
Abstract
Objective
eHealth interventions are being developed to meet the needs of diverse populations. Despite these advancements, little is known about how these interventions are used to improve the health of persons experiencing homelessness. The aim of this systematic review was to examine the feasibility, effectiveness, and experience of eHealth interventions for the homeless population.
Methods
Following PRISMA guidelines, a systematic search of PsycINFO, PubMed, Web of Science, and Google Scholar was conducted along with forward and backward citation searching to identify relevant articles.
Results
Eight articles met eligibility criteria. All articles were pilot or feasibility studies that used modalities, including short message service, mobile apps, computers, email, and websites, to deliver the interventions. The accessibility, flexibility, and convenience of the interventions were valued by participants. However, phone retention, limited adaptability, a high level of human involvement, and preference for in-person communication may pose future implementation challenges.
Conclusions
eHealth interventions are promising digital tools that have the potential to improve access to care and service delivery. eHealth interventions are feasible and usable for persons experiencing homelessness. These interventions may have health benefits by augmenting existing services and if implementation challenges are addressed. Further evaluation of the effectiveness of eHealth interventions is needed before widespread implementation. Those with lived experience should also be engaged in developing and evaluating these interventions.
Introduction
Persons experiencing homelessness have poorer physical and mental health than the general population. 1 Rates of chronic medical conditions, infectious diseases, mental illness, and substance use disorders are each high among the homeless population.2–5 Barriers to accessing healthcare are also common, leading to high levels of unmet needs, delayed help-seeking, and frequent use of emergency departments.6,7 When health services are accessed, care is often oriented toward addressing acute problems, as opposed to the management of chronic medical conditions, health education, or preventive care. Further, poor quality care and discrimination are common, which can decrease the likelihood that persons experiencing homelessness access treatment in the future and leave them with limited care options.8–10
Most persons experiencing homelessness have access to technology, including mobile phones, computers, and the internet. Although estimates vary between studies, 11 new research suggests that the digital divide between people who are homeless and the general population is narrowing. 12 Further, technology access is consistent across the lifespan, with similar rates being found among homeless youth, adults, and older adults.12–16 Persons experiencing homelessness use technology and the internet to stay connected with family and friends, search for housing and employment, and contact employers and case workers.11,17–19 Further, persons experiencing homelessness are open and willing to use technology for health-related purposes.20,21 Health information on nutrition and weight loss, mental health, management of chronic medical conditions, smoking cessation, and problematic substance use delivered via technology and the internet are the most frequently identified areas of need. 22 As such, given the barriers that persons experiencing homelessness can encounter when seeking and receiving healthcare, technology and the internet may be a promising approach to addressing the health needs of this population.
Electronic health (eHealth) initiatives refer to health services and information delivered through the internet and related technologies. 23 Over the past two decades, eHealth interventions have been widely developed and studied to understand their potential value in improving the health of various populations, including persons experiencing homelessness. Given that a range of factors can contribute to the success or failure of eHealth interventions, 24 it is important to understand the feasibility, effectiveness, and experience of these interventions for people who do not have a home. However, to our knowledge, no review of eHealth interventions for this population has been conducted. Accordingly, we conducted a systematic review to examine the feasibility, effectiveness, and experience of eHealth interventions for persons experiencing homelessness.
Methods
Search strategy
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 25 See Supplementary File 1. We conducted an electronic search of four databases: PsycINFO (1926–2019), PubMed (1971–2019), Web of Science (1969–2019), and Google Scholar (1915–2019). The database searches were completed in December 2019. Search terms included (homeless* OR shelter* OR unsheltered OR rough sleeper* OR street* OR runaway) AND (internet* OR online OR technology OR digital OR phone* OR smartphone). Seven keywords (homeless, shelter, street, internet, online, technology, and digital) were used to search Google Scholar generating 9,060 records. Results were sorted by relevance and reviewed until 200 consecutive records did not yield any potentially eligible articles—a strategy used frequently in other reviews.26,27 Additional studies were identified by manually searching personal records and bibliographies of relevant articles through backward and forward citation searching.
Studies were eligible for inclusion if they were original research, written in English, published in a peer-reviewed journal, and examined the use of an eHealth intervention among persons experiencing homelessness. For the purpose of this review, eHealth was defined as any health intervention that is delivered using technology and the internet. 28 Homelessness was defined as any person who is staying in an emergency shelter, outdoors, in an abandoned building, or temporarily with friends and family without paying rent. No eligibility restrictions were placed on study design, date of publication, homeless subgroup, or type of intervention as all were necessary to adequately assess the goals of the review. However, studies were excluded if the intervention did not have a web-based component (requiring internet access to deliver or use the intervention) or the sample included participants who were not homeless.
