
Abstract
Introduction
Innovative technological applications like smart continence care (SCC) offer potential benefits in healthcare delivery, particularly for individuals with profound intellectual and multiple disabilities (PIMD). SCC aims to prompt caregivers to change continence materials, potentially improving clients’ quality of life and reducing caregivers’ workload. Although the use of SCC in PIMD care is promising, research is needed to improve its use in these complex settings. The aim of this study was to reflect on the SCC implementation process in care organizations for people with PIMD.
Methods
Fifteen semi-structured interviews were conducted with key stakeholders, caregivers, and SCC project leaders, across four care organizations. Interviews utilized an integrated framework drawing from the centre for eHealth research roadmap and the nonadoption, abandonment, scale-up, spread, and sustainability framework, both addressing eHealth implementation. Thematic analysis and open coding were employed to identify key themes and sub-themes in the implementation process.
Results
Four main themes emerged as crucial for successful SCC implementation: creating support, communication between stakeholders, problem-solving, and willingness to adopt SCC. The first three themes were perceived as contributors to the success of SCC implementation, whereas the last theme showed factors impacting willingness to adopt SCC. Early involvement of key stakeholders and clear communication about expectations of their roles was perceived as crucial and created clarity. Adequate problem-solving was identified as influential in SCC utilization and willingness to adopt person-centred continence care.
Conclusion
Implementation of SCC requires changes in the work routines of those involved, and key stakeholders’ early involvement appears to improve support for these changes. Fostering communication between key stakeholders and adequate problem-solving contributes to positive experiences and the perceived success of sustainable implementation. This study offered a rich understanding of day-to-day practices around implementing SCC in disability care organizations. The findings may also be relevant for the implementation of technologies in other care settings.
Keywords
Background
Incontinence is common among people with profound intellectual and multiple disabilities (PIMD).1–4 Most people with PIMD cannot notify professional caregivers in residential care (hereafter referred to as caregivers) when their incontinence material needs to be changed because of their limited communication, cognitive, and motor skills.1–4 This leads to a highly intensive care process.5,6 Advanced technologies, such as the ones used for continence materials for smart continence care (SCC), can help people with PIMD to notify their caregivers when their continence material has reached a certain saturation level and needs to be changed. 7
The use of technological applications, such as for SCC, in (health)care settings may contribute to the improvement of the quality of care and person-centred care.8,9 The implementation in daily care is challenging and complex considering the magnitude and the heterogeneity of the disabilities among people with PIMD. 10 Therefore, caregivers need to be aware of the specificity of the disabilities and needs of each individual.5,10 However, usually, caregivers change incontinence materials at fixed times. Providing continence care at the time when incontinence material is saturated prevents leakages and avoids unnecessary changes of incontinence material, which leads to more sustainable and personalized care. 11 This is predicted to enhance clients’ quality of life while reducing the workload for caregivers. 7 Previous studies have demonstrated the applicability and effectiveness of various SCC systems in elder care settings.11–13 Despite its potential to enhance the care for people with PIMD, 7 experiences with SCC implementation in disability care organizations have not yet been structurally investigated.
Numerous theoretical frameworks exist on technology implementation. 14 More general frameworks are, for example, the updated Consolidated Framework for Implementation Research (CFIR), 15 Wensing and Grol's work, 16 or diffusion of innovation in service organizations. 17 Additionally, there exist eHealth frameworks specifically tailored to implementation processes of healthcare technologies, 18 such as the centre for eHealth research (CeHRes) roadmap and the nonadoption, abandonment, scale-up, spread, and sustainability (NASSS) framework. In the current study, we reflected on the SCC implementation process by using an integrated framework combining elements from the CeHRes roadmap and NASSS 19 to ensure a comprehensive understanding of the complexities involved within the context of implementing healthcare technologies.
The CeHRes roadmap and NASSS have an empirical base in healthcare technology research.20–23 The CeHRes roadmap can be applied to guide and reflect on the development, implementation, and evaluation of eHealth technologies.24,25 The NASSS framework guides and reviews the implementation of health and care technology in multiple domains (e.g., technology, value proposition, adopters, organization). 26 According to NASSS, technology development is a never-ending process in which technology can be adjusted to fit each specific setting and context, showing important preconditions for implementation. 27 The two frameworks complement each other and provide a comprehensive and iterative perspective on the complexity of the implementation process in healthcare and can be applied to guide and reflect on this process. 25
The main objective of this study was to reflect on the SCC implementation process in disability care organizations for people with PIMD by applying the integrated implementation framework 19 in gathering first-hand experiences from key stakeholders, i.e., caregivers and project leaders directly involved in applying SCC.
