
Abstract
Background
Telemedicine has emerged as a novel healthcare service model that plays a vital role in addressing the unequal distribution of medical resources. Telemedicine has recently gained significant traction in economically prosperous cities such as Beijing, Shanghai, and Guangzhou in China. However, Xinyang City in Henan Province is an economically less developed city, and telemedicine is still in its early stages. By exploring the views of medical staff and administrators at Xinyang City's tertiary A-level hospital on telemedicine, this study aims to determine the development status of telemedicine services in Xinyang City. The objective was to identify the challenges in the construction process and formulate corresponding strategies for advancing telemedicine in Xinyang City.
Methods
Face-to-face personal interviews were conducted with 16 medical staff and administrators from a tertiary A-level hospital in Xinyang City, Henan Province, and the data were collected and analyzed using grounded theory. In the process of data analysis, NVivo12 software was used to encode and organize the data line by line.
Results
The development of telemedicine in Xinyang City has the potential to benefit residents, hospitals, and healthcare personnel despite several challenges, including the absence of laws and regulations, inadequate policy support, limited hospital cooperation, and low resident awareness, which must be addressed to unlock the full potential of telemedicine.
Conclusion
The telemedicine system in Xinyang City is currently in a coordinated developmental phase, and several areas require further improvement. The development of standardized telemedicine in Xinyang City requires government support, better training for general practitioners, public awareness campaigns, and improved technology while ensuring reasonable work schedules and motivating medical personnel.
Introduction
The World Health Organization defines telemedicine as the utilization of information and communication technologies by healthcare providers to transmit information related to medical services, diagnosis, prevention, treatment, research, evaluation, and continuing education from a distance. This practice aims to enhance the health and well-being of individuals and communities. 1 Telemedicine strives to leverage the expanding realm of technology to establish a more streamlined healthcare delivery system, as a pivotal component of an extensive digital health service framework. With telemedicine equipment, information, and communication technologies advancing rapidly, this innovative healthcare model is experiencing exponential growth and widespread global adoption.2,3
Telemedicine has evolved over the course of a century, progressing from the initial stages of SMS services to the advent of app-based services, culminating in the establishment of comprehensive telemedicine centers that cater to hospitals at all levels. 4 The evolution of telemedicine in numerous countries has yielded tangible outcomes, including expanded access to healthcare services for the population, decreased instances of cross-infections, diminished healthcare expenditure, and the advancement of health education initiatives.5–10 The United States, United Kingdom, and Australia are making significant investments in telemedicine to curb the influx of patients seeking emergency department care for non-urgent issues. 7 In an effort to encourage telemedicine adoption, 32 states in the United States have mandated telemedicine coverage and reimbursement, and a remarkable 76% of hospitals have embraced telemedicine as a means of engaging with their patients. 6 Furthermore, in the United States, educational applications of telemedicine facilitate the reciprocal exchange of information by connecting tertiary teaching hospitals with community or rural practices. 10 The United Kingdom is experiencing a rapid surge in the utilization of telemedicine, with an impressive 5.4 million users engaging with the telemedicine service provided by Push Doctor. 5 In Asia, Singapore is at the forefront of telemedicine adoption. 11 In April 2019, the Health Sciences Authority of Singapore released regulatory guidelines to clarify existing regulations pertaining to telemedicine. These guidelines encompass the categorization of services, risk assessments, and regulatory oversight of medical devices. 11 South Korea and Canada have made significant strides in enhancing access to healthcare services through telemedicine, particularly for individuals residing in sparsely populated regions with limited access to hospitals.8,9 Japan issued a document indicating a growing reliance on telemedicine to address the decline in medical services. 12
