
Abstract
Background
Patient portal technology is increasingly utilized in the health care system for diabetes management as a means of communication and information-sharing tools, and it has the potential to improve access, quality, and outcomes for patients with diabetes. However, its adaptation is very low, and patients’ intention toward the patient portal is unknown. This study aims to fill this gap by determining the intention to use the patient portal and its predictors among patients with diabetes in Ethiopia.
Method
An institution-based cross-sectional study was conducted on patients with diabetes from April 3 to May 8 in eight referral hospitals in the Amhara region, Ethiopia 2023. Samples were proportionally allocated for each hospital, and participants were selected by using a systematic random sampling method. The data were collected by using an interviewer-administered questionnaire using the Kobo collection mobile app. Descriptive statistics were performed using SPSS version 26. The degree of association between exogenous and endogenous variables was assessed and validated using structural equation modeling using AMOS version 21.
Result
A total of 1037 (96.2% response rate) patients with diabetes participated in the study. Of them, 407 (39.25%), 95% CI: [36.4–42.2] were found to have an intention to use the patient portal. Digital literacy (β = 0.312, 95% CI: [0.154–0.465], p < .01), performance expectancy (β = 0.303, 95% CI: [0.185–0.420], p < .01), effort expectancy (β = 0.25, 95% CI: [0.131–0.392], p < 0.01) facilitating condition (β = 0.22, 95% CI: [0.081–0.36], p < .01) and habit (β = 0.111, 95% CI: [−0.009 to 0.227], p < .05) were significantly associated with the intention to use patient portals. Effort expectancy and facilitating conditions were positively moderated by gender.
Conclusion
This study found that patient with diabetes’ intention to use patient portals was low. To increase patients with diabetes’ intention to use the patient portal, interventions in digital literacy, performance expectations, effort expectations, facilitating conditions, and habits are required.
Background
Information technologies (ITs) are being implemented in the healthcare systems of developing countries. 1 A patient portal is one of them that helps patients manage their personal health information, request prescription refills, schedule appointments, communicate with their health care provider, receive laboratory results, and improve medication adherence.2–5 It provides patients with greater access to health care services and enables them to engage in their health care process, by increasing patient health literacy.2,6–8 It has a significant effect on improving self-management, especially for chronic diseases like diabetes, 9 and increases patient satisfaction. 10 Routine controls and follow-ups can be performed remotely to reduce unnecessary hospital visits. Care providers can check their patients’ health status digitally with wearable remote patient monitoring devices integrated with the patient portal system.11,12 In addition, it is important to minimize medical errors and medical fraud to improve patient outcomes in the healthcare process. 13
Diabetes mellitus is a chronic disease in which the body is unable to control the amount of glucose, and its essential symptom is high blood glucose levels.14,15 It is becoming a major global public health issue, with more than a half billion adults living with it and 1.5 million deaths attributed to it each year.14,16,17 According to a World Health Organization report, more than 24 million adults are living with diabetes in Africa, and it is anticipated to reach 55 million by the year 2045.18,19 Similarly, according to the International Diabetes Federation report, Ethiopia is one of the leading countries among the top five most prevalent nations in Africa. 18
Effective diabetes management requires continuous communication between the patient and the care provider. As a result, ICT is increasingly being used in diabetes patient care. In addition, promoting patient-centered care and empowering patient engagement are important to improve the quality of care, 20 and health information technologies play a significant role in achieving these goals and helping patients manage their health more effectively.2,21
Despite the increasing availability of the patient portal, provider enthusiasm, and the tool's potential benefits, its adoption is very low 22 and little is known about it by patients. According to the literature, patient portals are used by less than 7% of the total number of healthcare consumers worldwide.23,24 Moreover, adopting the portal technology is still facing difficulties in developing countries. 25 Patient portals, one initiative of the Ethiopian Federal Ministry of Health's digital health plan to provide patients access to their medical records, offer great promise to improve patient health and satisfaction with their care, as well as professional and organizational effectiveness in the health care system. 6
The possible barriers at the patient and provider levels that are associated with low adoption of patient portals have been identified in several studies. Lower socioeconomic status, older age, rural residence, male gender, and public or no insurance are consistently linked to the lower adoption of patient portals.26–28 There are also numerous barriers identified by studies, including low digital literacy, a lack of internet access, privacy concerns, and the existence of multiple provider-specific portals.29–32 The studies performed by UTAUT2 show that performance expectancy, effort expectancy, facilitating condition, social influence, price value, habit, hedonic motivation, and self-perception are indicated as factors for low patients’ behavioral intention to use the patient.33,34
Among the several factors contributing to the successful implementation of technologies, user perception and acceptance are important for sustainable technology adoption. According to the Unified Theory of Acceptance and Use of Technology, the adoption of innovative technology is dependent on the user's behavioral intention. 35 Effective technology use is also the result of an intention, and this intention is influenced by different factors.35,36 Therefore, to adapt and implement the patient portal for our country's healthcare system, it is crucial to understand how patients’ intention to use it and identify the predictors that influence their intention to use patient portals. Therefore, the aim of this study was to determine the intention to use a patient portal and its predictors among diabetes mellitus patients in Ethiopia.