Methods
Study design
This study used a qualitative design with semi-structured interviews to gather the experiences of key stakeholders from four disability care organizations involved in SCC implementation. The COREQ checklist was used as a reporting guideline (see Supplementary File 1). The participants gave their informed consent for their interview and recording. Ethical approval was obtained from the Medical Ethics Committee of Radboudumc (NL72751.091.20).
Study setting
This study was part of a 3-year cluster randomized trial aimed at researching the (cost-)effectiveness of SCC for people with PIMD. 7 Six disability care organizations participated in the trial, of which four were invited to participate in the present study because of the stage of the implementation at the time. Each of these care organizations implemented SCC for 26–31 persons with PIMD, distributed over four to seven residential homes. All these care organizations set up a project team and appointed a project leader specifically for SCC implementation. An implementation guideline, which will be published in due course, was developed a priori based on implementation theories and evidence15,16,28–30 and refined through co-creation with the participating care organizations. Additional consultation was available during the implementation process. The SCC used in this study consists of diapers and pads that contain urine sensors. a A removable clip attached to the incontinence material sends information about the saturation level to a receiver via Bluetooth and subsequently to an app on the caregiver's mobile phone. Caregivers receive colour-coded notifications depending on the set saturation level per user: change desired (orange), risk of leakage (red), or OK (green).
Participants
Purposive sampling was used to include a broad diversity of the experiences of the key stakeholders responsible for coordinating and executing SCC implementation in the four participating care organizations. The researchers involved in the implementation process identified key stakeholders who were closely involved in the implementation process of SCC. Of the 16 invited key stakeholders, 15 participated (14 females, 1 male). The study sample consisted of project leaders (n = 8) involved in the implementation process at these four organizations and caregivers (n = 7). The project leader group consisted of four participants specifically appointed to lead SCC implementation in their organization. Five participants were closely involved because of their daily work, two as team coordinators, one project coordinator, one programme manager, and a person combining the role of team manager and project leader. The caregivers interviewed were appointed or volunteered as SCC ambassadors, meaning that they were responsible for implementing SCC in their team and serving as the key SCC user. They were the spokesperson to the project leader and the SCC supplier. We, therefore, refer to the caregivers with an ambassador role group as ‘ambassadors’ when they spoke about their role as ambassador. We refer to them as caregivers when they spoke about their own role as professional caregivers, or their team members’ caregiver role. Since this interview was part of the trial they were already participating in, all interviewees were informed beforehand that they would receive an invitation for an interview.
Study procedure
Interviews were conducted between January 2022 and December 2022 by JvC and VvC. The duration of the interviews varied between 30 and 60 min. Twelve interviews were online, using Microsoft Teams; the other interviews were conducted onsite at a location of the interviewees’ choice. The interviews were transcribed, and participants were offered a member check, which did not lead to any changes.
