
Abstract
Objective
The scaling of digital health platforms, accelerated by the COVID-19 pandemic, has globally reshaped the delivery of healthcare services, presenting both opportunities and challenges. Ensuring equitable access, especially for digitally disadvantaged groups, is a critical concern, and this study explores older adults’ perspectives on digital health platforms during and after the COVID-19 pandemic and examines their strategies for coping with the general challenges of the digitalization of health.
Methods
A total of 77 older adults (aged at least 65), including both internet users and non-users, participated in 11 focus group sessions in Slovenia between September and December 2022. Hybrid thematic analysis was used to develop an understanding of the challenges confronted by older adults in the digital health landscape.
Results
Three key themes emerged from the focus group sessions, which highlight digital inequalities that impact access to digital health platforms and their services: the challenges of digitalized health services, coping with these challenges, and the outcomes of health service digitalization. The “digital health paradox” is evident, in which opportunities are provided for some while access is limited for those unwilling or unable to use digital health platforms. Proxy users, often family or friends, help bridge this gap.
Conclusions
Ensuring the availability and viability of traditional health service access is crucial for empowering older adults to choose between digital health platforms and alternatives. Recognizing the importance of traditional approaches is vital, and healthcare providers and policymakers should prioritize inclusivity to ensure a diverse and equitable healthcare system for older adults and vulnerable populations.
Keywords
Introduction
Healthcare digitalization is fundamentally transforming the provision of healthcare services and how the entire healthcare system works, 1 encompassing advances in internet-based technologies and their integration with new therapies and treatment practices that enable better health management. 2 Examples of such digital health services include digital health platforms (DHPs), remote monitoring, smart wearables, health apps, telemedicine and teleconsultation, and data-sharing tools. 3 Digitalization positively impacts prevention, medical diagnosis, treatment decisions, and data management, and the World Health Organization (WHO), United Nations, and European Commission consider it crucial to improving healthcare and system efficiency and to achieving universal healthcare coverage.3,4
The COVID-19 pandemic fast-tracked the digital transformation of healthcare,5–8 profoundly impacting the functioning of healthcare systems worldwide. For instance, primary care services have increasingly shifted toward DHPs, 9 facilitating online interaction between patients and healthcare professionals and online access to health data. DHPs, such as patient portals, facilitate appointment scheduling, secure communication between healthcare professionals and patients, and automatic prescription renewals for chronic diseases. 10 In Slovenia, where this study was conducted, the national eHealth system has played a central role in this transformation. In particular, the national patient portal, zVEM, a enabled continuity of healthcare during the COVID-19 pandemic, with more than 60% of the population consulting doctors or receiving prescriptions remotely.12–14
However, the fast-paced digitalization of healthcare during the COVID-19 pandemic also highlighted many challenges of digital healthcare provision and access, including issues related to costs, reliability, safety, privacy, system compatibility, disruption of patient–physician interactions, sustainability, accessibility, and the usability of various DHPs.15–19 In fact, the COVID-19 pandemic highlighted the “digital health paradox,” 5 in which socially and digitally disadvantaged groups face greater barriers to accessing the benefits of the digital healthcare transformation. In particular, previous studies have suggested that digital inequalities, which are disparities between individuals in internet access, use, skills, and tangible usage outcomes, 20 can lead to health inequalities among older adults. 21 Despite—or perhaps because of—the number of internet users among older adults rising considerably after the COVID-19 outbreak, digital inequalities among them have actually widened.22,23 This may not be surprising, as existing literature indicates that many older adults lack ubiquitous and multi-modal internet access and/or the internet skills needed for self-reliant use of digital health services.24,25 Accordingly, studies have shown lower usage of DHPs among older adults,26,27 particularly those aged 75 or older. 6 Now, as the COVID-19 pandemic has subsided, digitalization has continued and even accelerated, deepening the digital inequalities in healthcare, 6 with services progressively migrating to the internet—often only on DHPs and without alternative options.