The unequal distribution of healthcare resources in China has emerged as a pressing issue, and telemedicine is an effective approach for addressing this challenge.13,14 China's high-quality healthcare resources are predominantly concentrated in provincial capitals and major cities, leaving smaller cities and rural areas with inadequate access to healthcare resources.13,15 China's high-quality medical resources are mostly concentrated in tertiary-level hospitals. 16 However, a scarcity of these tertiary-level hospitals in prefectural-level cities creates significant hurdles for patients residing in counties and rural areas in their quest for high-quality medical services.13,17,18 In addition, rural areas are home to a substantial number of elderly in dire need of high-quality medical resources.19–21 The imbalanced distribution of healthcare resources in China, coupled with its vast population, has resulted in a significant increase in patient numbers in most hospitals, placing substantial strain on the utilization of healthcare resources. 22 Patients who are unable to travel to urban areas for specialized healthcare services may experience heightened financial strain and potential delays in diagnosis and treatment. These challenges can adversely affect the physical and psychological well-being of patients and their families.23–25 As China's internet technology advances and the quality of online health services continues to improve, traditional healthcare channels are becoming increasingly integrated into digital networks. This transformation ushers in new opportunities for the healthcare sector.26,27 In 2014, Guangdong marked a significant milestone in China's healthcare landscape by establishing an inaugural hospital offering telemedicine services. 28 Following this landmark achievement, numerous medical institutions in China embarked on the journey of exploring and developing telemedicine services.29,30 With an increasing number of healthcare organizations embracing telemedicine services, municipal and county hospitals are now equipped to offer teleconsultation services to primary care organizations. 27 Simultaneously, the government has launched numerous policies and documents to champion the expansion of telemedicine in townships and rural areas. 27 By June 2023, the number of internet users in China had surged to 1.079 billion, with internet medical users reaching 364 million, constituting 33.8% of the total internet user population. 31 This ongoing growth in the number of internet users bodes well for the continued development of telemedicine in China.
Xinyang City, situated in the southernmost region of the Henan Province, occupies a predominantly mountainous terrain and exhibits limited economic development, primarily centered around agriculture. 32 The city's resident population stands at 6.19 million, with 3.16 million residing in urban areas and 3.13 million in rural areas, resulting in an urbanization rate of 51.14%. Notably, 15.9% of Xinyang City's population is 65 years or older. 32 Thus, approximately half of the residents in Xinyang City reside in rural areas. Additionally, Xinyang City is home to only one tertiary A-level hospital, the Xinyang Central Hospital, with relatively limited medical resources. Although telemedicine services have been successfully implemented and are operational in economically developed regions such as Guangzhou, Beijing, and Shanghai in China, the introduction of telemedicine in Xinyang is a relatively recent pilot program.33–37 In 2018, Xinyang Central Hospital released the “Notice on the Issuance of the Working Program of Xinyang City Central Hospital for Advancing Internet Medical and Healthcare Accessibility and Benefits for the Public.” This notice outlined the establishment of a telemedicine center in Xinyang City that would offer a range of services to medical institutions within the healthcare consortium. These services include teleconsultation, tele-imaging, teleultrasound, tele-cardiography, tele-checkups, tele-supervision, and tele-training. In 2022, Xinyang Central Hospital issued a “Notice on the Establishment of the Internet Hospital Working Leading Group of Xinyang City Central Hospital.” This notice outlines the formation of an internet hospital working group comprising various segments, including medicine, information technology, pharmacy, nursing, outpatient services, finance, public relations, diagnostics, and legal affairs. In light of these developments, this study aims to facilitate the advancement of telemedicine in Xinyang City. This will involve conducting in-depth interviews with healthcare professionals and administrators at Xinyang's tertiary A-level hospital, focusing on the construction and utilization of telemedicine in Xinyang City with the aim of identifying any challenges encountered during its implementation, to propose corresponding strategic recommendations. This study is expected to serve as a valuable reference for the ongoing development of telemedicine in Xinyang City.
Methods
Researcher role
The research members in this study are doctors of medicine and masters of medicine. Specific interview members have good communication skills and systematically learned qualitative research methods.
Study design
Semi-structured interviews were conducted with medical professionals and administrators of Xinyang City's public tertiary A-level hospital. This study aimed to delve into the present operational landscape and prospects of telemedicine in Xinyang City, identifying the challenges encountered during the implementation of telemedicine, to propose strategic solutions for the development of telemedicine within the city. These findings provide valuable insights, informing and guiding the ongoing construction of telemedicine in Xinyang City.
Recruitment
A convenient sampling method was used to recruit the participants comprising medical staff and administrators from Xinyang City's public tertiary A-level hospital. The interviews were scheduled at the participants’ convenience. Participants were recruited until data saturation was reached with no new information obtained 38 and interviewed between April and May 2023. The research protocol was approved by the Ethics Committee of Xinyang Normal University (Study ID: XFEC-2023-021).