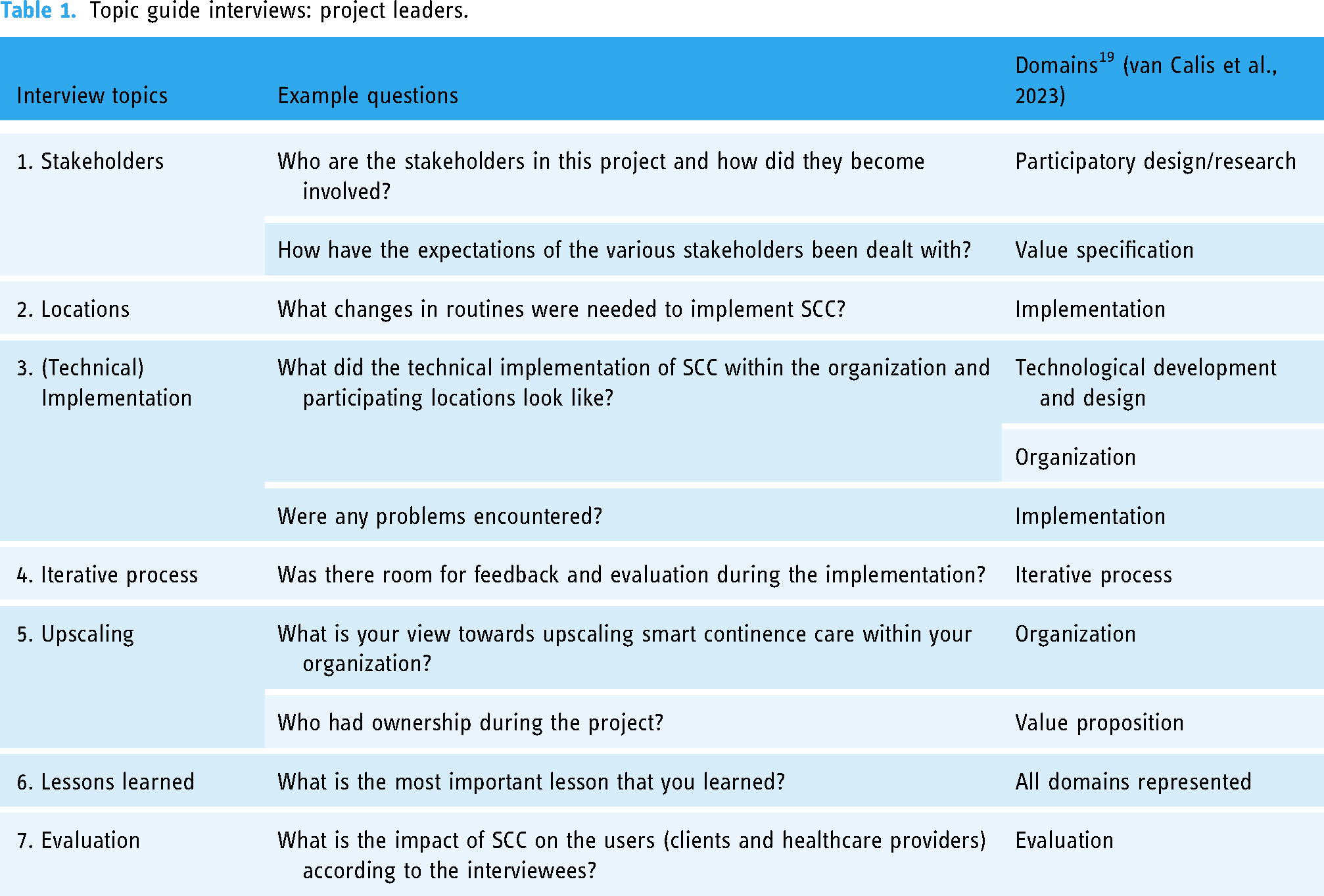
The interviews were tailored to match project leaders, caregivers, and their specific organizations based on the implementation logbook, kept by VvC, which contained information about salient events. This resulted in two topic lists developed based on the integration of the CeHRes roadmap and NASSS framework. 19 The topic lists incorporated nine domains derived from this integrated framework: (1) participatory development, (2) iterative process, (3) value specification, (4) value proposition, (5) technological development and design, (6) organization, (7) external context, (8) implementation, and (9) evaluation. 19 Tables 1 and 2 give an overview of how the topics, interview questions, and domains relate to one another. The first interview with a project leader served as a pilot, after which minor adjustments were made.
Topic guide interviews: project leaders.
Topic guide interviews: ambassadors.

Data analysis
After transcription, the qualitative data were analysed thematically, supported by the ATLAS.ti 9.1.6 software, in several steps, as described by Braun and Clarke.31,32 To gain familiarity with the data, transcripts were read, and audio recordings were listened to. The frameworks (CeHRes and NASSS) were used to reflect on the implementation process. We applied open coding to the data and analysed the data inductively, with the aim of formulating new themes based on the data itself rather than assessing the existing frameworks. Two authors (JvC, VvC) separately open-coded three transcripts. Relevant quotes and codes were identified and similarities and differences in coding were discussed, resulting in a first conceptual codebook. This codebook was subsequently applied to six transcripts independently by the two main authors (JvC, VvC). Discussing and comparing the codes between three authors (JvC, VvC, KB) led to the addition of new codes, rephrasing codes, and merging codes, resulting in a coding structure. This coding structure was applied to the remaining transcripts by two authors (JvC, VvC).
