
Abstract
Objectives
Digital health interventions offer promising avenues for enhancing health outcomes, the quality of life, and social participation among individuals with disabilities. This study aimed to evaluate the impact of these interventions on individuals with disabilities.
Methods
This study began with a comprehensive search of several electronic databases and the grey literature in hopes of selecting primary qualitative and quantitative studies that examined digital health interventions for individuals with disabilities. Our analysis categorized outcomes into health improvements, quality of life enhancements, and increased levels of social participation.
Results
Measures of the quality of life revealed enhancements in emotional, cognitive, and physical well-being, as well as reductions in pain and increases in the efficiency with which daily activities were accomplished. In terms of social participation, digital health interventions fostered stronger relationships and heightened levels of social engagement. Secondary outcomes of the study spotlighted user satisfaction and concerns with digital tool usability. However, design and user features, such as ease of use and privacy, influenced tool effectiveness. The results suggested that digital interventions, especially when paired with emerging technologies such as virtual reality and machine learning, have the potential to be engaging and effective. The research prioritized primary, empirical, and quantitative studies in setting up a solid foundation of data and ensuring minimal bias. However, the diversity of the studies reviewed made a meta-analysis challenging because the studies focused on various disabilities, interventions, and outcome measurements.
Conclusion
The nascent field of digital health would benefit from research with narrowly targeted goals, particularly research emphasizing societal participation for disabled individuals.
Keywords
Introduction
A disability is a condition characterized by reduced function due to the presence of a disease, disorder, injury, or other health issue. It may manifest as an impairment, restriction of activities, or limitation of participation. 1 The World Economic Forum (2021) estimated that 1.3 billion people, or 17% of the world's population, live with a disability, with most being visual, hearing, cognitive, speech, mobility, or neural impairments. 2 It is estimated that approximately 64 million people will have disabilities in the United States by 2025. 3 Individuals with disabilities face different challenges as they attempt to attain and maintain healthy outcomes and become integrated into society. 4 This implies they will likely need unique tailored interventions to improve their health outcomes while achieving an improved quality of life.
People with disabilities experience disproportionate levels of social exclusion compared with non-disabled compatriots.5,6 Digital health interventions may increase this group's empowerment and inclusion. The potential value of digital health interventions to increase access to healthcare is another area in which these technologies can bridge the gap created by the social exclusion of people with disabilities. Digital health was defined by Mesko et al. as “the cultural transformation of how disruptive technologies that provide digital and objective data accessible to both caregivers and patients leads to an equal level doctor-patient relationship with shared decision-making and the democratization of care.” 7 Telehealth technologies are one of the digital health interventions that have made it easier for people with disabilities to access quality care for mental health. 8 Previous studies have demonstrated the viability of digital health interventions among people with disabilities when they are provided in the right environments. 9 However, it is essential to acknowledge the complexity and heterogeneity within and between different groups of people with disabilities.
The COVID-19 pandemic highlighted significant issues of digital poverty, literacy, and exclusion for people with intellectual disabilities, with many experiencing reduced services, loneliness, and impoverished daily lives. While digital solutions like videoconferencing helped ameliorate some challenges, sociopolitical and structural barriers persisted, and despite an increased awareness of digital exclusion, substantial actions and changes that could eradicate digital poverty remained insufficient. 10 Similarly, the disability digital divide varied across different disability groups, with various studies highlighting specific challenges faced by each group. For instance, Lussier-Desrochers et al. studied the disability digital divide, particularly focusing on intellectual disabilities. 11 The study identified five key challenges or conditions associated with digital inclusion for people with intellectual disabilities, including access to digital devices, sensorimotor abilities, cognitive and technical requirements, and comprehension of codes and conventions. Through a qualitative analysis of scientific publications, the study elucidated obstacles and facilitators within each challenge area, ultimately proposing a model in the shape of a gear to conceptualize the interplay between individual resources and environmental support in promoting digital participation for individuals with intellectual disabilities.