Determination of sample size
Data saturation refers to the degree to which new data repeat previous data. 39 Theoretical saturation refers to “no new relevant data about a certain category, the category has developed well in terms of attributes and dimensions, showing changes. The relationship between genera has been fully established. 40 No further theoretical insights have been generated.” 41 In the practical research of grounded theory, the judgment of data saturation, theory saturation, and theoretical sampling are cyclic processes. The research team followed the principle of simultaneous data collection and analysis. In the data collection stage, to quickly collect effective data, data saturation must be determined to avoid information redundancy. If the data is saturated, data collection will be suspended. We then analyze the data and determine whether theoretical saturation has been reached based on the analysis. Otherwise, theoretical sampling is carried out. Currently, a new stage of data collection is entered, data saturation is judged again, data analysis is carried out, and theoretical saturation is judged based on the analysis. If the saturation is low, further theoretical sampling is conducted until theoretical saturation is reached. In this study, when the researchers analyzed the interview data of the sixteenth participant, it was found that it was highly coincident with the content and theme of the analyzed data, and no new code was generated. Therefore, it can be concluded that the data collection has reached the theoretical saturation and can pass the saturation test. 38 The study included 16 medical staff and administrators.
Data collection
Prior to formal interviews, the interviewer introduced himself to the interviewees and established a friendly and harmonious relationship. Individual face-to-face and one-on-one interviews were conducted according to the interview outline in a quiet office. Before the study, the researcher explained the theme and purpose of the study to the interviewees and informed them that the interview would be recorded and the information provided would remain anonymous. After signing an informed consent form, the interviewees first completed a demographic information survey that included basic sociodemographic information. The general information questionnaire is presented in Appendix S1.
The preparation of the interview outline consisted of three steps. First, an initial draft of the interview outline based on preliminary research by the research group was written. 42 Second, retrospective reading and adoption of previous qualitative telemedicine research literature were conducted. 43 Finally, the researcher invited two target participants to complete two pre-interviews and revised the interview outline according to the questions in the pre-interview, to structure the final interview outline. The main questions of the interview outline included reasons for the implementation of telemedicine, advantages and limitations of implementing telemedicine, shortcomings and challenges of telemedicine development, and how to promote the implementation of telemedicine. Appendix S2 presents an outline of the interviews.
Interviews and content coding were conducted simultaneously by two researchers, and the outline was dynamically adjusted iteratively during the interviews. The interviewees’ verbal and nonverbal expression were observed and recorded during the interview. The interviews typically lasted for approximately 22 minutes per individual. Recordings were promptly transcribed into text within 24 hours of the interview, resulting in a substantial document of approximately 50,000 words. The transcripts were returned to the interviewee to check for omissions or distortions, and a consensus was reached.
Data analysis
In this study, the NVivo12Plus software was used to initially conceptualize the transcribed text of the interviews, refining and clustering the concepts to form themes. This study adopted the programmatic grounded theory to conduct bottom-up three-level coding of the interview content, which emphasizes the systematic operation process, and the mining of practical phenomena, to reveal the internal correlation between categories in a more standardized way. 40 The rooted theory is coded in three steps: open, axial, and selective coding. 44 Open coding was used to conduct preliminary processing of the data collected in the interview, selecting the sentences or fragments that can be encoded and conceptualizing them sentence-by-sentence, to determine the concept categories from the data, whereby a total of 49 concepts were obtained. Axial coding involves deduction and induction, constantly comparing the different categories obtained in open coding for logical connection, to combine, extract, and integrate into a higher level of abstraction of the main category, whereby 13 main categories were formed. Selective coding summarizes the main categories obtained through associative coding to obtain the core categories. Through analysis and comparison of the original data, four core categories were extracted: Analysis of strengths, pre-service preparation, medium-term publicity channels, and analysis of obstacles. The encoding results are presented in Appendix S3.
Results
Participants
Sixteen participants, including medical personnel and administrators, participated in the study. Among them, there were eight females and eight males, with eight highly knowledgeable about telemedicine, seven with general familiarity, and one with limited or no familiarity on the subject. Table 1 provides an overview of the interviewees’ general information.