Next, two authors (JvC, VvC) discussed all coded data. In several rounds, codes were clustered into broader overarching categories. A third author (KB) joined in the last rounds of this step, leading to a final review and (re)naming the main themes and sub-themes. For example, the codes ‘discuss’, ‘inform’, ‘evaluate’, and ‘advise’ were clustered into the sub-theme ‘continuous communication’ as part of the main theme ‘communication between stakeholders’. Three authors (JvC, VvC, KB) grouped the sub-themes, resulting in four main themes described in the results section below.
Results
The analysis resulted in four main themes: (1) create support, (2) communication between stakeholders, (3) problem-solving, and (4) willingness to adopt SCC. Each theme has two or three sub-themes, which are described in this section and illustrated by quotes in the tables. The first three themes can be defined as contributors to the success of the SCC implementation, whereas the last theme shows how these factors impact the willingness to adopt SCC.
Create support
Support for SCC use was created through engagement during implementation itself and included several roles that key stakeholders played in the process (Table 3).
Sub-themes and quotes of the theme create support.

Engagement during implementation
Early in the implementation process, stakeholders were engaged consciously by the project leaders. This was perceived as having a positive influence on creating support for SCC implementation by the caregivers. For instance, the early involvement of support services such as IT and logistics departments was important, because they provided essential preconditions to contribute to the implementation, and by early involvement they were able to think along and prepare the implementation from their side [Quote 1.1.a]. Early involvement of managers is important to support SCC use in the organization and to ensure joint decision-making for possible further uptake.
Participants stated that the SCC implementation meant a change in work routine, from changing diapers at fixed times to diaper changing when a notification indicated full incontinence material. Caregivers felt supported when they were informed about the project before the implementation started [Quote 1.1.b]. Because of this early involvement, the expected added value of SCC for the client and the workplace was more evident to those involved; this was experienced as motivating and increased willingness to cooperate. Caregivers described the expected added value as the increased well-being of the clients with PIMD, elimination of unnecessary material changes, improved skin condition, and learning about clients’ voiding patterns.
Roles in the implementation process
Project leaders had a managing role in the implementation process, entailing the management of implementation at participating locations and keeping all stakeholders involved and connected by coordinating the necessary implementation steps and communicating with management and the SCC supplier. In this role, project leaders also had to deal with resistance from the caregivers, for instance, regarding diaper-changing routines. Therefore, proximity of the project leaders and ambassadors to first-hand users on the work floor – the caregivers – was considered important and led to positive experiences [Quote 1.2.a]. In line with this, a lack of contact and proximity resulted in negative experiences [Quote 1.2.b].
Caregivers who were ambassadors in the implementation process acted as key users to their colleagues. In this role, they were the liaison between the project leader, their team, and the supplier. This role was new to them and included tasks to involve and support colleagues in using SCC, changing work routines, and signalling issues as well as communicating with the project leader and the SCC supplier. Allocating dedicated hours and being explicitly assigned the role of ambassador was an important facilitator [Quote 1.2.c], as were their skills in dealing with resistance. Ensuring a collaborative feeling through close contact between the teams, ambassador, and project leaders created a feeling of ‘doing it together’, thereby contributing to a positive experience.
SCC implementation and use eventually takes place on the work floor. It is the caregivers that need to change their way of working. Although the caregivers stated that they understand the potential added value of SCC and understand that the existing routine is not optimal, it still can be hard for them to let go of the fixed schedules [Quote 1.2.d] and change on request indicated by the SCC has an impact on the rest of the day's programme.
Communication between stakeholders
Communication between different stakeholders entailed two sub-themes: continuous communication and communication channels (Table 4). Communication took place with external stakeholders, such as the supplier of the SCC material, but also between internal stakeholders, such as different care teams, the project leader, support services, and management of the care organization.
Sub-themes and quotes of the theme communication between stakeholders.

Continuous communication
Continuous communication gave the participants the experience of support and direction in what was needed for implementing SCC at multiple stages of the implementation process. During the preparation phase, this included informing many people throughout the organization and asking for their advice, for example, about the size of material to use and where to place the Bluetooth receivers. During SCC use, the care teams, together with the supplier, often discussed and evaluated SCC per individual client, so that adjustments could be made to ensure optimalization for the client. These junctures, together with informal points of contact [Quote 2.1.a], ensured continuous communication. This was an important prerequisite to keep the implementation on track and prevent delays arising from unsolved problems and inaction, which could result in a negative experience of ‘muddling through’ [Quote 2.1.b].
