
Abstract
Objective
With the coronavirus disease 2019 pandemic exacerbating mental health concerns, the prevalence rates of anxiety and sleep problems have increased alarmingly among youth. Although 90% of patients with anxiety experience sleep problems, current interventions for anxiety often do not target sleep problems in youth. Given this lack, we designed the SMILE app, an intervention that addresses both anxiety and sleep problems simultaneously.
Methods
As users’ perspectives are essential to ensure app engagement and uptake, the features, designs, and functions of the SMILE app were evaluated using a participatory app design approach. Participants (N = 17) were youth aged 15 to 25 who reported co-morbid anxiety and sleep issues above clinical thresholds. After completing an online screening survey assessing demographics, anxiety, and sleep problems, participants shared app feedback through group-based, semi-structured co-design sessions. Qualitative analyses were conducted to identify common themes from participants’ feedback.
Results
While participants expressed enthusiasm for the SMILE app's features, particularly the Visualization, Journaling, and Psychoeducation features, and their variety, they criticized the design aspects of the app, such as the font and text amount. Most participants stated they would use the SMILE app or recommend it to a friend.
Conclusion
By actively involving the target population in the design process, the SMILE app has the potential to notably improve the mental well-being of youth, though further research and development are required to realize this potential fully.
Introduction
Anxiety disorders are among the most common mental health problems among youth, with an estimated 6-month prevalence of 11–15%. 1 Additionally, the coronavirus disease 2019 pandemic has further exacerbated the prevalence of anxiety problems among youth.2,3 Anxiety problems in youth are associated with a variety of negative outcomes (e.g. alcohol abuse, suicide, academic failure).4–6 Many youths with anxiety problems also experience additional health problems, for example up to 90% of these youth report sleep problems, 1 which can aggravate their anxiety. 7 The relationship between anxiety and sleep problems is theorized to be bidirectional. Sleep problems may contribute to the development of anxiety problems, which in turn may be antecedents of sleep problems. 8 Previous empirical studies have supported both pathways. De Bruin et al. 9 found that anxiety problems in youth are associated with significantly longer sleep onset latency and significantly shorter sleep duration. Despite the high overlap and interrelatedness of anxiety and sleep problems in youth, standard interventions for anxiety do typically not target sleep problems. 8
Moreover, many youths with sleep problems face barriers to receiving services. 10 Yet, limited access to mental health services and long wait times can profoundly impact youth by decreasing treatment motivation, prolonging physical and emotional distress, and exacerbating mental health conditions.11,12 Mental health apps have been suggested as a possible solution for addressing unmet needs for youth mental health support.11,13 Many youths even prefer app-based solutions 9 over traditional services as mental health apps are easily accessible, anonymous, and can monitor mental health symptoms in real-time to provide immediate support. 14 Recent reviews demonstrated that mental health apps can effectively reduce anxiety in youths, but the reviewed apps rarely target sleep problems. 15 Some available mental health apps address both anxiety and sleep problems. However, these apps are primarily designed for, and used by adults, and are often static in design (i.e. do not change based on user input). 16
The few youths who use these adult-targeted apps find them difficult to navigate and commonly expressed dislike for the lack of personalization. 16 Personalizing mental health apps to increase youth user engagement can be challenging. New advances in technology, such as mobile sensing (i.e. the collection of behavioral data through mobile phones), 17 may help advance the personalization of interventions to the individual needs of users. Specifically, mobile sensing offers unprecedented opportunities to identify and understand distinct areas where youth experience problems by passively recording their daily life behaviors. 18 Using mobile sensing data, intervention features displayed to youth users could be highly tailored to their problem areas. Thus, mobile sensing offers promising avenue to address the lack of targeted and personalized e-mental health interventions for youth experiencing anxiety and sleep difficulties.
