
Abstract
Objective
This study analyses access to and use of eHealth services in Spain from a multidimensional perspective, considering how sociodemographic factors such as age, gender, educational level, income, nationality and place of residence influence digital divide in health. The digitalisation of public services has generated new opportunities, but it has also accentuated structural inequalities in access to key eHealth tools. Specifically, this study focuses on three components: the Digital Health Record (DHR), electronic prescriptions and digital certificate.
Methods
This research is based on a quantitative approach, using data from the three waves of the Health Barometer 2024 of the Centro de Investigaciones Sociológicas—CIS—with a total sample of 7.623 cases. Binary logistic regression models were applied to identify which variables predict the accessibility and usability of these services.
Results
The results show that variables such as age, gender, educational level, income, employment status, nationality, place of residence and health status have a significant impact on the probability of using eHealth tools. Especially older people, people with less education or low economic resources present greater barriers, which would evidence a structural and multidimensional digital divide.
Conclusion
This study suggests that the digitalisation of the healthcare system may reinforce existing inequalities. Particularly those associated with the factors that showed the greatest influence on access to and use of digital health services in the analysis, such as age, income and educational level. These findings highlight the need for inclusive digital health policies that address the multidimensional nature of digital divide.
Introduction
The evolution and consolidation of Information and Communication Technologies (hereafter, ICTs) within different spheres of society have generated new fields of relationship between citizens and public bodies.1,2 These technologies have been incorporated within the institutions in question and across the range of their services. This integration has resulted in a redefinition of the interactions that take place in these spaces.
In the context of the varied areas and public policies, the field of health has emerged as a notable sector, particularly regarding the advent of transformative technological advancements. These developments have contributed to the evolution of the concept of eHealth, which has gained significant prominence in recent times.3,4 As asserted by Jaworski et al., 5 this term functions as a comprehensive designation encompassing the adoption of a diverse array of digital tools and services, with the objective of furnishing citizens with access to these assets, and which aim to improve their health and well-being, both individually and collectively. 6 Therefore, eHealth has attempted to respond to these principles under the criteria of seeking better healthcare, updating and renewing the portfolio of services, reducing costs, promoting equity or guaranteeing better access to the services offered.7,8 Despite the growing literature on eHealth and digital inequalities, there is a notable research gap of nationally representative studies examining how accelerated healthcare digitalisation, particularly after COVID-19, has reshaped access to and use of important services
The evolution of the digitalisation of healthcare services has been vertiginous. The changes brought about by this transformation encompass both the adaptation of existing services and the development of new functions, platforms, devices and virtual applications.9,10 The functionalities that have been built have resulted in a wide variety of services, whether they are aimed at self-management—through tools such as mobile phones or other devices, interaction teleconsultations or video calls, data storage and management—Digital Health Record (hereinafter, DHR)—or web portals and electronic prescriptions11. 11 All these elements, present in the last decades, have received a boost during and after the COVID-19 pandemic,11–13 changing the previous doctor/patient relationship, leaving the door open to new opportunities, but also to risks, such as social exclusion. 12
Contrary to these expectations, the existing material conditions for some authorships resulted in a reduction of the transformative potential attributed to the different digital tools, which were expected to improve the universalisation of health services, 14 accentuated by the irruption of COVID-19.15,16 In this scenario, the consolidation of the eHealth framework 17 coexisted with exclusion dynamics that affected multiple groups, resulting in their marginalisation from the digital transformation and their exposure to the so-called digital divide. 18
This phenomenon has been characterised by the structuring of different barriers and therefore, distances or borders—between those people who achieve a certain ability, competence or skill, which enables them to access and make continued use of ICTs, and those who remain on the margins. 19 Furthermore, this division between groups has meant unequal access to the different media available, insofar as knowledge, skills and the different uses or employment of these have been determining factors in the development of their respective individual well-being, with special impact in the case of health. 20
The multidimensional nature of the digital divide results in their marginalisation within the ambit of digital development.10,21,22 Broad questions emerge at this juncture, where variables such as knowledge, ability, access or use converge. 23 In addition to this, classic forms of exclusion, such as time, capital, class, gender, age, income, level of education, health status or employment status, among others are also considered. 24 This makes it difficult to achieve a balanced equalisation between social groups, leaving a diversity of groups excluded, restricting multiple rights and opportunities for their well-being.25–27
In this sense, the literature focused on the sociology of medicine 28 has been intensifying its production in relation to the health-technological theme, as an element of change. ICTs have also contributed to the reshaping of numerous processes linked to individual wellbeing. An example of this has been the expansion of social media platforms and networks, consolidating themselves as alternative spaces where patients seek information about pathologies, treatments or experiences of other users in the healthcare system. 29 Thus, the empowerment of patients in terms of access produces what Lupton 29 denominates the ‘digitised healthy citizen’, an idea that encompasses the definition of a population that is more informed and prevented in terms of their health care. At the same time, other authors have pointed out that this information overload may result on the medicalisation and pharmaceuticalisation of society, giving rise to a debate surrounding the limits of scientific-technological progress in health.30–33
In the context of the depletion of human capital and infrastructure in public services,34–36 eHealth tools have been adopted as a potential solution to the issue of patient facing healthcare in the post-global economic crisis context of 2008. 37 In this environment, ICTs also face ethical challenges, as they can either reduce or contribute to medical negligence or iatrogenesis. Tools such as chatbots or prescriptions powered by Artificial Intelligence (AI) could potentially reproduce biases in healthcare, leading to a lack of personalised care, thereby reducing the quality and equity of healthcare treatments and negatively impacting individual well-being. 38
However, one of the main challenges of eHealth is those related to exclusion and the digital divide. With the irruption of the different digital tools, services and applications in the health sector, 39 it has been highlighted how certain social groups have been particularly disadvantaged, not only due to the lack of access, 40 but also by the consequences that this phenomenon generates on them, such as the lack of participation through these technologies, demotivation and frustration in the use and learning of ICTs or in the loss of quality of life.41,42 Within this field, the most extensive analysis has been conducted on two factors: age and gender.