Communication channels
The continuity of communication as described above was facilitated in different ways and through various channels, such as email, WhatsApp, phone, online meetings, and live meetings. Both online and offline meetings between care teams from different locations were scheduled, thereby ensuring that everyone could be involved in the changes that took place and in the agreements that they made with one another.
Caregivers experienced WhatsApp as a fast, accessible, and direct way of communication between the work floor and the supplier. A risk with this type of communication was that expectations were not always met and that misunderstanding could arise as a result of differences in the interpretation of written text in WhatsApp [Quote 2.2.a]. Frequent face-to-face contact was experienced as pleasant and helpful, especially when client-specific cases needed to be discussed. When there was too little face-to-face contact, this led to frustration [Quote 2.2.b].
Problem-solving
When starting the SCC implementation process, teams encountered problems and challenges relating to working routines, everyday-care situations, and technical or practical problems with the product itself. During the process, different strategies to address challenges and problems were used, as discussed below (Table 5).
Sub-themes and quotes of the theme problem solving.

Solving problems on the work floor
The situation occurred that one team's caregivers provided continence care in a way that the other team viewed as inappropriate. This arose because of differences in the vision on quality of care and that sleep is more important than changing continence materials. For example, night-care teams contended that the night was for sleep and that their clients should not be woken up for a diaper change, even if this could result in a leakage. Day-care teams, however, felt that waking a person at night was preferred to decrease the possibility of them having a wet bed. It could be difficult to overcome these differences [Quote 3.1.a]; participants felt that it was important to communicate and agree upon how care is delivered; however, this did not always happen [Quote 3.1.b]. In general, the most important thing to do according to the participants is to communicate and explain each other's point of view and together agree upon what is best for the specific client and then keep checking whether the change in continence care provided has the desired effect.
Caregivers encountered several problems in matching the SCC material with their clients’ individual characteristics. This included finding a comfortable size and absorption capacity, determining the notification saturation level that suited the person's skin condition, and determining the right time for a diaper change in line with the client's programme of daily activities. When information about an individual voiding pattern was made available through the online portal, this helped caregivers to determine a care strategy per person. Caregivers could even decide to stop using SCC for some persons with PIMD to match their needs [Quote 3.1.c].
Solving problems with the product
Problems relating to technical and practical issues with the SCC product, if not possible for the caregivers or the care organization's IT department to solve, were solved by the supplier. One such problem that appeared, for example, was malfunctions with the Bluetooth clips that either did not work or did not send information to caregivers adequately; this needed to be solved by changing the clip or installing additional receivers. Often, this and other problems were adequately and promptly addressed by the supplier, thereby helping the working relationship between the supplier and caregivers and the caregivers’ work [Quote 3.2.a]. When there were delays in responses, unhelpful solutions, or differences in perceptions of how a problem had to be addressed, this led to frustrations with the caregivers and ambassadors [Quote 3.2.b,] and affected the trust in the product [Quote 3.2.c]. Project leaders indicated that the way in which technical problems were addressed during implementation influenced the decision on further SCC uptake within the organization [Quote 3.2.d].
Willingness to adopt SCC
Willingness to adopt SCC was influenced by three key factors: product usability, care teams’ attitude and motivation, and the skills and competencies available within the care teams (Table 6).
Sub-themes and quotes of theme product usability.