In addition to disparities in internet access and skills, studies10,26–30 have identified several other barriers to the adoption of DHPs among older adults, including negative attitudes, accessibility, usability concerns, ease of use, privacy and safety concerns, technological anxiety, and a simple lack of interest or experience with internet or digital technology. Older adults’ overall perceptions of the benefits of DHPs therefore vary, ranging from negative 26 to neutral 31 to positive. 29 A recent study indicated that older DHP non-users in Sweden have more negative attitudes than their peer users, 26 while a study in Finland found that self-reliant older internet users perceive more benefits from digital health services than their peers without access and independent use. 31
However, the role of internet use-by-proxy (UBP) in overcoming some of the challenges associated with the digitalization of healthcare remains under-researched. UBP is the use of the internet indirectly through a third party (i.e. a proxy user), and prior studies on internet use and online health information-seeking suggest that many older adults—both users and non-users—engage in UBP,22,31–33 most commonly relying on family or peers as the proxy users.32,34–36 Barral Buceta's 36 study in Spain highlights this issue, showing that older adults often designate healthcare proxies or representatives when they lack the skills to navigate complex digital procedures or do not have internet access. There is also a lack of understanding of the perceptions of older adults who are affected by or at risk of digital exclusion, and with an aging population and accelerating digitalization, it is crucial to capture their attitudes toward the digitalization of services.31,37 While a few recent studies have considered older adults’ perceptions of digitalization, they have focused on topics such as overall engagement in a digital society,38,39 the impact of digitalization on social participation, 38 perceptions of digital technologies, 39 and experiences during the COVID-19 pandemic, with an emphasis on the advantages and disadvantages of accessing services online. 40 At the same time, most research on healthcare digitalization has focused on its impact on the health-sector41,42 or healthcare workers,43,44 often emphasizing metrics and health outcomes rather than users’ engagement with DHPs. 45
Slovenia provides a good context for the current study in several ways. The country boasts a high proportion of older people (consistent with the EU-27 average of 21.1%) 46 with 65.7% of internet users in the 65–74 age group and 35.7% in the 75 + age group. Slovenia also lags behind the EU average in people possessing basic (54%) and advanced (26%) digital skills. 47 Thus, many older internet users are engaged in less advanced online activities, 48 with 50.1% turning to proxy users for help with online activities—almost as high a proportion as among non-users (64.4%). 49 On the other hand, Slovenia has a universal healthcare system and has strongly prioritized the digital transformation of healthcare since 2016. 14 For instance, 80% of Slovenian citizens had access to their electronic health records in 2022, 50 while zVEM, the national DHP, played a key role in healthcare provision during the COVID-19 pandemic, which the government declared between 11 March 2020, and 31 May 2022. Nevertheless, there is still a lack of empirical studies of patients’ and older adults’ perceptions of healthcare digitalization in Slovenia.
This study therefore seeks to delve into the first-hand perspectives and experiences of older adults in Slovenia, including both internet users and non-users. The focus is on exploring their views of and attitudes toward the digitalization of health services, particularly DHPs, capturing their experiences with it, and on identifying their strategies (such as UBP) for coping with the challenges of the fast-paced digitalization of healthcare both during and after the COVID-19 pandemic.
Material and methods
Research design
An exploratory–descriptive qualitative study51–53 was conducted to investigate our research topic, which has limited coverage in the literature. 54 This design allowed us to describe and explore a little-researched phenomenon in a real-life context, gain new insights and knowledge, and identify potential problems. 55 As emphasized by Denscombe, 56 such studies are essential for understanding what is happening, finding new perspectives, and investigating unexplored problems. Using a qualitative approach enables a nuanced exploration of the complexities in users’ experiences with telemedicine platforms, and offers rich insights into user perceptions, challenges, and expectations, which are essential for an evolving field in which quantitative methods may fall short. 57 We used semi-structured focus group interviews to gather data. Each group consisted of six to eight participants, consistent with group-size recommendations, 58 to ensure diverse perspectives and broad participation. The groups were homogeneous in terms of age range (65–74 and 75+ years) and internet use (users or non-users) for more open and natural discussions.
Recruitment and participants
The data were collected using purposive sampling. Participants from the Central Slovenia region were recruited between September and December 2022 with the help of a marketing research company. They were invited through various communication channels, based on the company's contact list and a minimum age criterion (65 + years). The company was also instructed to recruit both internet users and non-users with an even split between two age groups (65–74 and 75 + years). Invitations to complete the recruitment questionnaire were sent to 1562 participants, of whom 398 completed the questionnaire either fully or partially. Of these, 96 were classified as eligible based on the predefined criteria linking internet use and age composition. Ultimately, 77 participants were allocated to 11 focus groups (Table 1, Supplemental Material 1).
Structure of the focus groups.

Note. FG: focus group.
The average age of the 77 participants was 74.25 years (SD = 5.34); 30 were male and 47 female; 48 had a secondary professional/technical degree or vocational training/lower degree, while 29 had higher or university education; and 37 lived in a two-person household, 15 in a household with three or more people, and 24 alone. There were 48 internet users and 29 non-users among the participants; in addition, 31 acted as proxy users and 55 were users-by-proxy. See Supplemental Material 1 for more socio-demographic data.
Ethical approval
The study adhered to Slovenian and international research ethics guidelines and the General Data Protection Regulation (GDPR). 59 The research received ethical approval from the Commission for Ethics in Research of the Faculty of Social Sciences, University of Ljubljana (801-2022-018/JG; 801-2022-027/JG) (Supplemental Material 2). The participants were fully informed, both verbally and in writing, about the study's purpose, data confidentiality, and their voluntary participation rights. Before the focus groups began, the participants provided written informed consent to participate in the study.