Theoretical model background
To determine the association between the independent and dependent variables, the “Unified Theory of Acceptance and Use of Technology” has been introduced as one of the most widely accepted models. 36 The Unified Theory of Acceptance and Use of Technology Extended (UTAUT2) theory has three main structural components, such as exogenous, endogenous, and moderators, similar to the original UTAUT model, with substantial modifications in constructs and moderators. As a result, the UTAUT2 model added three significant constructs, including hedonic motivation, price value, and habit, as independent variables in addition to the four variables shared with UTAUT (performance expectancy, effort expectancy, social influence, and facilitating conditions), with moderators age, sex, and experience. 35
In this study, we adapt the Venkatesh UTAUT2 model into eight independent constructs, one dependent construct, and two moderators. Actual use behavior, which was considered a dependent variable and moderator experience in the original UTAUT2, was not assessed in this study since the investigated technology was a predicted technology that has not been implemented currently in Ethiopia, and there is no current actual use of the patient portal in the referral hospitals under study. Digital literacy was used as an independent construct in addition to the original UTAUT2 model constructs in our study, as indicated in Figure 1.

Theoretical framework for intention to use patient portal among DM patients, adopted from UTAUT2 modeling.
According to the literature, the potential user's intention toward the technology is the most important determinant of its acceptance and sustainability.35,37 The user's desire to use technology in the future is explained by their intention to use it. In this study, the behavioral intention to use the patient portal was used as an outcome variable since it has been found to be a substantial determinant of actual patient portal usage.38–40 The patient portals’ adoption has varied from country to country due to different factors, and the factors affecting consumer behavioral intention to use and the actual use behavior may also vary.7,13 The literature shows that predictors that affect the patients’ intention to use the patient portal are perceived usefulness, perceived ease of use, facilitating condition, social influence, hedonic motivation, price value, and habit.34,35,41 The moderators such as age, gender, and experience affect the association between the behavioral intention to use the patient portal and its predictors. These moderators can alter the intensity and direction of the association. The effects of performance expectancy on behavioral intention were moderated by age, gender, and experience, with a greater effect among younger males.35,36 In comparison, the impact of effort expectancy on behavioral intention was moderated by age and gender, with younger women experiencing a higher impact.35,36,42 The influence of social influence on behavioral intention was moderated by age and gender, with older women experiencing a higher impact.35,36 Although the influence of facilitating conditions on behavioral intention was moderated by gender and age, older women were more strongly affected. 35 The impact of hedonic motivation on behavioral intention was moderated by age and gender, with younger males experiencing a higher impact. 35
Performance expectancy (PE) is defined as the degree to which using a technology will provide benefits to consumers in carrying out certain activities..36,41,43,44 According to our literature review, health-care consumers are more likely to adopt e-Health technologies that provide clear benefits, such as obtaining an electronic medical prescription through patient portals.21,45–47 The following is the proposed hypothesis to test the effect of PE on the behavioral intention to use the patient portal.
H1: Performance expectancy has a positive influence on patients’ intentions to use the patient portal. H2: The effect of performance expectancy on patients’ intentions to use the patient portal is moderated by gender. H3: The effect of performance expectancy on patients’ intentions to use the patient portal is moderated by age. H4: Effort expectancy has a positive influence on patients’ intentions to use the patient portal. H5: The effect of effort expectancy on patients’ intentions to use the patient portal is moderated by gender. H6: The effect of effort expectancy on patients’ intentions to use the patient portal is moderated by age. H7: SI has a positive influence on patients’ intentions to use the patient portal. H8: The effect of social influence on patients’ intentions to use the patient portal is moderated by gender. H9: The effect of social influence on patients’ intentions to use the patient portal is moderated by age.
Effort Expectancy (EE): Effort expectancy is the level of comfort a consumer can expect when using technology.36,44 The easier it is for consumers to understand and use the e-Health technology, the greater the likelihood that consumers will adapt it.21,41,46–48 The following is the proposed hypothesis to test the effect of EE on behavioral intention to use the patient portal.
Social Influence (SI): refers to how much a consumer believes others who are significant to them, such as friends and family, believe they should use a particular technology.
35
In the context of e-Health, this can also be a crucial concept because people who have the same diseases tend to be influenced by others who also have the conditions.49–51 In the other study, it was not a significant predictor of behavioral intention to use the technology.
33
The following is the proposed hypothesis to test the effect of SI on the behavioral intention to use patient portals.
Facilitating Condition (FC): defined as the individual perception of the support available for using a technology activity.
35
The lack of resources for consumers to access these platforms is one of the obstacles to their use of health services over the Internet, suggesting that users with better access to e-Health technologies will favor the adoption of EHR portals.
46
In another study, facilitating conditions had no significant effect on the behavioral intention to use portals.
33
The following are the proposed hypotheses to test the effect of FC on behavioral intention to use patient portals.