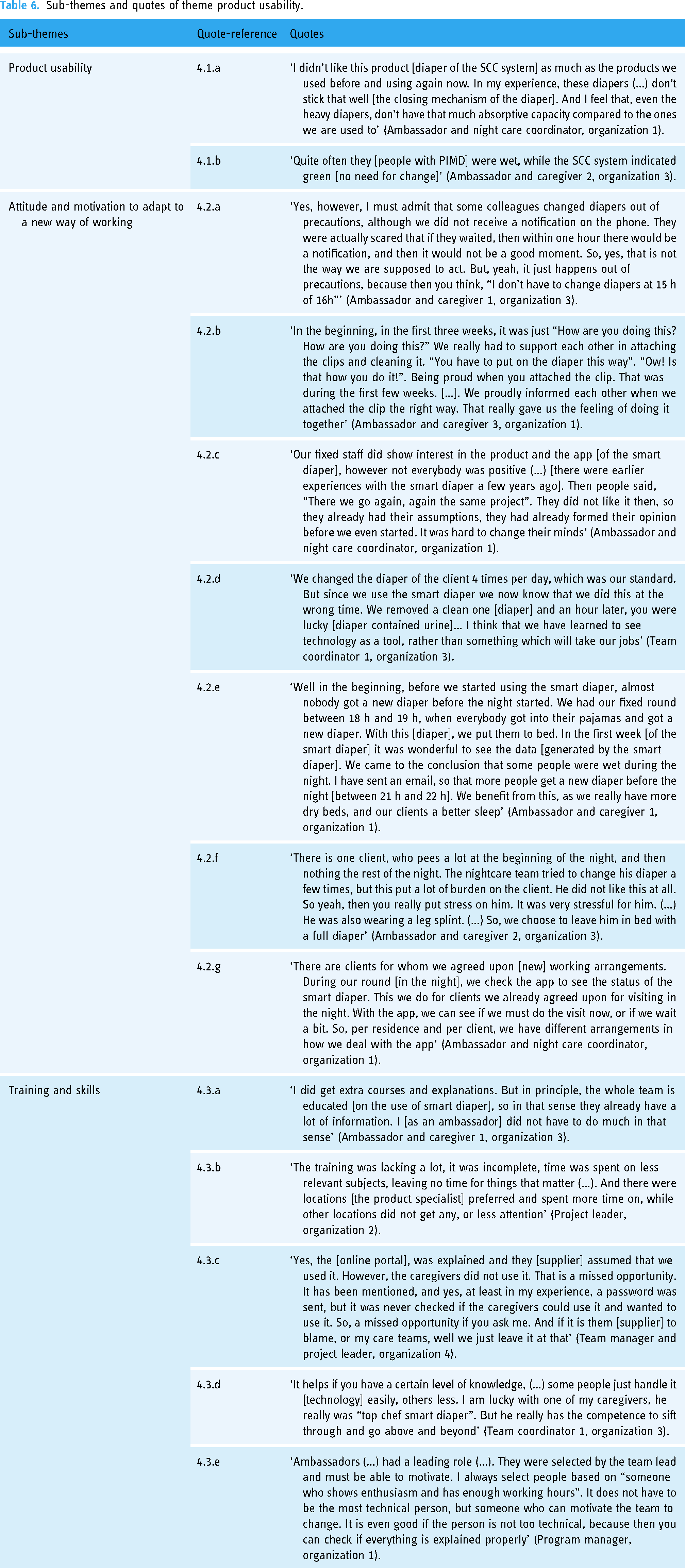
Product usability
Participants had different experiences regarding the usability of the product. For example, the absorption capacity could be different than their usual product, or characteristics like closing mechanisms were experienced as less favourable [Quote 4.1.a]. This influenced willingness to adopt the product after having experienced it. Technical issues or product malfunctions influencing the quality of care [Quote 4.1.b] had an impact on the trust in the product itself and was an important issue raising doubt about its further adoption.
Attitude and motivation to adapt to a new way of working
Teams struggled to adapt to the new working routines, as, with SCC, diapers should be changed promptly, instead of according to a fixed time schedule [Quote 4.2.a]. Adapting to this new work routine also meant that a team had to learn how to use SCC. An ambassador explained that her team learned together and helped one another [Quote 4.2.b]. However, previous negative experiences with SCC by colleagues resulted in a less favourable attitude towards using SCC, decreasing motivation, and making implementation more challenging [Quote 4.2.c].
Caregivers experienced the SCC as a tool to achieve person-centred continence care [Quote 4.2.d]. Considering the personal information about each participant's voiding volumes and patterns, caregivers were rethinking the thickness of the incontinence products used and the time at which they were putting on a diaper for the night [Quote 4.2.e]. Thinking about how to provide continence care in such a way that it best suits the needs of that specific person was a motivator for caregivers to use SCC. However, this also meant that sometimes the best thing to do was not to adhere to the SCC notifications [Quote 4.2.f].
Another example of when care teams did not adhere to the SCC notifications was when they decided to combine changing of continence material with the transfer of the person with PIMD to bed during the day. They explained that, because of the transfer by patient lift, they preferred to change the diaper during this transfer, avoiding an extra burdensome transfer later on. Thus, caregivers carefully considered when to provide continence care, for which SCC provided them with additional information to guide their decision [Quote 4.2.g].