General information of interview subjects.

Note: Familiarity with telemedicine: very familiar = 5, generally familiar = 4, moderately familiar = 3, unfamiliar = 2, very unfamiliar = 1.
Implementation and obstacles of telemedicine in underdeveloped cities of central China
The theoretical model diagram derived from this study is shown in Figure 1, which primarily includes: analysis of strengths, pre-service preparation, medium-term publicity channels, and analysis of obstacles.
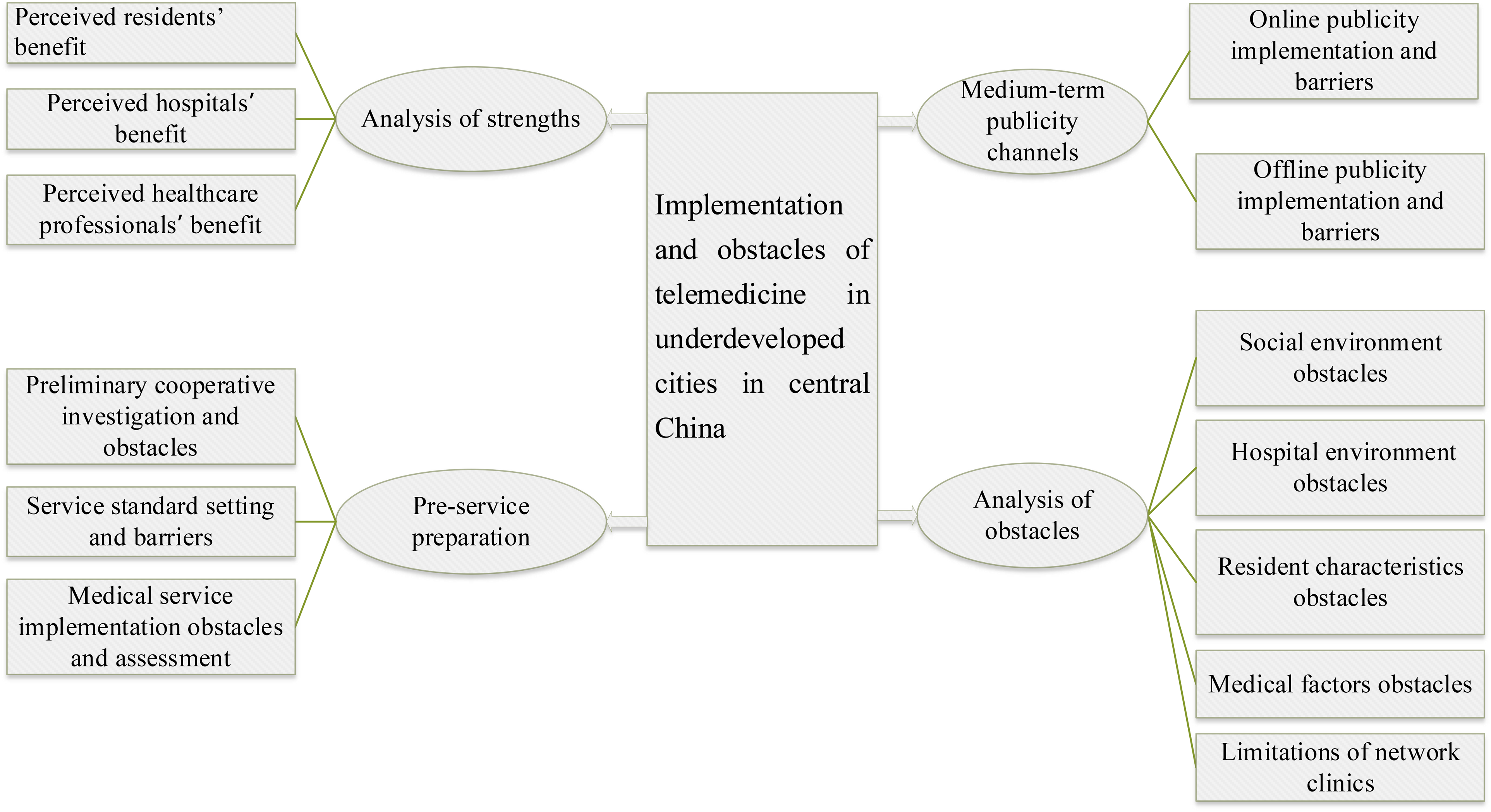
Implementation and obstacles of telemedicine in underdeveloped cities in central China.