H10: Facilitating conditions have a positive influence on patients’ intentions to use the patient portal. H11: The effect of facilitating conditions on patients’ intentions to use the patient portal is moderated by gender. H12: The effect of facilitating conditions on patients’ intentions to use the patient portal is moderated by age. H13: Hedonic motivation has a positive influence on patients’ intentions to use the patient portal. H14: The effect of hedonic motivation on patients’ intentions to use the patient portal is moderated by gender. H15: The effect of hedonic motivation on patients’ intentions to use the patient portal is moderated by age. H16: PV has a positive influence on patients’ intentions to use the patient portal. H17: The effect of price value on patients’ intentions to use the patient portal is moderated by gender. H18: The effect of price value on patients’ intentions to use the patient portal is moderated by age. H19: Habit has a positive influence on patients’ intentions to use the patient portal. H20: The effect of habit on patients’ intentions to use the patient portal is moderated by gender. H21: The effect of habit on patients’ intentions to use the patient portal is moderated by age. H22: Digital literacy has a positive influence on patients’ intentions to use the patient portal. H23: The effect of digital literacy on patients’ intentions to use the patient portal is moderated by gender. H24: The effect of digital literacy on patients’ intentions to use the patient portal is moderated by age.
Hedonic Motivation (HM): defined as intrinsic motivation (enjoyment) and has been taken into account as a significant predictor in many studies on consumer behavior.
35
When a patient has a chronic disease, obtaining and handling information about their health status using e-Health technologies may or may not be a pleasant process. Hedonic motivation, however, was discovered to have a significant influence on behavioral intention in a recent study with UTAUT2 in e-Health.
52
In contrast, another study shows that there is no meaningful correlation between hedonic motivation and behavioral intention. Patients do not seem to enjoy using portals, which is likely because the presence of a disease drives much of the usage of portals.33,53,54 The following is the proposed hypothesis to test the effect of HM on the behavioral intention to use patient portals.
Price value (PV): in a consumer-use environment, it is also a relevant factor, as unlike workplace technologies, consumers must bear the costs related to the purchase of devices and services.
35
If patients can obtain their medical prescription, appointment, and other services via patient portals, they can save transportation costs by avoiding unnecessary travel to a health institution. The better health care service consumers have about the price value of an e-Health technology can help save money, the more likely they intend to use it,
55
and older people tend to give more importance to price in e-Health.
56
In another study, PV had no significant effect on behavioral intention to use the technology.
33
The following is the proposed hypothesis to test the effect of PV on behavioral intention to use patient portal.
Habit (HA): the degree to which people carry out behaviors unconsciously after learning.
35
Since habit is a concept that should not be exclusive to IT technology, we can anticipate that habit will positively influence e-Health adoption, as it has in other IT adoption fields. According to a review of the literature, women and younger people have a habit of using e-Health technologies more frequently.57,58 The following are the proposed hypotheses to test the effect of HAs on the behavioral intention to use patient portals.
Digital literacy (DL) is the awareness, attitude, and skill of individuals to use digital technologies and facilities to identify, access, manage, integrate, evaluate, and synthesize digital information, create new knowledge, communicate with others, and use in the context of certain health or other life activities.59,60 Many studies have explored the relationship between digital literacy and intention to use. A study reports that digital literacy positively impacts the intention to use digital technology.61,62 Another study stated that higher digital literacy would have a positive impact on users’ effectiveness and a direct influence on their intention to use digital technology.
63
Methods
Study design
An institution-based cross-sectional study was conducted to determine the intention to use a patient portal and its predictors among patients with diabetes in Ethiopia.
Study period and study area
This study was conducted in public referral hospitals in the Amhara region of northwest Ethiopia from April 3 to May 8, 2023. The regional state is estimated over 32 million people. 64 The region still faces difficulties due to lack of professionals, equipment, and medical supplies, and insufficient healthcare resources. 65 In the region, there are eight referral hospitals: the Debremarkos referral hospital, the Tibebe Gion Specialized Hospital, Felege Hiwot Referral Hospital, the Debre Tabor Referral Hospital, University of Gondar specialized teaching hospital, the Woldia Referral Hospital, the Dessie Referral Hospital, and the Debrebrehan Referral Hospital. These are the hospitals where this study was conducted.
Population
All patients with diabetes who had follow-ups in referral hospitals in the Amhara region, northwest Ethiopia, were used as the source population. All patients with diabetes who had follow-ups in the Amhara region referral hospitals during our study period were used as a study population. All adult ≥18-year-old patients with diabetes who had follow-ups in the referral hospitals during the study period were included in our study.
Sample size determination and the sampling procedure
The sample size was determined using the number of free parameters that had been estimated in the model specification, including all regression coefficients between observed exogenous variables and latent variables, regression coefficients between latent variables, all factor loading on indicators other than those with paths fixed to one, all variance of exogenous variables (error covariance), and all covariance between exogenous variables (error covariance), has factors taken into consideration when determining the sample size for structural equation models. Therefore, the model can be specified according to the following (Figure 2).

AMOS software sample size determination.
In the above model specification, the number of distinct elements in the structural equation system (∑) or available inputs needs to be greater than the number of free parameters to be estimated to proceed with the given model. Therefore,
Total variances of the independent variables are parameters = 40
The covariances between independent variables are parameters = 28
The load factors between the latent and its indicator without fixed load factor = 22
The regression coefficients between observed or latent variables are parameters = 8
Therefore, the free parameters to be estimated were a total of 98 parameters; the degree of freedom (DF) was calculated as the number of available inputs minus the number of free parameters to be estimated, which was equal to 496–98 = 398. This implies that the above model is a structurally over-identified model since DF > 0. It is recommended to use 5–10 participants per variable of free to be estimated.
