying proficiency. (b) Comprehensive mechanism analysis: This study examines pathways to improving residents’ health from the perspectives of income status, social participation, and information acquisition. (c) Novel research perspectives: While most existing studies focus on the impact of internet use on health, this study further explores how variations in digital skills across age groups and between urban and rural areas affect health inequalities among different income groups.
Theoretical analysis and research hypotheses
Digital skills affect residents’ health status
The impact of digital skills on residents’ health is multifaceted, mainly through the following three channels.
First, higher digital skills can expand income sources and improve residents’ income levels, which in turn enhances their ability to access higher-quality health services. In the context of the digital economy, the internet has become a widely accessible entrepreneurial platform with low entry barriers. Increasingly, individuals are establishing e-commerce businesses, engaging in webcasting, and other online enterprises, using these activities as essential income sources. Therefore, proficient digital skills can increase the possibility of residents participating in the digital economy and growing sources of income, thereby prompting residents to have more funds to invest in their health and promoting the improvement of health levels. For example, Hargittai et al. 26 found that older adults are at a disadvantage in earning additional income due to their limited internet skills, which directly impacts their mental health. Sonia et al. 27 pointed out that digital skills are crucial for improving the employability of young people, which, in turn, enhances their living conditions. Similar studies conducted by Choi and DiNitto 28 and Estacio et al. 29 also suggested a “digital skills-income level-health status” transmission mechanism.
Second, digital skills can enhance residents’ level of social participation, which is a vital source of psychological comfort and support. 30 Research has shown that social participation is related to the improvement of self-rated health status.31,32 Digital skills enable residents to easily stay connected with others through social media, online communities, and other digital platforms. These social connections can provide emotional support, which can have a positive impact on health. For example, Wang et al.’s 33 study involving adolescents demonstrated that internet use and online social engagement can reduce loneliness and social isolation, strengthen interpersonal relationships, alleviate anxiety and depression, and improve mental health.
Third, digital skill levels will affect residents’ ability to obtain health information and health knowledge, affect residents’ health behaviors, and thus affect residents’ health status. Under the background of the rapid development of the digital economy, digital medical care, digital health care, and digital health care, with internet hospitals as the core, have gradually matured.
34
Higher digital skills can reduce information friction and enable individuals to fully utilize health-related information. For instance, individuals with proficient digital skills can more easily access internet hospital services such as online consultations, online registration, and online medication purchases.
35
They can also directly engage in audio and video consultations for remote diagnosis and treatment.
36
These measures can effectively help residents improve the efficiency of medical care, reduce overall health care costs, and improve residents’ health.37,38 In addition, Van Parys and Brown’s
35
research indicated that internet use can enhance residents’ access to health knowledge and medical information, thereby influencing their health behaviors and outcomes. Figure 1 shows the impact mechanism of digital skills on residents’ health.
H1: Digital skills have a positive impact on residents’ health. H2: Digital skills influence residents’ by enhancing economic status, increasing social participation, and improving access to information.

The impact mechanism of digital skills on residents’ health.
Regional and age heterogeneity in the impact of digital skills on health
On the one hand, the impact of digital skills on health outcomes is more significant in urban areas. Factors such as varying levels of economic development, internet penetration, and education create disparities in internet exposure among residents in different regions.39,40 Urban residents, who generally have earlier and more extensive exposure to the internet, tend to have higher awareness and more frequent use of digital technologies. In contrast, economically disadvantaged areas often lag in these aspects.41,42 Consequently, the impact of digital skills on health is more significant in urban areas, while it is relatively weaker in rural regions.
On the other hand, digital skills have a more significant impact on the health of young and middle-aged people. Generally, these age groups use the internet more frequently and possess higher digital skill levels.43,44 In contrast, the elderly tend to have lower digital proficiency,45–47 making young and middle-aged individuals more susceptible to the benefits of digital skills.
Overall, variations in digital skills across different regions and age groups lead to differing effects on health status.
H3:Significant regional and age heterogeneity exist in the impact of digital skills on health.
Digital skills influence levels of health inequalities between groups
A digital divide exists between people of different income levels, where disparities in internet access and digital skills contribute to health inequalities among income groups. Low-income individuals often face time constraints and lack educational opportunities, making it difficult for them to access high-quality internet services and related training. This limitation hinders their ability to obtain health information and utilize online medical resources,48,49 resulting in a weaker impact of digital skills on their health. Conversely, high-income individuals typically have more time and greater access to digital skills training or daily learning, enabling them to use these skills to select better information tailored to their needs their needs.
50
As digital medical resources—such as online diagnosis and treatment, health applications, and health information platforms—become increasingly widespread, specific digital skills and language proficiency are essential for accessing these resources. Low-income groups with insufficient digital skills may struggle to fully utilize these resources, missing opportunities for health management and treatment. In contrast, high-income individuals often benefit from digital health tools such as smart devices and health trackers, leveraging their digital skill advantages to monitor their health status better and take corresponding measures.