Regarding to age, the adoption of ICTs in healthcare systems has been accompanied by a generational gap,43,44 raising questions about societal acceptance of digital advances. Significant differences in the utility given by each age group have been identified. 45 These differences are intertwined with other signifiers, such as gender, ethnicity, class, level of education or income, etc. All these factors have a decisive impact on the use of these eHealth tools, challenging the idea of homogeneity within these groups.46,47
Concepts such as ageism48,49 or gerontophobia50,51 can arise, which may foster feelings of demobilisation regarding participation, employment or in the engagement of these groups in using and learning about ICTs. It is worth noting that even when the population is ageing and becoming increasingly connected, it is the over-75s who are most affected. This is related to the fact that older people who have recently left the workforce often already have certain digital skills. 52 As pointed out by the National Technology and Society Observatory 53 in its report on the use of technologies by the elderly, 54 in Spain, less than half of the those over-75s (41.7%) have ever accessed the Internet, far from the general population, where more than nine out of 10 (92.9%) have accessed it at some time.
Regarding the gender variable, the literature identifies differences in relation to ICTs in terms both of access and in carrying out activities through platforms or searching for information.55,56 These issues are therefore embedded in a framework of the reproduction of inequalities in the health sector, which is particularly directed towards the most vulnerable people, especially women and other traditionally excluded groups. 57
Both images contrast with Lupton's proposal of that ‘digitised healthy citizen’, 29 since neither access nor technological skills can be taken for granted, and, in view of the literature, the mere existence of eHealth services does not imply their use and correct usability. It should be noted that such services may be offering more possibilities to those in privileged positions, failing to mitigate existing differences and worsening the relative position of a part of society that is already vulnerable.
Consequently, healthcare becomes yet another domain in which social disparities are accentuated on the basis of access or utilisation. 58 In this sense, the consumption of these services by men and women is partly determined by the design and implementation of the different measures, including eHealth. 38 These policies often fail to address issues that disproportionately affect women, such as poorer self-perception of health, greater mental health deterioration,59,60 drug consumption 61 or violations of human and sexual rights, including obstetric violence. 62
Also relevant is the issue of the traditional role of women as caregivers, particularly in relation to health. 63 As the World Health Organisation (WHO) pointed out, 64 up to 80% of all care work is performed by women, much of which is both unpaid and unrecognised. Consequently, despite the advancement in care issues, these dynamics persist and are exacerbated by the increase in life expectancy. This results in the feminisation of care across all generations. 65 In Spain, as in many other contexts, women disproportionately assume informal caregiving responsibilities within families, especially for older adults and dependents. 66 This caregiving role often requires frequent interaction with healthcare services, making access to eHealth tools—such as digital health records, electronic prescriptions, and online appointment systems—particularly critical. Therefore, gendered patterns in digital access have direct implications for both individual and family-level health management. 46
In this way, the research has gathered materials to identify not only the digital divide, within these groups, but also those excluded from the potential benefits of eHealth. In the case of Spain, public administrations and institutions have not adequately addressed this issue, implementing different measures and services without considering potential digital divides. 67
The adoption of ICTs in healthcare services has also been supported by national bodies that have gradually introduced mechanisms to measure this phenomenon. The most significant cases are those of the National Statistics Institute (INE), with the Survey on Equipment and Use of Information and Communication Technologies in Households 68 —launched in 2006; ONTSI—since 2004—and the Centro de Investigaciones Sociológicas (hereinafter, CIS), which since 2012 has been asking in successive Health Barometers various questions and opinions about eHealth and the corresponding tools, services and uses that the public administration itself has been implementing. 69
From a national perspective, the outbreak of the pandemic led to a significant increase in the uptake of eHealth services among the general population. Although many of these tools had been implemented in previous years, 67 their development was significantly accelerated from 2020 among the different Spanish healthcare systems-one per autonomous community, despite them essentially share common characteristics in the most basic aspects.
Therefore, the literature review provided a global overview of the various aspects of socioeconomic inequalities, paying particular attention to the intersection of ICTs with factors such as gender and age. The interaction between these variables plays a fundamental role in technological development expectations within different administrative spheres, both dismantling and creating new channels for the exclusion of citizens.
The main objective of this study is to explain access to and use of the main eHealth tools through various sociodemographic factors. To achieve this, it aims to identify the variables that significantly determine the probability of engaging with these electronic services in Spain.
This study addresses a significant gap in the literature on eHealth in Spain. There is a shortage of studies based on nationally representative data that evaluate the use of eHealth services in the post-pandemic context. The accelerated digitalisation of the healthcare system during COVID-19 has transformed access to key services, such as digital medical records, electronic prescriptions and digital certificates. This transformation may have contributed to widening the digital divide between different social groups.
This work, based on the Health Barometers published during 2024 by the CIS, contributes to filling this empirical gap and proposes a multidimensional approach, allowing to observe the simultaneity of social factors concerning the use and access of eHealth. Based in the above, this study establishes the following research question: Do sociodemographic factors significantly predict the likelihood of accessing and using eHealth tools in Spain?
Methodology
The quantitative methodology employed in this article draws on the Health Barometer 2024 databases, published by the CIS in several waves throughout 2024. The questionnaires were administered via computer-assisted telephone interview (CATI). To conduct this study, the three databases from each wave—comprising 7623 cases—were pooled into a single dataset using simple random sampling, ensuring a 95.5% confidence level and a ±1.1% sampling error. The sampling procedure, which is essential for more accurately reflecting the surveyed population, incorporated sex and age quotas consistent with Spain's 17 autonomous communities and two autonomous cities.
The CIS-provided population weighting factor was applied to the combined dataset to preserve representativeness. According to the CIS methodological report, the combined identified in the key study variables.