66
Therefore, considering 98 free parameters as a rule of thumb, 10 observations per indicator variable and a 10% nonresponse rate were considered for the study. The final sample size was calculated as follows: Sample size = (Free parameter × ratio of respondent to free parameter) plus nonresponse rate. N = (98*10) = 980 Nonresponse rate = 0.1*980 = 98 Final sample size = 980 + 98 = 1078
Sampling procedure
Study participants were selected from eight referral hospitals in the Amhara region of northwest Ethiopia. Proportional allocation was performed for each referral hospital, and finally, the participants were selected using a systematic random sampling method. The number of patients who came for follow-up was determined based on the hospital's monthly disease report. According to recent-month disease reports of the hospitals, there were 4590 patients with diabetes in those hospitals. The first patient was randomly selected using the lottery method, followed by the selection of every study participant at every kth interval until the needed sample size was reached.
Variables
Dependent Variable
Intention to use patient portal
Independent variables
Socio-demographic characteristics
Performance Expectancy (PE)
Effort Expectancy (EE)
Social Influence (SI)
Facilitating Condition (FC)
Hedonic Motivation (HM)
Price Value (PV)
Habit (HA)
Digital Literacy (DL)
Moderators
Age
Gender
Operational definition
Patient Portal: A secure online website or application that works integrated with EMR or EHR that enables patients’ convenient 24-h access to personal health information from anywhere with an internet connection. Using a secure username and password, patients can view their medical records, such as recent doctor visits, discharge summaries, prescriptions, immunizations, allergies, lab results, scheduling appointments, and medication adherence guidelines. 67
Intention to use the patient portal: The degree to which a patient has made intentional plans to engage in or resist engaging in a specific future behavior while using the patient portal system.37,68
Intended to use the patient portal: the patient who rates the intention to use a technology measurement scale scored median and above were intended to use the patient portal; otherwise, they are not intended to use it, with a five-point Likert scale of three questions. Medians were used since the nature of the data distribution lacks normality.
Data collection tool and procedure
The data collection instrument that we used for this study was adapted from a study done by V. Venkatesh and other studies that were previously conducted using UTAUT2.12,35,69 During adaption, the digital literacy construct was added to the original data collection instrument and also underwent forward and backward translation. The first part focuses on participants’ socio-demographic characteristics. The second part contains 31 questions that enable the measurement of the participant's intention towards the patient portal and each of the constructs was measured using a 5-point Likert scale question, in which 1 denotes strongly disagree, 2 denotes disagree, 3 denotes neutral, 4 denotes agree and 5 denotes strongly agree.
The data was collected using the Kobo Collect mobile app, and an interviewer-administered structured Amharic language questionnaire was used. The data collection process, respondent's right, and the objective of the research were informed to the respondent in the data collection, those who were willing to participate and gave consent were interviewed by the data collector. The case scenario was presented to the participant during data collection.
Data quality assurance
Data collectors and supervisors received one day of training on the study's objectives, data collection methods, data collection tools, respondent approach, data confidentiality, and respondent rights prior to the start of data collection and during data collection. The respondents were selected by systematic random sampling to minimize bias. The supervisors regularly monitored the data collection process, accuracy, and completeness.
After the data collection, the data were cleaned up and cross-checked before being analyzed. Although a questionnaire is a standard tool, a pretest with 10% of the actual sample size was conducted on diabetes patients at the Injibara General Hospital before actual data collection; the pretest was performed with characteristics that are comparable to those of the real study participants. The results of the reliability of latent variables were assessed with the threshold value of composite reliability and Cronbach’s α (>0.7) cut point. Based on the results of the pretest, with minor adjustments, the actual data were collected.
Data management and analysis
Data preprocessing was performed by the Statistical Package for Social Science (SPSS) version 26 software before data analysis. The descriptive statistics of demographic variables and the magnitude of intention to use the patient portal were estimated using SPSS version 26. The indicator variable's reliability and validity were assessed by measurement model confirmatory factor analysis (CFA). Convergent validity (CV > 0.70), discriminant validity (DV > 0.6) and construct reliability (CR > 0.7) were assessed. The model was assessed with the chi-square ratio (<3), goodness-of-fit index (GFI > 0.9), adjusted goodness-of-fit index (AGFI > 0.8), root mean square error of approximation (RMSEA < 0.08) and normed fit index (NFI > 0.9). Structural modeling analyses were carried out to test the hypothesis and identify the most important predictor variables of the intention to use patient portals. Critical ratios and standardized path coefficients were used to measure the association of dependent and independent variables, and 95% confidence intervals and p values (p < .05) were used to evaluate statistical significance.
Ethics approval and consent to participants
In this study, all the necessary methods were carried out in accordance with relevant guidelines and regulations. The data collectors (interviewers) were needed to read the information sheet to the respondents/legal guardians, and informed consent was obtained from the respondents/legal guardians and ethical approval was obtained from the University of Gondar Institutional Ethical Review Board (ref no: IPH/2501/2023). Participants were also notified that participation is completely voluntary and that they can stop or quit their participation at any point without any justification if they are uncomfortable with it. The collected data are kept private to protect the confidentiality of any information provided by study participants and their privacy.
