
Abstract
Objective
To evaluate the design, implementation, and early impact of the Tasty Spoon™ – a hybrid digital–analogue, electrostimulation device intended to restore taste perception in people with dementia – and to identify the organisational and market conditions required for its routine use.
Methods
A ProcessOriented Holistic (PrOH) Modelling Methodology was applied across four phases:
1. Userneeds assessment through three focus groups (n = 28), semistructured interviews with individuals living with dementia (n = 10), caregivers (n = 5) and healthcare professionals (n = 15).
2. Iterative codesign and lab prototyping, informed by thematic analysis and smallscale electrogustometry studies (n = 15; people with dementia = 10, control = 5).
3. Feasibility testing the prototype in care-home dining routines to explore practicality, user acceptance, and caregiver workload, documented through field notes, post use interviews and caregiver workload diaries.
4. Regulatory and commercial pathway mapping (UKCA/CE precompliance review, 3i stakeholder analysis). Quantitative data were analysed descriptively; qualitative insights were integrated into the PrOH workflow to expose implementation pinchpoints.
Results
PrOH analysis identified three design features that underpinned acceptability – familiar spoon form, automatic activation on contact, and dishwashersafe construction – while highlighting outstanding challenges in cost control, training, and individual differences in taste sensitivity. Participants consistently reported that the Tasty Spoon™ made food ‘taste stronger’ and restored variety to meals they had previously found bland. Our research also highlighted the importance of co-developing ethical procedures in collaboration with people with dementia.
Conclusion
Early, smallscale evidence suggests that a sensoryfocused assistive device can complement existing cognitive and mobility technologies in dementia care by enhancing mealtime enjoyment and easing caregiver burden. Larger, rigorously controlled studies are needed to quantify nutritional and clinical outcomes and to refine personalised stimulation settings before widescale deployment.
Keywords
Introduction
There are currently 57 million people with dementia globally and nutrition is a fundamental aspect of their physical and cognitive health. 1 However, studies indicate that 50%–60% of people with dementia experience malnutrition due to sensory changes, such as diminished taste and smell, which result in reduced appetite and altered preferences.2,3 Neurological research suggests that degeneration of the gustatory cortex and taste receptors significantly reduces the ability to distinguish between flavours, leading to a reliance on excessive salt or sugar intake, which can contribute to hypertension, diabetes, and cardiovascular disease.4,5 This reliance on excessive salt intake results in people with dementia having the highest incidence rate in people with hypertension in the United Kingdom. 6 Langa et al. 7 report on the effect of sugar as a cause for type 2 diabetes, which is higher in people with dementia.
Olfactory dysfunction in neurodegenerative conditions is linked to dopamine deficiencies, further impairing food enjoyment and nutritional balance. 8 Marin et al. 9 show that olfactory dysfunctions appear years before motor symptoms and cognitive decline in people with dementia. Indeed, caregivers and individuals with dementia often report frustration and distress related to the loss of pleasurable eating experiences. This leads to daily food and drink dilemmas, which can be difficult for family carers to manage. 10 These predicaments have an emotional impact upon the carer, particularly when they feel that an important component of their relationship with the person with dementia had been lost through the sharing of meals. Despite the recognised importance of the relationship between nutrition and taste perception, existing assistive technologies in dementia care have largely overlooked taste, focusing instead on cognitive stimulation, mobility, and safety. 11 Yet individuals with dementia, report that one of the most overlooked areas of concern is the loss of taste perception. A recent survey by Alzheimer Research UK 12 demonstrated that more than 50% of respondents associated dementia with memory loss or forgetfulness, more than 20% with old age as well as other classifications ranging from personality to motor changes. Loss of taste, even though it can contribute to malnutrition, hypertension, type 2 diabetes or kidney diseases as well as diminished quality of life are not part of the public perception of dementia. 13 This gap highlights the need for alternative assistive technologies that focus on the sensory experiences that contribute to well-being.14,15
These creative technologies utilise the principles of digital design aimed at bridging the digital and the analogue thereby creating new sensory experiences16–18 [with a view to flavour and taste, see 19 ]. A growing body of research suggests that interventions that improve sensory engagement have psychosocial and emotional benefits, improving the overall quality of life for dementia patients.4–21 For instance, research by Cavanagh et al. 22 shows how such sensory engagements have physiological and psychological health benefits ranging from increased attention capacity, improved immune system to reduced stress and anxiety. Building on that, this study focuses on a creative technology that seeks to restore the sensory enjoyment of food.
The technology concerned (see Figure 1) called the Tasty Spoon™ offers a novel focus on sensory enhancement, an area less explored compared to cognitive or mobility-oriented solutions. The Tasty Spoon™ seeks to enhance mealtime satisfaction and social interaction during meals. 23

Tasty Spoon, Source: Authors.
Implementation challenges in healthcare and health markets
The implementation of technologies in healthcare contexts (from medical healthcare to well-being consumer markets) faces several significant challenges, many of which stem from how these technologies are researched and developed. One key issue is the lack of patient or consumer involvement in the development process, leading to technologies that do not align with real-world user-needs. 24 Electronic health records have been criticised for poor usability, increasing clinician workload rather than improving efficiency. 25 Studies have shown that when patients and clinicians are not engaged in the design phase, digital health solutions may fail to meet their expectations or support effective workflows. 26 Additionally, disciplinary boundaries between medical, engineering, and social sciences hinder the creation of transdisciplinary healthcare technologies. For example, artificial intelligence (AI) applications in diagnostic imaging often focus on technical accuracy without considering how radiologists integrate AI outputs into clinical decision-making. 27
Overcoming such disciplinary barriers requires closer collaboration between healthcare professionals, social scientists, and technologists to develop solutions that are robust and usable. Furthermore, many healthcare technologies are inherently complex demanding considerable behavioural changes from clinicians, patients, and administrators. The introduction of robotic surgical systems, such as the Da Vinci robot, illustrates this challenge; despite their potential benefits, they required extensive modification to traditional surgical workflows, making adoption slow and costly. 28 Addressing these challenges early necessitates a more transdisciplinary, user-centred approach to healthcare technology development. 29
The Tasty Spoon™
The Tasty Spoon™ is an assistive device designed to enhance the eating experience for individuals with dementia. Developed by researchers at the University of Sheffield's Management School, Healthy Life Institute, and the Advanced Manufacturing Research Centre (AMRC), the Tasty Spoon™ employs electrostimulation technology through a programmable microchip that emits sets of frequencies – being a digital–analogue hybrid – encased within a spoon-like design that discreetly accommodates the technical apparatus while ensuring ease of use, ultimately enhancing taste perception and restoring sensory engagement often diminished by dementia. 30 Research on electrostimulation has demonstrated that it can be useful to enhance taste perception. Studies have shown that targeted electrical stimulation of the tongue can activate dormant taste receptors, improving the ability to perceive sweet, salty, and umami flavours.31,32
Unlike digital monitoring systems or AI-driven applications, the Tasty Spoon™ is a hybrid technology combining principles of digital technologies with sensory-focused interventions that directly enhance the everyday experience of eating. Compared to alternative taste-enhancing methods such as flavour-modified diets, 33 electrostimulation provides a more individualised and adjustable solution, ensuring personalised taste enhancement. The aim of this paper is to examine the factors – such as organisational structures, regulatory environments, research development and end-user acceptance – that influence whether this solution can be adopted effectively. Rather than focusing primarily on the efficacy of the technology under controlled conditions, this type of implementation research investigates how to maintain efficacy in everyday practice. To address this aim a Process-Oriented Holistic (PrOH) Modelling Methodology will be used.