Based on these data, this research aims to study whether the different sociodemographic variables, especially gender and age, can predict the use or non-use of the different eHealth tools present in the National Health System (hereinafter, NHS). Different binary logistic regression models were conducted due to the inherent properties of the available survey questions. The aim was to establish a correlation between factors that could potentially impact the increase in the digital divide with regard to eHealth services and tools. This technique was also chosen given the dichotomous nature of the dependent variables, the availability of the data, and the interpretability of the results. Thus, the following sociodemographic variables were selected (see Table 1): gender, age, place of residence, education, income, social class, employment status, nationality, health status, and chronic illness. It should be noted that all stratification variables have undergone an additional recoding process, transforming them into dummy variables—0 ‘absence of condition’ and 1 ‘presence of condition’—to adjust them to binary logistic regression models. However, the variables gender—0 ‘female’ and 1 ‘male’—and chronic disease—0 ‘no’ and 1 ‘yes’—have not undergone this recoding, as they are dichotomous variables in origin.
Recoded variables.

Source: Prepared internally based on Health Barometers (2024).
At the same time, six eHealth-related variables have been selected. The first four are related to DHR: access to this tool; main reasons for not using the DHR: knowledge about the existence and access to DHR; knowledge and ability to use Internet; and necessity percept. Next, about electronic prescriptions, question if people take medicines outside their autonomous community. The last of the variables, to determine entry to these services, was whether they use the digital certificate to carry out administrative procedures. It should be noted that all eHealth variables are dichotomised between ‘yes’ and ‘no’ responses.
With this selection of variables, this research focuses on analysing the relationship between the different stratification variables and those corresponding to eHealth collected by the health barometers. Thus, the analytical procedure to be followed will be that of a binary logistic regression analysis.70–72
In this case, the different models are set at a 95% confidence level, under the objective of studying whether these social and economic factors can predict the use of eHealth tools.
Statistical analysis
Following the methodology, this section outlines certain issues related to the statistical analysis of this research. First, to explore the relationship of dependence between the different dependent variables, a bivariate correlation analysis was performed using Spearman's coefficient. This test revealed various associations which, although statistically significant, illustrate low to moderate magnitudes in terms of issues such as access to the DHR, knowledge of it, and use of the electronic certificate (see the Supplementary Material). These correlations indicate that, even with the existence of a certain interdependence, each variable represents a distinct model, justifying its separate structuring within the analytical framework.
With the binary logistic regression analysis, six different models were collected, the results of which are distributed across three graphical elements. The first of these, corresponding to the ‘Model Summary’, contains the main statistics obtained, which provide an overview of each of the analyses performed. This section presents different pseudo R2 values—McFadden's R2, Cox and Snell's R2, Nagelkerke's R2 and Tjur's R2—which are key measures for assessing the degree of fit of the model to the data.
Next, the ‘Model Coefficients’ table is detailed, intended to indicate the different strength of the independent or predictor variables on the dependent variable. In this case, a series of statistics that are decisive for the statistical analysis are included, such as the Beta estimator (B), in addition to the level of significance—identified by asterisks—such as the standard error or the Z and Wald statistics.
Similarly, to complete the coefficient table, a graphical representation is included using forest plots. These plots show the odds ratios, which are essential for interpreting the models.
Finally, the appendices provide other information that is essential for the validity of the different models. This section includes criteria such as the Hosmer-Lemeshow Test, which indicates issues such as the level of significance, the Chi-Square statistic and the degrees of freedom of the model. In addition, the Omnibus Plausibility Ratio Test and the VIF (Variance Inflation Factor) statistic are detailed, which are used to detect possible multicollinearity in the models created, as well as their robustness.
Results
The findings obtained through the corresponding binary logistic regression analyses are shown below. It should be noted that different asterisks are used in the graphical representation, which follow the following logic: *** for a significance level of 1% (α = 0.01) and ** for 5% (α = 0.05), so that the models presented include those variables that are significant at a confidence level of 95%. At the same time, this graphical representation is accompanied by the different forest plots used to provide a better illustration of the odds ratios for each of the binary logistic regression models.
On the other hand, and before analysing the different models, it should be noted that all of them are free of multicollinearity, as shown by the VIF statistic, demonstrating solid robustness in all the studies carried out. Furthermore, they are also adjusted to the data, as determined by the Hosmer-Lemeshow statistic (see Supplementary Material).
The first of the analyses is for access to the DHR via the Internet, where this regression model achieves a Nagelkerke R2 of 0.112 (11.2%)—R2McF (6.42%); R2CS (8.35%) and R2T (8.07%). As indicated in Table 2, all of the resulting variables in the model are significant at a 99% confidence level, except for people with income between €1801 and €2700 (p = 0.011), which is significant at 95%.
Binary logistic regression model of access to DHR

Source: Prepared internally based on Health Barometers (2024)
Binary logistic regression model for not accessing DHR because I was unaware of that possibility

Source: Prepared internally based on Health Barometers (2024)
In relation to the variables exhibiting a negative B coefficient, as well as the odds ratios are found to be less than one—which indicates a decline in probability of access to the DHR—the following factors were identified: basic (−1.582; 0.21), secondary (−0.659; 0.52) or intermediate (−0.257; 0.77) studies; with an income of less than €1.100 (−0.748; 0.47) or between €1100 and €1800 (−0.413; 0.66); with other nationality (−0.440; 0.64); over 65 years old (−0.537; 0.58); and residents in municipalities of between 10,000 and 100,000 inhabitants (−0.151; 0.86).
On the other hand, the sociodemographic factors that increase the probability of accessing this service are those related to employment status—scientific or intellectual (0.214; 1.24)—and having a chronic illness (0.358; 1.43) (Figure 1).

Forest plot for Model 1. Source: Prepared internally based on Health Barometers (2024).
Continuing with the battery of questions relating to DHR, Table 2 shows the response to the question about not knowing about this health service. With regard to Nagelkerke's R-squared, this model has a value of 0.131, meaning these sociodemographic variables account for 13.1% of the model's explanatory power—R2McF (7.63%); R2CS (9.60%) and R2T (9.39%).
As for the level of significance, this model is again divided between variables that have a 95% confidence level—gender, income of less than €1100, administrative technicians, dual nationality and the possession of chronic diseases—and those that are admitted with a 99% confidence level.