Digital technologies have been widely used in healthcare to improve healthcare outcomes. 12 One commonly used framework is the “Digital Health Taxonomy” developed by the World Health Organization (WHO). This taxonomy categorizes digital health interventions into various domains, such as health information systems, telemedicine, mHealth, health information management systems, and digital health interventions for persons, health providers, and health managers.13,14 The use of these digital health interventions to address the unique needs of people with disabilities is an area of interest. The overlap between well-being and quality of life lies in the shared focus on aspects such as physical health, psychological well-being, social relationships, and overall life satisfaction. 15
The rapid growth of technology and its integration into the healthcare sector has brought forth a breakthrough of digital health tools aimed at improving the well-being and health of individuals across various strata. A particularly important subset of the population that stands to benefit immensely from these advancements is individuals with disabilities. They can expect enhanced access to healthcare services, personalized support, and the implementation of innovative assistive technologies tailored precisely to their unique needs, thereby fostering an improved quality of life and autonomy. 16 For our research objectives, we used the WHO definition of health, emphasizing physical, mental, and social well-being. 17 Well-being encompasses psychological, physical, and social aspects that are relevant to life satisfaction and emotional balance. 18
This study aimed to comprehensively assess the digital health interventions developed specifically for individuals with disabilities. The primary objective was to determine the range of digital health interventions developed for individuals with disabilities and to understand their impact on health outcomes, the quality of life, and social participation.
This study was necessary to fill the gap in the current research related to the effectiveness of digital health interventions tailored for individuals with disabilities, a group often overlooked in healthcare innovation. The novelty of this research lies in its comprehensive evaluation of diverse digital health strategies and their impacts on health outcomes, the quality of life, and social participation for this heterogeneous population. The main outcomes include tangible health improvements and enhancements of the quality of life, while the secondary outcomes focus on social participation and user satisfaction.
Methods
The research question
Primary research question
The primary research question had two parts: Which digital health interventions and strategies have been explicitly developed for individuals with disabilities? Moreover, how well do these interventions translate into tangible health outcomes?
Secondary aims
Beyond its focus on health outcomes, this research also explored the broader impacts of digital health tools, particularly emphasizing their role in promoting social participation for individuals with disabilities. Understanding how technology can mitigate feelings of isolation or exclusion is essential, and this aspect was reframed as a key contributor to the overall well-being of this population.
Protocol and registration of the study
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used in this systematic review to guide article selection and screening. 19 The protocol was registered at the online database of PROSPERO (accession number CRD42024522671).
Search strategy
Articles from electronic databases and libraries were systematically searched using selected search criteria. The databases and libraries that were searched were Google Scholar, PubMed, and Cochrane Central Register of Controlled Trials between January 2013 and June 2024. The search prioritized quantitative randomized controlled trials (RCTs), but it also included other article formats, such as cross-sectional studies and experimental research studies examining digital health interventions' impact on people with disabilities. Other sources outside of these databases and libraries were identified, as well. In performing the search, keywords and Medical Subject Headings (MeSH) in English were used, such as “digital health technologies,” “digital health interventions,” “telehealth,” “persons with disabilities,” “quality of life,” “healthcare outcomes,” and “social participation” (Supplementary File 1). All of the identified studies were summarized in a Microsoft Excel file. Details such as the author's name and location, article's year of publication, and sample variables and measured outcomes described in the article were summarized in the document for analysis.
Eligibility criteria
Digital health, as a broad and rapidly expanding field, has produced a vast and diverse range of publications. However, when focusing specifically on digital health interventions for individuals with disabilities, the scope of relevant studies tends to be more limited. This limitation is due to the unique challenges and specific needs of this population, which are not always addressed in the general digital health literature. To ensure the relevance of the systematic review, we applied specific inclusion and exclusion criteria. We prioritized studies that directly assessed the impact of digital health interventions on key outcomes such as health outcomes, quality of life, and social participation. These outcomes were chosen because they effectively represent of the effectiveness of digital health interventions in the context of disability.
Studies were included if they (a) investigated the impact of digital health interventions on individuals with disabilities; (b) the studies had to demonstrate how digital technologies impacted the dimensions of health outcomes, quality of life, and social inclusion of people with disabilities; (c) were published from January 2013 onward to capture the recent developments in the field (d) were in English, and adopted various research designs such as RCTs and case reports (Table 1).
Criteria for inclusion and exclusion in the review of studies focusing on digital technologies for people with disabilities.

Exclusion criteria were applied to studies that (a) did not involve digital interventions (e.g. traditional health interventions). (b) Did not measure outcomes related to health, quality of life, or social participation. (c) Focused on non-human participants or were purely theoretical in nature. (d) Were published before January 2013 or were not available in English.
Qualitative studies were selected based on their methodological alignment with our objectives, specifically, those employing thematic analyses or cross-sectional designs. The aim was to capture diverse perspectives and in-depth insights into digital health and disabilities, which were essential for addressing our research questions.