Sleep tracking has been shown to be a highly effective component of sleep interventions. 19 Sleep can be successfully measured via mobile sensing. Specifically, mobile-sensed sleep measures have recently been shown to correlate well with actigraphy data and sleep diaries. 20 Mobile sensing can also help uncover maladaptive behaviors that could contribute to anxiety and sleep problems. For example, mobile sensing data can help identify avoidance patterns that may hinder youth in overcoming their anxiety problems (e.g. lack of social contacts via call and text message logs), 21 spending time primarily at home via GPS data.17,22 Logging screen activity, noises, and light mobile sensing can also uncover bad sleep habits, such as high screen time before bed or a very loud environment. 23 Most intervention apps rely on self-reports for behavior tracking. 24 However, the completion of daily ratings may be too burdensome, especially for youths.25,26 Passive tracking could reduce the perceived usage burden and potentially help mitigate app attrition.25–28 While mobile sensing may raise certain privacy concerns, a recent survey outlined the acceptability and usability of mobile sensing by youth patients and their parents to increase awareness of poor habits and its potential to promote behavioral change. 28 In line with these concepts, the Smile for Life (SMILE) app was developed, leveraging mobile sensing to measure maladaptive behavior and personalize intervention content for youth with anxiety and sleep problems.
To ensure that the newly designed SMILE app could truly address the needs of youth with anxiety and sleep problems, a co-design study involving 17 youth was conducted. This allowed youth with sleep and anxiety problems to see and evaluate the app and ultimately influence the app's design and features. Evaluating the SMILE app with youth users was imperative, as research has shown that independent of their evidence-based content, mental health apps are often not well adopted. Approximately 70% of patients who used or were invited to use mental health apps stopped prematurely or declined, with lack of engagement cited as a major contributor. 29 The objectives of the study thus were to examine youth users’ perspectives to identify facilitators and barriers of use and to reveal specific features, designs, and functions that may help with engagement and uptake of the SMILE app.
Method
This qualitative co-design study was approved by the IWK Health Centre research ethics committee (approval no. 1026748) on 11 May 2021.
Participants
Study participants included youths between the ages of 15 and 25 who self-identified as experiencing co-morbid anxiety and sleep problems and were able to speak and read English fluently. Participants were excluded if they did not own a smartphone. Youth were recruited using two approaches. First, advertisements were posted at local clinics in Halifax, NS, Canada, where the study took place. Second, advertisements were posted on various social media platforms (e.g. Instagram, Facebook, Twitter). Recruitment was conducted between November 2022 and April 2023. Seventeen youth attended co-design sessions. Participants who attended co-design sessions were compensated for their time with a $20 Amazon gift card.
Procedure
The screening, consent, and online survey were completed online via the secure Research Electronic Data Capture (REDCap) 30 platform. Interested youth who clicked on the hyperlink embedded in advertisements were automatically directed to an eligibility screener. The screener included seven items, which asked participants their age and six yes or no items that assured participants (1) experienced anxiety, (2) experienced sleep problems, (3) could read English, (4) could speak English, (5) currently owned a smartphone, and (6) were interested attending a co-design session. Interested participants who met inclusion criteria were then guided through a detailed study information and consent process, which was necessary to participate. Once participants provided their written (electronic) informed consent, they reported their demographic information, anxiety, and sleep problems in the form of a short survey. After survey completion, participants were invited via email to participate in one-on-one or group-based co-design sessions. The co-design sessions were conducted in person at the IWK Health Centre and via Zoom by two of the authors (M.O. and A.K.). The sessions lasted approximately 60 min and were carried out using a semi-structured guide. The guide facilitated author' questions and included demonstrations of SMILE app prototypes to obtain relevant user feedback on the SMILE app and its features, as well as participants’ general opinions on mental health apps and their features (see Supplemental Material S1). During sessions, participants also had opportunities to interact with SMILE app prototypes. All sessions were audio recorded and transcribed verbatim. Changes or recommendations to the sleep intervention features were prioritized for future development if it was mentioned by at least 10% of the sample during sessions.
Measures
Demographic questionnaire
The demographic questionnaire asked participants to report their age, gender, sex, ethnic or cultural heritage, and community (i.e. rural, town, city under/over 500,000).