Thus, among the variables that show a lower probability of access: are being over 65 (−1.394; 0.25) and between 50 and 64 (−0.633; 0.53); basic (−0.679; 0.51) or secondary (−0.379; 0.68) education levels; with income lower than €1100 (−0.267; 0.77); and being male (−0.169; 0.84).
The model indicates a higher probability of knowing about this possibility among unemployed people (0.389; 1.48), salespeople (0.322; 1.38) or administrative technicians (0.257; 1.29); with dual nationality (0.319; 1.38); and with chronic illnesses (0.182; 1.20) (Figure 2).

Forest plot for Model 2. Source: Prepared internally based on Health Barometers (2024).
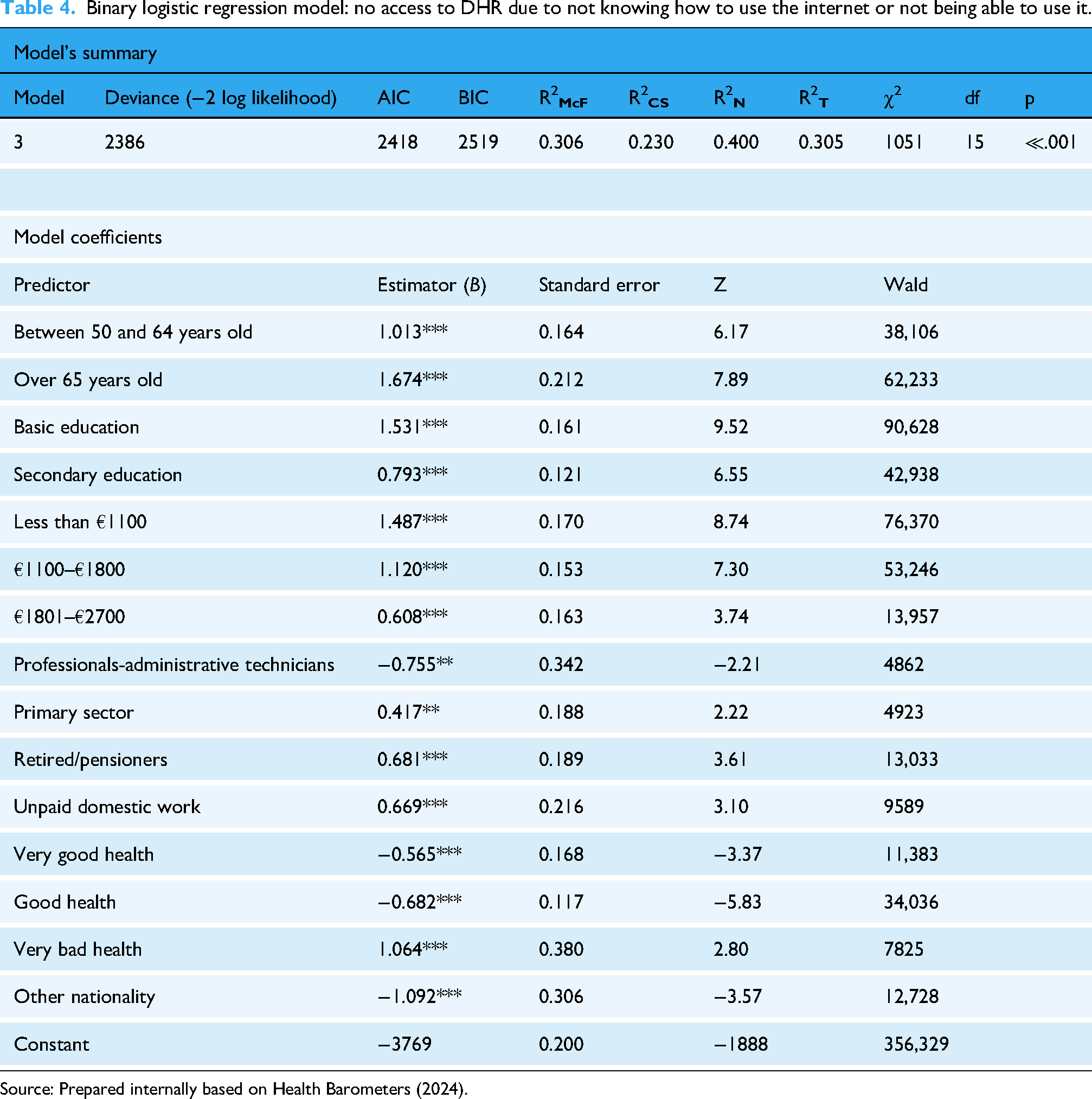
Continuing with the models, a Nagelkerke R2 value of 0.400 was obtained (see Table 4), which explains a 40% of the variance in not accessing the DHR due to not knowing or not being able to use the internet—R2McF (30.6%); R2CS (23.0%) and R2T (30.5%).
Binary logistic regression model: no access to DHR due to not knowing how to use the internet or not being able to use it.
Source: Prepared internally based on Health Barometers (2024).
All variables in this model, except for administrative technicians, in the primary sector and with a poor health status (sig. = 0.05), are at a 99% confidence level.
Thus, the variables with a negative B coefficient and below one in the forest plot are those related to health status—very good (0.565; 0.57), and good (−0.682; 0.51), fair (−1.078) and bad (−0.982), having other nationality (−1.092; 0.34) and being an administrative technician (−0.756; 0.47).
In terms of the variables that increase the probability of not accessing the DHR due to not knowing or not being able to use the Internet, the following are noted: people over 65 (1.676; 5.33) or between 50 and 64 (1.013; 2.75); having a basic (1.531; 4.62) or secondary (0.794; 2.21) level of education; earn less than €1100 (1.484; 4.42), €1.100–€1800 (1.120; 3.06) or between €1801 and €2700 (0.609; 1.52); perceive a very bad health (1.064; 2.90) as well as being a pensioner (0.679; 1.98), an unpaid domestic worker (0.667; 1.95) or employed in the primary sector (0.414; 1.52) (Figure 3).