Theme: advantage analysis, pre-service preparation, medium-term publicity channels, analysis of obstacles
Advantage analysis: perceived residents’ benefit, perceived hospitals’ benefit, Perceived healthcare professionals’ benefits
Perceived residents’ benefit
All interviewees indicated the benefits of telemedicine services for their residents. First, China grapples with the persistent challenge of uneven distribution of medical resources.
45
Telemedicine serves as an effective remedy that erases temporal and spatial barriers in optimizing efficiency.
46
The development of telemedicine in China has shown a growing trend and provides great benefits, especially to medical institutions located in less-developed regions and senior citizens with less mobility.
27
Second, telemedicine services can mitigate overcrowding, thereby reducing the risk of cross-infection. This creates a conducive healthcare environment for patients. In addition, after the doctor writes a prescription online, the patient can directly go to the hospital or fill in the information, such as the receiving address, to obtain the drug, which ensures that the drug needs of the patient are met. With telemedicine evolving, its reach has extended to include remote health monitoring based on body-worn sensors and devices. This technology enables real-time tracking of residents’ health status by family members or healthcare professionals from a distance. In cases of abnormalities, timely interventions can be performed to prevent the exacerbation of the ailment. The most significant advantage, in my opinion, is the cost-saving aspect for patients. They no longer need to incur unnecessary expenses, such as taxi fares or accommodation costs, and it also saves them valuable time. (N11) Telemedicine boasts numerous advantages, including the ability to deliver prescribed medications right to the patient's doorstep, offering unparalleled convenience in this regard. (N4) Telemedicine establishes direct connections between local patients and specialists, reassuring patients as they receive remote but personal guidance on their diagnosis and the subsequent steps in their treatment. (N7) Telemedicine effectively curtails the necessity for patient travel and mitigates the potential for cross-infection, representing a substantial benefit for patients’ well-being. (N3) This Internet hospital doesn't simply manage diseases; it's more about managing health, focusing on “preventing illness rather than treating it.” It's akin to constructing an individual's health profile from birth and subsequently intervening in their health behaviors. While direct disease treatment remains challenging, managing an individual's health can significantly reduce the onset of illnesses. (N13)
Perceived hospitals’ benefit
Telemedicine services can not only enable hospitals to introduce advanced technology but also promote the development of graded diagnosis and treatment in China. First, remote consultations afford hospitals the opportunity to tap into advanced medical technologies of both domestic and international sources, such as the Internet of Things, cloud platforms, and medical big data technology.47–49 Medical staff in hospitals can be an important resource for scientific medical research, improving the level of medical services through extensive exposure to difficult and complicated diseases. Second, telemedicine uses information and telecommunication technology to transmit medical information for diagnosis, treatment, and education.
50
Digital and intelligent operation models have broadened the applications of telemedicine and health management.