Training and skills
Caregivers received training on how to use SCC. This entailed instructions on how to put on the diaper and how to use the mobile app. There was additional training about the web portal. The experiences of the training differed across organizations and even between teams [Quote 4.3.a and b]; the instruction on the web portal provided by a product specialist from the supplier was not always enough for the caregivers to put this knowledge into practice [Quote 4.3.c]. The training, together with skills such as technological capability and interest, the ability to motivate others [Quote 4.3.d and e], and personal motivation contributed to a more positive or negative experience in implementing SCC.
Discussion
The aim of this study was to reflect on the SCC implementation process in disability care organizations for people with PIMD. Based on the analysis of the interviews, we identified four main themes important to the implementation process: create support, communication between stakeholders, problem-solving, and willingness to adopt SCC. The first three themes related to the success of SCC implementation, whereas the last theme related to SCC's practical use impacting the willingness to adopt it. Our findings showed that it is crucial that key stakeholders are involved early in the implementation process and that communication between all the key stakeholders is important to create clarity about expectations of their roles. In addition, adequate problem-solving is important, as it influences SCC use and thus the willingness to provide person-centred continence care.
In line with other implementation theories,16,33,34 our findings showed that creating support for the implementation of technology is important. This can be achieved when project leaders responsible for the implementation process ensure early involvement and close proximity of its end-users and by appointing project leaders and caregivers as ambassadors. The ambassador's role can facilitate the implementation process on the work floor. This role is similar to that of change agents as described by Greenhalgh et al., 2004; 17 it is suggested that change agents are successful if they are selected on the basis of their credibility with the potential users, develop strong personal relations, communicate users’ needs to the supplier, and empower users to evaluate the innovation in order to decide about further uptake. 17 Both ambassadors and project leaders do this by creating support at different organizational levels, by engaging with other key stakeholders, and by having an intrinsic motivation to use a new (health)care technology. Implementation requires behavioural change among stakeholders in order to implement technological applications properly. Change agents are therefore needed to create and guarantee this behavioural change. This study added empirical evidence on how stakeholders can actually fulfil this change agent role as ambassadors. These findings suggest to involve stakeholders early in the implementation process and ensure clear communication about their roles and expectations. Additionally, we recommend to appoint project leaders and caregivers to facilitate this process by fostering support at all organizational levels.
According to the NASSS framework and CeHRes roadmap, close proximity and good cooperation are seen as fostering for implementation.24,26 Our study showed the close proximity of the project leaders’ with the care teams and other departments such as IT and management, which was experienced as helpful. Shared problem-solving allowed the care teams to learn from one another about using SCC. Problem-solving at the product level could be used to further develop the product during implementation.23,25 For example, the supplier of study has been working on an updated version of the product that addressed the issues also raised by the participants of this study. This illustrates the opportunity to further develop a product during implementation.
Our study also demonstrated that a shared vision and cooperation between the key stakeholders is important for incorporating new working routines, thereby ensuring adequate SCC use. This is in line with the constructs of the CFIR framework that should be taken into account when a (technological) innovation is being implemented. 15 For example, the framework's constructs ‘teaming’, ‘planning’, and ‘tailoring strategies’ show the importance of working together in a team, aligning expectations, and adapting to the context. Careful consideration of these constructs can assist the appropriate and effective implementation of SCC use in care teams’ day and night work routines. Additionally, communication between stakeholders and across departments about the expected value of an innovation and interpersonal relations within an organization contribute to positive experiences and the perceived success of sustainable implementation. For example, the project leaders in our study kept close contact with care teams and departments such as IT and management by keeping them informed and engaged throughout the implementation and by ensuring communication about their roles and what was expected from them. Part of the project leaders’ and the caregivers’ motivation was found to be determined by the expected value of SCC for the people with PIMD and for them as caregivers. This is in line with research by Damschroder et al. (2009) 33 and Greenhalgh et al. (2004) 17 underlining the importance of intra-organizational communication and inter-organizational networks and how effective communication across these domains enhances the success of the implementation and routinization of new structures. 17
Furthermore, our study showed the importance of skills and training and how this influenced the willingness to adopt SCC. The literature contends that the complexity of a technological innovation can hamper its adoption or at least lead to frustration in using the technological innovation adequately. 34 Training is one way to overcome these difficulties – and some persons need less training than others – but it is as important to have a support network, i.e., caregivers helping one another to use SCC. 33 In discussions with relevant stakeholders, the question of the potential added value of implementing the new technology should be raised with them. Doing so can foster the intention to change work routines by creating a common sense of the relative advantage, by planning carefully, and by involving key stakeholders. 16
Our main findings suggest that shared problem-solving among care teams, ongoing training, and the development of a strong support network are essential to overcome challenges related to SCC. Finally, a shared vision between stakeholders of SCC's value will encourage the adoption and sustainability of new work routines. These recommendations can be used to inform and supplement the implementation guide used in this project.