Methodology
Overview and frameworks
We applied PrOH Modelling to analyse, structure, and refine the Tasty Spoon™ development and implementation workflow for people with dementia.34,35 The work proceeded in two linked tracks: end-user service workflows and the interdisciplinary R&D workflow. Throughout, we used layered process maps and swim-lane diagrams rooted in holonic systems theory to represent interactions between micro-level actions and macro-level constraints. 36 We complemented these maps with input–transformation–output (ITO) process analysis and iterative stakeholder validation sessions.
Traditional implementation frameworks in healthcare tend to focus on identifying the forces that enable or block an innovation, whereas PrOH Modelling focuses on redesigning the system once those forces are known. The Non-adoption, Abandonment, Scale-up, Spread, and Sustainability (NASSS) framework 26 asks why many digital interventions stall by assessing complexity across seven domains that range from the clinical condition to the wider policy landscape. It offers a rich diagnostic picture but stops short of showing teams how to reengineer daytoday work. The Consolidated Framework for Implementation Research (CFIR) takes a different tack, 37 cataloguing more than 40 barriers and facilitators within five domains so that researchers can create consistent interview guides or survey instruments; yet CFIR, too, is primarily a determinant checklist. The UK Medical Research Council's (MRC) guidance on complex interventions provides a lifecycle view – from development to evaluation to implementation – but its main contribution lies in telling investigators when to iterate and refine rather than how to do the detailed redesign. 38
Process-Oriented Holistic modelling procedures
PrOH Modelling complements these frameworks by shifting attention from determinants to flows. PrOH Modelling is a systems-thinking approach designed to analyse, structure, and improve complex organisational processes. Rooted in holonic systems theory (Inspired by the work Arthur Koestler, 39 this part of systems theory stresses the complex dynamics of systems, where each ‘holon’, which is a unit that is simultaneously a whole in itself and a part of a larger whole, is both autonomous and interdependent. These systems exhibit self-organizing tendencies, meaning they can handle contingencies and maintain stability without external interventions contributing to their complexity and as such implementation challenges. 40 ) it uses layered process maps and swimlane diagrams to visualise how microlevel actions (a caregiver rinsing a spoon) interact with macrolevel forces (regulatory classification or procurement policy) in real time. 34 This designoriented stance means that a PrOH workshop can move directly from diagnosis to cocreation of alternative workflows (something NASSS, CFIR and the MRC guidance intentionally leave to subsequent phases). 41 By utilising ITO process analysis and ensuring stakeholder validation throughout, the methodology enhances consensus-building making it particularly effective. 42 As such, PrOH Modelling extends traditional healthimplementation frameworks by moving from enumerating barriers to engineering solutions. It visualises how microdesign decisions scale through organisational strata, offering a concrete bridge between innovation teams, frontline staff, and decisionmakers.
Matrix of study dimensions
To consolidate study outputs relevant to implementation planning, we compiled a summary matrix (Table 1) indexing four dimensions – health and well-being impact, caregiver burden, economic feasibility, and policy/regulation – and populated it with the corresponding considerations for the Tasty Spoon™ that emerged from our mapping and validation activities. This matrix was used as a study artefact to accompany the phase-wise process flow.
Holistic considerations for Tasty Spoon™, Source: Authors.

PrOH: Process-Oriented Holistic.
User journeys and stakeholder interactions
We mapped complete user journeys for people with dementia, informal caregivers, and healthcare professionals – from identification of need to sustained daily use – focusing on routine meal contexts for the Tasty Spoon™. We examined workflow transitions to capture how user choices intersected with organisational structures such as regulation, procurement, distribution, and production models. In parallel, we developed a stakeholder interaction map covering patients, caregivers, healthcare professionals, policymakers, and technology developers, tracing roles and handoffs across the product lifecycle. 43 To ensure person-centred alignment with routine care, we assessed familiarity, ease of use, and minimal disruption in daily routines. 44
End-to-end study phases
We organised the work into five sequential phases (Figure 2). Phase 1 covered ethical considerations, approvals, and safeguarding procedures. Phase 2 comprised user needs assessment using the journey maps and interaction maps to specify requirements for the Tasty Spoon™. Phase 3 involved person-centred design and iterative co-development, using PrOH artefacts to generate and refine alternative workflows and design specifications. 35 Phase 4 addressed prototyping and feasibility testing, combining quantitative experimentation with qualitative co-design feedback in iterative prototype cycles. 34 Phase 5 conducted a market-readiness assessment integrating regulatory classification, standardisation needs, and adoption pathways identified in earlier phases. Across phases, we synchronised software, clinical, and human-factors workstreams to support interdisciplinary development. 45

End-to-end workflow analysis in PrOH modelling for the development and testing of the Tasty Spoon™, Source: Authors. PrOH: Process-Oriented Holistic.
R&D workflow application
We applied PrOH Modelling not only to service delivery but also to our interdisciplinary R&D workflow. We decomposed parallel engineering, clinical, and human–computer interaction activities into linked subprocesses, modelled iteration points for usability testing, feedback incorporation, and regulatory documentation, and specified coordination mechanisms to reduce misalignment across disciplinary methods. 35 We used these models to schedule iterative testing and validation gates and to maintain traceability from user needs to design changes and verification activities. We reviewed adaptability requirements to support later-stage modifications as user needs evolved, informed by prior evidence on assistive technologies’ long-term performance. 36
Study design, duration, and setting
This study adopted a mixed-methods, multi-phase design combining qualitative research, participatory co-design, user testing, and laboratory-based feasibility testing. Participants were recruited through public channels. We used purposive, maximum-variation sampling to capture a range of dementia experiences (diagnosis, stage, living situation) and caregiving contexts. Participant recruitment and data collection took place between 2023 and 2025. Semi-structured interviews were conducted throughout this period, focus groups were held between September 2024 and April 2025, and user testing occurred between January and April 2025. User testing was conducted in Sheffield, United Kingdom. Interviews were conducted in person within the UK and online with participants based in the United States, Germany, and Japan.
Participants were recruited via an open media call (press and social media) and through partner organisations (Age UK, Alzheimer's Society) who distributed the invitation to their networks. Interested individuals contacted the team directly, we then screened for eligibility and arranged participation.