51
Patients can access medical consultations through the Internet, allowing doctors to assess their physical condition and determine whether a referral to higher-level hospitals is necessary. Local health care facilities can directly diagnose and treat common diseases with the assistance of professionals from tertiary hospitals. Thus, top-tier hospitals have more time to focus on serious and intractable cases.46,52,53 Patients can consult doctors via the Internet. This approach contributes significantly to alleviating the burden on tertiary hospitals, thereby preventing the inefficient allocation of medical resources. I believe that hospitals embracing telemedicine can introduce new technologies and programs from more advanced first-tier cities. (N1) We can learn advanced technologies from other hospitals based on telemedicine platforms, such as remote consultation, to promote the development of hospitals. (N9) In our hospital, we have a specialized medical development section that focuses on internet-based initiatives. It is advantageous to have dedicated personnel and departments responsible for handling these endeavors. Furthermore, the convergence of computerization with new technologies represents a commendable initiative to enhance hospital processes. (N2) The telemedicine service can promote the information reform of the hospital. It can bring convenience to common people and promote the development of the hospital. (N3) For instance, this can further the ongoing promotion of tiered diagnosis and treatment, enabling common cases to be managed effectively in third- and fourth-tier city hospitals. (N1) I feel that simple diseases can be solved by telemedicine instead of going to a tertiary hospital. The telemedicine service is conducive to promoting the development of hierarchical diagnosis and treatment, with different levels of medical institutions undertaking the treatment of different diseases. (N10)
Perceived healthcare professionals’ benefits
As telemedicine advances, an increasing number of patients can resolve their health concerns through online consultations, thereby alleviating the strain on in-person clinics. Furthermore, medical professionals can use smartphones or computers to assist individuals during their free time, enhancing their intrinsic value. Additionally, healthcare personnel can engage in learning, communication, and dialogue with medical experts, which facilitates the enhancement of their medical skills, ultimately enabling them to deliver superior diagnostic and treatment services. When executed effectively, these initiatives yield numerous benefits, such as providing patients with easy and timely guidance. This approach alleviates the burden on doctors, as patients visiting Tertiary A level Hospitals tend to have more complex conditions. (N16)
Pre-service preparation: service standard setting and barriers, Preliminary cooperative investigation and obstacles, Medical service implementation obstacles and assessment
Service standard setting and barriers
In the preliminary phase of telemedicine services, establishing standardized protocols for telemedicine services is a fundamental and pivotal task. This includes enhancing the service process and establishing an equitable fee structure. In the interviews, the respondents believed that refined service processes would provide convenience to patients; the telemedicine services of different regions and hospitals are different, and the service process should be formulated according to the actual situation of the hospital and region. The development of service processes and precautions can help reduce security risks and improve service quality. The respondents in this study believed that the current telemedicine service fee standard is still unclear, and many factors need to be considered, such as whether the standard is appropriate in view of the offline consultation fee standard, local economic level, and input cost. A previous study suggested that online visits cost less than offline visits, frustrating doctors and subduing their enthusiasm and initiative for online visits that do not reflect the value and differentiation of expert knowledge.
54
For patients, the cost of telemedicine affects their judgment of the doctor's service quality and influences their choice.
55
We have a lot of work ahead of us, particularly in ensuring that our fees are both reasonable and standardized. Furthermore, effective leveraging of Internet platforms will be crucial for seamless implementation. (N16) The specific precautions and processes of telemedicine should be clarified. Preparations need to be adequate and secure. The procedures vary from one medical institution to another. (N6) At present, the country, including our province, has not issued a telemedicine charging standard, which should be formulated according to various situations. (N10) At present, there is no transparent pricing system for telemedicine services in Xinyang City. Telemedicine services need to be transparent and have reasonable charging standards. However, there are also obstacles to the development of charging standards. For example, the cost of telemedicine services needs to refer to the charge of offline consultation. (N1)
Preliminary cooperative investigation and obstacles
In rural areas where medical resources are scarce, patients require telemedicine support to solve medical problems.
26
As an underdeveloped city, the medical care in Xinyang City is at a low level with only a single third-level hospital, 12 second-level hospitals, and 20 first-level hospitals.
56
Cooperation between telemedicine service institutions can help solve the problems of the imperfect layout of existing medical service system, insufficient quality medical resources, and unreasonable allocation. In addition, some participants expressed the view that telemedicine equipment was insufficient. Doctors communicate with patients only through mobile phones. A survey of medical institutions that conduct telemedicine would enable hospitals to further learn and improve telemedicine facilities and technologies to provide better medical services for the majority of residents. A pre-survey of residents is essential for gauging their medical service requirements and healthcare concerns, to comprehend the ideal telemedicine services desired by the community. Before launching telemedicine, the first thing to do is to research. Furthermore, the relevant departments of the hospital seek cooperative hospitals. We get prepared to debug equipment. (N1) Doctors now check patients’ information through mobile phones, and there is no advanced equipment, which is also not conducive to the development of telemedicine. (N5) It's crucial to conduct surveys with residents to ascertain their healthcare needs before introducing the program. Alternatively, after implementing the program for a period, assessing people's satisfaction levels and soliciting additional suggestions or comments from the public, will allow us to make continuous improvements. (N2)
Medical service implementation obstacles and assessment
According to the Henan Provincial Bureau of Statistics, there were 12,154 professional doctors and 18,724 registered nurses in Xinyang in 2023.