Limitations
This study is one of the first that addressed experiences with implementing SCC in disability care. We used an integrative framework combining the NASSS framework and the CeHRes roadmap to develop a broad topic list for data collection to obtain a broad perspective of the implementation process from the interviewees. 19 Although the frameworks were not used in the analysis of the data, our findings provided insight into a number of the nine domains. For example, the domains participatory design/research, iterative process, value specification, and implementation were reflected in all themes, because the key stakeholders were actively involved and the implementation process was continuously evaluated to ensure that their needs and requirements were met. Having a shared vision gave substance to the domain value proposition, as it ensured that stakeholders knew what the added value was and fulfilled their role in this regard. The domain organization was elaborated on in all four themes; they showed which changes were necessary to implement and how these changes were achieved.
However, various other frameworks, theories, and models can be used to research and reflect on the implementation process for healthcare technologies such as technology acceptance model, unified theory of acceptance and use of technology, and CFIR. 14 Using these theories might have highlighted different factors and components of healthcare technology implementation other than those in the NASSS framework and the CeHRes roadmap. Nevertheless, this study only used the integrated CeHRes roadmap and NASSS framework to collect the data structurally. We coded the data openly to leave room to identify other themes.
Four organizations and 15 interviewees participated in this study. The inclusion of all project leaders of these four organizations, combined with purposive sampling for caregivers, provided a broad range of experiences with the implementation process. Including different perspectives from other stakeholders, such as managers in the care organizations and the SCC suppliers, can capture additional important aspects of the implementation process.
Conclusion
SCC implementation requires various stakeholders to be involved, contributing to the process to ensure use and make the implementation a success. Creating a common goal towards the expected value by ensuring early engagement and offering support are valuable and necessary steps. Moreover, the implementation of advanced care technologies in working routines requires efforts to communicate, coordinate, and motivate on the part of key stakeholders, such as caregivers, IT and logistics departments, and management. This study suggested that fostering communication between these key stakeholders and adequate problem-solving contribute to positive experiences and the success of sustainable implementation. This study offers a rich understanding of day-to-day practices around implementing SCC in disability care organizations – an understanding that may be of use for the implementation of technologies in other care settings too.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241290399 - Supplemental material for The implementation of smart continence care for people with disabilities: A qualitative study of key stakeholders’ first-hand experiences
Supplemental material, sj-docx-1-dhj-10.1177_20552076241290399 for The implementation of smart continence care for people with disabilities: A qualitative study of key stakeholders’ first-hand experiences by Julia FE van Calis, Vivette JC van Cooten, Odile Smeets, Jenneken Naaldenberg, Brigitte Boon, Geraline L Leusink and Kirsten E Bevelander in DIGITAL HEALTH
Footnotes
Acknowledgements
We thank the participants for sharing their experiences with us.
Contributorship
JvC shaped the study design, collected data through interviews with the project leaders, analysed, and interpreted the data and drafted the manuscript. VvC shaped the study design, collected data through interviews with the ambassadors, analysed and interpreted the data, and drafted the manuscript. OS gave feedback on the topic lists and drafts of the manuscript. JN, BB, and GL supervised the research and co-authored the manuscript. KB supervised the research, assisted in the data analysis, and co-authored the manuscript.
Availability of data and material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study, as part of the cluster randomized trial, has been reviewed and approved by the Medical Ethics Committee of Radboudumc (NL72751.091.20).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by ZonMw, the Netherlands Organization for Health Research and Development (grant 80-85300-98-19110). No funds were received from the supplier Abena Healthcare.
Guarantor
JvC.
Informed consent
All participants received oral and written information about the study aim and procedure and gave their written consent.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.