Data collection
The Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist was used to ensure comprehensive reporting of the research process (Supplemental Material 3). Before starting the focus group discussions, we administered a questionnaire to collect sociodemographic data and other relevant information related to the participants’ internet use. The questionnaire (Supplemental Materials 4 and 5) included a modified version of the Internet Use Scale60,61 and questions regarding internet engagement and sociodemographics, which are validated and regularly used in Slovenian and international research (e.g. International Social Survey Programme). The focus groups themselves were audio-recorded and moderated by SHT and JL, with the support from AP. At the start of each focus group session, the moderators provided a concise overview of the study process and encouraged the participants to engage actively in the discussions by emphasizing that there were no definitive right or wrong answers. Close attention was paid to nonverbal cues, to ensure that everyone had the opportunity to voice their opinions. The discussions were generally organic, with a natural flow of dialogue. There were no disputes within the group.
The focus group guide (Supplemental Material 6) was developed using findings from an extensive literature review,22,61 and its aim was to encourage discussion about the participants’ views of the internet, internet access, (in)direct internet uses, internet skills acquisition, and the impact of the COVID-19 pandemic on their self-reliant and indirect online activities, potentially including the use of DHPs. The focus group sessions were conducted in Slovenian and lasted between 55 and 112 min, with an average duration of 76 min. An audio recorder was used to record the sessions, and field notes were taken throughout. Participants received small monetary compensation.
Data analysis
Quantitative data about the sample were analyzed using IBM SPSS 28. b Qualitative data from the recordings were transcribed verbatim by two students who participated as research assistants in the focus group sessions and analyzed using ATLAS.ti 9. c Pseudonyms were assigned to each participant, and all identifiable information was removed.
We conducted an exploratory–descriptive qualitative study characterized by describing rather than explaining phenomena. 57 (pp49–53) The data were subjected to thematic analysis, which offers a high degree of flexibility and is not bound by particular epistemological or theoretical perspectives. 54 A common method used in qualitative data analysis is looking for important themes that emerge when describing phenomena. 62
Many forms of thematic analysis exist. We chose a hybrid thematic analysis 63 in this study to incorporate a deductive theoretical process—inspired by the literature review, research questions, and individual questions posed to study participants—and an inductive, data-driven approach to identify themes. This hybrid approach allowed us to build on existing knowledge about the phenomenon while also gathering new defining information from the data. 63 The hybrid thematic analysis process followed a sequential three-stage approach: 63 8 Phase 1 involved preparing a table of codes and information, creating a priori codes, and familiarizing ourselves with the data; Phase 2 involved starting a priori and a posteriori coding and summarizing information about the participants in a table; and Phase 3 involved selecting excerpts of each code and categorizing the a priori and a posteriori codes into themes.
In Phase 1, the codes generated from the sociodemographic questionnaire were entered into ATLAS.ti 9. The transcripts were closely examined. We identified large segments of text on broader topics related to the experience of using DHPs during and after the COVID-19 pandemic (i.e. structural coding), 64 which formed the basis for further analysis. An initial coding scheme with a priori codes was developed deductively (top-down approach) based on the literature. 63 In Phase 2, the participants’ sociodemographic information and answers to questions on topics such as internet knowledge and use were summarized. The coding scheme was updated with a posteriori code developed inductively (bottom-up approach). We discussed the a posteriori codes and other issues related to the coding process until we jointly developed a final coding scheme. Saturation was observed during coding, meaning that we evaluated similar examples and empirically concluded that the data was saturated and could not form new categories or themes. 65 (p61) The coding process categorized the data into 111 codes (29 a priori and 82 a posteriori codes) based on thematic affinities, which were then grouped into 13 categories related to the digitalization of healthcare during and after the COVID-19 pandemic. In Phase 3, the most meaningful excerpts from the text that corresponded to the codes were identified. The categories were integrated into three overarching themes, which are presented in the following section. Participants were not provided with final transcripts for comment.
Results
The analysis identified three themes (Table 2): (a) challenges of digitalized health services; (b) coping with the mainstreaming of DHPs; (c) outcomes of the digitalization of health services.
Themes and categories derived from the focus group data.