Data screening and extraction
Two reviewers (AP and SGR) independently reviewed the titles and abstracts of all articles and the full texts of eligible articles. If it was unclear whether or not a study met the eligibility criteria, its authors were contacted to retrieve additional information. A structured data extraction tool was developed using the CONSORT-EHEALTH checklist and piloted on 2 randomly selected articles. 29 A finalized version of the tool was used by two reviewers (AP and SGR) to extract data from included studies. See Supplementary File 2 for a list of extracted variables and their descriptions. Study quality was assessed independently by the two reviewers using checklists from the Joanna Briggs Institute. 30 Findings were compared in regular meetings with the research team and any discrepancies were resolved by a third member of the research team (NK). Inter-rater agreement was excellent (94%) for article eligibility and good (88%) for quality assessment.
Results
Study selection
The database searches yielded 7,822 articles with one additional article identified through backward and forward citation searching. After removing duplicates, 7,026 titles and abstracts were screened and the full-text of 84 articles were reviewed for inclusion. Of them, 76 articles were excluded for the following reasons: no intervention (n = 51), not original research (n = 7), not published in a peer-reviewed journal (n = 1), ineligible sample in that participants were not experiencing homelessness (n = 6), no health intervention (n = 6), and no web-based component (n = 5). A total of 8 articles were included in this systematic review. The study selection process is outlined in Figure 1.

Flow diagram outlining the selection process for studies included in this review.
Study characteristics
Study characteristics are presented in Table 1. Studies were conducted in the United States (n = 7) and the United Kingdom (n = 1) and published between 2012 and 2019. Samples included homeless youth aged 9–25 years (n = 4), homeless veterans (n = 2), and homeless single adults (n = 2). Sample sizes ranged from 6 to 149, with most participants recruited from homeless shelters (n = 4) or health care clinics (n = 3). Studies had primarily qualitative (n = 4) or quasi-experimental designs (n = 3); there was only one randomized-controlled trial (RCT). Qualitative studies examined the feasibility, acceptability, and usability of electronic case management, web-based personal health records, computer-assisted substance use treatment, and a mobile app to help homeless youth access resources. Quasi-experimental and RCT studies evaluated the effects of mobile apps and short message service (SMS) text messaging interventions on primary outcomes of smoking abstinence, appointment attendance, and treatment adherence. Secondary outcomes included mental health symptoms, treatment adherence and engagement, appointment attendance, emergency department visits, hospitalizations, and cost-effectiveness. Length of follow-up in the studies ranged from one to six months.
Characteristics of included studies.
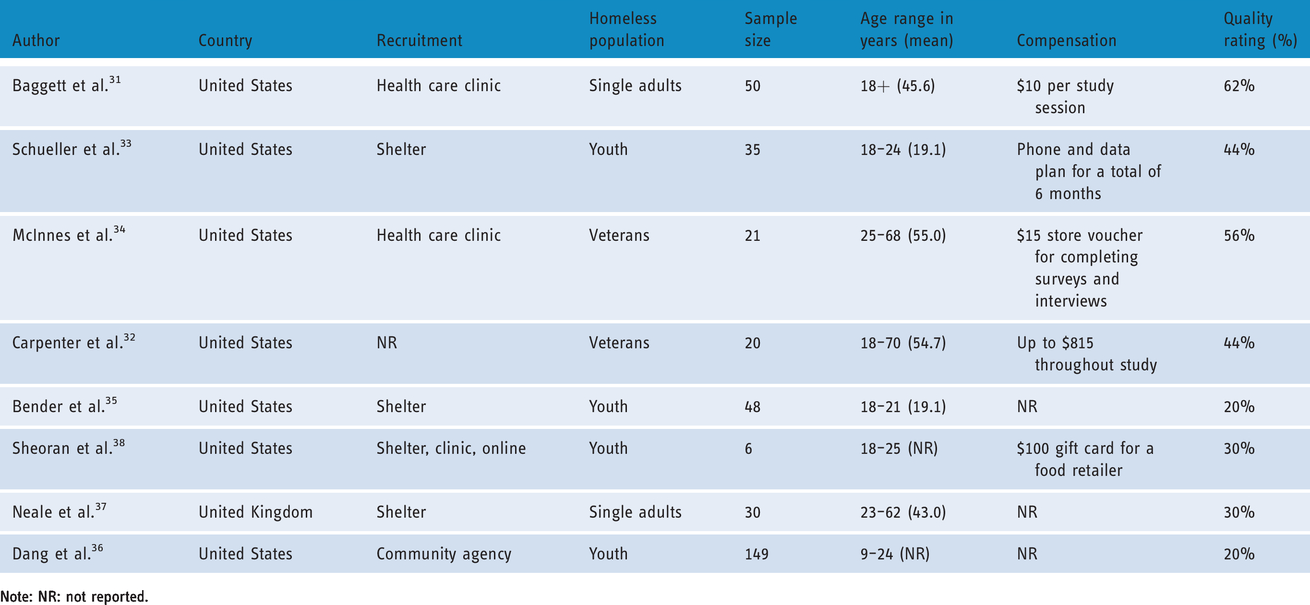
Note: NR: not reported.