Results
Socio-demographic characteristics of the participant
A total of 1037 (96.2% response rate) adult patients with diabetes participated in the study. The median age of the respondents was 39 years (IQR = 28–48). Of the study’s participants, 35.5% were over the age of 44. Of the total responses, 58.7% were male. Of the total participants, 55.8% were urban residents, and 61.7% reported being married. Forty-eight percent of the participants were orthodox Christians. Thirty-eight percent of the participants had higher education. A total of 37.3% of participants had internet and social media exposure. The results showed that 50.8% of the participants had a monthly income of less than 5000 ETB. A total of 57.5% of participants were type 2 diabetes patients, and 44% of participants had lived with diabetes for less than 3 years. A total of 15.3% of participants had comorbidities, as indicated in the (Table 1).
Socio-demographic characteristics of patients with diabetes in Amhara region referral hospital, 2023.

Note: other in occupation category contains unemployed, daily laborer and students.
Behavioral intention to use patient portals
In this study, 407 (39.25%) (95% CI: [36.4–42.2]) of the participants intended to use the patient portal and were scored at the median and above the value of intention to use the patient portal. The outcome variable intention to use the patient portal was measured using three questions with a five-point Likert scale; the median score was 10 (IQR = 6–12), as summarized in Figure 3.

Behavioral intentions to use the patient portal among patients with diabetes in Amhara region referral hospitals, Ethiopia, 2023.
Measurement model
Before proceeding to structural modeling, we developed the measurement model as shown in Figure 4 and assessed composite reliability, convergent validity, discriminant validity, and model fitness by performing confirmatory factor analysis (CFA). The multivariate kurtosis value was >5 (62.584), and the multivariate critical ratio was not between −1.69 and 1.69, CR = 22.278. The data failed to exhibit multivariate normality assumption, so by resampling the data that were previously assumed to have been distributed normally, the nonparametric test of bootstrapping methods helps to evaluate the significance of the path coefficients, standard errors, and confidence intervals of non-normally distributed data. Consequently, 5000 bootstrap samples were used in AMOS, with a 95% confidence interval.
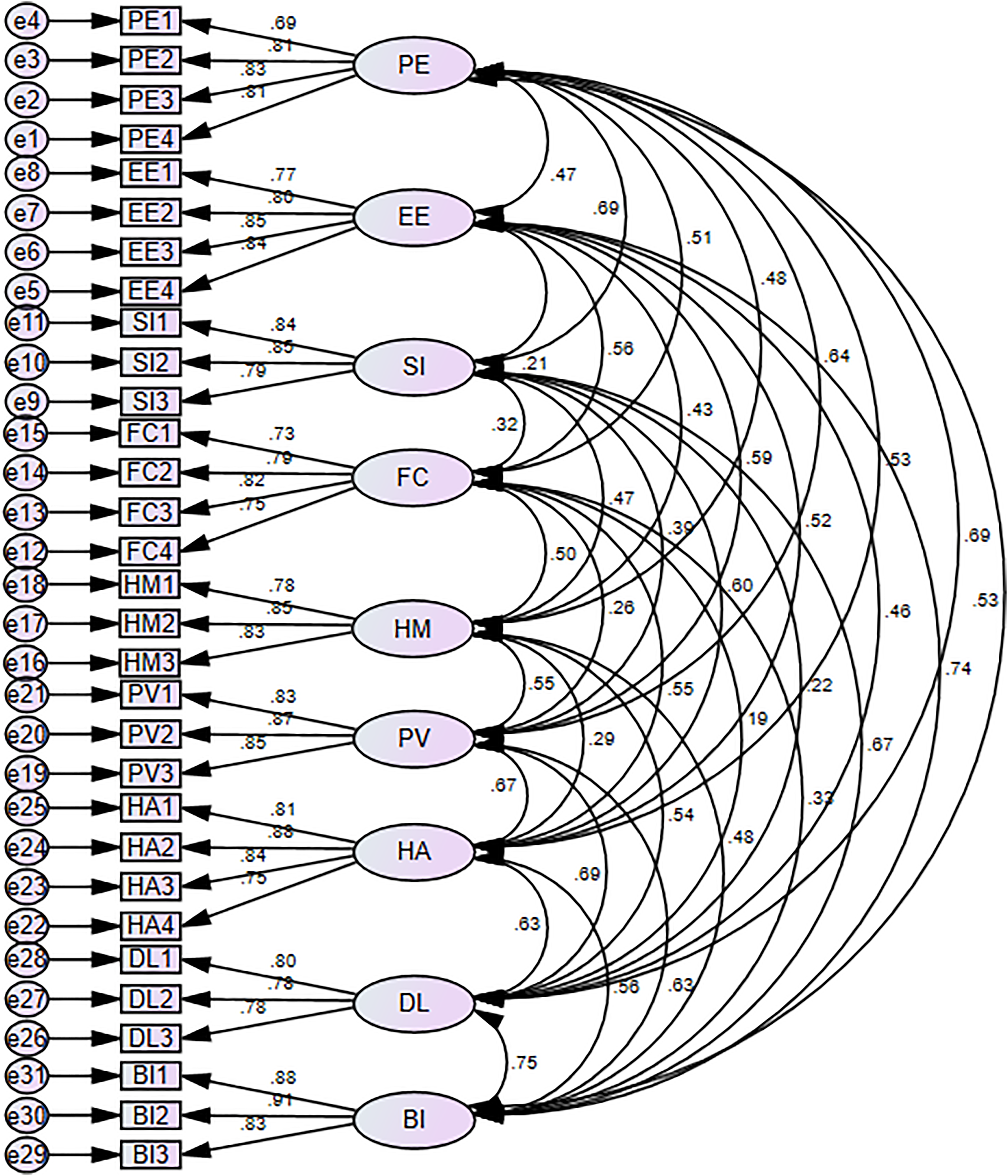
Confirmatory factor analysis of intention to use patient portal among patients with diabetes in Amhara region referral hospitals Ethiopia 2023.