H4:Improving digital skills will widen the health inequality between different income groups.
Methods
Data sources
This study employs a cross-sectional design, utilizing data from the 2017 CGSS. The CGSS is a large-scale, nationally representative survey that gathers information on a wide array of social, economic, and cultural dimensions of China, particularly investigating personal health and internet usage in detail. Conducted from June to November 2017, the survey employed multistage stratified sampling across 31 provinces, autonomous regions, and municipalities directly under the central government, collecting data at the individual, household, and community levels. Missing values and outliers were excluded, resulting in a final sample of 2195 valid responses.
Variable selection
Dependent variable
Health status.
The variable explained in this article is the health status of residents. Self-assessed health status is an individual's subjective judgment based on their objective health status, which can comprehensively reflect the multidimensionality and integrity of health. Therefore, this study used self-rated health to measure an individual's health status. The CGSS2017 questionnaire asked the respondent, “What do you think your current physical health status is?” The respondent's answers were “very unhealthy, relatively unhealthy, average, relatively healthy, and very healthy,” with values ranging from 1 to 5. At the same time, physical health was measured using the questionnaire “In the past four weeks, the frequency with which work or other daily activities were affected by health problems.” The respondents’ answers were “always, often, sometimes, rarely, and never” and were assigned an integer from 1 to 5. From the Mental Health Adoption Questionnaire: “In the past four weeks, how often have you felt depressed or depressed?” The respondents’ answers were “always, often, sometimes, rarely, and never,” which were assigned an integer from 1 to 5. The evaluation results are shown in Table 1.
Distribution of residents’ health status.

Note. Calculated by the author.
Among the 2072 residents interviewed, the most significant proportion of self-assessed health was “relatively healthy” at 41.67%, followed by “very healthy” at 25.19% and the minor proportion was “very unhealthy” at only 2.16%. Overall, the average self-assessed health level of the residents interviewed was 3.78, roughly between “average” and “relatively healthy.”
Among the answers to physical health (because health affects work frequency), the most significant proportion is “never” at 50.32%, followed by “rarely” at 31.51% and the minor proportion is “always” at only 1.47%. Overall, the average physical health level of the residents interviewed was 4.23. It is roughly between “never affecting work due to health” and “rarely affecting work due to health.”
Among the answers to mental health (depressed mood or frequency of depression), “rarely” accounted for the most significant proportion at 35.85%, followed by “never” at 32.23% and “always” accounted for the minor proportion at only 1.34%. Overall, the average physical health level of the residents interviewed was 3.90. Roughly somewhere between “sometimes feeling depressed or depressed” and “rarely feeling depressed or depressed.”
Independent variable
Digital skill.
Digital skills refer to the ability to use information technologies such as the internet and cloud computing to obtain and produce essential information and solve complex problems in reality through practical evaluation and processing of information.51,52 As discussed in the Theoretical analysis section, these skills may impact individual health through various mechanisms.26,30,36 This article employs internet usage skills as a proxy variable for digital skills. Previous researches will refine internet usage skills into six abilities for using information technology: simple operation, understanding the structure, searching for information, external communication, content creation, and achieving goals.53,54 The CGSS2017 questionnaire asked the following questions for respondents, effectively covering the definitions of internet usage skills outlined in existing literature: “I can use a computer to open websites,” “I can use a smartphone to download and install APPs,” “It is not difficult to find the information you want online,” “Online (such as WeChat, Weibo) When I see important news forwarded by people around me, I will verify it first before believing it.” “When I want to express my thoughts online, I know how to do it.” “When making payments or transactions online, I Will observe the use environment to determine whether to use.” Accordingly, this study utilizes the above questions as a standard to measure digital skills. By answering “strongly inconsistent,” “not consistent,” “it does not matter whether consistent,” “compliant,” and “very consistent,” each is assigned a value of 0–4, according to the score. A total score is added, with higher scores indicating more excellent numerical skills. See Supplementary Material for definitions of variables.
Mediating variables
Income status, social participation, and information acquisition.
Based on the theoretical analysis, this study selects mediating variables from three dimensions: income status, social participation, and information acquisition. To achieve a comprehensive measurement of these dimensions, four variables were chosen for income status: individual annual income, individual labor income, total family income, and financial stability. Social participation was measured using four variables: connections with family, friends, and close friends through online social activities, as well as the frequency of communication through online activities. Information acquisition was measured using four variables: frequency of acquiring, browsing, commenting, and posting information online. See Supplementary Material for definitions of variables.
Control variables
Based on the CGSS2017 questionnaire, a series of control variables are included in the subsequent empirical analysis. As shown in Table 2, the selected control variables mainly include age, gender, years of education, marital status, political affiliation, income level, basic medical insurance, and health behaviors. See Supplementary Material for definitions of variables.
Descriptive statistics of variables.