Appraisal of study quality
Critical appraisal of individual studies are shown in Supplementary File 3. No study met all the methodological criteria needed to be considered high quality. The RCT had the highest quality assessment rating (62%). 31 It was unclear who was blinded to treatment assignment and if reliability was assessed. The reasons for loss to follow-up were also not reported. The quasi-experimental studies had moderate quality assessment scores (44%–56%).32–34 Common problems included absence of a control group, no information about loss to follow-up, and attrition and co-intervention bias. It was also unclear if studies had adequate power or evaluated reliability. Because the qualitative studies assessed feasibility, they did not fulfill all the requirements of qualitative research resulting in low quality assessment scores (20%–30%).35–38 Authors did not state their philosophical and methodological stance or discuss their positionality in the research process. One study did not report ethics approval and another did not include adequate quotes to highlight participants’ experiences.
Intervention characteristics and outcomes
Intervention details are outlined in Table 2. Seven studies used mobile phones and two used computers as platforms to deliver eHealth interventions. Two studies delivered SMS texting interventions, three were mobile app interventions, and three were interventions that leveraged email, social networking sites, and web portals. Six studies provided participants with devices and six had interventions with 2-way communication capabilities. Five studies had co-interventions that involved mental health coaching and assessments, assistance with using devices, counselling, nicotine replacement therapy (NRT), and medication for smoking cessation. A high level of human involvement was needed for the co-interventions, as well as on the back-end when designing and delivering eHealth interventions to study participants. Intervention length ranged from four to twelve weeks.
Intervention details of included studies.

Note: CO: carbon monoxide; N/A: not applicable; NRT: nicotine replacement therapy; SMS: short message service.
SMS texting interventions
Study results are highlighted in Table 3. SmokefreeTXT and Texting Intervention for Linkage and Engagement were two SMS texting interventions piloted on small samples.31,34 In an RCT of SmokefreeTXT, participants were sent one to five automated texts with tips on quitting smoking and 2-way texts offering supportive comments and mood check-ins. 31 Counselling on tobacco addiction and NRT were also provided alongside the texting intervention. This study did not find significant differences in smoking abstinence or attendance (at study visits and counselling sessions) between participants receiving SmokefreeTXT and those in the control arm. 31 The Texting Intervention for Linkage and Engagement sent 1-way text reminders five days and two days before their outpatient appointments. 34 The texting intervention was associated with reduced appointment cancellations and emergency department visits, with smaller effects for appointment no-shows and hospitalizations. 34
Results of included studies.

Note: NR: not reported; N/A: not applicable; RCT: randomized controlled trial; QE: quasi-experimental; QUAL: qualitative; CO: carbon monoxide; OR: odds ratio; PTSD: post-traumatic stress disorder; ED: emergency department; NRT: nicotine replacement therapy.