Screen for child anxiety related disorders
To measure anxiety problems, participants who reported that their age was between 15 and 18 completed the validated 41-item Screen for Child Anxiety Related Disorders (SCARED). Participants responded to questions about their anxiety symptoms/experiences as not/hardly ever true (0), somewhat/sometimes true (1), or very/often true (2). The SCARED demonstrates good internal consistency (α = 0.86–0.97) and good discriminant validity between anxiety and other disorders and within anxiety disorders for generalized and social anxiety. 31 All youth participants endorsed scores greater than or equal to 25 indicating the presence of an anxiety disorder.
Screen for adult anxiety related disorders
To characterize the anxiety problems, participants who reported their age was between 19 and 25 completed the validated 44-item Screen for Adult Anxiety Related Disorders (SCAARED). Participants responded to questions about their anxiety symptoms/experiences as not/hardly ever true (0), somewhat/sometimes true (1), or very/often true (2). The SCAARED demonstrates good internal consistency (α = 0.90) and good discriminant validity between anxiety and other disorders and within anxiety disorders for generalized and social anxiety. 32 All adult participants endorsed scores greater than or equal to 25 indicating the presence of an anxiety disorder.
Insomnia severity index
To obtain information on sleep problems, all participants were asked to complete the validated seven-item Insomnia Severity Index (ISI). Participants were asked to report the severity of their difficulty falling asleep, staying asleep, and waking up too early on a 4-point scale (i.e. 0 = none, 4 = very severe). They also were asked to report how satisfied they are with their sleep, how noticeable they believe their sleep problems are, how worried/distressed they are about their sleep problems and the extent to which their sleep problems interfere with their daily functioning. The ISI demonstrates good internal consistency (α = 0.90 and 0.91) and good discriminant validity between symptoms of insomnia. 33 Scores between 8 and 12 indicate subthreshold insomnia, scores between 15 and 21 indicate moderate clinical insomnia and scores between 22 and 28 indicate severe clinical insomnia. All participants endorsed at least subthreshold insomnia levels (n = 4), with a majority endorsing clinical insomnia (n = 13).
Co-design interview guide
The author-created interview guide (see Supplemental Material S1) was adapted from the framework of Werner-Seidler et al. 34 in consultation with youth, service providers, and clinician-scientists. The interview guide asked participants about their use of mobile apps, and their opinions of the SMILE app (e.g. which features they liked or disliked, what they would improve, if they would recommend it). The same interview guide was used during all group interviews. Co-design session interviews were conducted by M.O. (a male post-doctoral fellow, PhD) and A.K. (a female undergraduate research assistant, B.Sc.). Interviewers expanded beyond the interview guide (i.e. probes and prompts) throughout each interview to promote elaboration on given responses. To ensure that input was received from all participants, interviewers sought to encourage responses through direct questioning, provision of elongated pauses, and reflective listening.
SMILE app
The SMILE app (see Figure 1) was developed from a cumulative research and parallel consultation approach. Consultation with youth consultants, service providers, and clinician-scientists informed the initial prototype app development. App features were consequently developed to target anxiety and sleep problems via evidence-based techniques in line with the suggestions of the consultants. For example, the Psychoeducation feature was added to help youth learn about the different facets of anxiety problems. 35 The Journal feature was included considering the long-term benefits evidenced by expressive writing. 36 Based on the wishes of youth consultants, the Journal feature enables searches of previous entries and supports speech-to-text functions. The Relaxation and Guided Meditation features support self-regulation and decreased physiological arousal, 37 and diverse types of mediations presented in different modalities were included as suggested by the consultants. The Mood Tracking feature was designed to encourage attention toward positive (versus negative) moods and help users understand and manage their emotions. 38 The Visualization feature was included to increase self-awareness of daily behaviors 39 (i.e. sleep, physical activity, and screen time), as many consultants expressed an interest in simple visualizations. The Challenges feature was included to motivate exposure to feared stimuli so that users learn and understand that their anticipated negative consequences are ill-founded. 40 Service providers and clinician-scientists not only highlighted the value of the Challenges feature but also remarked on the need to ensure that the selected Challenges are not too demanding for users. Accordingly, the Challenges features only present tasks of moderate complexity and intensity. The Goals feature was designed to stipulate behavioral activation.41,42 The final version of SMILE app is currently planned to be accessed by users as a stand-alone University Health Services resource.