Note. aNot in school = 0 years, primary school = 6 years, junior high school = 9 years, high school (including technical secondary school) = 12 years, junior college = 15 years, undergraduate = 16 years, postgraduate = 19 years.
Statistical analysis
The characteristics of respondents, health status, digital skills, income, social participation, access to health information, were described using frequencies and percentages for categorical variables and means with standard deviations for continuous variables. Digital skills were presented by summing the scores of the six individual competencies. The ordered Probit (O-Probit) model and ordinary least squares (OLS) regression analysis were conducted to explore the impact of digital skills on health. The models were adjusted stepwise for age, gender, education level, medical insurance, marital status, political status, and health behavior. Additionally, potential confounders and interaction effects were examined; no significant effect modification was identified. All statistical analyses were performed using Stata version 17.
Model setting
The impact of digital skills on health
First, we set up the OLS regression model
The O-Probit model is also applicable because the variables described in this article can also be treated as ordered discrete variables. Therefore, to examine the robustness of the OLS regression model, this article further sets up the O-Probit model to contrast with the OLS estimation results. The specific model settings are as follows

Health concentration index and its decomposition
The health concentration index is a commonly used indicator to measure the degree of health inequality among different income groups.55–57 The calculation of the health concentration index must include two elements: first, the indicators for measuring health, usually binary or continuous variables, cannot be multivariate ordered variables. This study uses self-assessment of health, physical, and mental health to measure health status. The second indicator is to measure economic status, that is, to measure income status. This study measures household per capita income. The health concentration index specifically manifested as the area between the health concentration curve (the horizontal axis represents the cumulative percentage of individuals ranked from low to high income, and the vertical axis represents the cumulative percentage of individuals ranked by health status) and the fairness line (45 degrees diagonal), which is twice the area. Therefore, this study draws on the approach of Kakwani et al.,
58
Wagstaff,
59
and Wagstaff
60
and defines the expression of the health concentration index as
The health concentration index measures the extent of health inequality relative to income. Nevertheless, we are more concerned about what factors affect the degree of health inequality related to income, so we further decompose the health concentration index. Referring to the practices of previous studies,55–57 the health concentration index is decomposed into the sum of the contributions of each health factor. The contribution of each factor can be divided into the direct impact of the factor on health (measured by the elasticity) and the indirect impact of the factor on income-related health inequalities by covering different income groups (measured by the concentration index of the factor).
Therefore, it is necessary to calculate the concentration index and elasticity of each influencing factor. We first need to analyze the marginal effects of each factor on health. This study uses the OLS model for identification. The specific model settings are as follows

Results
Baseline regression analysis
Table 3 shows the estimation of the OLS model and O-Probit model results on the impact of digital skills on residents’ health. The results showed that whether it was an OLS regression that treated self-rated health as a continuous variable or an O-Probit model that considered intrinsic ordering, the variables’ influence direction and significance level did not change significantly between columns. In the OLS model, the regression coefficient of numerical skills is 0.0182, while in the O-Probit model, the regression coefficient of numerical skills is 0.0200, and there is little difference between the coefficients. The regression coefficient of digital skills is significant at the 1% level in both models, strongly indicating that residents’ health levels also improve as digital skills improve.
The impact of digital skills on residents’ health.

Note. OLS: ordinary least squares; O-Probit: Ordered Probit.
* P < .1. ** P < .05. *** P < .01.
In terms of control variables, age, income, and health behaviors have a significant impact on health. Taking self-rated health as an example, age hurts residents’ health at the 1% significance level; the older they are, the worse their health status is, which is consistent with common sense. Personal income positively impacts residents’ health at the 1% significance level. The higher the income, the richer the resources available and the greater the ability to enjoy medical care services, thus improving individual health. Marital status has a significant positive impact on residents’ health. Married people generally participate less in risky activities that are out of consideration for their partners and families, lead a more regular life, and receive better care from their partners to be healthier. Political outlook has a significant positive impact on residents’ health. Following organizational disciplines, accepting political education, paying attention to social responsibilities, and influencing and helping each other encourage Communist Party members to pay more attention to health and develop healthy living habits. Healthy behaviors positively impact residents’ health at the 1% significance level. For example, regular physical exercise will improve people's cardiopulmonary function, physical fitness, and health level.
Endogeneity discussion
Regarding possible endogeneity problems, this article has made more significant efforts to select control variables and control-relevant influencing factors as much as possible to reduce the problem of omitted variables caused by unobservable factors. At the same time, this article will look for instrumental variables for digital skills to reduce biased and inconsistent estimation results caused by possible endogeneity problems.
To be effective, instrumental variables must satisfy two conditions: they must be correlated with endogenous variables and uncorrelated with random disturbance terms.61–63 Based on the research by Luo et al., 64 this study selects the 2017 provincial rural household internet penetration rate and internet-enabled devices as instrumental variables for residents’ digital skills.