Our inclusion criteria (qualitative & lab testing) adults with a clinical diagnosis of dementia (any subtype) able to provide informed consent or, where appropriate, consultee agreement. They were able to eat soft foods safely and had a self-reported loss or diminished taste. We had to exclude people for the lab testing safety that had food allergies that would undermine the coherence of the food being served, but also people with health issues, such as, active electronic implants or severe dysphagia.
Qualitative data collection and analysis
The qualitative phase involved direct engagement with people living with dementia, caregivers, healthcare professionals, and care-home staff. Three focus groups were conducted, involving a total of 28 participants, with an average of eight to ten participants per session. Across these groups, 18 participants were people living with dementia, six were carers or relatives, and four were healthcare professionals.
In addition, 15 semi-structured interviews were conducted, including interviews with 10 people living with dementia and five carers. Among participants with dementia, there was near-equal gender representation, and all were aged between 80 and 85 years. All carers and healthcare professionals were female. Approximately 85% of participants identified as White British or White Other, 10% as South-East Asian, and 5% as Black British or Black African.
To identity themes, we used reflexive thematic analysis with iterative refinement and theme development. (Meaning saturation (no new nuances in theme interpretation) was reached by transcript 13 of 15. No new themes emerged after interview 13. However, we note in the Limitations that this was a small sample.) To enhance trustworthiness, we used analyst triangulation (CM; mixed-methods researcher; RA qualitative sociologist; BG public health researcher) and method triangulation (focus groups, interviews, stakeholder interviews). We also performed light member checking by sharing a short plain-English summary of themes with three participants (people with dementia = 2; carer = 1, professional = 1) to verify interpretive resonance.
Banding was derived qualitatively and triangulated across three focus groups, 15 interviews with people with lived experience, and 15 interviews with industry experts. For each stakeholder group, we assessed concrete cues for each dimension – Interest (proactive engagement, willingness to pilot), Influence (budgetary authority, procurement or policy levers), and Impact (directness and frequency of effect on outcomes and workflow). Ratings were agreed by consensus and are intended to guide prioritisation rather than quantify effect sizes.
Laboratory feasibility and electrostimulation testing
A within-participant laboratory feasibility study was conducted to estimate the direction and magnitude of change in taste perception and to inform future sample-size calculations, rather than to provide a fully powered efficacy trial. Ten participants with dementia and five control participants were recruited as a pragmatic pilot sample to assess safety, usability, and signal detectability under standardised tasting conditions.
The lab study was a within-participant feasibility test to estimate direction/magnitude of change and inform future sample-size calculations, rather than to deliver a fully powered efficacy trial. We selected n = 10 (dementia; five per session) (Participants were between 70–85, all white and equal in their gender distribution.) and n = 5 (control) (Participants were between 30–55, white and Hispanic, four men and one woman.) as a pragmatic pilot sample to assess safety, usability, and signal detectability under tightly standardised tasting conditions.
Participants tasted two foods (tomato soup and sweet porridge) in repeated spoonfuls (7 per food). For each spoonful the device delivered either active stimulation or sham (off). To minimise expectancy effects, stimulation status was concealed from participants and the on/off sequence followed a pre-generated pseudo-random list with the constraint of no more than two identical conditions in a row. The researcher operating the device knew the condition. Between spoonfuls we imposed a brief rinse/washout (e.g. water sip, ∼10–15 s) and standardised serving temperature and portion size. Based on sessions, we had 105 valid (Valid means that participants correctly assessed that they had heightened sensation when the spoon was turned on and changed perception when it was turned off.) data points. Using R alongside SPSS, we analysed pre–post changes for each questionnaire item using a two-sided Wilcoxon signed-rank test (α = 0.05), reporting the Wilcoxon V statistic (sum of signed ranks), exact p-values, the Hodges–Lehmann median paired difference with exact 95% CIs, and the rank-biserial correlation (rrb) as an effect size. In this paper, we report the taste perception result only. A full item-by-item analyses (e.g. enjoyment, flavour identification, appetite, social meal enjoyment) will be presented in a separate publication.
Ethical approval
This study received ethical approval from University of Sheffield's Research Ethics Committee (Approval No. [061428, 064796, 064862]). All participants provided informed consent, with additional considerations for individuals with dementia, ensuring their capacity to consent was assessed in line with ethical guidelines. Data collected from focus groups, interviews, and surveys were anonymized during transcription, and all identifying information was removed. The anonymized data was securely stored on a password-protected server at the University of Sheffield, accessible only to the core research team to maintain confidentiality and data integrity.
Results
The research and development of the Tasty Spoon™ emerged from the pressing need to address taste loss in dementia patients, a condition that significantly affects nutrition, well-being, and quality of life. Through a structured, multi-phase research process, the project refined its approach, seeking to ensure that the assistive device was not only effective but also practical for real-world application. This section presents key results from the development and testing phases, emphasising how the device was iteratively improved based on empirical testing, user engagement, and real-world feedback. The discussion explores implementation challenges and opportunities, culminating in an evidence-based strategy for integrating the Tasty Spoon™ into dementia care using a person-centred approach alongside established research frameworks for assistive technology deployment.
Ethical challenges
Ethical challenges nearly always happen during the research itself and we found one important ethical challenge during the early phases of the research. This problem was ensuring that all participants in the study fully understood their involvement and were capable of providing informed consent. Ethics reviewers raised concerns about how mental capacity would be assessed and whether all participants could fully comprehend the consent process, this was also discussed in one of the focus groups.
Participant 2 (person with dementia) argued against using the Mini-Mental State Examination (MMSE), stating: ‘It would be an insult to most people. Many of these questions are completely irrelevant’. Participant 3 (a carer) suggested a more person-centred approach: ‘Just a simple question– ‘Do you understand why you are here?’ – should be enough’. Participant 10 (a person with dementia) strongly criticised long and complex consent forms, noting: ‘I do hope you think of people as people, not scientists. Get it down to two pages – no more’.
As based on the strong criticism of the MMSE, it was decided to follow the suggestions of the focus group and to consider a more person-centred approach when gaining consent. This included to consider how a person is approached, whether they reply to the invitation themselves, and whether they require assistance to attend the interview. For instance, we contacted participants with dementia by e-mail, or they had already contacted us or had asked to be added to the newsletter, which offered a strong indication of their ability to understand the project. We also ask participants to read the Participant Information Sheet together with a carer, relative, or partner. The sheet is written in line with DEEP communication principles
46
(DEEP stands for the Dementia Engagement and Empowerment Project managed by the UK Network of Dementia Voices. They have developed a number of guidelines widely used in this area including: Writing dementia-friendly information or Dementia words matter: Guidelines on language about dementia. They are available at https://www.dementiavoices.org.uk/deep-resources/making-things-more-accessible/), an established approach for making written material dementia friendly. On the day of the interview, we would reiterate a brief summary of the Participant Information Sheet and ask whether anything is unclear. If we would have sensed that a participant appears confused or withdrawn, we would ask them to explain in their own words what they believe the study involves. We would emphasise that the interview can be stopped at any time and typically check after about 15 minutes that they are happy to continue. In general, it is important to watch for signs of tiredness or reduced concentration, such as speech difficulties or confused answers. If such signs arise, we would have considered it advisable to take a break or reschedule the interview. Furthermore, the interviews included a range of prompts in this context:
Pause the recording ‘Let's take a quick break. Can you remind me what we’re doing today?’ Re-check consent ‘Are you still happy for me to use what you’ve told me so far?’ If the participant is sure and comfortable Note the reconfirmation in field notes and continue.