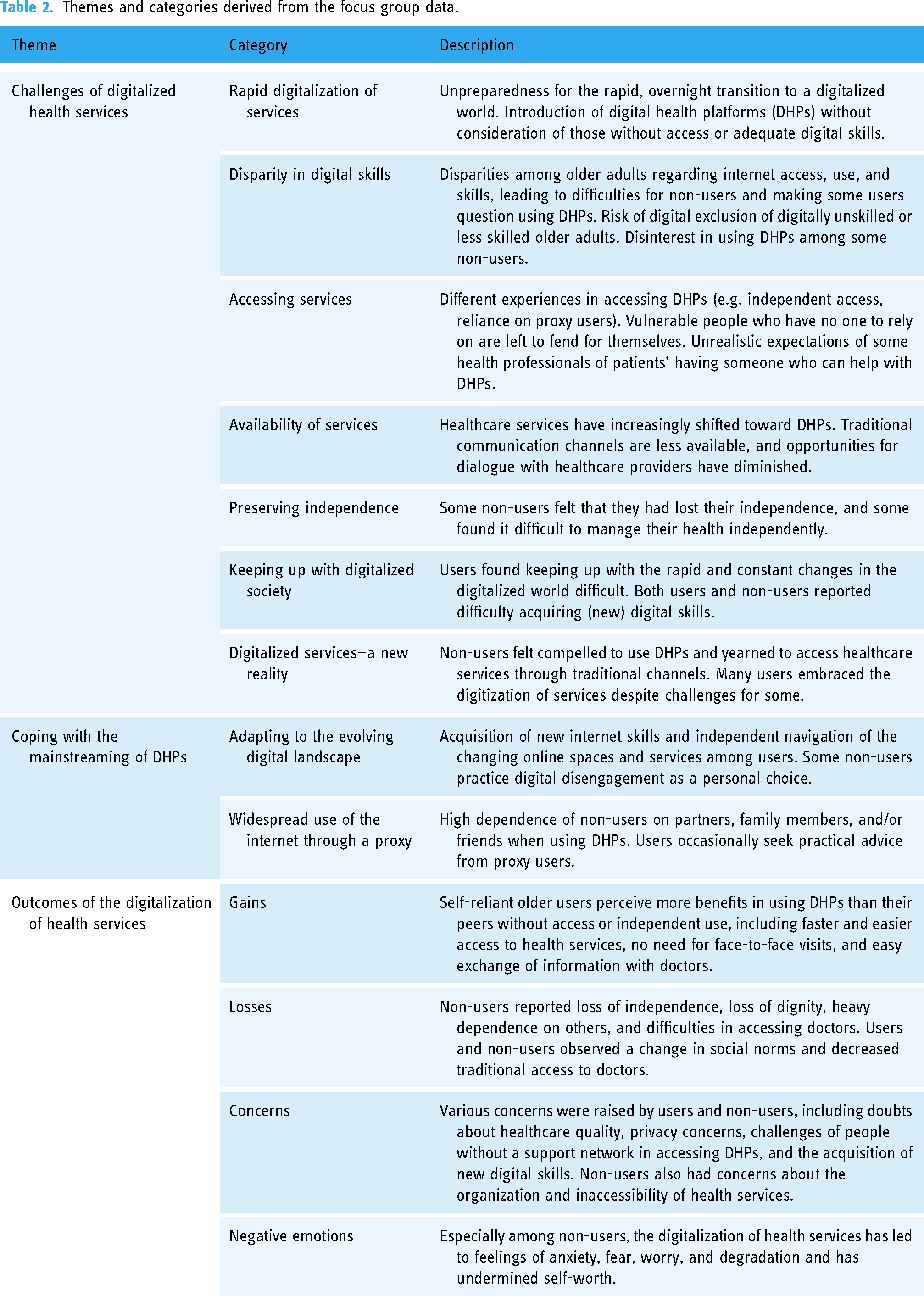
Challenges of digitalized health services
The first theme includes seven subcategories related to the challenges that participants faced during and after the COVID-19 pandemic related to the digitalization of health services, which, according to the participants, were a necessity during the COVID-19 pandemic but then changed how they used and accessed healthcare services. For many, this change became a major challenge because of the sudden and unexpected overnight transition to a digital world without alternatives, for which they felt unprepared. Both internet users and non-users mentioned that, during the COVID-19 pandemic, online services were implemented not only suddenly but also without considering that some might struggle to use them. As Iva (FG1), a 71-year-old user, said, “COVID forced us to do everything by email. It's true, they threw us in at the deep end, and now we must swim. Now it's like we’re figuring things out as we go. We’re learning all the time.”
Some internet users mentioned that the innovations associated with the digitalization of healthcare can be challenging, even for highly skilled internet users. As Miran (FG6), a 74-year-old user, stated, “They developed an app to book appointments with doctors, and now they don’t want to accept emails. When you send emails, they tell you that you must make the appointment through this app for patients...”
Some participants initially tried to use DHPs but not always successfully, as in the case of 75-year-old non-user Viktoria (FG9): “I can’t even figure out email addresses, passwords, and usernames, so the basics. I mainly need them for doctors’ appointments and searching for health-related information. So, I tried using the new portal for patients, but I didn’t know how to do it. It didn’t work.” Similarly, 73-year-old Borut (FG1), a proficient internet user, commented on how difficult it was to acquire new skills related to this transition. He was also broadly concerned about the coping ability of his generation: “Put yourself in the position of a 75-year-old who has been out of work for who knows how long and is trying to cope. Society has rushed to make us all intelligent and [digitally] literate. It just doesn’t work. You can’t learn that in five or ten years, it must be passed down through generations. But the problem is that our age group needs these services practically every day.”