The internet penetration rate reflects the extent of internet infrastructure coverage in a region. A higher penetration rate increases residents’ access to the internet, providing more opportunities to learn and use digital technologies, thereby enhancing their digital skills. 65 Consequently, there is a significant positive correlation between internet penetration rates and residents’ digital skills. However, internet penetration rates are primarily determined by external factors such as government policies, economic development levels, and infrastructure construction, 66 which are not directly related to individual digital skill levels. Thus, the rural household internet penetration rate can be considered exogenous and appropriate as an instrumental variable.
Internet-enabled devices are fundamental for residents to use the internet. Residents who own such devices are more likely to engage in activities like learning, working, and entertainment online, which helps them continuously improve their digital skills.26,67 Thus, there is a significant positive correlation between the internet-enabled devices and residents’ digital skills. However, the ownership of these devices is largely influenced by factors such as household economic conditions,68,69 personal preferences, 20 and market supply,70–72 which do not directly affect residents’ digital skill levels. Therefore, the number of internet-enabled devices is considered exogenous and is suitable as an instrumental variable.
As can be seen from Table 4, in the regression where the explained variables are self-rated health, physical health, and mental health, the P values of the Durbin–Wu–Hausman test are .0035, .0024, and .0004 respectively, at the 10% significance level. The homogeneity hypothesis is rejected, and there is indeed an endogeneity problem. Moreover, in the regression, internet skills still significantly impact health, and the direction of the effect has not changed; both are significant at the 1% level; the Cragg-Donald Wald F statistics are also more important than the critical value under 10% bias, the weak instrumental variable problem can be ruled out. 73 The tests above indicate that even when using instrumental variable methods, digital skills still significantly improve residents’ health.
Instrumental variable estimation.
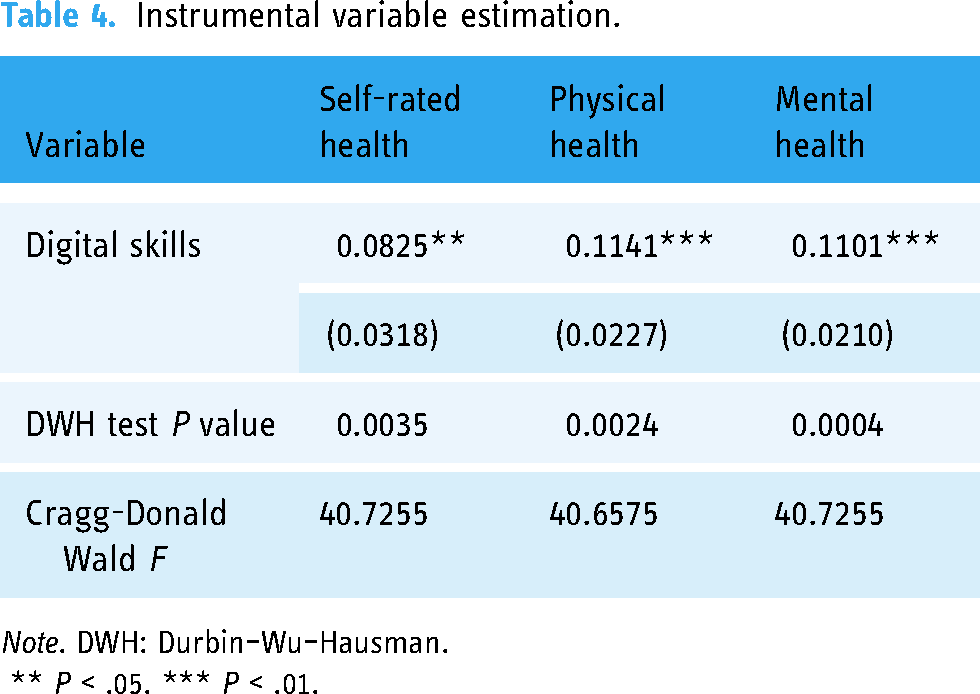
Note. DWH: Durbin–Wu–Hausman.
** P < .05. *** P < .01.
Robustness check
This study used six separate questions that quantify numerical skill proficiency by summarizing calculations: “I can use a computer to open websites,” “I can use a smartphone to download and install APPs,” “It is not difficult to find the information you want on the Internet,” and “See the surroundings on the Internet (such as WeChat, Weibo) I will first verify important information forwarded by others before I believe it.” “When I want to express my thoughts online, I know how to do it.” “When making payments or transactions online, I will observe the usage environment to determine whether to use.” In the robustness test, six questions were used to regress health separately.
As can be seen from Table 5, whether it is self-rated health, physical health, or mental health, the impact coefficients of various digital skills on health are all positive, consistent with the conclusion of the baseline regression. However, there are differences in the impact of different digital skills on health. The skills of “opening websites” and “finding information” significantly positively impact residents’ self-evaluated, physical, and mental health. The skills of “installing apps” and “expressing ideas” significantly positively impact residents’ self-evaluated health and physical health. There is a positive impact, while the “verification information” and “online payment” skills only positively impact residents’ self-rated health.