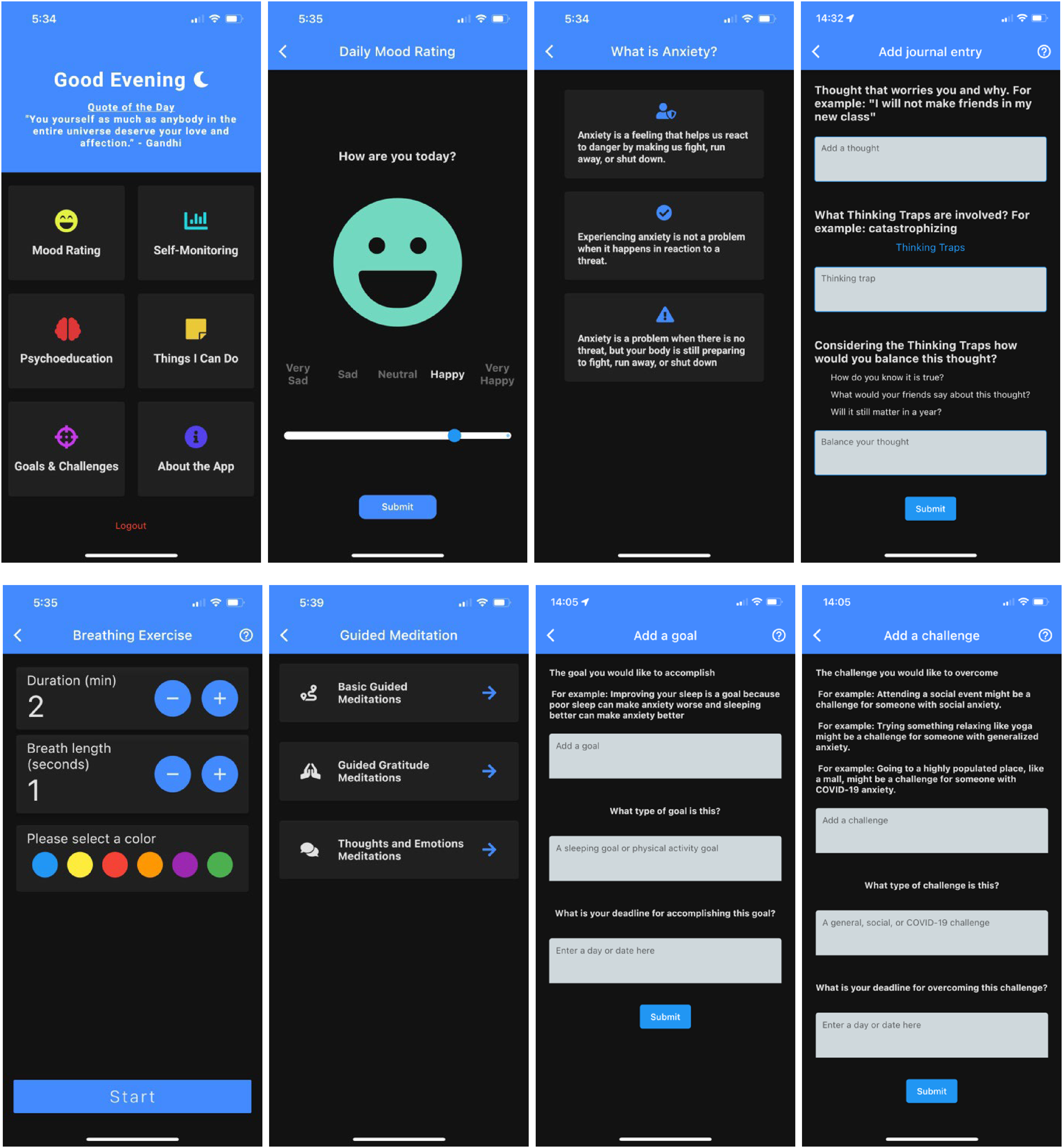
SMILE app.