Iva (FG11), a 71-year-old internet user, voiced her concerns about how non-users were managing with digitalization during the COVID-19 pandemic: “I actually thought about it during the COVID time. Well, we’re getting old, and we’re struggling, right? But what about the people who don’t even have a smartphone, who don’t know anything? How do they reach the doctor? They must rely on their children. I’ve often thought about the fact that these people are really in a difficult situation.” In response, Jože (FG11), a 65-year-old internet user, replied, “There are also individuals who do not turn to others for help, either due to family conflicts or simply because they do not want to or have no one to rely on.” Several participants expressed unease about the overlooked challenges in accessing DHPs that are faced by people without a support network. They wondered how these people would navigate this change—even more so because access to healthcare through traditional channels (e.g. telephone calls, personal visits to the doctor) has proven difficult for many internet users and non-users even after the COVID-19 pandemic.
Frequent reliance on immediate family members, usually children or partners who take on the role of proxy users, was reported by all non-users and some users. While some took such support for granted, others expressed a desire to maintain their independence while grappling with the challenges of doing so. They found it particularly difficult because of the expectation among some healthcare professionals that older people who lack the necessary digital skills will have a support system in place. This way of thinking was summarized by Zdravko (FG8), a 75-year-old internet user: “Normally, you get the answer, ‘Don’t you have a son or daughter who can do that for you?’” Alja (FG9), an 81-year-old non-user, reported a similar experience with her doctor, who said, “‘Make an appointment’, and I tell her, ‘I don’t know how to send it’, and she says, ‘You have children’. I say, ‘My children are abroad’, and the answer is, ‘Well, they can do it from abroad too’.”
The feeling among many participants of being forced to adopt DHPs as they emerged during the COVID-19 pandemic has persisted. At the same time, there was a yearning, especially among non-users, to be able to access health services as they were offered before the COVID-19 pandemic, which was triggered by several factors, including a lack of digital skills, disinterest, and deliberate resistance to digitalization. However, as many participants stated, the accessibility of health services over the phone remains problematic, even after the COVID-19 pandemic, as 72-year-old non-user Tina (FG3) described: “They left the phone for the older people, but they cannot be reached [group agreement]. Just today, I was on the phone for a whole hour trying to reach them.”
Coping with the mainstreaming of DHPs
The second theme focuses on two overarching aspects of the coping strategies the participants used to resolve the challenges of the digitalization of health services during and after the COVID-19 pandemic. Many internet users have adapted to the evolving digital landscape, navigating changing online spaces and services independently by acquiring new internet skills (e.g. patient portals, digital certificates). Marko, a 73-year-old internet user, noted that the management of health services has changed with the arrival of DHPs, and they have therefore learned many new things: “We learned how to use the portal for patients and how to get the digital vaccination certificate on your smartphone. We had no idea about any of this before, it was all new. From then on, you could get your referrals via the portal, and you got your prescriptions on your mobile phone and no longer on paper. You have everything on the portal. But you had to learn all that first.” While most internet users relied primarily on themselves to use DHPs and similar new services, some occasionally turned to their proxy users for practical advice or to do something online on their behalf. For instance, 72-year-old internet user Borut (FG1) said, “They [proxy users] helped me with advice on what I need to do to get these digital certificates and so on.”
Some older adults sought health services through traditional channels, such as phone calls, seeking to avoid DHPs. However, health centers often did not pick up the calls, so the participants turned even more to their family and friends to access DHPs, leading to a significant increase in UBP during and after the COVID-19 pandemic. Tellingly, non-users became highly dependent on their family members or close friends for accessing DHPs. For married participants, their partner was frequently an important source of help with internet activities. For instance, 68-year-old Sara (FG3), a non-user, who needed to see an orthopedist, said, “My partner had to find out where, when, and how. He gave me the phone numbers, and then I rang. When there are things like that … that's why you have a partner, so you don’t burden your children because they’re not there.” If a partner was not available or did not have the necessary skills, adult children and sometimes grandchildren stepped in as proxy users.
However, a few non-users deliberately chose to manage their health services independently and were not deterred by difficulties in accessing the doctor by phone; 75-year-old non-user Viktorija (FG9), for example, turned down DHPs at the cost of spending more time getting an appointment with her doctor. She said, “I go to the doctor in person because the doctor never answers me [on the phone]. I also call the information desk, but nobody answers me there either. So, I go to the health center, write a letter, and present it at the information desk, and then I get an answer.”