Smoking cessation mobile apps
Stepping Stone and Mobile CM were also mobile interventions evaluated using a single group quasi-experimental design.32,33 Mobile CM was a mobile app that allowed users who were enrolled in a smoking cessation intervention to video record themselves taking a carbon monoxide reading and they would upload it to a website that was only accessible to the research team. 32 Mobile CM was used in addition to counselling on smoking cessation, NRT, and medication. In this study, half of the sample had quit smoking by the end of treatment (four weeks) and quit rates remained relatively stable at 3- and 6-month follow-ups. 32 Stepping Stone was comprised of three mental health apps containing a daily survey and tips on coping skills, mindfulness audio recordings, and a sleep tracker. 33 Participants were also given access to remote coaching sessions by phone or text as a co-intervention. No significant changes were found in depressive, trauma, or emotion dysregulation symptoms over time. 33
Other platforms
The other four studies examined the feasibility and experience of eHealth interventions for persons experiencing homelessness using qualitative and survey methods. YTH StreetConnect was a mobile app that provided its users with weekly tips, a discussion forum to share experiences, emergency hotlines, and a list of resources in the community with their location and contact information. 38 Service providers could also refer users to services through the app. Healthshack was a portable personal health record that stored information gathered during intake assessments with a nurse. Users could share their personal health record with others, store documents securely, and access links to community resources. 36 Breaking Free Online (BFO) was a secure, online substance use treatment that incorporated 20 psychosocial strategies; however, intervention details were limited. 37 Electronic case management (ECM) provided sessions through email, text message, social networking sites, and phone calls. Trained graduate students delivered the intervention and incorporated case management components into the sessions, such as check-ins, assessments, goal development, and problem-solving. 35
Feasibility and experience of eHealth interventions
Seven studies explored the feasibility of eHealth interventions among persons experiencing homelessness. Several studies cited mobile phone retention as a challenge due to phone theft, loss, and damage, or participants not being able to pay for their monthly phone plan,31–33 with only 40% of participants still having their phone by the end of one study. 31 Attrition rates were variable (4%–37%)31–35,37 and attendance at study or counselling sessions ranged from low to moderate, with only 31–76% of participants in three studies attending half or all of their sessions.31,33,35 Two studies found SMS texting interventions consisting of appointment reminders and check-ins to be encouraging, useful, easy to use, informative, and applicable to their needs.31,34 However, participants also felt that the text messages were impersonal, repetitive, unhelpful, stigmatizing, and not applicable to the homeless population. 31 Some also expressed a preference for in-person communication, as well as more interactive and flexible SMS intervention features. 31
Two studies assessed the feasibility of using mobile apps to improve the mental health of youth experiencing homelessness and help them to access services.33,38 Youth reported that they were satisfied with the mobile apps, found them helpful and easy to use, and were able to learn useful skills and contact resources in their communities if needed.33,38 Youth spoke highly about the daily tips feature incorporated into the Stepping Stone mental health app, 33 as well as the contact information and map of local resources within the YTH StreetConnect app. 38 At the request of youth, a community board was added to the YTH StreetConnect app to help youth bond with each other and share resources. Youth also stressed the importance of providing mobile app users with information on available community services. 38
Three studies examined the feasibility of using computer- and mobile-based interventions to deliver case management, substance use treatment, and a portable personal health record.35–37 Youth reported that they found ECM convenient and accessible, and they appreciated virtual check-ins with their case manager. 35 Youth also preferred text messaging their case managers, as some felt that their case managers called at inconvenient times during the day. 35 Individuals who had substance use problems reported that they found BFO, the computer-assisted drug treatment program, accessible, interactive, flexible, helpful, and easy to use. 37 They also spoke about the digital literacy skills they gained from using the intervention. However, BFO was located on a computer in an emergency shelter, which was slow and often had technical problems. 37 In the study examining the feasibility of Healthshack, the portable health record, youth viewed it positively and found it easy to use. 36
Discussion
This systematic review examined the use of eHealth interventions among persons experiencing homelessness. Despite there being only eight studies in this review and even fewer that measured intervention effectiveness, leveraging eHealth technology to support this population is promising and has the potential to improve health service delivery and, in turn, the lives of persons experiencing homelessness. However, although eHealth interventions have been found to be effective in prior studies with other populations,39,40 few conclusions can be drawn about the effectiveness of these interventions for persons experiencing homelessness, as all studies were pilots or examined feasibility with small samples and had low or moderate study quality scores. Accordingly, before eHealth interventions are scaled-up and disseminated widely, implementation challenges must be addressed and more high quality trials of eHealth interventions for persons experiencing homelessness are needed.
All eHealth interventions were brief and many included co-interventions. Given the complex health needs of the homeless population, it is important to be realistic with expectations and intentional in targeted outcomes when designing and implementing these interventions. eHealth interventions on their own are unlikely to yield lasting improvements in mental health or substance use when people are experiencing homelessness and exposed to ongoing danger. Moreover, it is important to be mindful of the dose-response relationship and the possibility that eHealth interventions need to be longer in duration and greater in intensity to effect meaningful change. Yet, as the intensity of care available through eHealth interventions may be limited, their utility may be highest as an adjunct to other services.