These short, plain-English prompts reflect not only best practices, but follow the Mental Capacity Act (understand, retain, weigh, communicate) and HRA good-practice guidance.
Furthermore, participants also highlighted the importance of setting expectations for the Tasty Spoon. Some worried that unrealistic expectations could lead to frustration or disappointment if the device did not work as anticipated.
Participant 6 (a carer) and Participant 10 (a person with dementia) stressed the need for familiar caregivers to be present, as ‘any situation outside their comfort zone can be distressing’.
This feedback resulted in the creation of easy-to-read participant information sheet based on the abovementioned DEEP principles. We reinforced that every participant could bring a trusted caregiver and implemented a step-by-step user guide to manage expectations.
User needs assessment
The research began with an extensive analysis of user needs to identify the challenges associated with nutrition and mealtime experiences in dementia care, 47 which provided insights into the difficulties individuals face due to taste impairment, revealing common issues such as an overreliance on sugar and salt, reduced appetite, and a general loss of pleasure in eating.
One of the key findings from our user discussions was the variability in taste perception decline among individuals with dementia. While some participants had not noticed any changes, others described significant alterations in their sense of taste over time.
Participant 5 (person with dementia) noted: ‘I started to lose my sense of taste and smell about 10 years ago, but I didn’t relate it to dementia at the time. Some things I can’t taste at all, including very hot curries – I can just eat away like mad while everyone else is suffering after the first teaspoonful’.
Participant 7 (a relative) noted that her husband, who had dementia, ‘always found my grandchildren's chocolate and would devour the whole lot at night’.
Participant 11 (a carer
Furthermore, participants talked about not just the nutritional value of food, but also the meanings associated with food particularly on what it means to go shopping for food, food preparation and its consumption.
In the early design stage of this research, participants (see Figure 3) highlighted the social and psychological importance of ‘meaning making’ for people with dementia (Morgner et al. 2019). In particular, they focused on the role of emotions in the framing of mealtime experiences with food being a common feature. As a consequence of this, interviews were conducted with caregivers and healthcare practitioners to gather perspectives on dietary management strategies and potential solutions. The findings from this phase highlighted a clear demand for a non-invasive, easy-to-use intervention that could restore some level of taste perception without requiring complex modifications to daily routines. 11 These findings were instrumental in defining the core problem around which the design principles of the Tasty Spoon™ would be based. The goal became making sure that these principles aligned with the real-world needs as defined by its potential users.

Food is more than nutrition, source: research data.
Person-centred design and iterative co-development
In the co-design phase, the problem became focusing on making sure that the subsequent prototype of the device closely matched the needs of individuals living with dementia. Testing sessions included end-users (individuals living with dementia), their caregivers, and healthcare professionals, who assessed different aspects of the device's functionality, e.g. ease of cleaning or activation/deactivation and provided valuable feedback. A significant finding from these trials was the importance of familiarity in product design. Participants living with dementia responded positively to a design that closely resembled traditional spoons, this was because it minimised cognitive load and enabled a more ‘seamless’ integration into daily routines. One participant commented, ‘It feels just like my old spoon – I don’t have to think about using it’. Caregivers also emphasised the need for a secure grip, this resulted in refinements in the handle texture and curvature to accommodate those users with reduced dexterity. Furthermore, staff from care homes emphasised the need to easily activate the spoon as well as ensuring the ongoing activation of the Tasty Spoon™. As a result of these findings, the Tasty Spoon™ was subsequently designed without a switch-on and switch-off button. One carer in a care home mentioned that up to 200 meals can be served during mealtimes and turning on 200 spoons would be too demanding. The result was designing the Tasty Spoon™ with a contact sensor that would be activated and deactivated via skin contact.
Participants in the testing phase reported that the Tasty Spoon™ noticeably improved the taste of their meals, with several stating that foods that once seemed bland or flavourless regained distinctive taste characteristics. This enhancement led to increased food consumption, addressing one of the primary concerns of malnutrition in dementia patients. One caregiver noted, ‘I used to have to add extra salt to everything. Now my father eats without complaining about the taste’. This shift demonstrated the potential for improving both nutritional intake and meal satisfaction.
Prototyping and feasibility testing
Early prototypes of the Tasty Spoon™ underwent rigorous material testing and ergonomic refinements to ensure safety, durability, and comfort. A key challenge was finding the optimal balance between weight and ease of grip, as many individuals with dementia also experience reduced dexterity and muscle control. The initial designs, while functionally effective, were subsequently adjusted based on user feedback, leading to modifications in handle design, weight distribution, and electrode positioning for more effective stimulation and improved usability.
Material selection was another crucial consideration. It was identified that the final prototype should employ non-toxic, food-grade materials that met regulatory safety standards while ensuring resistance to frequent washing, including high-temperature dishwasher cycles. The durability of the electrostimulation mechanism was also tested to ensure consistent performance over time, with refinements made to protect electronic components from moisture and food residue buildup. One focus group participant highlighted the importance of hygiene, stating, ‘If it's going to be used every day, I need to know it won’t be a hassle to clean. I already have too many things to wash’. These findings led to enhancements in waterproofing and ease of maintenance.
Electrostimulation efficacy studies
A central aspect of the Tasty Spoon™'s development was its electrostimulation mechanism, designed to enhance taste perception for individuals experiencing diminished sensory function. ‘Electrogustometry’ 48 (Electrogustometry is the measurement of taste threshold by passing controlled anodal current through the tongue. It is a well-established as a clinical tool for the estimation of taste detection thresholds.) research has shown that low-frequency electrical stimulation can successfully amplify taste perception without discomfort. 49 Laboratory studies have assessed the effects of low-frequency electrical stimulation on different taste profiles, including sweet, salty, and umami flavours. Results have confirmed that mild electrical currents could successfully amplify taste perception; however, no such studies have conducted to define the relevant and optimal stimulation for people with dementia.