In the measurement model, we assessed the measurement properties in terms of reliability, convergent validity, and discriminant validity. For reliability, we report composite reliability and Cronbach's alpha coefficients in which all values consistently exceeded the recommended cutoff point of (0.7), 70 indicating that the scales are internally consistent. Convergent validity was assessed to determine whether the variable contribution to the variance of the factor is valid to describe the factor accordingly or not. It was assessed by the item loadings for all factors, which were above the recommended cut point of (0.6), 71 which implied that our measurement tool has acceptable convergent validity. Table 2 summarizes the value of the constructs’ Cronbach's alpha, construct reliability and average variance extracted.
Reliability of predictors and intention to use patient portal among patients with diabetes in the Amhara region referral hospitals Ethiopia 2023.

The discriminant validity was evaluated using the Fornell-Larcker criterion. According to this criterion, the latent variable shares more variance with its indicators than with the other latent variables. 72 Discriminant validity was assessed by the square root of the average variance extracted (AVE), which is larger than the inter-construct correlations (off-diagonal elements) in the model. As indicated in Table 3, the requirement was met, which implies that our measurement tool has satisfactory discriminant validity. All the above model index assessments were established.
Discriminant validity between constructs using the fornell larcker criterion.

In this study, we used the tolerance (>0.1) and variance inflation factor (VIF < 10) to assess the degree of collinearity between independent variables. 73 According to our test results, there is no collinearity between them, summarized as (Table 4).
Multicollinearity test between predictors of intention to use the patient portal at referral hospitals in the Amhara region, Ethiopia, 2023.

Structural equation model fit indexes
The measurement model (CFA) results revealed that the model fit measures had the following values: chi-square (χ2/df = 2.418), goodness-of-fit index (GFI = 0.942), adjusted goodness-of-fit index (AGFI = 0.927), comparative fit index (CFI = 0.975), root mean square error of approximation (RMSEA = 0.037), and standardized root mean square residual (SRMR = 0.028).35,74 Considering this, the results of the goodness-of-fit model satisfied the criteria. As a result, it is possible to draw conclusions on the study hypotheses using the structural model (Table 5).
Model fit indexes intention to use patient portal among diabetic patients Amhara region referral hospitals, Ethiopia 2023.

Structural equation modeling
Structural equation model path significance levels were estimated using a bootstrap with 5000 iterations of resampling to ensure the highest level of consistency in the results after the measurement model was assessed. The structural model was evaluated using R2 = 0.73. Overall, the model explains 73% of the variance in behavioral intention to use the patient portal using exogenous variables in the model: digital literacy, effort expectancy, performance expectancy, facilitating condition, habit social influence, hedonic motivation, and price value. SEM analysis results presented in Figure 5 and Table 6 show that predictors of performance expectancy, digital literacy, effort expectancy, facilitating conditions and habit had a significant positive association with patients’ behavioral intention to use the patient portal technology. The digital literacy level of individuals has a significant positive effect on the intention to use the patient portal (H22) (β = 0.312, 95% CI: [0.154–0.465], p < .01). Similarly, performance expectancy (H1) has a significant positive influence on patients’ intention to use the patient portal (β = 0.303, 95% CI: [0.185–0.420], p < .01). Effort expectancy (H4) was significantly associated with patients’ intention to use the portal (β = 0.25, 95% CI: [0.131–0.392], p < .01). Facilitating conditions (H10) have a significant influence on the intention to use a patient portal (β = 0.22, 95% CI: [0.081–0.36], p < .01), and habit also had a significant effect on patients’ intention to use patient portals (H19) (β = 0.111, 95% CI: [−0.009–0.227], p < .05). In contrast, the results revealed that social influence (H7) has no significant effect on the intention to use the patient portal (β = 0.01, 95% CI: [−0.134 to 0.163], p > .05), as well as hedonic motivation (H13) (β = −0.023, 95% CI: [−0.129 to 0.078], p > .05) and price value (H16) (β = 0.045, 95% CI: [−0.074 to 0.158], p > .05) have no significant influence on intention to use the patient portal.

Structural equation modeling for intention to use patient portal among patients with diabetes in Amhara region referral hospitals Ethiopia 2023.
Structural equation modeling of the association between predictors and intention to use the patient portal among patients with diabetes at referral hospitals in the Amhara region, Ethiopia, 2023.

Note: S.E.: standard error; C.R.: Critical ratio; *p <.05.
Moderation effect
A multi-group SEM analysis was performed to ascertain the effect of moderators on the relationship between predictor variables and behavioral intention to use the patient portal.