Forest plot for Model 3. Source: Prepared internally based on Health Barometers (2024).
The model, corresponding to non-use of DHR based on not having needed this service (see Table 5), indicates a Nagelkerke's R2 of 0.051, so the selection of sociodemographic questions has explained 5.1%—R2McF (2.79%); R2CS (3.79%) and R2T (3.80%). All variables in the model are significant at a 99% confidence level.
Binary logistic regression model for not accessing DHR due to not needing that service.

Source: Prepared internally based on Health Barometers (2024).
A lower probability of needing this service is shown by those with a basic level of education (−0.514; 0.60), a chronic illness (−0.376; 0.69), an age between 18 and 34 years (−0.311; 0.73) and being male (−0.215; 0.81).
On the other hand, people who report a greater need for DHR are students (0.707; 2.03), in very good (0.516; 1.68) or good (0.321; 1.38) health, aged over 65 (0.390; 1.41) or between 50 and 64 (0.345; 1.48) and middle class (0.192; 1.21) (Figure 4).
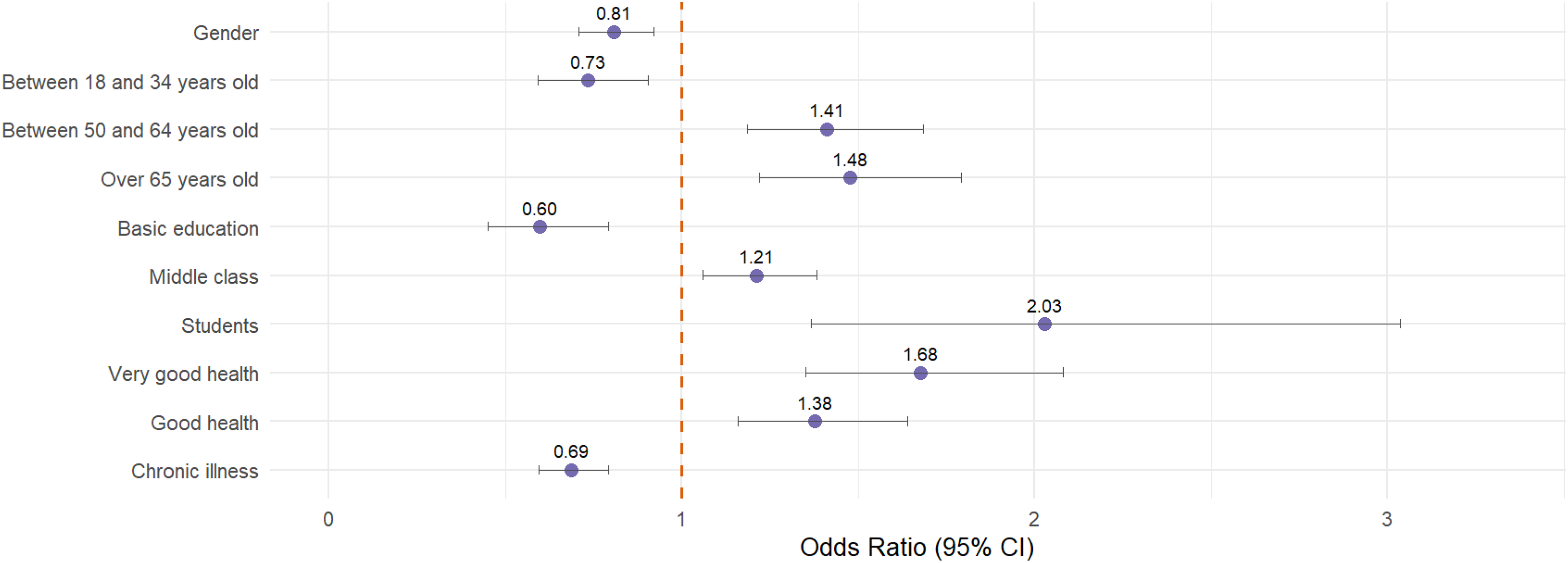
Forest plot for Model 4. Source: Prepared internally based on Health Barometers (2024).
Changing the focus to electronic receipts, explanation of e-prescribing use outside the autonomous community indicates a Nagelkerke R2 value of 0.036, which corresponds to an explanation of 3.6% of the phenomenon by the selected variables—R2McF (2.00%); R2CS (2.72%) and R2T (3.63%) (see Table 6).
Binary logistic regression model of the use of electronic prescriptions outside one's autonomous community.

Source: Prepared internally based on Health Barometers (2024).
In this sense, the confidence level is 95% for the variables of sex, residing in a municipality of less than 2000 inhabitants and level of education—basic and secondary. The rest of the model shows a confidence level of 99%.
Thus, the variables with negative coefficients are grouped around place of residence—less than 2000 (−0.440; 0.64), between 2000 and 10,000 (−0.472; 0.62), between 10,000 and 100,000 (−0.507; 0.60) and between 100,000 and 400,000 inhabitants (−0.518; 0.60), level of education—basic (−0.360; 0.70) and secondary (0.175; 0.84), class—low (−0.403; 0.67) and medium (−0.390; 0.68)—and having other nationality (−0.421; 0.66).
Of the variables in this model, only two have positive coefficients: being chronically ill (0.503; 1.65) and being female (0.134; 1.14) (Figure 5).

Forest plot for Model 5. Source: Prepared internally based on Health Barometers (2024).