Data analysis
The analysis consisted of a mixture of quantitative and qualitative methods and took place between April 2023 and October 2023. Descriptive statistics were used to characterize the sample in terms of demographic characteristics, anxiety, and sleep problems. M.O., M.C., and H.M. were the only research team members involved in data analysis. M.O. checked transcripts for accuracy before data analysis and imported them into NVivo Software 12. Inductive content analysis was used to analyze the transcripts of the co-design sessions. 43 Content analysis was guided by the descriptive methods suggested by Braun and Clarke 44 and Hsieh and Shannon. 45 Each coder familiarized themselves with the data (i.e. read through all transcripts), and then each coder generated initial codes. Each coder then re-read the transcripts and coded instances of each initial code. These steps were all done independently. Coders M.C. and H.M. each independently coded half of the transcripts for reason of availability, while coder M.O. independently coded all transcripts. All coders then met to review and revise codes. Finally, codes were defined and categorized by consensus among coders. Using the criterion suggested by previous studies of eHealth interventions, which have used participatory design, a change or recommendation to the intervention features will be prioritized for future development if it is mentioned by at least 10% (i.e. 2) of the sample. 46 This low threshold for prioritization was also used to ensure minority voices were heard and prioritized. M.O., M.C., and H.M. performed the coding, categorization, and mapping, and discussed all steps with the last author (S.M.). Discrepancies throughout the analysis process were resolved by consensus. Data saturation was based on category saturation and the richness (quality) and thickness (quantity) of the data. 47 While data saturation was achieved with 12 participants (i.e. interviews and analytic procedures provided no new material for analysis), five additional youth participated in co-design sessions given the interest of youth in the study.
Results
Participants
Of the 117 participants who were screened for eligibility, most (n = 70, 60%) were not eligible (n = 4 were too young, n = 11 were too old, n = 13 reported no anxiety problems, n = 8 reported no sleep problems, and n = 2 were not interested in participating in a co-design session) or did not complete informed consent (n = 32). Of the remaining 47 participants who completed consent, most (n = 30, 64%) dropped out of the study before completing participation due to scheduling difficulties. The remaining 17 participants fully completed the study. Participants who completed the study did not differ in their demographics or clinical symptoms from participants who could not attend the co-design session due to scheduling conflicts.
Sample characteristics
Table 1 presents the demographic characteristics of the 17 participants who completed the co-design sessions. The average age was 20.29 years (SD = 2.59). Most of the participants reported their gender (n = 13, 80%) and sex (n = 14, 82%) as female, identified themselves as White (n = 8, 47%), and were living in a city with a population less than 500,000 (n = 9, 53%). For participants who completed the SCARED (n = 2), the average score was 57.50 (SD = 12.02). For those who completed the SCAARED (n = 15), the average score was 55.73 (SD = 15.05). These average scores are above the clinical thresholds for anxiety disorders (i.e. greater than or equal to 25). The average score on the ISI was 22.12 (SD = 4.74), indicating an average level of sleep problems that are equivalent to severe clinical insomnia.
Demographic characteristics of participants.

Note: Mean (M) and standard deviation (SD).
Qualitative feedback
Table 2 presents the feedback participants provided on the SMILE app and its features. We identified the five most frequent categories of responses from participants including Likes, Dislikes, Concerns, Suggestions, and Potential Uptake. Each of these categories included many sub-categories and codes within them; however, codes were only included if mentioned by at least two participants. The number of unique mentions of a code by all participants was tallied.
Content analysis results.