Quality assessment
The risk of bias in the included RCTs was assessed using the Cochrane Collaboration's Risk of Bias 2 (RoB 2) tool. 20 The following domains were evaluated: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was rated as having a “low risk,” “some concerns,” or a “high risk” in terms of bias, and an overall risk of bias judgment was provided for each study. We used the National Institutes of Health (NIH) tool for both case series and single-arm studies. 21 Finally, we used the Critical Appraisal Skills Program (CASP) for qualitative studies. 22
Data extraction and synthesis
Data from the eligible articles were extracted and summarized in Microsoft Excel by two authors, with any discrepancies resolved by a third author to ensure accuracy and consistency in the extraction process. The summarized data included the author's name, article's year of publication, study type and the study outcomes. The summary of procedures is provided in the PRISMA flow diagram (Figure 1).

PRISMA flow diagram for study selection on digital health interventions. A flowchart illustrating the step-by-step process of identifying, screening, and including studies in a systematic review on digital health interventions.
Results
Study selection
The databases, libraries, and other reference sources were searched from January 2013 to June 2024. From the search, a total of 441 articles that initially identified the use of digital technology interventions among people with disabilities were investigated. The researchers excluded 121 articles that were found to be duplicates in the preliminary screening. Additionally, 240 articles were eliminated during title and abstract screening for non-relevance and a failure of focus on the research topic. During the full-text screening of the remaining 80 articles, 74 were eliminated for having a limited focus on the targeted outcomes. Specifically, these studies did not address health outcomes, quality of life, or social participation as primary or secondary outcomes. The remaining 6 articles were included after the screening and elimination. Three articles were added after reference list searching, and one study was added during manuscript revision. Figure 1 shows the PRISMA diagram representing the identification, screening, and inclusion processes used in the study.
Quality assessment
Regarding the included RCTs, three studies were judged as having an overall low risk of bias. The article by Rossetto et al., was concerning because of its lack of blinding of participants (Figures 2 and 3).

Bar chart of the risk of bias assessment. The vertical axis lists different domains that can affect the quality of the studies included in the analysis, such as bias arising from the randomization process, deviations from intended interventions, or missing data on the outcomes, measurements of the outcomes, and selection of the reported results. The horizontal axis represents the percentage of risk, ranging from 0% to 100%.

Risk of bias summary across five domains of potential bias. The green plus symbols indicate a low risk of bias, and the yellow minus symbols indicate some concerns about bias.
Regarding the two included case series studies, Portaro et al. was judged as having fair quality and Hawley et al. as having good quality. The two included single-arm studies were judged as having fair quality. Finally, the two included qualitative studies were judged as having an overall low risk of bias (Supplementary File 2).
Overview of analyzed research
The included studies varied in their focus, with some addressing health outcomes, others focusing on the quality of life, and a few examining social participation. Our study included a diverse range of study designs, with three RCTs,23–25 two qualitative studies,26,27 two case series studies,28,29 and two single-arm studies.30,31 This analysis encompassed ten research studies; all were conducted between January 2013 and June 2024 and published in journals with peer review processes (Table 2). The interventions across the studies encompassed a diverse range of approaches tailored to address the needs of individuals with disabilities. These included computer games for skill development, smartphone-delivered exercise programs, virtual reality interventions, telemedicine activities, mood management programs, machine learning aids for speech impairment, telerehabilitation systems, and digital storytelling interventions.
Summary of studies examining the impact of digital health interventions on various disabilities across different countries.