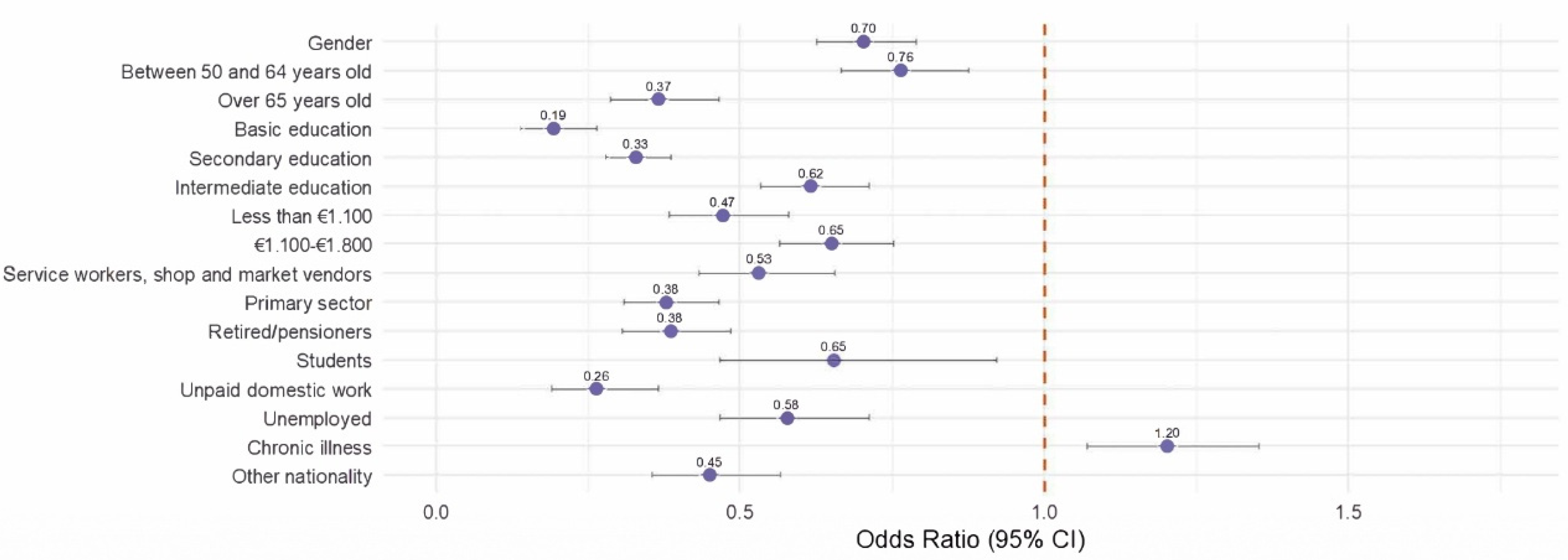
The last of eHealth-related variables is the use of a digital certificate. In the final model, a Nagelkerke R2 of 0.307 was obtained, representing an explanation of the phenomenon at 30.7%—R2McF (19.2%); R2CS (22.6%) and R2T (24.2%).
For this model (see Table 7), a 99% confidence level was obtained for all variables, except for the option of being a student, where 95% was reached (p = 0.014).
Binary logistic regression model of digital certificate usage.

Source: Prepared internally based on Health Barometers (2024).
Among the variables that showing a lower probability of not using this tool are people with: basic (−1.645; 0.19), secondary (−1.114; 0.33) or intermediate (−0.485; 0.62); in an employment situation of unpaid domestic work (−1.330; 0.58 and 0.26), in the primary sector (−0.969; 0.38), pensioners (−0.955; 0.38), service workers (−0.632; 0.53), unemployed (−0.552; 0.58), students (−0.427; 0.65); other nationality (−0.802); over 65 (−1.006; 0.37) or between 50 and 64 (−0.271; 0.76); with income below €1100 (−0.753; 0.47) and between €1100 and €1800 (−0.431; 0.65); and male (−0.354; 0.70).
The only variable that increases the probability of using electronic prescriptions is having a chronic illness (0.185; 1.20) (Figure 6).
Forest plot for Model 6. Source: Prepared internally based on Health Barometers (2024).
In summary, Table 8 is added as a guide for interpreting the different odds ratios collected in the six models. This figure ranks all the factors that have proved significant in the models in order of importance and presence, from highest to lowest. It should be remembered that values below 1 indicate a lower probability, while those above 1 indicate a higher probability of occurrence.
Summary of variables, models and odds ratios.

Source: Prepared internally based on Health Barometers (2024).
Educational level emerges as the most consistent determinant: basic education appears in all six models and secondary education in five, associated with lower probabilities of access (odds ratio well below 1). Age-related factors also have a significant influence, as people over 65 are present in five models and those between 50 and 64 in four, again indicating a lower probability of accessing services. Income brackets below €1100 and between €1100 and €1800 repeatedly appear as negative predictors. In addition to the above, there are three other factors that appear predominantly in the models: having a chronic illness, having another nationality, and gender.
Discussion of results
Taking into account the results presented and the explanatory capacity of the different models, some of the points raised by academic literacy have gained relevance. The stratification variables collected in this analysis would reveal the predictive value for some of the eHealth tools. Issues such as not accessing the DHR due to not knowing or not being able to use the Internet (40% explanation) or the (non)use of the digital certificate (30.7%) are subject to the influence of different sociodemographic factors. In contrast, issues such as not needing the DHR (5.1%) or the use of electronic prescriptions outside the autonomous community (5.1%) are less influenced by these factors. As indicated by these models, the influence of different variables on eHealth services within the Spanish NHS would not be uniform; disparities have been identified in the extent to which they contribute to predictions and their relative influence.
Following the two variables that underpin the initial approach, age and gender, divergent results were found. Therefore, age is a key factor in determining who is excluded from eHealth services in Spain. In particular, people over 65 years are the most affected showing a lower probability of access in the DHR, being especially relevant in the reason for not accessing this service for not knowing about this possibility and in the use of the digital certificate. At the same time, there are values that reflect a greater probability of not accessing the DHR because of not knowing or not being able to use the Internet or not needing it. This reflects the trend indicated by the literature, 73 articulating a digital-generational divide,43,44 where older people are less likely to have access to the NHS e-services network.