Robustness check.
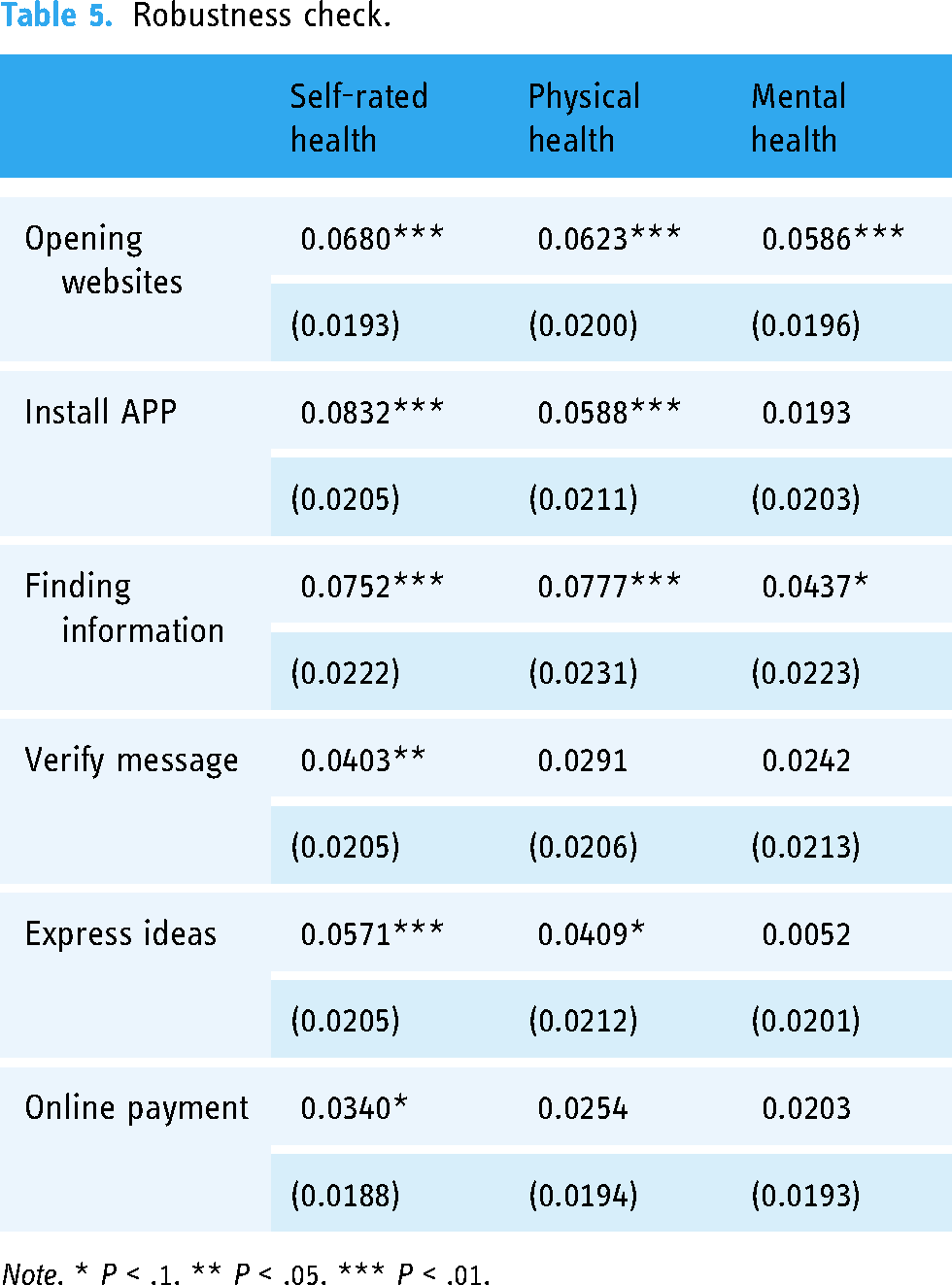
Note. * P < .1. ** P < .05. *** P < .01.
Analysis of impact mechanism
Given the main results above, it is crucial to understand the specific mechanisms through which digital skills can enhance residents’ health. In this section, we explore potential channels from the perspectives of income status, social participation, and information acquisition. The impact of these variables on health has been confirmed in many studies, such as Deaton and Paxson 74 and Marmot. 75 Therefore, based on relevant research, we further conduct mechanism testing.
Income status
Some research has proven that income status is closely related to health because it determines residents’ ability to access medical services, healthy food, and a good living environment, thereby directly or indirectly affecting their overall health.76,77 Table 6 shows that digital skills have a significant positive impact on individual annual income, individual labor income, total family income, and financial stability. This indicates that enhanced digital skills can contribute to increased income at both the individual and family levels, potentially easing the challenge of balancing income and expenses. Consequently, digital skills can enhance health by improving income status.
Impact of digital skills on income status.