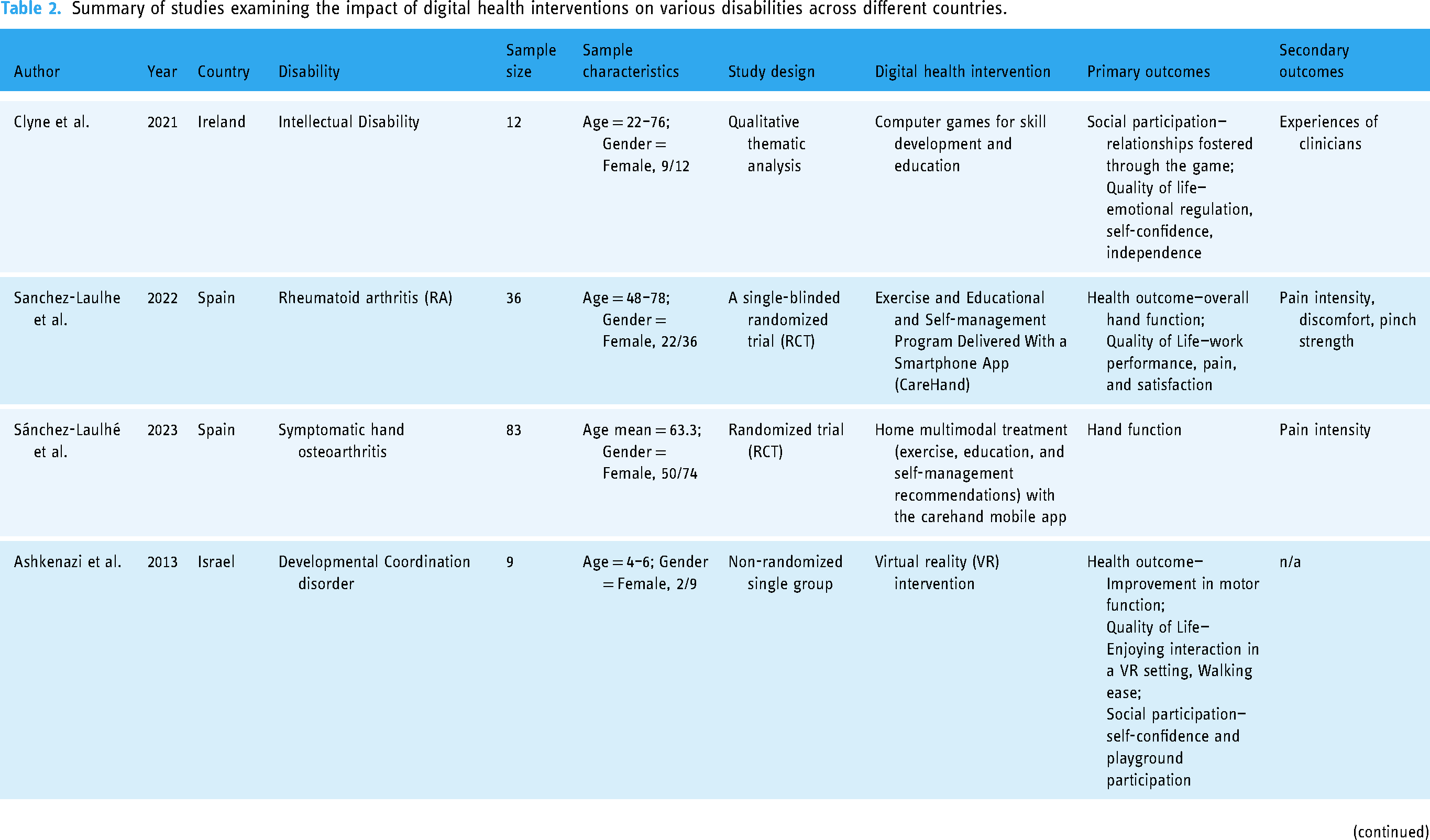
Two studies concentrated on intellectual disabilities,26,27 while the rest addressed a range of other conditions, such as speech disorders, 28 Alzheimer's disease, 25 strokes, 31 multiple sclerosis, 31 rheumatoid arthritis, 24 developmental coordination issues, 30 facio-scapulo-humeral muscular dystrophy (FSHD), 29 disorders related to the musculoskeletal system, reduced muscle strength, limited range of passive motion, missing limbs, discrepancies in leg length, abnormal shortness, hypertonia, ataxia, athetosis, and challenges in vision. 23
The research included various digital health solutions, such as telehealth systems, online programs for mood regulation, virtual reality, speech recognition via machine learning, computer-based games, and digital narrative platforms. These studies investigated several outcomes of these technological health interventions for individuals with disabilities, focusing on general health outcomes,25,26,28–31 quality of life,23,24,26,27,29–31 and societal integration.25,26
Outcome measures
The studies explored various facets of outcomes, clustering them into three primary categories: health outcomes, life quality outcomes, and societal participation outcomes. In terms of health, the focus was on enhancements in cognitive abilities and functionality in areas of disability. Life quality measures in these studies spanned areas such as emotional balance, self-assurance, autonomy, minimized hospital stays, occupational efficiency, pain management, satisfaction, and general well-being. In contrast, social participation measures comprised the relationships developed via digital health tools and observed behavioral indicators. Patient viewpoints shed light on the tool's operation and its ease of use. Notably, the research by Clyne et al. (2021) included feedback from clinicians regarding the digital tool's efficacy. 26
Of the studies with a control group, digital health interventions were compared with traditional care, standard rehabilitation practices, or no intervention. For instance, Rossetto et al. (2023) compared telerehabilitation with usual care for Alzheimer's disease patients, while Sánchez-Laulhé et al. (2022) compared a mobile app intervention with standard care for rheumatoid arthritis patients.