Although older people are aware that they need this eHealth tool, they do not access it, perhaps not because they do not want to, but because they cannot. On the one hand, this could be due to a digital skills gap to use these services independently. On the other hand, it may be due to the lack of mechanisms and measures available from the public administration to ensure the inclusion of this group. For instance, use could be increased through more accessible design and easier access to digital identities supported by public administrations. Broader digital health policies should also aim to ensure equitable access for all users.9,44
In terms of gender, the results show that this factor is present in four out of six models. In these scenarios, men are less likely to use certain digital health services, or at least demonstrate less interest in them, even when they are aware of their existence. Specifically, men report greater familiarity with services such as the DHR, less frequently mention feeling the need to access their DHR, more often use prescriptions outside their autonomous community, and are also less likely to use digital certificates.
These results are consistent with the different ways in which men and women use eHealth services, with men being less likely to use them (although there are some exceptions relating to situations in which they work/live outside their home autonomous community). Thus, this pattern may be related to the prospect of the care sector becoming more female-dominated, 46 a role which has traditionally been assumed by women, who are responsible for managing family health. 63 This aspect is reflected in the fact that women are more likely to use electronic certificates, which can be associated with caregiving and an advanced use of services (with a bigger level of security but also more utilities and with access to specialised services or sensible information) and may reinforce their role as ‘managers’ of family health.
In this sense, incorporating other sociodemographic variables into regression models highlights the multidimensional and intersectional nature of the digital divide74–76. Its many facets affect potentially vulnerable groups in different ways. Thus, factors such as educational level, income level, employment status, nationality or health status are identified as key determinants of the digital divide.
Starting with educational level, people with basic education are less likely to use eHealth services, particularly DHR and electronic certificates. They had also a higher probability of not knowing about the DHR or of not knowing or being able to use the Internet. These results emphasise the link between digital literacy and digital capital 77 and highlight the crucial role of digital skills plays in facilitating the transfer of technological knowledge, which is essential for engagement with eHealth services. 78 Consequently, a lack of basic competences amplifies the digital divide among less educated groups.
In turn, the economic issue also shows a lower likelihood of using electronic tools, conditioning access to them due to a lack of resources. This makes it difficult to acquire the necessary technological devices and therefore to access eHealth services. 79 Employment status is also a major determinant affecting access to eHealth. People who are unemployed, retired, in primary occupations or in unpaid domestic work are less likely to use digital tools. Conversely, occupations in technical, administrative or scientific fields are associated a with higher probability of access. Hence, a lack of labour market integration in certain positions can result in lower access to eHealth tools and hinder the development of digital competencies acquired in work environments supportive to technological change. 52
When it comes to nationality, people with other nationality are less likely to access the DHR or to use electronic prescriptions outside their autonomous community, but especially the digital certificate. In this sense, certain language-related difficulties could be related. As Thonon et al. 80 point out, migrants are likely to receive poorer medical care, have longer and less satisfactory consultations and experience worse clinical outcomes.
With regard to health status, following Lupton's concept of the digitised healthy citizen suggest that differences are reflected in self-perceived health status and the presence of a chronic illness. 29 Thus, people's self-image, especially those with positive views, indicates a lower likelihood of not requiring the DHR. Conversely, people with chronic conditions are more likely to use both the DHR and the electronic prescription, indicating a greater presence in the eHealth circuit. On the other hand, the most positive perceptions are less focused on the use of these tools and may rely on other digital media to support their assessment of their health status. 29
Finally, it should be noted that the results show an ascending logic in terms of place of residence, in that e-prescription use—outside the autonomous community—is less common among populations with more residents compared to those with fewer inhabitants. This contrasts with the literature trend65,81 of identifying this factor as a variable that could lead to digital divide. Consequently, these challenges the idea that rural areas are mostly situated in this situation of vulnerability. What could be happening is that people living in areas with fewer than 400,000 inhabitants travel less between autonomous communities than those living in urban centres. This would lead to a lower need for this service in municipalities with fewer than 400,000 inhabitants. However, there do not appear to be any significant disparities between urban and rural areas beyond those mentioned above.
Limitations
While this study provides a rigorous quantitative analysis of the sociodemographic determinants shaping digital divide in eHealth within Spain, several methodological constraints should be acknowledged.
The first limitation concerns the cross-sectional design of the research. Since the data were collected at a single point in time from the 2024 CIS Health Barometer, the study can only establish associational, not causal, relationships between variables. As this is not a longitudinal study, changes over time cannot be evaluated, which is especially relevant in the wake of COVID-19. Therefore, conclusions regarding the expansion of digital divides or the broader effects of digitalisation should be interpreted with caution.
A second limitation relates to the self-reported nature of the survey data. Although the dataset is nationally representative, responses based on participants’ perceptions may be affected by recall and social desirability bias, potentially leading to overestimations of access to or use of eHealth tools.
Additionally, the CIS dataset does not include psychological or attitudinal variables—such as digital anxiety, perceived usefulness, or privacy concerns—that could offer valuable insights into individual-level barriers to digital engagement. The absence of these dimensions restricts the interpretative depth of the analysis, preventing the measurement of issues such as digital literacy and people's motivation regarding the use of eHealth. The inclusion of questions such as this in future surveys would help to complete the analysis and understanding of the phenomenon.
A further conceptual limitation relates to the interpretation of gendered patterns in eHealth engagement. Although the study appropriately refers to the notion of the ‘feminisation of care’ to explain women's higher use of electronic prescriptions, the dataset does not allow for distinguishing between personal use and proxy use (for example, managing prescriptions for children, partners, or elderly relatives). The same applies to other moderating or mediating factors associated with gender differences, such as digital self-efficacy, social norms, or institutional design. Given this data constraint, our discussion relies on previous literature to hypothesize potential explanations. Future research should explicitly address this distinction to deepen the understanding of how gendered shape digital health practices.
From a methodological perspective, the study also faces constraints in regional representativeness. Due to the considerable heterogeneity across Spain's 17 autonomous communities and the limited availability of disaggregated data, it is challenging to obtain sufficiently large and balanced regional samples. Consequently, single-level logistic models could not account for potential intra-regional clustering or policy-specific effects.