Discussion
The escalating rates of mental health problems among youth, compounded by the limited accessibility of mental health services, 48 necessitate innovative solutions, with mental health apps emerging as a promising avenue. Emphasizing a comprehensive approach, the National Canadian eHealth guidelines advocate for a multi-method strategy in the development and evaluation of mental health apps, explicitly including the perspectives of youth users to ensure acceptance.13,49 Recognizing the significance of these perspectives in tailoring apps to individual needs and stipulating the acceptance and uptake of mental health apps, the objective of the current study was to collaborate with youths in the design of a novel mental health app leveraging mobile sensing to improve anxiety and sleep problems.
Overall, the results of the study affirm the acceptance of the SMILE app among youth with anxiety and sleep problems, as evidenced by the high number of positive comments (Likes, n = 248). The app's perceived ease of use, accessibility, and integration, attributed to its diverse features, resonated well with the youth. Their endorsement of a wide range of features underscores the importance of variety in enhancing the acceptance and utilization of mental health apps, aligning with existing research.50,51 Additionally, the expressed willingness of most youths to use or recommend the SMILE app to a friend or family member with mental health problems indicates positive attitudes, a crucial factor in predicting acceptance and long-term engagement with mental health apps.52,53 Amid these generally positive perspectives, the invaluable feedback provided by youth serves as a foundation for future improvements to the app, ensuring alignment with their needs and promoting sustained acceptance and use.
Addressing a common barrier to user engagement, the SMILE app endeavors to overcome issues related to personalization by tailoring intervention features to the mobile-sensed daily behaviors of youth users, 54 aligning with the broader paradigm shift towards precision medicine in mental healthcare. The appeal of the app's visualization features, which present mobile-sensed behaviors through simple graphs, highlights the potential of leveraging mobile sensing for effective self-monitoring and mental health care. 55 Importantly, features, such as mood tracking, activity recognition, and sleep pattern analysis, have contributed to a more comprehensive understanding of users’ mental health, fostering a sense of agency and self-awareness. 56 Self-monitoring and the ability to identify patterns in emotional responses and behaviors are further integral to many forms of psychotherapy. 57 Consistent with our findings, self-monitoring seems to be a widely valued and desired aspect by mental health app users.51,58–60
While youth appreciated the enhanced tracking and self-monitoring features of the SMILE app, concerns regarding the accuracy and privacy of mobile sensing data also emerged. Mobile sensing has enormous potential to enhance healthcare, but it is not without risks.61,62 This is a perspective that many youth participants seemed to share. Privacy concerns must be taken seriously and addressed by clear communication. Previous research suggested that perceived control and trust can influence the privacy protection behaviors of users, and that trust is enhanced by offering individual choices. 63 Future iterations of the SMILE app should incorporate specific permissions for mobile sensing features to enable users to choose what behaviors will be tracked. Similarly, the app should provide even clearer information on how mobile sensing contributes to the personalization of the app and emphasize the state-of-the-art techniques and safeguards in place to protect user privacy.
The design of the SMILE app emerged as a focal point for improvement. Youth provided both positive and critical reviews of the app's design but were also eager to provide design recommendations. Some common additions, from the many, suggested, included the ability to customize app visuals and text (i.e. color scheme, font style/size) and add a built-in notification system or a widget to increase personalized usage and engagement. Aligning with prior research on mental health apps, users desire a diverse array of features that are flexible or customizable enough to accommodate various needs.51,58,64,65 Theoretically, by supporting user-customizable features, messages within the app can be tailored to users’ needs and interests, which can then have greater potential for deep (rather than shallow) processing; this is in line with the Elaboration Likelihood Model of Persuasion 66 and the Persuasive Systems Design Model. 67 Enhancements of existing features were also recommended to boost utility and ease of use. Youth suggested extending the app's tracking abilities by requesting access to older data and data visualizations of behavioral changes across longer time frames in the Visualization features. Concurrently, prior research highlights enhanced tracking ability as a common user-requested app feature.58,68 More information on sleep problems in the Psychoeducation feature was another enhancement request. Positive user experiences of youth are often associated with engaging, interactive, and personalized psychoeducational content, further emphasizing the importance of tailoring information to individual needs. 69
Incorporating user feedback plays a pivotal role in ensuring functionality and continued use of mental health apps.50,51 Users are unlikely to persist with apps that fail to engage them from the start, 70 and neglecting user feedback can impede vital technical improvements, setting back evaluative research and the overall clinical effectiveness of an app.29,70 Consequently, the developers of the SMILE app emphasize a commitment to considering youth user perspectives and recommendations at each stage of development and implementation to ensure the app remains user-focused, engaging, and effective.