Health outcomes
The effectiveness of digital health interventions in improving health outcomes was the main focus of six studies.25,26,28–31 Rossetto and colleagues 25 observed enhanced neuropsychological states in individuals receiving digital health interventions during their treatment and subsequent follow-up periods. Notable improvements were witnessed in areas such as memory, language, executive capabilities, and overall cognitive functions following the deployment of telerehabilitation strategies for patients with Alzheimer's disease. 25 Similarly, Portaro and his team (2019) investigated the effects of telehealth strategies, noting positive changes in both neurological and respiratory conditions in patients suffering from FSHD. 29 In another study by Sánchez-Laulhé et al. (2022), the research focused on the efficacy of independently operated digital health programs in enhancing hand mobility for individuals with rheumatoid arthritis. 24 Their findings highlighted a substantial enhancement in hand mobility for app users in contrast to those in the non-user group, with a mean difference of 13.36 (ranging from 2.85 to 23.87) in the third month and 7.19 (ranging from ‒4.79 to 19.16) in the sixth month. Additionally, Hawley et al. (2013) identified increased functionality in patients with pronounced speech impairments in a separate investigation, recording an average accuracy enhancement in recognition generation of up to 96% post-implementation of the Voice Input Voice Output Communication Aid (VIVOCA) initiative. 28 Furthermore, a study by Ashkenazi and his team (2013) documented positive outcomes in various motor skills, including movement precision, equilibrium, coordination, and fine motor skills, along with manual dexterity and proficiency in aiming and catching, following the patient's engagement with a digital health intervention. 30
Quality of life
The impact of digital health interventions on the quality of life of people living with disabilities was examined in multiple studies.23,24,26,27,29–31 These studies highlighted the positive effects of digital health interventions on various aspects of patients' well-being. For instance, Levy et al. (2015) utilized the Montreal Cognitive Assessment (MoCA) to explore improvements in eight domains of cognitive functions. They found that the intervention not only enhanced physical abilities but also significantly elevated the mental well-being of participants, as reflected in the rise in their MoCA scores (p = .01, r = 0.44). 31 This was particularly evident in areas such as conceptual skills, memory, and executive functions.
Sánchez-Laulhé et al. (2022) investigated a digital tool's influence on rheumatoid arthritis patients' daily activities and work productivity. They found not only a notable improvement in daily functions and job performance but also a significant decrease in pain levels for those who underwent the treatment compared with a control group. 24 In another study by Vereenooghe et al. (2021), participants emphasized the digital tool's importance in helping them manage feelings of depression and homesickness. 27 Lastly, Ofoegbu et al. (2020) found that disabled athletes experienced a decline in burnout sensations after participating in a digital storytelling initiative, pointing to enhanced psychological outcomes. 23
Sanchez-Laulhe et al. (2023) showed that a group of patients who had used the CareHand mobile app showed significant improvements in hand function at 6 months, whereas the usual care group did not demonstrate such changes. 32 At 3 months, neither group showed improvements in hand function. For secondary outcomes, the CareHand group exhibited better results in upper limb function at both 3 and 6 months, as well as in pain reduction at 1 and 3 months, compared with the usual care group. Linear regression models indicated that baseline scores of pain intensity, hand status, and upper limb function were associated with greater improvements in hand pain and physical function.