To test moderators, model comparisons were performed between unconstrained and structural weight models. The structural weight (constrained) shows that the moderator variable has no effect on the relationship between the predictors and dependent variable; on the other hand, the unconstrained model revealed whether the moderator has a significant difference in influence on the relationship between predictors and the dependent variable. The moderator variable was identified as a moderator when a significant difference between the two models had to be substantial (p <.05 or chi-square difference > 5) to be considered significant. 75
The results in presented in Tables 7 and 8 show that there was a statistically significant difference between being male or female on the effects of the effort expectancy and facilitating conditions on the intention to use the patient portal. Despite this, there was no statistically significant difference in gender for the other predictors. Additionally, there was no statistically significant difference in the intention to use the patient portal across different age groups for any of the predictors in this study.
Moderating effects of gender on the intention to use patient portals among patients with diabetes at referral hospitals in the Amhara region, Ethiopia 2023.

Note. *p < .05, **p < .01
Moderating effects of age on the intention to use patient portals among patients with diabetes at referral hospitals in the Amhara region, Ethiopia 2023.

Note. *p < .01.
Discussion
This study aims to determine the intention to use a patient portal and to identify predictors among patients with diabetes using the UTAUT2 model. This study's findings show that of the total participants in the study, 39.25% were found to have an intention to use the patient portal, which is less than half of the participants. This study result is lower than studies performed on diabetic patients’ intentions to use m-Health applications 76 and willingness to receive m-Health services among patients with diabetes in Ethiopia. 77 This discrepancy might be due to sample size and awareness differences between m-Health apps and patient portal technology, as well as 75% and 77.8% of participants, respectively, in those studies being mobile owners. In addition, most of our study participants intended to learn about patient portals for future use; this implied that patients’ knowledge about patient portals and poor culture of information utilization could have an impact on their intention to use the portal. 78
Similarly, this study's result is lower than that of a study performed on the intention to use personal health records in Egypt. 79 And also, this finding was lower than a study done in the United States; this discrepancy might be due to the study participants and sample size. They used high usage from a survey of respondents (n = 3162) in the United States. Another reason might be that the participants were aware of the portal technologies that were beneficial to health, and the study time period was during the pandemic COVID-19; this may also have had an effect on the study result. 80 Another study was done on patients with diabetes in Lebanon 81 and other study done in Canada, 82 which are higher than our study. The possible explanation for this discrepancy might be that the majority of participants in our study are not familiar with patient portal technology. Moreover, there is a low level of emerging patient portal technology development in Ethiopia. The likely reason might be that low internet penetration, low digital device penetration 83 and low levels of digital and health literacy might have contributed to this result.84,85
According to our study findings, the endogenous variables performance expectancy, effort expectancy, facilitating conditions, habit and digital literacy were significantly associated with the intention to use the patient portal. On the other hand, social influence, hedonic motivation, and price value had no direct considerable influence on the behavioral patient's intention to use the patient portal.
This study's findings revealed that the digital literacy level of individuals has a direct positive and highly significant effect on behavioral intention to use the patient portal, which has the greatest influence over all other predictors. This implied that those individual patients who have better digital literacy skills, which include technical skills such as login, searching, and evaluation skills to obtain information from the patient portal, were more likely to intend to use the patient portal technology. 84 The probable reason might be that more than one-third of participants in this study had internet and social media exposure, and more than two-thirds of the participants had secondary or higher education status. This study’s findings aligned with other study results.41,62,86
Based on our study-findings, performance expectancy has a direct positive effect on the intention to use the patient portal. This indicates that those individual patients who perceive the usefulness of the patient portal to access their medical records as helping them accomplish health-related tasks quickly and effectively are more likely to intend to use the patient portal.44,87,88 Consumers need to believe the system is useful; they will attempt to use it, regardless of how easy or difficult it is to use. Therefore, it is important to ensure that the system will improve the desired health outcomes when developing it. 89 This study's results are consistent with the studies performed.12,21,41,42,76,90,91
Similarly, effort expectancy directly influences behavioral intention to use a patient portal. This finding shows that the individual patients who perceived the ease of use and ease of learning to operate the patient portal are more likely to intend to use the patient portal. In this case, if the patient portal feature is functionally simple, clear, and understandable, patients are more likely to intend to use it. 92 This may also be the result of patients’ perceptions that using a portal may simplify their work and enable the handling of information and data in a readily available and systematic way.56,57 According to a study, awareness and training of innovative technology improves users’ perceived ease of use and, consequently, increases intention to use the technology. 92 The lack of user-friendly features is also a reason for most patient portals and other eHealth technology failures. 25 This result is consistent with other evidence.21,44,76,87,90,91
The other finding of this study is that facilitating conditions also have a positive direct effect on patients’ intentions to use the patient portal. This implied that those individual patients who had the necessary infrastructure, resources, support, and expertise to utilize the patient portal were more likely to intend to use the patient portal. 47 In addition, patients may prefer to use the patient portal system since it makes their medical records accessible to improve their health status, and favorable technological and environmental conditions may also encourage them to intend to use patient portal technologies. 93 The other studies are consistent with this study result.12,21,69,88
Another study result shows that Habit is weakly associated with the patient's intention to use the patient portal. Those individual patients may think that accessing and using their medical records through the patient portal system is a good habit. 44 This may be due to more than one-third of our participants having social media and other mobile app usage habits, which can be another justification for this result. If patients experienced using other similar technologies to patient portals, they would become exposed to relying on and frequently using the existing system and are more likely intending to use the new system. 94 This result is supported by other studies.35,42,44,95
According to our study findings, the influence of the effort expectancy on the intention to use the patient portal was positively moderated by gender, and our study result is supported by other studies.12,47 This result revealed that being male was more impacted by effort expectancy than being female to intend to use the patient portal or that females’ behavioral intention to use the patient portal was less affected by effort expectancy than being male.