We collected information about their current sense of taste via an amended altered (The altered eating scale focuses on swallowing difficulties but is developed with a sense of considering eating impairments in general and could therefore be amended for this purpose.) eating scale that focused on taste. 50 We used questions from this scale to evaluate their impression after using the spoon (see appendix). Descriptive results of the changes, for instance, general taste perception or enjoyment of food, would see that averages for these rose by roughly two scale points, moving from the ‘poor / little enjoyment’ range into the ‘well / very enjoyable’ range after using the spoon. Due to the ordinal nature of the data (Likert scale), we conducted a Wilcoxon signedrank for this small sample. Compared with baseline, participants reported markedly better taste perception after using the Tasty Spoon™ (median 2 → 4 on a 5point scale; W = 0, p = 0.005, rrb = 1.00; using R's convention this corresponds to a large V since V = S+). Similar, statistically significant gains were observed for food enjoyment, ability to identify flavours, appetite, and social meal enjoyment (all p < 0.02). Across 105 trials, participants correctly (Typically, most mistakes would appear at the last test cycle, when the spoon was switched off, but people reporting being able to have a stronger sensation. While further research is needed, it can be assumed that the electrostimulation has a delayed effect that increases with its usage.) detected stimulation 84.8% of the time (95% CI 76.4%–91.0%). (For instance, one participant reported that only when eating extremely spicy food that this would trigger a minor sense of flavour, which involved eating porridge with chilli peppers.) In the dementia group, accuracy was 83.8% (67/80; 95% CI 73.8%–91.1%), while controls achieved 88.0% (22/25; 95% CI 68.8%–97.5%). These proportions with 95% confidence intervals serve as the effect sizes for the detection task. The findings of user testing highlighted that electrostimulation was most effective when using a certain frequency and providing multiple possibilities for tongue and receptors making contact. This led to refinements in the positioning of electrodes on the spoon, ensuring optimal contact with the tongue during regular use. Additionally, our testing demonstrated that the enhancement effects lasted for a short time after stimulation, allowing users to eat without continuous activation. One trial participant remarked, ‘I hadn’t tasted tomato soup properly in years – now it's like is has flavour again’. While such feedback underscored the profound impact the device could have on restoring lost sensory experiences, the results arise from a small sample and should be interpreted cautiously.
Stakeholder mapping using the 3i framework
Applying PrOH Modelling implies to view caregivers, residents, care-home administrators, and policymakers as interconnected and not in isolation to each other. This also aligns with a person-centred implementation approach and involves considering the person affected by a disease within their broader ‘network’ in order to develop a intervention plan that places the person and their network at the centre of the planning process. Based on such a systems approach, modifications to one element (e.g. simplifying Tasty Spoon usage) ripple through the entire network, reducing caregiver burden and potentially accelerating market uptake.
It is important to understand this interconnectedness in the development of the Tasty Spoon™, which implies to consider the involvement of a variety of people, for instance, those involved in the process of purchasing such technologies, cleaning, or charging them. Finally, raising awareness of the problem of loss of taste in people living with dementia involves raising awareness about this problem across a range of interest groups. In order to map these different groups and their interconnectedness, the 3i framework (Interest, Influence, and Impact) was used to identify key stakeholders relevant to the Tasty Spoon™.51,52 This was achieved through a number of workshops with specialist academics, policymakers and commercialisation experts. The framework subsequently developed helped to classify these stakeholders based on their level of engagement, power, and affectedness in relation to the Tasty Spoon™. To assist with this analysis, the stakeholders were initially differentiated into end-users, direct and indirect beneficiaries and influencers. Based on this initial differentiation, the following categories of stakeholder were identified:
End-users: People living with dementia
They are the ‘direct’ consumers of the effects of the Tasty Spoon™ in the sense that they experience a direct impact on nutrition, health, and well-being.
Direct beneficiaries
We identified three direct beneficiaries, such as, care homes as well as family members or relatives providing care, medical professionals, and medical care enablers. Care homes (private & public) as well as family members or relatives provide meals and care for dementia patients and as such have influence meal choices and dietary plans. Medical professionals (dementia nurses, GPs, dietitians, neurologists, psychiatrists, occupational therapists) directly impact the nutritional recommendations for people living with dementia. Medical Care Enablers like insurance companies influence accessibility and affordability of dementia-care solutions, including eating aids like the Tasty Spoon™.
Indirect beneficiaries
We identified three direct beneficiaries, such as, food & catering providers, for instance, Apetito, Compass Group, Sodexo, Holroyd Howe, Elior UK or Signature Dining could adopt or integrate the Tasty Spoon™ as part of their specialised meal solutions. Distribution Channels (Retailers) could provide the Tasty Spoon™ as well-being involved in building awareness for further nutritional supplements. Medical Suppliers, for instance, Mediquip or NHS Supply Chain could serve as potential partners for nutritional medical support (e.g. fortified foods, supplements).
Influencers
We identified two groups of influencers, such as, policymakers & public bodies as well as academic & research institutions. This might include local councils, chief medical officers, and ministerial departments, but also influential charities as they can shape regulations on nutrition and dementia care. Academic & research institutions can influence nutritional guidelines and innovation assistive technologies.
These PrOH modelling outcomes reinforced that people living with dementia should be prioritised in product design and engagement efforts (see Table 2). The 3i matrix shows that the people most directly affected by the Tasty Spoon™ – people living with dementia, their family carers and professional carehome staff – also score highest on interest and impact, but comparatively low to medium on influence. In contrast, medical professionals and policyshaping bodies (regulators, insurers, large retailers, catering suppliers) hold high or medium decisionmaking power, yet their personal stake in daytoday outcomes is lower. This split implies that successful implementation hinges on bridging a power–interest gap: the voices of highimpact, lowinfluence users need to be channelled through the highinfluence groups that control procurement, reimbursement, and menu planning.
3i framework stakeholder's Tasty Spoon: Source: Stakeholder Workshops.

This mapping also identified the role of regulators and policymakers for bringing any assistive device to market. Finally, the stakeholder mapping also pointed to need for a market implementation strategy and how market conditions are to be integrated into the development of the Tasty Spoon™’.