Social participation
Most of the included studies did not much explore the role of digital health interventions in promoting social participation. Only two studies highlighted how the interventions improved social participation.25,26 In a 2021 study by Clyne and colleagues, it was observed that digital health interventions played a role in strengthening relationships. Participants seemed to form connections with the virtual entities, viewing them as genuine individuals offering assistance. From the standpoint of social engagement, the patients appreciated having someone to converse with and benefited from the experience. Similarly, a 2023 study by Rossetto et al. found that after participating in digital health interventions, there was an enhancement in social participation among Alzheimer's disease patients. This was evident in their daily autonomy, behavioral symptoms, and increased engagement in conversations and outdoor pursuits after the interventions. The growth they demonstrated surpassed that of a comparison group. 25
Secondary outcomes
Levy et al. (2015) examined patients' satisfaction with the digital health intervention telerehabilitation. 31 The respondents noted that they were either “satisfied” or “very satisfied” with their experiences. The high satisfaction rate was attributed to the short time needed to access the therapist, the privacy of the intervention, the interaction with physicians, the audiovisual quality, and the operation of the equipment. Vereenooghe et al. (2021) identified concerns associated with ease of use, the understanding of the purpose of the intervention, and the skills and support needed to get the most out of the intervention. 27
Discussion
This study explored the outcomes of studies focusing on using digital health interventions in persons with disabilities. The current findings illustrate the potential value of digital health interventions in improving the health outcomes, quality of life, and social participation of people with disabilities. While these studies provide promising evidence, their small number limits the generalizability of the conclusions. Further research with larger sample sizes and diverse populations is needed to confirm these findings. The use of digital health interventions in different populations of people with disabilities is important in illustrating the value of these tools. Technology interventions for people with disabilities are designed to address their specific challenges, enhancing independence and inclusion through tools such as screen readers and communication aids. In contrast, mainstream technologies often overlook the unique needs of individuals with disabilities, focusing on the broader public. These general technologies may not be fully accessible, potentially excluding those with disabilities. This distinction highlights the importance of tailored solutions for supporting full participation and accessibility.5,33
The diverse population of individuals with disabilities has a wide spectrum of digital needs, ranging from accessibility features for those with visual or auditory impairments to specialized interfaces for cognitive or motor challenges. 34 Research by Venkatesan et al. (2013) highlighted that digital interventions must be tailored to address not only the primary disability but also to consider potential comorbidities and varying levels of digital literacy among users. 35 Furthermore, Erku et al. (2023) emphasized the importance of considering cultural and socioeconomic factors in designing digital health solutions, as these can significantly impact a user's access to, adoption of, and success with using interventions for different subgroups within the disability community. 36
Our study identified a variety of digital health interventions for individuals with disabilities, including telehealth, mobile health applications, virtual reality, computer games, telerehabilitation systems, and machine learning aids. These interventions have had several positive impacts on health outcomes. For instance, studies reported improvements in cognitive functions such as memory, language, and executive functions, enhancements in motor skills and hand mobility, and effective symptom management for conditions such as rheumatoid arthritis and Alzheimer's disease. The findings demonstrated that digital health interventions can have positive impacts across various domains for individuals with disabilities. In terms of health outcomes, improvements were seen in areas such as cognitive function, motor skills, speech recognition, and disease symptoms for conditions such as Alzheimer's disease, rheumatoid arthritis, and neuromuscular disorders. Regarding the quality of life, the interventions enhanced psychological well-being, reduced depression and burnout, decreased pain, and boosted independence in performing daily activities and being productive in work situations. However, impacts on social participation were less explored, with only a couple of studies noting increased social engagement and strengthened relationships through the digital tools.
The heterogeneity of disabilities—ranging from physical impairments like mobility restrictions to cognitive challenges necessitates a personalized approach when designing and implementing digital health interventions. This diversity is reflected in the clinical instruments and methodologies employed in the studies included in our review (Table 2). For instance, studies focused on patients with neurological conditions such as stroke and multiple sclerosis, often utilized methods that assess motor function, cognitive recovery, and activities of daily living.31,37 In contrast, studies involving developmental disabilities employed tools designed to measure social participation, communication skills as well as motor coordination.30,38 Our review highlights the need for future research to not only employ digital health interventions to the specific needs of different disability groups but also to standardize the use of clinical instruments where possible.
Co-creation in digital health interventions is pivotal for enhancing public health outcomes because it fosters a collaborative development process involving stakeholders such as providers, customers, and suppliers. It ensures interventions are user-centered, addressing real needs through innovative solutions. Benefits include improved public health outcomes, positive emotional impacts, better self-management, and greater acceptability of interventions. Co-creation also navigates challenges such as budget constraints and power dynamics, tailors strategies for diverse populations, and supports information and communication technologies for effective collaboration.39,40 This approach not only fosters innovation and user engagement but also ensures that interventions meet the specific needs of target populations, leading to more sustainable and effective healthcare solutions. This study would call for more co-creation developments to provide digital health interventions that would meet the challenges of having a disability.