Outcomes of the digitalization of health services
The third theme, with four subcategories, deals with participants’ perceptions of the positive and negative outcomes of the digital transformation of health services on their lives. The participants observed that digitalized healthcare continued after the COVID-19 pandemic, accompanied by shifting social norms. The prevailing expectation now is that individuals either possess the skills needed to handle DHPs independently or have a proxy user who can assist them. While most internet users and some non-users have benefited from DHPs since the COVID-19 pandemic, most non-users have continued to rely heavily on proxy users to access them. As some non-users expressed, this heavy reliance on others can undermine their sense of independence and self-worth, leading many to wish they could manage their affairs independently without proxy users’ support, as they had done before the COVID-19 pandemic. They would therefore try to reach the healthcare center using alternative means of communication, even if this meant constantly calling, sometimes for several days if necessary, visiting in person, or writing letters to the doctor.
Importantly, internet users perceived the outcomes of DHPs more positively than internet non-users, as they could benefit more directly from them due to their better internet access and greater internet skills. However, the differences in the levels of internet skills among internet users were clearly reflected in their perceptions of the outcomes. Multi-device and highly skilled users said that DHPs were convenient because they enabled access to their doctors faster, easier, and without in-person visits; they also mentioned easy information exchange with their doctors. Ficko (FG8), a 75-year-old internet user who has been battling a chronic illness for two decades, commented on his familiarity with DHPs: “Whenever I get a report from a specialist, I just email it to my doctor. It's a very elegant solution.” However, only a few non-users said that health digitalization has increased their motivation to learn internet skills.
The negative aspects of the digitalization of health services that raised concerns among participants mainly related to the organization of services (e.g. communication exclusively via the Internet, difficulties in obtaining referrals, medication prescriptions, and check-up appointments). Several non-users expressed fear of DHPs becoming the “default mode” of healthcare provision in Slovenia and of reduced availability through once-ordinary channels (e.g. phone calls and in-person visits). They believed that, because of DHPs, their health would no longer be managed in the same way as before the COVID-19 pandemic, and they felt unprepared for such sudden changes. As Borut (FG1), an internet user, put it, “If you’re not digitally literate, you lose out.” Another internet user, 82-year-old Klara (FG8), shared an experience that resulted in anxiety: “I still don’t know how to deal with this new portal; I’m still struggling with it, and it scares me. They should definitely train people on how to deal with it.”
Many participants, most of whom were non-users, found it difficult to see a doctor. They mentioned that the phones in health centers were often not answered and that the health centers were empty when they managed to see a doctor in person. They sometimes felt desperate because it was difficult to see a doctor in person and blamed the internet. For instance, 71-year-old Renata (FG3), a non-user who used to manage all her healthcare over the phone, expressed her frustration: “You ring and you ring; I can spend a whole morning trying and still not get through. I’m used to using the phone because I’m not familiar with the internet and don’t use it.”
Several participants felt anxious about how they would access healthcare in the future, and some were made to feel deeply degraded, as 73-year-old non-user Anita (FG3) emphatically described: “They completely degraded me because I can’t use a smartphone. I can’t even get hold of the nurse, and I had an agreement with the doctor that I could call her on such-and-such a number. That's impossible. But they forced this on me. I feel like they forced this on me. And they act like they’re a bit above me.”
Ultimately, the changes in the participants’ access to primary health services raised doubts among them about the quality of the healthcare itself. For instance, some questioned the accuracy of “remote diagnostics”; Iris (FG1), a 65-year-old user, said, “In healthcare, I don’t understand how you can now just take a photo of everything and send it in, and a diagnosis is made. I can’t understand how this has suddenly become the norm. If you want to make an appointment, you’re asked to take a photo and send it in. No, that's not how it should work.”
Discussion
This study aimed to examine an emerging topic,35,36 that is older adults’ perspectives on healthcare digitalization during and after the COVID-19 pandemic. Both internet users and non-users recognized the advantages and disadvantages of digitalization in healthcare, consistent with previous research.10,26–30,39 Internet users emphasized the benefits, such as faster, easier, and remote access to DHPs, but also had issues with quality, accessibility, and ease of use; such dissatisfaction with the accessibility of healthcare services during and after the COVID-19 pandemic was also found in another study in Slovenia. 66
Our findings show that many older adults felt unprepared for the overnight digitalization of health services during the COVID-19 pandemic. They felt that DHPs were imposed on them, creating additional stress and burdens for those who lacked digital resources, including internet access, skills, and UBP support networks. Criticism also extended to the limited phone accessibility of primary healthcare centers. Both internet users and non-users had concerns about the long-term reduced accessibility of health services that was caused by the COVID-19 pandemic and that could lead to institutional ageism and systematic discrimination toward older adults in healthcare.67–69
Another important finding of this study is the role of UBP in the use of DHPs. While internet users only occasionally turned to proxy users—because they managed to use DHPs independently—non-users relied on them heavily for accessing DHPs during and after the COVID-19 pandemic. In fact, the participants in the focus groups reported an implicit expectation from medical professionals that older adults without internet access or the necessary internet skills to use DHPs should, by default, rely on assistance from family and friends. Moreover, older adults who sought help from others to access DHPs, especially their children and grandchildren, often felt a loss of independence and that their autonomy and self-worth had been compromised. This observation is consistent with a study among older adults (75 + years) in Norway, suggesting that the digitalization of health has made older adults feel more vulnerable and even humiliated when they need to ask for help, leading to a loss of personal dignity. 30 The same study also raised concerns about privacy, diminishing opportunities for dialog with healthcare providers, and the desire of non-users to take back control of their healthcare by being able to access healthcare services in person.