Caregiver and healthcare provider perspectives
Based on the stakeholder analysis, caregivers and healthcare professionals provided critical insights into how the Tasty Spoon™ could be incorporated into care routines with minimal disruption. While the Tasty Spoon™ is designed to be low-maintenance and user-friendly, studies indicate that caregiver burden often hinders the adoption of new interventions unless they are low-maintenance and easy to integrate. As noted by a carer: ‘We’re short-staffed most days. If there's a new device, it needs to be quick and simple. I don’t have spare minutes to fiddle with extra steps or complicated instructions’. Participant 13 (a carer
Institutional adoption also presents challenges as noted by a carer: ‘I have to manage everything from bathing to medication – mealtimes are already hectic. The idea of adding something new can feel overwhelming’. Participant 4 (a carer
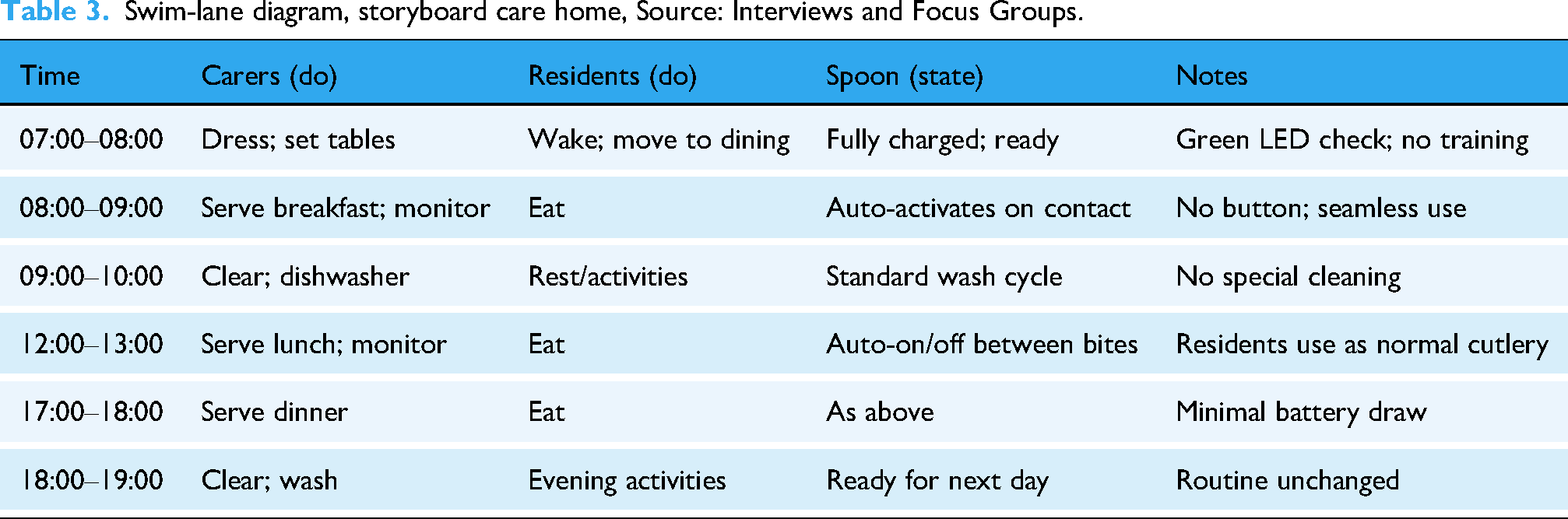
Furthermore, to understand the implementation of the device in daily routines, we co-created storyboards on daily routines in a care home in order to understand where the Tasty Spoon™ would be implemented and could be a source of disrupting these routines.
Our swim-lane storyboard (Table 3) serves as a holistic lens – a core PrOH modelling technique – to trace how micro-level daily tasks in care homes (dishwashing, setting tables) interact with macro-level frameworks (insurance reimbursement, procurement guidelines). By visualising these processes, we identified overlapping dependencies across holons – for instance, demonstrating that minimal training at the care-home level complements the broader need to show cost-efficiency for insurers. This enabled us to recognise the importance that the device required very little training, making it an immediately accessible solution for care-home staff and family caregivers. Unlike many other digital interventions, which often require interface learning and troubleshooting, the Tasty Spoon™ functioned as a simple, intuitive tool. This has the benefit of being able to reduce the burden on caregivers due to their interrelations and demand from other parts of the system. The hygiene and maintenance of the device were also identified as key problems as based on the storyboards. It was found that dishwasher compatibility was seen as an essential feature for use in institutional settings, ensuring that the device met hygiene standards without requiring additional cleaning effort. Prototyping therefore also involved research by using a commercial dishwasher, understanding temperatures in order to develop a heat-resistant design.
Swim-lane diagram, storyboard care home, Source: Interviews and Focus Groups.
Market-readiness assessment
By mapping micro-level mealtime workflows onto macro-level regulatory procedures within the PrOH framework, we also uncovered the need to ensure dishwasher compatibility (a caregiver-driven need) also streamlined the device's journey toward regulatory compliance (an organisational-level concern). This involves navigating a complex regulatory landscape, especially in well-being and consumer technology sectors. Consultations with legal advisors concluded that the Tasty Spoon™ should be considered a consumer aid with medical endorsement, operating in a regulated environment where compliance with safety, hygiene, and product reliability standards is mandatory. In the UK, compliance with CE and UKCA marking standards will ensure that the product meets regulatory guidelines for electrical safety and food-grade materials. Consequently, this involved a compliance review of existing UKCA (UK Conformity Assessed) marking procedures. This mapping process involved identifying the applicable UKCA marking regulations, the relevant requirements in the regulations and supporting standards which dealt with the particular hazards present to assess the equipment for compliance with these requirements by inspection, testing, calculation, and assessment, while recording any non-compliances and rectifying any problems, or alternatively to document how an equivalent level of compliance can be achieved through other means. This mapping resulted in the compilation of a ‘Technical File’ containing the relevant technical details, sufficient to demonstrate compliance with the directives and standards. Furthermore, this work is not only crucial in securing regulatory approval but also in maintaining ongoing compliance as the product evolves. Future modifications to the design, such as enhanced battery life, alternative materials, or software-driven personalisation features, may require additional regulatory review. Developing a clear compliance roadmap early in the commercialisation process was therefore essential for understanding implementation challenges, such as, barriers to market entry.
Market implementation: Market education and market penetration
PrOH modelling also involved mapping the integration of the Tasty Spoon™ into relevant markets. This type of explorative market research involved understanding how different types of consumers learn about innovations as well as understanding which consumer are most likely to adopt the technology. A product's success is not determined solely by its effectiveness but also by its ability to sustain consumer interest, compete with emerging alternatives, and remain financially viable. Sustainability is especially relevant when considering potential future iterations of the product, such as models designed for broader demographics, including cancer patients or individuals with aging-related taste loss. It was therefore important to understand which consumer groups are most likely to adopt certain technologies as well as understanding factors that could prevent such an adoption. To deliver this agenda, a detailed value proposition with different hypothesis was developed. Based on this, we conducted semi-structured interviews with a variety of professionals (n = 15) working in the manufacturing of medical devices, market research, procurement, local authorities, and care homes. Based on this data, we were able to consider different consumers in terms of the adaptation of the technology. It became necessary to differentiate between innovators and early adopters, as well as early majorities, later majorities and laggards. 53
Adoption moves from curiositydriven testing (Innovators) to evidencedriven purchase (Early/Late Majorities) and finally to mandatedriven compliance (Laggards) (see Table 4). Moreover, Innovators and Early Adopters act as opinion leaders; their public endorsements are the fastest way to pull the Early Majority across the line. Furthermore, financial constraints grow stronger down the curve; packaging the product with costsharing or grant options accelerates LateMajority uptake. While Rogers’ model (see Table 4) is helpful in understanding different market segments integrating a PrOH analysis complements it, because it enabled us to understand how early adopters (macro-level influencers in private care facilities) shape micro-level acceptance (caregiver training), which in turn fosters broader adoption. This highlights that the diffusion is not purely linear but also shaped by the holarchy of care. Based on the results of this analysis, it was concluded that early adopters, such as leading healthcare professionals, private dementia-care facilities, and policymakers, will play a vital role in advocating the device. Since they hold influence in their respective fields, securing endorsements from this group could enhance credibility and demonstrate the Tasty Spoon™'s foundation in emerging, research-driven practices. This insight subsequently informed a market strategy aimed at developing the implementation of Tasty Spoon™ in collaboration with private care facilities and specialised home care providers. For example, offering pilot programmes and early access would provide these organisations with a competitive advantage while generating real-world case studies for further market penetration. Furthermore, it has become apparent that additional research will need to be conducted into developing a compelling analysis of the problems surrounding the need for the Tasty Spoon™, this research will be based on narrative interviews with people living with dementia and their caregivers. This approach seeks to capture the personal stories through which individuals make sense of the impact of declining taste on their everyday lives. Such research is central to person-centred care.