The secondary outcomes examined in the literature showed that design and user features impacted the ability of digital health interventions to achieve the desired outcomes. Levy et al. (2015) and Vereenooghe et al. (2021) demonstrated that ease of use, understanding of the intervention, support, privacy, and user interface were variables that determined the impact of the tools.27,31 These factors were demonstrated to impact the outcomes of the digital interventions as they impacted adherence, enjoyment, and engagement of the persons with disabilities. While two studies provided self-administered interventions, healthcare professionals administered or supported others. This illustrated the value of integrating clinicians and other healthcare professionals in developing these digital health interventions for people with disabilities.
The rapid development of novel technologies, especially in the realms of virtual reality and machine learning, presents tremendous potential for enhancing the capabilities of existing digital solutions. 41 These advancements can lead to optimized outcomes in a myriad of sectors, including healthcare, entertainment, education, and more.42,43
Within the context of digital health interventions for individuals with disabilities, engagement stands out as a critical component for success. Ashkenazi et al. (2013) emphasized the pivotal roles of enjoyment and motivation in this regard. 30 If the users found the digital tools pleasurable and motivating, they were more likely to engage with them actively and consistently, thereby deriving greater benefits.
Previous studies have underscored the importance of enjoyment in intervention outcomes. Graf et al. (2009) and Jannink et al. (2008) have particularly emphasized this for children with disabilities. Their findings suggested that when these children found enjoyment in the activities presented through digital interventions, their engagement levels rose significantly.44,45 Not only did this increase their active participation and energy expenditure but it also boosted the chances of the intervention being effective and improving the physical response. Such results highlighted an important consideration for developers and practitioners. When designing digital interventions, especially for specific populations such as children with disabilities, the user experience should be at the forefront. By integrating elements of fun, motivation, and enjoyment into the design process, the interventions can be made more engaging and, consequently, more effective.
Our review aligns with the broader trends identified in the literature on health and rehabilitation for people with disabilities. The literature highlights a critical junction digital health in healthcare, particularly in the United States, driven by increasing demand for healthcare services. 46 Similarly, our review underscores the potential of digital health interventions to address these growing healthcare needs in individuals with disabilities. However, our findings suggest that while the technological frameworks for health and rehabilitation are maturing, the specific needs of people with disabilities are not always fully addressed in these interventions. This highlights the necessity of linking digital health solutions to the unique challenges posed by various disabilities. The literature emphasizes that technologies enabling rehabilitation, such as wearable sensors and in-home environmental monitors are universally applicable and transcend national boundaries. 46 Our findings further support this notion, demonstrating that while digital health interventions hold significant promise, their success largely depends on their ability to meet the specific needs of diverse disability groups.
Similar to the systematic review conducted by Zhou and Parmanto 2019, which evaluated digital interventions such as videoconferencing for individuals with disabilities in remote regions, our review also identified a limited number of studies, many of which were small-scale and lacked robust RCTs. 47 Both reviews highlight the positive outcomes reported by these studies, particularly in terms of functional improvement and quality of life. However, the small sample sizes and methodological limitations in both our review and that of Zhou and Parmanto suggest that while the potential of digital health interventions is promising, the evidence base remains insufficient to definitively prove their effectiveness across diverse disability populations.
This study had several strengths. It followed the rigorous PRISMA guidelines and searched multiple databases to comprehensively identify relevant studies on digital health interventions for individuals with disabilities. The included studies covered a diverse range of disabilities and digital interventions, providing a broad overview of the field. The quality assessment tools used helped evaluate potential biases.
However, the study also had some limitations, both in its methodology and in the quality of available studies. Regarding the study's design, the heterogeneity across the studies in terms of disabilities, interventions, and outcome measures made a meta-analysis challenging. While health and quality of life outcomes were well-represented, fewer studies explored impacts on social participation, an important outcome for this population; this was possibly due to our inclusion criteria. One limitation of this study is related to the search terms used during the systematic review process. While we aimed to capture a broad spectrum of digital health interventions for individuals with disabilities, the search strategy may not have fully encompassed all relevant disease-specific or disability-related terms.