We identified several other barriers to the acceptance of DHPs, including lack of digital skills and knowledge, lack of interest in learning or acquiring (internet) skills, lack of support from proxy users in mastering DHPs, fear or dislike of the internet, and negative attitudes. Similar barriers, with the exception of UBP, have been found in prior research.10,26–30 In addition, some older adults might refrain from using DHPs due to the belief that the effort required to learn internet skills outweighs the perceived benefits.70,71 However, our results also highlight the distinction between digital disengagement, as a personal choice among older adults, and digital exclusion, which affected many non-users in this study and hampered their access to the positive effects of DHPs. 72
Health systems aim to improve patient outcomes, yet increasing reliance on DHPs requires internet access and digital skills—resources that not everyone possesses. As observed in our study, those lacking these resources often must rely on others to act as proxy internet users to access healthcare services. This issue is not exclusive to Slovenia but is also evident in other countries, including Spain. 36 Barral Buceta 36 emphasizes that relying on others for digital access should not be the default solution, nor should it be expected of patients. Although alternatives exist, including healthcare representatives who manage patients’ service requests, they are inadequate. While some have suggested employing “digital navigators” 73 to assist patients with DHPs, this approach is only a temporary fix. Instead of waiting for them to acquire digital skills, older adults should be proactively equipped with the necessary tools and support to ensure equitable access to healthcare in a digitalized world.
Furthermore, many previous studies have highlighted positive outcomes of digitalization for older adults30,40,74,75 and demonstrated that internet use76,77 and participation in digital literacy training programs 78 led to increased social inclusion and physical activity during the COVID-19 pandemic. Likewise, epidemiological studies have found health benefits from internet use through the promotion of physical activity, well-being, active aging, and the preservation of cognitive abilities among older adults.76,78–83 While our results corroborate the existing literature on the benefits of DHPs, they also underscore the negative aspects of the adoption and scaling of DHPs associated with the digital health paradox. 5 Notably, the COVID-19 pandemic galvanized many highly skilled users in our study to acquire or master the internet skills needed to use DHPs, but for many more narrowly skilled users and non-users, it caused anxiety and feelings of dependency and helplessness.40,84 These negative emotional responses to DHPs were further exacerbated by some healthcare providers’ considering DHPs to be the default for everyone. Accordingly, we found that the positive outcomes of DHPs were difficult to obtain for both non-users without highly skilled proxy users and self-reliant older users who lacked the necessary internet skills. Research has indicated that age-related digital inequalities in public health are often overlooked 79 and that greater digital inequalities can even contribute to adverse health outcomes for digitally excluded groups.79,85 In our increasingly digital society, the inability of older adults to engage in digital health services is a growing concern. 86 According to Helsper's corresponding fields model, 60 digital exclusion—rooted in longstanding social, economic, and regional inequalities—intersects with social exclusion, with access, skills, and attitudes being key mediators. Digital exclusion can be understood on three levels: access, skills, and outcomes. Many older adults are excluded at the first level due to limited internet access and device availability, particularly in rural and low-income areas. 87 However, our focus groups highlighted the second level of exclusion, in which a lack of digital skills is most evident. These skills, influenced by an individual's resources, affect not only patients’ ability to engage digitally but also their social inclusion. The third level of exclusion relates to outcomes, where a lack of digital skills directly affects access to healthcare services, and exacerbates health inequalities, which was also observed in our focus groups.