Desiging eHealth interventions that match the needs and wants of persons experiencing homelessness is critical. Continuity of care outcomes, which were examined in the Texting Intervention for Linkage and Engagement study, 34 may be particularly amenable to eHealth interventions. For example, given the rates of traumatic brain injury and cognitive impairment in the homeless population,41,42 eHealth interventions that offer compensatory strategies for helping people remember appointments or access services may be particularly beneficial. Social connection and support may be another key domain worth examining in eHealth interventions that have a peer support component, such as the one integrated into the YTH StreetConnect app at the request of youth who were using it. 38
Although questions related to effectiveness require further examination, the evidence is clearer with regard to the feasibility and usability of eHealth interventions by persons experiencing homelessness. Persons experiencing homelessness generally found eHealth interventions to be convenient, informative, and accessible.31,33–38 Satisfaction was high with SMS interventions and a mental health mobile app.31,33,34 Interventions that had 2-way interactive features, daily tips delivered through SMS or mobile apps, and virtual check-ins with case managers were also components that were valued by persons experiencing homelessness.31,33,35,37 In two studies, homeless youth and veterans preferred to communicate by text message because it was cheaper, and more convenient and flexible.34,35 In contrast, another study found that people preferred receiving smoking cessation support in-person rather than by SMS. 31 This is a particularly noteworthy finding given that persons experiencing homelessness are vulnerable to social isolation and thus, may prefer to meet with service providers in person. 43 Accordingly, eHealth interventions may be better suited to complement rather than replace health and social services as service providers can help persons experiencing homelessness build connections in their community in a way that cannot be replicated by technology.
It is important that eHealth interventions are personalized for persons experiencing homelessness and that they are involved in designing and implementing them. In one study, the SMS intervention was perceived to be repetitive and not relevant to the needs of persons experiencing homelessness. 31 Because this intervention was not intended for persons experiencing homelessness and not sufficiently adapted for this population, it resulted in stigmatizing text messages that upset particpants. 31 One of the studies included in this review gathered user feedback from homeless youth and service providers to improve the prototype of the YTH StreetConnect app. 38 The feedback was used to add new features and resources to the app, change the way information and symbols were displayed, and make it visually appealing. 38 Actively engaging people with lived experience in this process is essential and their involvement on steering committees or research teams can lead to meaningful collaboration and help ensure that eHealth interventions meet the needs of persons experiencing homelessness.
Even though almost all studies provided participants with devices, some had their own phones, computers, and tablets prior to the studies, with ownership rates ranging from 54% to 76% in two studies.31,33 These rates are slightly higher than those found in a prior systematic review with persons experiencing homelessness. 11 Phone retention may pose an implementation challenge as 3 studies found that some participants were not able to maintain their device throughout the study period,31–33 with 1 study having to replace 11% of phones. 33 It may be beneficial for researchers of eHealth interventions for this population to include costs in their budget that allow them to provide access to devices, internet, and phone and data plans. Incentivising participants to keep their devices throughout the study may also improve retention, 31 but it is likely that some devices will have to be replaced.
Similarly, services should provide persons experiencing homelessness with prepaid phones and data plans and safe storage of their devices if needed. Building partnerships with telecommunication companies may help services that are already under-resourced cover these costs. In Canada, mental health organizations have partnered with telecommunication companies in the past to launch mental health initiatives.44,45 A similar approach has been implemented in the United States via government programs. 11 Expanding these initiatives to provide mobile phones and data plans to persons experiencing homelessness may help increase access to technology and address the barrier of device loss. Moreover, recently, there has been a rapid shift toward providing virtual care during the coronavirus disease global pandemic. 46 As these digital health interventions remain in place and become integrated into routine care, differential access to technology and the internet may become a critical barrier to receiving services, further isolating and excluding persons experiencing homelessness. Older adults and those who have been incarcerated for long periods who are experiencing homelessness may also not have the digital literacy skills required to use eHealth interventions and engage with services that are delivering virtual care, emphasizing the need for digital literacy training for this population. Closing this digital divide should be a priority for services and government agencies.
Another challenge to the feasibility of using eHealth interventions with persons experiencing homelessness is the high level of human involvement that is required to deliver these services and their co-interventions. Adding a digital navigator to the research or care team has been discussed in prior studies. 47 Responsibilities of digital navigators would vary depending on the needs of the setting or population being served, but may involve choosing and evaluating the quality of eHealth interventions (i.e., SMS, mobile apps, computer programs), troubleshooting technical or usability problems, identifying safety issues, and encouraging user engagement and adherence. 47 Similarly, designating a health professional to deliver eHealth interventions and teach people how to use them may be helpful in providing care to a greater number of persons experiencing homelessness.