Limitations and future directions
It is essential to acknowledge the limitations of the study and delineate potential avenues for future research. While the study collected a diverse range of perspectives from youth with anxiety and sleep problems, the results represent participants’ opinions and may not capture the views of all youth facing these issues. Moreover, caution due to sampling bias is recommended, as a sizable number of participants did not attend the focus groups despite some confirming their interest and availability. Those without the resources and/or motivation to attend the session may hold different opinions from those who attended. Assessing app acceptance among youth who declined participation may have resulted in more negative feedback. Additionally, participants may have been biased to respond positively due to sharing feedback directly with researchers during sessions. Negative feedback is essential for informing the continued adaptation of the app to meet the diverse needs of youth.29,71 Future research should consider strategies to seek critical feedback, mitigate bias, and ensure youth perspectives are representative. Despite efforts to recruit an ethnically diverse sample, the qualitative focus and small sample size limit representation across certain demographic groups and broad generalizability. The predominant representation of females among the participants calls attention to the well-documented sex and gender differences in the acceptance of new technology72,73 and outlines the need for future research that includes more diverse gender identities. In addition, more information is required on the socioeconomic background of users in future research, as prior research has established links between anxiety and sleep problems in youth and socioeconomic status.74,75 Finally, while the study provides insights into user acceptability of the SMILE app, only an efficacy trial will test its ability to alleviate the burden on youth with anxiety and sleep problems.
Conclusions
In conclusion, this qualitative study marks an important stride in addressing the mental health needs of youth dealing with co-morbid anxiety and sleep problems. The positive reception of the SMILE app, coupled with constructive feedback, positions it to be refined into an impactful, user-friendly intervention. The study contributes to the growing body of evidence supporting mental health apps as accessible, helpful, and timely interventions, particularly when aligned with the preferences and needs of youth users. By integrating mobile sensing technology to extend tracking and personalization abilities, the SMILE app has the potential to modernize the delivery of mental health care. The recommendations and suggestions we collected are indispensable in ensuring that future iterations of the SMILE app have a meaningful impact on the mental health of youth facing anxiety and sleep problems. Ongoing research and development will be imperative to fully realize the SMILE app's potential and ensure its meaningful impact on the mental well-being of youth.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241283242 - Supplemental material for Sleep well, worry less: A co-design study for the development of the SMILE app
Supplemental material, sj-docx-1-dhj-10.1177_20552076241283242 for Sleep well, worry less: A co-design study for the development of the SMILE app by Marcus Cormier, Matt Orr, Alanna Kaser, Hannah MacDonald, Jill Chorney and Sandra Meier in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076241283242 - Supplemental material for Sleep well, worry less: A co-design study for the development of the SMILE app
Supplemental material, sj-pdf-2-dhj-10.1177_20552076241283242 for Sleep well, worry less: A co-design study for the development of the SMILE app by Marcus Cormier, Matt Orr, Alanna Kaser, Hannah MacDonald, Jill Chorney and Sandra Meier in DIGITAL HEALTH
Footnotes
Acknowledgements
The research team would like to thank all the participating youth for their contribution to the co-design sessions. We also thank the programmers of the SMILE app.
Contributorship
MO and SM researched literature and conceived the study. MO and SM were involved in protocol development, gaining ethical approval, and funding. MO and AK recruited youth participants, and MC, MO, and HM completed data analysis. MC and MO wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research ethics board of The IWK Health Centre approved this study (REB number: 1026748) on 11 May 2021.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dalhousie Medical Research Foundation under grant number 1026097.
Guarantor
SM
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.