Diffusion of innovations, Source: Modelled after. 33

In addition to this exploratory market research has been conducted to understand different routes to market, involving interviews with stakeholders in the United Kingdom, Germany, Japan, and the United States. The findings revealed significant diversity in how knowledge is distributed. For instance, we discovered critical pinch-points where care-homes demand near-zero complexity for daily use, yet consumer-tech manufacturers propose adding data-logging features for market competitiveness. Furthermore, we discovered that knowledge distribution is not a unidirectional pipeline; rather, each stakeholder – ranging from individual occupational therapists to entire care-home networks – collects, adapts, and re-shares insights about the Tasty Spoon™. For instance, while smaller clinics rely on specialised conferences for critical updates, larger care-homes leverage their in-house innovation leads to evaluate the device's suitability before disseminating training to staff. This multilevel interplay underscores how a market education strategy must address individual needs for learning, from straightforward, on-site demos to broader policy endorsements. For instance, some early adopters, such as occupational therapists, emphasised the importance of selective conferences and trade shows, while others highlighted the role of innovation leads in larger private care homes. Training was also identified as a crucial factor in acquiring new knowledge. As such, market implementation will depend on developing a market education strategy, which includes presenting the Tasty Spoon™ at relevant conferences and developing training materials to support its implementation.
Discussion
Principal findings
This study shows that a lowcost, electrostimulation spoon can be folded into everyday dementia mealtimes with very little disruption. Participants consistently described a return of ‘missing’ flavours, while caregivers noticed a smoother serving routine because the device looks and behaves like familiar cutlery – no buttons, no special cleaning steps. PrOH modelling helped reveal why those microlevel design choices mattered: when carers found the spoon easy to clean or charge, procurement managers and regulators also viewed it as lowrisk and lowmaintenance, accelerating organisational buyin. In short, usability at the table translated into credibility at policy level.
Comparison with prior work: The significance of creative sensory-based assistive technologies
Recent research highlights the importance of digital as well as multisensory interventions in dementia care. 54 However, many assistive technologies for dementia emphasise cognitive prompts, wandering alerts, or tremor compensation. Taste rehabilitation has remained largely unexplored. Flavour-enhanced diets and olfactory stimulation target mealtime enjoyment indirectly – by modifying food or the ambient sensory context – whereas the Tasty Spoon™ delivers on-tongue augmentation of perceived taste intensity. Reviews of sensory programmes in dementia report heterogeneous methods and mixed, mostly small-study effects on appetite, intake, or mood (e.g. multisensory/olfactory activities, environmental cues).11,30 Flavour enhancement can help, but common practices (extra salt or sugar) may clash with comorbid hypertension and diabetes, issues disproportionately affecting people with dementia; the Tasty Spoon™ aims to improve palatability without adding sodium or calories. Olfactory approaches are mechanistically plausible – smell loss is common and often precedes cognitive decline – yet gains tend to be psychosocial and context-dependent and require ongoing materials and staff time.9,30,55
By contrast, electrogustometric augmentation directly stimulates gustatory pathways and showed high detection accuracy in our pilot while preserving routine workflows (no recipe changes, no extra cleaning/training beyond dishwashing). Furthermore, the Tasty Spoon™ may present a scalable and sustainable model that could be expanded to cancer patients, post-COVID-19 recovery, and age-related taste loss. However, our evidence is early phase (small, convenience samples) and we have not yet demonstrated downstream clinical outcomes (e.g. sustained intake, weight, metabolic markers).
Nevertheless, the development of the Tasty Spoon™ represents a significant departure from conventional assistive technologies that primarily focus on monitoring, mobility support, and cognitive interventions. While digital technologies have played an important role in dementia care, they often do not directly address sensory and nutritional challenges, leaving a critical gap in holistic care approaches. Our findings echo multisensory–interaction research showing that discreet, tonguebased electrostimulation can modulate flavour perception without altering the food itself. 17 They also complement Manera et al.'s 21 observation that sensory enrichment improves mood and social engagement at the table. Unlike stabilising spoons designed for Parkinson's tremor, the Tasty Spoon™ targets the gustatory deficit directly, aligning with a personcentred movement toward maintaining pleasure and dignity in dementia dining.
By prioritising taste enhancement and meal enjoyment, the Tasty Spoon™ introduces a novel dimension to assistive technology – one that combines principles of digital creativity and sensory impact. This shift in focus aligns with broader discussions in dementia-care research, where quality of life, dignity, and social engagement are increasingly recognised as equally important as safety and cognitive support. 56 Food is not only a nutritional necessity but also a source of pleasure, memory, and social connection. Enhancing taste perception in individuals with dementia restores a fundamental human experience, helping to maintain appetite, nutritional intake, and so has the potential to improve well-being. This sensory-based intervention thus complements existing digital solutions, potentially presenting a more holistic approach to dementia care. Furthermore, the Tasty Spoon™ provides an alternative approach to assistive technology design, illustrating that low-cost, non-invasive solutions may address certain sensory needs similarly to more complex digital interventions. As dementia research continues to explore new frontiers in sensory rehabilitation, the success of the Tasty Spoon™ offers insight into how similar approaches could be applied to other sensory impairments, such as hearing loss, touch sensitivity, and olfactory dysfunction.
Limitations
The present work drew on a small, convenience sample of residents and carers in two care settings and relied mainly on selfreported sensory improvement and observer field notes. We did not quantify nutritional intake, biochemical markers, or longterm health outcomes, nor did we test the device in homeliving individuals with dementia. These factors limit generalisability and preclude causal claims about clinical benefit. This requires further clinical research. Furthermore, the altered eating scale 50 is validated for use in altered eating, for instance, due to swallowing problems, this is the first time it has been used in altered taste. As such further work is needed to validate the scale for use in this way. We also note that recruitment via charities and media may favour motivated participants. These factors mean the present results are best viewed as signal-seeking and hypothesis-generating, a fully powered, preregistered, randomised, double-blind crossover with longer washout and broader menus will be required to estimate effects with adequate precision and to establish clinical relevance.