Concerning the limitations of the reviewed literature itself, as the field of digital health for disabilities is still emerging, more targeted research may be needed, especially on facilitating societal integration through technologies. One of the primary limitations in the existing studies was the scarcity of direct measures of motivation and enjoyment in digital health interventions in disabilities. Although these factors are widely recognized for their critical role in determining the success and user engagement of digital health tools, their direct impact was not quantifiable due to the lack of explicit measurement in the studies analyzed. Therefore, future primary research could significantly benefit from incorporating the assessment of motivation and enjoyment.
The practical implications of our findings highlighted several key benefits that could directly impact individuals with disabilities. Digital health interventions have shown a potential to enhance health outcomes by improving cognitive functions, motor skills, and overall health conditions. Additionally, these tools can enhance the quality of life by reducing pain, increasing daily activity efficiency, and promoting emotional well-being, as seen in the CareHand mobile app for rheumatoid arthritis patients. Furthermore, digital health interventions can increase social participation by fostering stronger social relationships and engagement. Participants using digital tools for mood management and cognitive assistance reported meaningful interactions and reduced feelings of isolation.
This study findings offer insights into the application of digital health interventions for persons with disabilities. While digital health tools hold significant promise, their success largely depends on the alignment of the intervention with the specific needs of the disability it aims to address. The evidence supports the need for co-creation with end-users to ensure that these interventions are both accessible and effective, further emphasizing the importance of patient-centered design in digital health.
Conclusion
This study investigated the potential of digital health interventions to benefit individuals with disabilities across multiple domains. The analyzed studies demonstrated that these technological tools can lead to improved health outcomes such as enhanced cognitive function, motor skills, and speech recognition and better symptom management for conditions such as Alzheimer's disease, rheumatoid arthritis, and neuromuscular disorders. Moreover, digital interventions were found to elevate the quality of life by promoting psychological well-being and reducing depression, burnout, and pain levels, while boosting independence in daily activities and work productivity. However, the review also revealed a dearth of research examining the impacts of digital health tools on social participation, a crucial aspect influencing well-being for the disabled community. The limited number of studies in this area pointed to a significant gap that needs to be addressed through future targeted research efforts. By synthesizing the current evidence base, this review could inform the development and implementation of more effective, user-centric digital health solutions tailored to the unique needs of individuals with disabilities. While the reviewed studies suggested that digital health interventions can lead to improvements in various health outcomes, quality of life, and social participation, the evidence is not yet definitive. It is essential to consider the heterogeneity of the studies and the varying quality of the evidence. Therefore, we advocate for cautious optimism and emphasize the need for further rigorous research to validate these preliminary findings
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241294190 - Supplemental material for Digital health interventions for individuals with disabilities and their impacts on health, quality of life, and social participation
Supplemental material, sj-docx-1-dhj-10.1177_20552076241294190 for Digital health interventions for individuals with disabilities and their impacts on health, quality of life, and social participation by Mahmoud Kandeel, Mohamed A. Morsy, Khaled Alkhodair and Sameer Alhojaily in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241294190 - Supplemental material for Digital health interventions for individuals with disabilities and their impacts on health, quality of life, and social participation
Supplemental material, sj-docx-2-dhj-10.1177_20552076241294190 for Digital health interventions for individuals with disabilities and their impacts on health, quality of life, and social participation by Mahmoud Kandeel, Mohamed A. Morsy, Khaled Alkhodair and Sameer Alhojaily in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241294190 - Supplemental material for Digital health interventions for individuals with disabilities and their impacts on health, quality of life, and social participation
Supplemental material, sj-docx-3-dhj-10.1177_20552076241294190 for Digital health interventions for individuals with disabilities and their impacts on health, quality of life, and social participation by Mahmoud Kandeel, Mohamed A. Morsy, Khaled Alkhodair and Sameer Alhojaily in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors extend their appreciation to the King Salman Center For Disability Research for funding this work through Research Group no KSRG-2023-136. The authors extend their appreciation to the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia under Annual Research Track (Grant No. KFU242153).
Contributors
Conceptualization, M.K. and MAM.; methodology, M.K.; software, M.K.; validation, M.K., K.MA and S.A.; formal analysis, M.K.; investigation, K.MA and S.A.; resources, M.K.; data curation, M.K., K.MA and S.A.; writing—original draft preparation, M.K.; writing—review and editing, MAM., K.MA and S.A.; funding acquisition, M.K. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the King Salman Center for Disability Research (grant number KSRG-2023-136). This work was supported through the Annual Funding track by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia [Project No. KFU242153].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.