Note. The variables individual annual income, individual labor income, total family income, and financial stability are expressed as logarithmic values. ** P < .05. *** P < .01.
Social participation
Social participation significantly impacts health by facilitating social interactions and strengthening social connections, which enhances mental health and may positively influence physical health by reducing loneliness and stress.78,79 This study examined the impact of digital skills on social participation as shown in Table 7 (see supplementary material for definitions of variables). The results indicate that digital skills are significantly and positively associated with the frequency of communication through online social activities, as well as with connections to family, friends, and close friends. These findings suggest that digital skills play a crucial role in enabling social interaction via the internet, thereby promoting health.
Impact of digital skills on social participation.

Note. *** P < .01.
Information acquisition
Access to health information promotes health by enabling individuals to learn about disease prevention, healthy lifestyles, and other critical health-related topics. This knowledge empowers them to make informed health decisions, adopt positive health behaviors, and enhance their self-management capabilities.80,81Although the CGSS2017 database does not directly inquire about residents’ access to health information, it does assess their access to information via the internet. Generally, better access to information correlates with better access to health information. 82 Table 8 illustrates the effect of digital skills on residents’ information access behaviors. The results indicate that digital skills are positively correlated with the frequency of acquiring, browsing, commenting, and posting information online. Improved digital skills facilitate more frequent engagement with health information through the internet. These findings suggest that digital skills play a crucial role in enhancing residents’ information acquisition.
Impact of digital skills on access to health information.
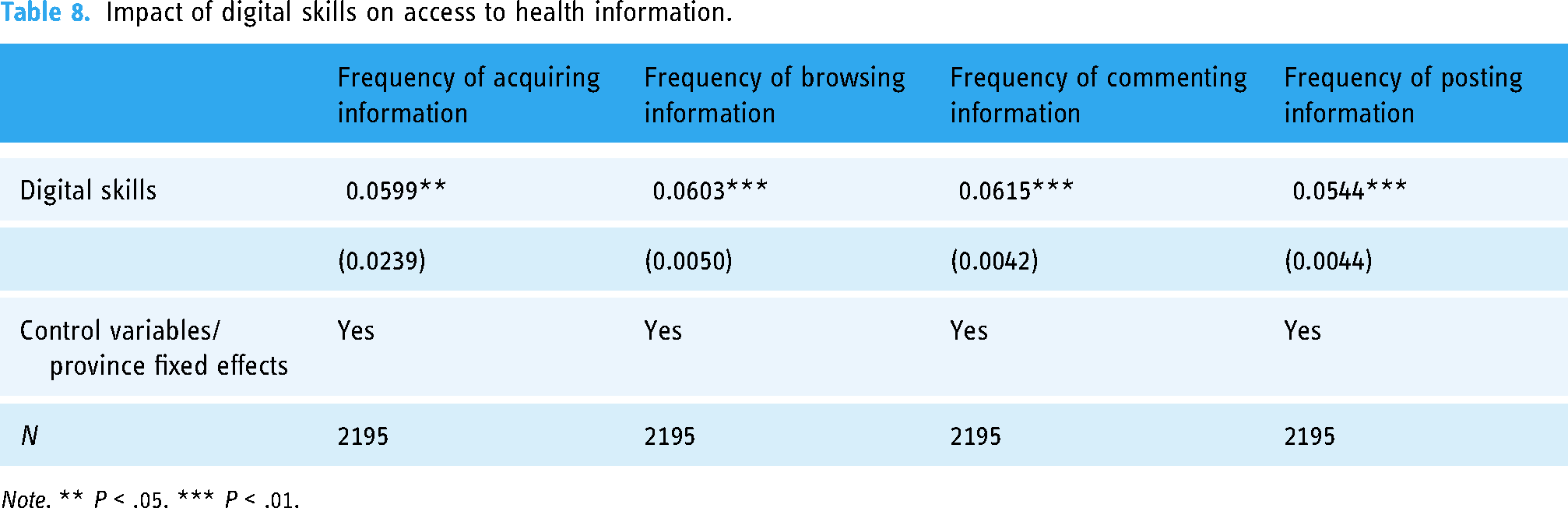
Note. ** P < .05. *** P < .01.
Heterogeneity analysis
The above analysis has shown that digital skills can significantly promote residents’ health. However, this is only an average estimate and does not consider group differences. To this end, this article will further explore the heterogeneous characteristics of the impact of digital skills on residents’ health in different ages and regions. When assessing the impact of digital skills on health, it is essential to consider age and urban–rural differences. Digital skill proficiency, usage habits, and health information access methods vary significantly across age groups. For instance, younger individuals are typically more skilled in using digital technologies and more frequently obtain health information online, while older individuals may rely on traditional channels. Likewise, urban residents generally have better access to advanced digital technologies and abundant health information, whereas rural residents often encounter digital divides and information scarcity. Thus, accounting for these differences is crucial for understanding the diverse effects of digital skills on health and for developing targeted health intervention policies. The regression results using the OLS model are shown in Table 9.