Conclusion
The aim of this paper is to explore how addresses how the PrOH Modelling Methodology was applied to optimise the development, adoption, and integration of an assistive technology, such as the Tasty Spoon™. The focus was on mapping top-down or bottom-up flows but reciprocal interactions, for instance, how feedback from the micro-level (carers finding the spoon easy to clean) influenced macro-level marketing or policy decisions (ease of regulatory compliance). This in turn impacted on the overall implementation dynamics.
The Tasty Spoon™ was subsequently developed to bridge a critical gap in dementia care by restoring taste perception through combing principles of digital creativity to modify and improve sensory experience. What we found is that is that implementation challenges are not resolved in a linear way or resolved by identifying individual problems, but that the changes in one element change the overall dynamics of implementation. This required to approach this technology in a more iterative designed using the PrOH Modelling Methodology.
The development and implementation of the Tasty Spoon™ underscores the potential of sensory-based assistive technologies in address previously overlooked challenges in dementia care. While assistive technologies in this field have predominantly focused on cognitive and physical support, the Tasty Spoon™ shifts attention toward taste perception and nutritional well-being, seeking to address the critical issue of malnutrition and its cascading health effects. The research findings indicated that electrostimulation-enhanced taste perception can effectively improve food intake, meal enjoyment, and overall quality of life for individuals experiencing dementia-related taste loss. Furthermore, the implementation of the PrOH Modelling Methodology enabled a detailed assessment of how the device could be follow a person-centred design, focusing on ease of use, and compatibility with existing care practices, while examining how these are embedded within a wider regulatory and professional field. Understanding how these various problems are defined has contributed to assessing its viability as a real-world intervention.
Based on the PrOH methodology employed in this project, we were able to devise a process that would outline the different system levels and their interconnectedness, for instance, micro-level elements, e.g. daily mealtime routines, are interlinked with meso-level processes, e.g. care-home or organisational processes, as well as, macro-level structures, e.g. policy and regulatory environment (see Table 5).
Key insights from the PrOH model analysis, Source: Authors.

PrOH: Process-Oriented Holistic.
Each phase contributed valuable insights that informed refinements in device design, electrostimulation efficacy, and integration strategies. Testing with individuals living with dementia confirmed that the Tasty Spoon™ is well received, easy to adopt, and capable of addressing the sensory challenges associated with dementia-related taste decline. Feedback from caregivers and healthcare professionals further emphasised its potential to fit seamlessly into care routines, provided that sufficient training and awareness campaigns accompany its rollout. However, several barriers to implementation were also identified. There remains variability in individual taste responses, a need for regulatory compliance, the challenge of caregiver engagement, and cost considerations have emerged as key obstacles that must be addressed for successful large-scale deployment. Despite these challenges, the project has considered a variety of challenges for further refinement, commercialisation, and integration into dementia-care frameworks.
The future of the tasty spoon™: Implementation implications
For carehome managers, the message is pragmatic: if a sensory aid can be dropped into the existing mealtime workflow – same dishwasher rack, no extra training modules – it is far more likely to survive beyond the pilot phase. Designers of future devices should treat ‘looks like ordinary cutlery’ as a critical usability requirement, not a cosmetic afterthought. Policymakers and commissioners might consider adding sensorysupport tools to dementiacare equipment lists, positioning taste rehabilitation alongside mobility aids and memory alarms. Recognising taste loss as an avoidable contributor to malnutrition could also unlock broader compensation pathways.
While this article has outlined key steps for the implementation of the Tasty Spoon™ further work needs to be done to ensure successful scale-up and commercialisation, several strategic steps must be undertaken. One key area for further development is expanding product customisation. While early findings confirm that electrostimulation is effective in enhancing taste perception, individual variability in sensory response suggests that further refinements in stimulation settings could optimise effectiveness across a broader user base. Research into adaptive electrostimulation technologies, where the device automatically adjusts intensity based on user feedback, could enhance its personalisation and usability. Additionally, expanding the application of the Tasty Spoon™ beyond dementia care presents an opportunity for broader market adoption. Many individuals beyond the dementia population experience taste loss due to chemotherapy, COVID-19, ageing, or neurological conditions. Developing variant models tailored to different user needs could significantly broaden the device's impact and commercial potential. Further research is also needed to assess the long-term health benefits of sustained use. While initial trials confirmed short-term improvements in meal enjoyment and food intake, understanding whether these benefits translate into better long-term nutritional and health outcomes requires larger-scale clinical studies. Collaboration with nutritionists, geriatricians, and public health experts will be essential in quantifying these impacts and making a case for healthcare adoption.
Finally, piloting the spoon with other populations that experience taste loss (e.g. chemotherapy patients, postCOVID cases, Parkinson's) would test its versatility (This could consider integrating other technologies, for instance, self-stabilizing spoons tailored for individuals with Parkinson's disease.) and support scalable manufacturing.
Footnotes
Acknowledgements
We would like to thank the anonymous peer-reviewers for their comments. AI had been used to proofread previous versions of the paper and to format tables.
Ethics approval
This study received approved from University of Sheffield's Research Ethics Committee (Approval No. [061428, 064796, 064862]).
Consent for publication
Written informed consent for publication of the participants’ anonymised quotations was obtained from all participants or, where appropriate, their legal guardians.
Author contribution(s)
CM contributed to the conceptualisation, formal analysis and writing and BG to the review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alzheimer's Society Accelerator Funding No. 184825
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Due to GDPR, data cannot be shared publicly.
Permission to use all applicable tools/questionnaires
The authors hold the necessary permissions and licences to use all applicable tools and questionnaires employed in this study.
Permission to use the trademarked product (tasty spoon™)
The corresponding author confirms they hold the relevant rights and permissions to use the trademarked product, Tasty Spoon™.
Pre-testing questionnaire (Appendix E. Altered Eating scale)
1. How important is it for you to be able to enjoy the flavours, tastes, and textures of food?
2. To what extent is your ability to enjoy your food impacted by your ability to taste it?
3. How well can you taste different flavours (e.g. sweet, salty, sour, bitter)?
4. How important is it for you to eat the food you like?
5. How is eating the food you like impacted by your tasting difficulties?
6. To what extent is your ability to make these choices about food impacted by your tasting difficulties?
It give me greater choice as I can eat more extreme flavours, like eating the whole lime
8. How important is it for you to be able to socialise when eating food?
(e.g. eating out with friends, family, or work colleagues.)
9. To what extent is your ability to socialise around food impacted by your tasting difficulties?
(e.g. like you are not enjoying your food.)
10. How important is it to you that eating is associated with positive emotions?
11. To what extent is your ability to experience positive emotions while eating impacted by your tasting difficulties?
(e.g. unable to comment on other people's cooking skills or unable to share recipes or talk about food in general.)