The WHO 3 stresses the need for digital equity, to ensure that everyone can benefit from digital technologies in healthcare. Social inequities are reflected in digital health inequities. Disadvantaged groups are disproportionately affected by exclusion from digital health services. 88 Indeed, Brenda and colleagues 85 suggested that high-speed and multi-device internet access should be recognized as a social determinant of health and that disparities in internet access should be addressed as a public health issue due to their impact on the health of individuals and their communities. In this context, many participants in our focus groups underscored the importance of “age-friendly design” in the uptake of DHPs, which should also consider the heterogeneity of older adults, and address the factors that may limit or facilitate their ability to fully benefit from digital engagement. 40 Such an approach could prevent DHPs from becoming a new source of digital exclusion and health inequalities, instead making them tools for more equal access to health services through digital inclusion. It is also important that traditional alternatives to DHPs be available so that older adults can decide for themselves what methods and services they want to use. By recognizing the importance of such alternatives, healthcare providers and policy makers can build a more inclusive and equitable healthcare system that meets the diverse needs of older adults and other vulnerable populations.
Limitations and future research
A strength of this study is that we included both internet non-users and users from different older age groups. However, because the focus group sessions were held outside the participants’ homes, frail older adults who may have both lower digital skills and a greater need for health services were not included. Future research is therefore needed to better capture the heterogeneity of the aging population in exploring perceptions and adoption of DHPs. Our study was also conducted in a single country, and national differences in health systems, responses to the COVID-19 pandemic, and access to various health services, including DHPs, could affect the applicability of our findings to other cultural contexts. Nevertheless, despite its limited scope and country-level specifics, we believe our results provide many original insights and a nuanced understanding of older users’ and non-users’ challenges and strategies for coping with the digitalization of health services during and after the COVID-19 pandemic. This rich material, which complements previous research, is a solid foundation for further research on age-related digital health inequalities.
Conclusions
The COVID-19 pandemic exposed digital inequalities and low levels of internet skills among older adults both in Slovenia and worldwide. Our results underscore the key role of digital inequalities in the uptake of DHPs among older adults. Indeed, we found that the sudden shift to the digitalization of health services increased digital inequalities not only between internet users and non-users but among users with different levels of internet skills. Consequently, there has been an increase in UBP, but such support is also unevenly accessible to older adults.
The participants in our study recognized both the benefits and drawbacks from the digitalization of health services, with the latter stemming from a lack of tools and/or skills to independently access health services due to rapid digitalization, which left them unprepared and helpless. Our results also revealed the importance of providing “traditional” alternatives to DHPs and the perils of a “digital by default” logic for healthcare management. The findings provide a basis for reflection on how we should address these aspects of digital inequalities among older adults both in policy initiatives and daily practice. Validation and further investigation of questions arising from our study are therefore needed to better understand the socio-technical implications of DHPs for aging societies.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241282247 - Supplemental material for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19
Supplemental material, sj-docx-1-dhj-10.1177_20552076241282247 for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19 by Simona Hvalič-Touzery, Jerneja Laznik and Andraž Petrovčič in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076241282247 - Supplemental material for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19
Supplemental material, sj-pdf-2-dhj-10.1177_20552076241282247 for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19 by Simona Hvalič-Touzery, Jerneja Laznik and Andraž Petrovčič in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241282247 - Supplemental material for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19
Supplemental material, sj-docx-3-dhj-10.1177_20552076241282247 for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19 by Simona Hvalič-Touzery, Jerneja Laznik and Andraž Petrovčič in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076241282247 - Supplemental material for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19
Supplemental material, sj-docx-4-dhj-10.1177_20552076241282247 for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19 by Simona Hvalič-Touzery, Jerneja Laznik and Andraž Petrovčič in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076241282247 - Supplemental material for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19
Supplemental material, sj-docx-5-dhj-10.1177_20552076241282247 for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19 by Simona Hvalič-Touzery, Jerneja Laznik and Andraž Petrovčič in DIGITAL HEALTH
Supplemental Material
sj-docx-6-dhj-10.1177_20552076241282247 - Supplemental material for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19
Supplemental material, sj-docx-6-dhj-10.1177_20552076241282247 for “I’m still struggling with it, and it scares me”: A qualitative analysis of older adults’ experiences with digital health portals during and after COVID-19 by Simona Hvalič-Touzery, Jerneja Laznik and Andraž Petrovčič in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank the participants for their time and willingness to take part in the study, as well as the students Nuša Cekuta and Živa Šubelj who helped with the transcriptions of the focus groups.
Contributorship
All authors (SHT, JL, and AP) worked together on this study. They researched, planned the study, and developed the methods. SHT led the process of gaining ethical approval and ran the focus groups with JL. Then, SHT and JL analyzed the data. SHT wrote the first draft of the manuscript, which all authors reviewed, edited, and approved. SHT and AP were responsible for funding acquisition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research received ethical approval from the Commission for Ethics in Research of the Faculty of Social Sciences, University of Ljubljana (801-2022-018/JG; 801-2022-027/JG).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Slovenian Research and Innovation Agency [grant numbers J5-4578, P5-0399, and J5-2558] and jointly by the Slovenian Research and Innovation Agency and the Ministry of Digital Transformation [grant number V5-2275].
Guarantor
SHT.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.