Finally, the findings of this study show that the relationship between facilitating conditions and behavioral intention to use patient portals was positively moderated by gender. This finding implied that the availability of resources, infrastructure support and knowledge have a higher impact on females than on males to intend to use patient portals, which is the effect of facilitating conditions on behavioral intention to use patient portals and is stronger in females. This result is also supported by other studies. 96 A likely reason for this significant difference might be the digital divide. In our study, males had approximately 58% social media exposure. In our country, males have better internet and digital device access, which helps them use the patient portal.97,98
Implication of the study
The results of this investigation have theoretical and practical implications. In theory, our results could allay concerns regarding patient portal use in areas with limited resources. It serves as a baseline for researchers, particularly in settings with limited resources, because of the limited evidence regarding the patient's intention to utilize the patient portal. Our study provides statistical support for the UTAUT2 model's significance in evaluating the patients with diabetes to use portal technology and the results may be applicable in other countries. Our comprehension of the importance of the major determinants of intention to utilize the patient portal for health management has also been enhanced as a result of this study.
Practically, this study offers insights for developers, managers, and decision-makers in the healthcare industry to improve the use and acceptability of patient portals among patients with diabetes. Moreover, it contributes to increasing the adoption of patient portals to reduce the prevalence of diabetes mellitus complications across Ethiopia. Implementers can enhance the usability of portal technology in the healthcare sector by ensuring that they complete healthcare services more quickly and that top management supports, allocates resources, and provides the knowledge for users to achieve the relative advantage of patient portal technology. Finally, this finding offers an input for policymakers creating healthcare policies that will encourage the acceptance of patient portals for health information management. Because performance expectancy, facilitating conditions, effort expectancy, and digital literacy have a significant impact on a user's intention to use the patient portal, practitioners should concentrate on those predictors to encourage patients to utilize the patient portal.
Strength and limitation of the study
Our study found significant insight into important predictors of behavioral intentions with the new external construct of digital literacy in addition to the original UTAUT2 constructs and used a large sample size. This study's limitations were, first, that since our study is cross-sectional, we are unable to draw conclusions on the causal relationship between the predictors and behavioral intentions to use the patient portal. Second, the study was quantitative, so we could not include patient perceptions about patient portal technology. Third, the study was conducted only at a public referral hospital, but it needed a study on general, primary, and private hospitals for more generalizability of the study results.
Conclusions
This study found that patients’ intention to use the patient portal was low. Most of the patients intended to learn about the patient portal. Digital literacy, performance expectancy, effort expectancy, facilitating conditions, and habit were identified as significant predictors of patients’ intention to use the patient portal. In addition, gender was found to have a moderating effect on the relationships between behavioral intention to use the patient portal and effort expectancy, as well as facilitating conditions. Despite this, age was found to have no significant influence on the relationships between all predictors in this study and intention to use the patient portal. Therefore, interventions are needed to improve patients’ intention to use the patient portal through awareness, capacity building, and improving the digital literacy level of patients. This will help improve patients’ intentions to adapt the patient portal technology for our country to improve patient-provider communication and give them access to their medical information.
Additionally, we suggest that implementers consider predictors such as performance expectancy, effort expectancy, facilitating conditions, and habits during portal implementation, as well as develop a patient portal with user-friendly features that enable patients to access their medical records through the portal system. So that according to this study result, we recommend the following interventions:-
Awareness and Capacity Building: Educational initiatives can raise awareness about patient portals, their benefits, and how to use them effectively. Digital Literacy Training: Programs can equip patients with the necessary digital skills to navigate the portal with confidence. User-Friendly Portal Design: Developing patient portals with intuitive interfaces and clear functionalities can enhance ease of use and encourage adoption. Facilitating Conditions: Ensuring access to devices and reliable internet connectivity, along with ongoing support from healthcare providers, can create an environment conducive to portal use.
Finally, we suggest that future researchers investigate using a qualitative approach to know patients’ perceptions about the patient portal and with additional constructs such as attitude, trust, and privacy concerns to generate more evidence in the area.
Footnotes
Acknowledgments
The authors want to acknowledge the University of Gondar, College of Medicine and Health Science, Institute of Public Health, for the approval of ethical clearance and provided support during the study. Finally, we also thank the data collectors, supervisors, and study participants.
Authors’ contribution
AWA was responsible for a significant contribution to the conceptualization, study selection, data curation, formal analysis, investigation, methodology, and original draft preparation. Resources management, software, supervision, validation, visualization, and reviewing are all handled by BT, MDT, and ZAM. They wrote the final draft of the manuscript, and the final draft of the work was read, edited, and approved by all authors.
Data availability
The data are available from the authors and accessible upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Aschale Wubete Abebe.