Heterogeneity analysis.

Note. Both have used control variables and province fixed effects. *P < .1. **P < .05. ***P < .01.
Regarding heterogeneity at the age level, 60 is usually an essential mark for dividing young, middle-aged, and elderly groups, so this article divides different age groups according to this age. Columns 1 to 3 of Table 9 show that improving digital skills can significantly improve the health status of young and middle-aged people. Columns 4 to 6 show that internet use does not significantly impact the health indicators of the elderly group over 60 years old. This may be because the internet is more integrated into the lives and careers of young and middle-aged people. At the same time, due to their relatively high acceptance and adaptability, they are more receptive to emerging things. This makes their cognitive patterns, social interaction styles, and lifestyles more sensitive to the impact of the internet. Overall, the effect of digital skills on residents’ health is age specific. In particular, digital skills significantly impact the health of young and middle-aged people aged 18–60.
Regarding the heterogeneity at the residence level, columns 1 to 3 of Table 9 show that digital skills significantly impact the self-rated health, physical health, and mental health of the group living in urban areas, and they are significant at the 1%, 5% and 10% levels, respectively. Columns 4 to 6 show that digital skills have a substantial impact on the self-rated health and physical health of the group living in rural areas and are significant at the 5% and 10% levels, respectively, but have no significantly impact on the mental health of the group living in rural areas. This may be because residents in urban areas have access to a broader range of health information, online health services, and social interaction opportunities due to their relatively developed digital environment. In addition, because urban residents have higher information literacy regarding access to information and data screening, they can more effectively identify the credibility and value of information. Overall, the impact of digital skills on residents’ health is heterogeneous between urban and rural areas of residence. In particular, digital skills significantly impact the health of groups living in urban areas.
Analysis of health inequalities
The self-rated health concentration index, physical health concentration index, and mental health concentration index of residents are 0.0199, 0.0200, and 0.0182, respectively, all positive values. The concentration curves of health inequality are below the diagonal line, indicating that those with poorer health residents are mainly concentrated in groups with lower socioeconomic status. High-income groups have better health status, and health inequality favors high-income groups.
The health concentration index was further decomposed based on the OLS model's regression coefficient, and each variable's elasticity was measured. The concentration index of each variable was measured. Finally, the contribution rate of each variable to income-related health inequality was calculated (the overall contribution of each variable was divided by the health concentration index). As shown in Table 10, the contribution rates of digital skills to self-rated, physical, and mental health inequality are 17.34%, 12.66%, and 8.94%. The contribution rates are favorable, meaning digital skills will intensify health inequalities across income groups.
Decomposition of residents’ income-related health inequality.

Note. Calculated by the author.
Among other control variables, this study also found that factors such as years of education, personal income, and political affiliation are essential factors in exacerbating income-related health inequality. For example, the contribution rate of pay to self-rated health inequality is as high as 37.01%. The more unequal the income distribution, the more high-income people have better equipment, network access, and digital literacy, and they use the internet more fully to obtain health information, online medical services and health management tools to improve health levels, thereby achieving better health improvement results and expanding health inequality among people with different incomes.
Discussion
Principal findings
This study found significant positive associations between digital skills and health, which aligns with existing literature.33,37,64 However, the impact of different types of digital skills on health varied, in particular, the skills of “opening websites” and “finding information” demonstrated notably strong positive effects on self-assessed health, physical health, and mental health. Individuals who mastered these two skills navigated online information more efficiently, reducing asymmetries in health resources and information, 1 which led to more informed health decisions.
Further analysis revealed that digital skills contributed to increased personal and household income; alleviated the pressure between income and expenditure; and enhanced access to health care services, healthy food, and good living environments, thereby positively influencing health status. Additionally, improved digital skills fostered social interactions, allowing individuals to maintain more frequent contact with family and friends, which, in turn, improved mental health. Enhanced digital skills also enabled individuals to seek and share health information within social networks, 34 reducing information asymmetry and enhancing knowledge about disease prevention, healthy lifestyles, and other health-related topics. Future research should delve deeper into these mediators to provide empirical support for enhancing digital skills and health.
Interestingly, despite the overall advantages of digital skills, disparities can act as barriers when considering differences among groups such as age and socioeconomic status. Specifically, older adults and rural residents tend to have lower levels of digital skills, which adversely affect their access to health resources and necessary health information. This finding aligns with previous research on the digital divide and its implications for health equity.37,74,83 Therefore, future studies should focus more on these vulnerable populations and develop targeted strategies to improve their digital skills and health.