This study acknowledges the methodological limitations of applying intersectionality to quantitative models. Although our findings identify sociodemographic factors that often coexist in the same individuals—for example, being an older woman with low income and limited education—which reinforces the relevance of an intersectional perspective, we recognise that our statistical approach cannot fully capture the complexity of intersectional experiences. To address this issue, future research should consider adopting designs that allow for a more comprehensive understanding of intersectionality in the field of health.
Finally, the quantitative nature of this research limits the interpretative depth of its findings. Future studies should combine quantitative and qualitative approaches to explore the lived experiences of digitally excluded populations and to provide a more comprehensive understanding of the mechanisms sustaining digital inequality in health.
Conclusions
This work has identified how different groups are less likely to use the various eHealth services available in the Spanish healthcare system by exploiting the databases of the Health Barometers published by the CIS throughout 2024. The main conclusions of the study are outlined below.
Throughout the course of this research, binary logistic regression analysis was employed to formulate a series of models, thereby indicating the impact of a variety of sociodemographic factors on the utilisation of diverse eHealth tools. Thus, this study demonstrates the strength of these variables in terms of use and knowledge of eHealth tools, while also establishing hypotheses highlighted in recent literature. At the same time, the study sheds light on Spain's specific characteristics and illustrates the social groups most affected by the digital divide.
First, the eHealth services and tools identified in the opinion surveys show different trends in terms of their usage. Of the six models analysed, it is those most closely linked to digitalisation—namely, not accessing the DHR due to a lack of internet access or digital literacy, and not using the digital certificate—that are most explained by sociodemographic factors. Thus, two main barriers to accessing eHealth are identified: not having a certificate or access to the Internet. This means that certain groups are unable to take advantage of eHealth tools.
While it is found that both age and gender are significant factors, this study specifies how these inequalities manifest in Spain. Age has been confirmed as one of the main drivers of digital divide. People over 65 are less likely to have access to digital services, which restricts their access to health services and can lead to feelings of disempowerment and exclusion.
In terms of gender, men are less likely to use certain digital services. In contrast, women, traditionally linked to the role of carer, tend to make greater use of tools such as electronic prescriptions. The feminisation of caregiving could mean that women play a greater role in managing their families’ health. This could explain why they use certain eHealth services more often, not for themselves, but for their descendants, ancestors or partners—a role they traditionally fulfil, which affects family health dynamics in other EU welfare states.46,63 In addition, there are other factors that could be mediating these differences, such as digital self-efficacy, social norms or institutional design, which would need to be addressed in future research.
Furthermore, this study reiterates the need to examine digital divide from an intersectional perspective, recognising that multiple dimensions of inequality are interconnected. The relationship with these digital services is not only conditioned by age or gender, but also by their combination with other factors such as educational level, income, employment situation or health status. Those with lower levels of education, low incomes and/or precarious or no employment are less likely to access digital health services. People of other nationality are also likely to be in this situation, which could be related to barriers that are not only technological, but also linguistic, cultural and structural.
Although place of residence has an influence, its impact on this analysis is less significant than expected. This study reveals that certain urban areas have limitations regarding the use of e-prescriptions, prompting a rethink of the territorial dynamics of digital divide.
This study highlights that the digitalisation of Spain's healthcare system, if not guided by equity principles, may reinforce existing social inequalities. To ensure inclusive digital transformation, the findings of this study should be taken into account in order to anticipate critical factors in the design. Public policies and policymakers should address the structural and individual barriers identified in the analysis. Developing age-friendly and cognitively accessible digital interfaces would reduce these barriers and foster trust among older users. Similarly, educational and income inequalities strongly shape access to digital health services. Embedding digital literacy programs in primary care and community settings can strengthen digital skills among socioeconomically disadvantaged populations, where access barriers are most acute. Also, the lower engagement of other nationals in eHealth underscores the need for multilingual portals and culturally tailored support mechanisms to overcome linguistic and cultural barriers.
Overall, the results reinforce the idea that the digital divide in health cannot be understood as an isolated phenomenon, but rather as another manifestation of existing social inequalities. If inclusive policies that consider the diversity of the population are not designed, eHealth may be reproducing or even amplifying these inequalities.
Upcoming studies should build on this investigation by adding a more qualitative element that thoroughly documents the groups’ experiences with eHealth tools. This is particularly relevant given that administrations are currently in the midst of the fourth technological revolution (bigdata, AI, IoT technology, robotics), the effects of which are yet to be measured, while public data and surveys do not pay sufficient attention to this issue. In short, this study shows that the digitalisation of the healthcare system is characterised by social inequalities that influence access to and use of eHealth tools. The main exclusion factors identified in Spain, such as age, educational level, economic resources and employment status, reflect classic forms of exclusion and the common challenges of digital inclusion efforts at a European level. Furthermore, the identified services largely correspond to the most basic and essential elements of public eHealth models. This means that the Spanish case could potentially be generalised to a European framework focusing on models such as DIGCOM and the SDGs.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076251414467 - Supplemental material for Digital divide in eHealth: Sociodemographic determinants of access in Spain
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076251414467 for Digital divide in eHealth: Sociodemographic determinants of access in Spain by Antón Lodeiro-VÁzquez, Bran Barral-Buceta and Irene Loureiro-Álvarez in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to express their gratitude to the CIS for making the various Health Barometer databases freely available.
Ethics approval and consent
Ethical approval is not applicable as all data are derived from publicly available sources.
Author contribution(s)
All authors contributed equally to the development of each phase and section of the article, from its conception and execution to the analysis of results and conclusions.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. Funding for this research was provided by Convocatoria Consolidación 2025 GPC. Xunta de Galicia, Consellería de Educación, Ciencia, Universidades e Formación Profesional Research Group ISOPOLIS (GI-2142) and ‘Knowledge Generation Projects’ of the State Research Agency (AEI/10.13039/501100011033/ ERDF, EU – Identification N°: PID2022-138892OB-I00).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data can be accessed in the public repository set up by the CIS, where it is available to consult without restriction. Access to the aforementioned links is permitted via the following URLs:
Supplemental material
Supplemental material for this article is available online.