Limitations
This systematic review has several limitations. First, given the heterogeneity of the eHealth interventions included in this review, comparisons and conclusions were limited. Nonetheless, the clearest finding is that eHealth interventions are feasible for persons experiencing homelessness, irrespective of intervention type and platform. Second, because of our inclusion criteria, eHealth technology that was not web-based and studies that were not published or written in English were excluded from this review. As such, our review is at-risk of publication and language bias. Third, feasibility studies received low quality assessment ratings, as they were evaluated using criteria meant for qualitative studies. Systematic reviews of SMS interventions for other populations have also encountered this challenge. 48 As eHealth research continues to grow, this limitation highlights the need to develop measures that can more accurately assess the quality of eHealth studies. Fourth, because this area of research is still in its infancy, all studies in this review were either pilots or examined feasibility and had low or moderate study quality scores. As such, we were not able to assess the effectiveness of these interventions, further limiting our findings and highlighting a need for future research.
Future research
There is a critical need for more evidence on the effectiveness of eHealth interventions for persons experiencing homelessness. This issue is not limited to this population, as the emergence of mobile apps designed for commercial use has led to frequent efficacy claims despite a lack of scientific backing.49–51 Accordingly, eHealth interventions that have been found to be feasible for persons experiencing homelessness should consider further examination of their effectiveness. This systematic review yielded few findings about persons experiencing homelessness and their perspectives on the data safety and privacy risks that may be associated with eHealth interventions. Since prior studies have found that persons experiencing homelessness may mistrust service providers, 52 it is worth exploring if similar concerns extend to eHealth technologies in future qualitative studies. Lastly, similar to findings in this systematic review, a recent pilot study of an SMS intervention was well-received by people living in permanent supportive housing who were formerly homeless. 53 Given the increased stability that permanent supportive housing yields in the lives of persons with histories of homelessness, eHealth interventions may be particularly suitable for this group and warrant further examination.
Conclusions
eHealth interventions are promising digital tools that have the potential to improve access to care and service delivery. Overall, the findings from this systematic review suggest that eHealth interventions are feasible and acceptable for persons experiencing homelessness, particularly when used as an adjunct to other services. However, before these interventions are scaled-up, implementation challenges must be addressed and their effectiveness evaluated in more high quality trials. Further, co-designing eHealth interventions with persons experiencing homelessness can be a way to ensure that these interventions are adapted and developed to meet the needs of this population.
Supplemental Material
sj-pdf-1-dhj-10.1177_2055207620987066 - Supplemental material for The use of eHealth interventions among persons experiencing homelessness: A systematic review
Supplemental material, sj-pdf-1-dhj-10.1177_2055207620987066 for The use of eHealth interventions among persons experiencing homelessness: A systematic review by Alexia Polillo, Sophia Gran-Ruaz, John Sylvestre and Nick Kerman in Digital Health
Supplemental Material
sj-pdf-2-dhj-10.1177_2055207620987066 - Supplemental material for The use of eHealth interventions among persons experiencing homelessness: A systematic review
Supplemental material, sj-pdf-2-dhj-10.1177_2055207620987066 for The use of eHealth interventions among persons experiencing homelessness: A systematic review by Alexia Polillo, Sophia Gran-Ruaz, John Sylvestre and Nick Kerman in Digital Health
Supplemental Material
sj-pdf-3-dhj-10.1177_2055207620987066 - Supplemental material for The use of eHealth interventions among persons experiencing homelessness: A systematic review
Supplemental material, sj-pdf-3-dhj-10.1177_2055207620987066 for The use of eHealth interventions among persons experiencing homelessness: A systematic review by Alexia Polillo, Sophia Gran-Ruaz, John Sylvestre and Nick Kerman in Digital Health
Footnotes
Acknowledgements
This study does not have any acknowledgements.
Contributorship
Alexia Polillo was responsible for conceptualizing the study, collecting literature, conducting reliability checks, analyzing and interpreting data, writing the first draft of the article, and accepting final revisions. Sophia Gran-Ruaz helped collect literature, conduct reliability checks, analyze data, and write and edit the article. John Sylvestre helped interpret data and write and edit the article. Nick Kerman helped conduct reliability checks, analyze and interpret data, and write and edit the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Institutional review board approval was not required as this article was a systematic review of the literature and not original research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Alexia Polillo.
Peer review
Harmony Rhoades, University of Southern California has reviewed this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.