Enlightenments
This study provides evidence for the significance of digital skills in enhancing health outcomes. With the rapid advancement of digital technology, improving individuals’ digital skills is critical not only for promoting health equity but also for significantly enhancing overall well-being. Based on these findings, we recommend focusing on the following three key areas:
Widespread promotion of digital skills education: Emphasizing digital skills education, particularly for middle-aged and elderly individuals, is essential. Digital skills can be enhanced through the establishment of community training centers, education programs that integrate online and offline methods, and the provision of specialized courses and resources. Additionally, targeted promotional efforts should be strengthened to help this demographic make better use of digital technology to improve their health. Strengthening digital infrastructure in underserved areas: The development of digital infrastructure in rural and underdeveloped regions must be prioritized. Due to inadequate infrastructure, the potential benefits of digital skills remain largely untapped in these areas.
1
The government, in collaboration with the private sector, should be encouraged to invest in infrastructure development to ensure comprehensive network coverage and equipment accessibility. This investment will facilitate the promotion and application of digital health technologies, improving rural residents’ access to health information and services. Focus on health assistance for low-income groups: While enhancing digital skills can improve health outcomes, it may also exacerbate health inequalities during implementation. Therefore, it is crucial to develop health care support policies specifically for low-income groups to ensure equitable access to health resources. Providing free digital skills training and access to health information will help reduce health disparities and improve overall health outcomes for disadvantaged populations.
Strengths and limitations
This study offers several key advantages. First, the digital skill indicators employed in this article are more multidimensional than those in previous studies.45,53 By utilizing six distinct questions from the CGSS dataset, the study provides a comprehensive measurement of the population's digital skill levels, yielding more credible findings. Second, the study conducts an in-depth mechanistic analysis to uncover the various pathways through which digital skills affect health. Specifically, it examines the mediating roles of economic status, social participation, and access to information, offering detailed insights into how these factors contribute to health improvements and providing empirical evidence to support the promotion of population health. Third, by considering differences in digital skills across population groups (e.g., age and place of residence), the study offers new perspectives on the digital divide and its implications for health inequalities.
While this study provides valuable insights into enhancing digital skills and improving population health, it has several limitations. First, due to data constraints, the study relied solely on the 2017 CGSS data. As a cross-sectional study, it has limited ability to establish causality, 84 and the data's time lag may not accurately reflect the current situation. Future research could address these limitations by employing more recent and longitudinal data, combining multiple periods, and incorporating individual case studies to supplement and refine the findings. Second, there may be potential biases in participant data collection, recruitment, and selection. The indicators used—such as health status and digital skills—were based on self-reported data, which may not always be accurate due to measurement errors or reporting biases, despite literature supporting the validity of this approach. 21 Future studies could enhance the robustness of findings by integrating data from comparable sources, such as the 2020 and 2022 China Rural Revitalization Survey. Additionally, with the support of data and funding, the potential to conduct more detailed case studies in the future would enhance our research and strengthen the credibility of our results. Third, while this study focuses on the positive impact of digital skills on population health, it overlooks potential negative effects of prolonged electronic device use. 85 For instance, extended screen time may lead to eye strain or fatigue, adversely affecting physical and mental health. This aspect warrants consideration in future research.
Conclusions
Based on the CGSS (2017), this article uses OLS and O-Probit models to verify the impact of digital skills on residents’ health and health inequality from a micro perspective. On this basis, it explores the impact mechanism of digital skills on residents’ health. Endogeneity discussion, heterogeneity discussion, and robustness test were also conducted. Research results show that digital skills have a significant positive impact on residents’ health. Heterogeneity analysis indicates substantial differences in the impact of digital skills on residents’ health in different ages and regions. Digital skills have a more significant impact on young and middle-aged groups and residents in urban areas than older groups and rural groups. The impact mechanism analysis found that digital skills can improve health by boosting economic status, increasing social participation, and improving access to information. The health concentration index analysis found that digital skills impact health inequality, favoring high-income groups and expanding health inequalities among people with different incomes.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241304592 - Supplemental material for The impact of digital skills on health: Evidence from the China General Social Survey
Supplemental material, sj-docx-1-dhj-10.1177_20552076241304592 for The impact of digital skills on health: Evidence from the China General Social Survey by Cheng Qin, Yuchen Zhu, Donglin Li and Can Liu in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to sincerely thank the China General Social Survey (CGSS) 2017 Team.
Contributorship
QC was responsible for conceptualization, formal analysis, methodology, writing the original draft, supervision, and writingreviewand editing. ZYC handled data curation, methodology, formal analysis, writing the original draft, and writing-review and editing. LDL contributed to conceptualization, writing the original draft, supervision, funding acquisition, and writing-review and editing. LC conducted formal analysis and wrote the original draft. All authors reviewed the final manuscript.
Data availability
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical review and approval were waived for this study, as the study used the open database of the China General Social Survey (CGSS) and did not include experimentation that may bring possible risk of harm to participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been funded by the National Social Science Fund Youth Project of China (No. 24CJY012), the Key Research Base of Humanities and Social Sciences of Universities in Guangxi Zhuang Autonomous: China-ASEAN Collaborative Innovation Center for Regional Development (No. CWYB202405) and the research fund of School of Economic, Guangxi University (No. 2024JK11).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.