57
However, a previous study suggested that while doctors can obtain key information from patients within a few minutes through in-person communication and examination, the information received in the same amount of time online tends to be limited.
54
In addition, patients who use internet hospitals have a more negative view of the doctor-patient relationship. Thus, doctor-patient communication problems may pose new challenges in telemedicine.58–61 To overcome these challenges, medical personnel engaging in telemedicine must undergo comprehensive training and credentialing tests to ensure proper implementation of technology and medical procedures in this domain.
62
Medical professionals participating in telemedicine must be patient and responsible. Doctors should receive more training to better communicate with patients. The level of medical care in Xinyang City is still uneven. Therefore, hospitals need to carry out special qualification training and assessment for medical personnel participating in telemedicine services. Only qualified medical personnel can engage in telemedicine services to improve service quality. (N2) I think doctors in telemedicine services should have a scientifically rigorous attitude. They should follow the rules of the medical system. They should have certain qualifications. (N2) I think the doctor in telemedicine must be a general practitioner. For example, a patient with a headache does not know whether to go to a medical or a surgical doctor. At this time, I think the general practitioner is better. (N9) In remote consultations, people may struggle to articulate their physical condition due to nervousness or network issues. Therefore, doctors must be careful and patient to thoroughly comprehend the condition, assess it comprehensively, and then prescribe medication. The approach should not involve hasty conclusions or arbitrary medication prescriptions. (N16)
Medium-term publicity channels: online publicity implementation and barriers, offline publicity implementation and barriers, Public promotion is less intensive than commercial promotion
Online publicity implementation and barriers
In an era of widespread internet usage, online platforms represent a crucial avenue for telemedicine promotion. Interviewees recognized the significance of leveraging the Internet, suggesting that promotions be conducted through online media outlets and the hospital's WeChat public account. However, some interviewees expressed reservations about relying solely on online channels for promotions. As residents of rural areas have low levels of smartphone use and education, promoting telemedicine is difficult.
63
While our hospital does use the public account to promote telemedicine, its reach is somewhat limited. Some people don't read public accounts. (N3) I think the obstacle to online publicity at this stage is how to cover the content of our hospital's telemedicine service from a broader perspective and let other people know. (N8) We have patients coming to see a doctor; we can also prepare a wechat QR code for patients to scan so that inpatients can get familiar with it. Sometimes online publicity may not have a very good effect because some patients do not use mobile phones. (N4)
Offline publicity implementation and barriers
Telemedicine in Xinyang City is still in its nascent stages and requires robust outreach from residents. Offline promotional strategies primarily involve establishing dedicated telemedicine consultation counters within hospitals, crafting informative brochures, and conducting telemedicine educational initiatives. By employing a diverse range of offline promotional tactics and collaborating across multiple departments, more effective outreach efforts can be achieved, bolstering residents’ trust in telemedicine. However, there are obstacles to offline promotion. For example, how to inform patients about these propaganda activities in their daily lives, how to guide residents to the telemedicine consultation window, and how to teach elderly residents to use telemedicine services. When introducing telemedicine to residents, initially skepticism may arise, but I believe that through comprehensive explanations, gradual acceptance can be fostered. (N5) We need to invite some well-known experts, and then promote the visibility of experts. Only face-to-face communication in advance can make residents believe in telemedicine services. However, if residents are aware of these offline promotional activities, it may also be an obstacle, including a series of processes that need to be carefully arranged. (N1) Another way for us telemedicine doctors is to also promote other doctors, that is, doctor to doctor promotions expand the scope of publicity because some doctors are not good at using smart phones. (N6)
Public promotion is less intensive than commercial promotion
In the era of user-generated content and self-media, a plethora of mobile phone applications offer online medical consultation services, some formalized, often with commercial motivations. However, the overall quality of such consultations tends to be subpar, engendering risks in the process. The advertising of these commercialized online medical consultations spans a wide array of domains, fostering increased competition in the online medical consultation market. This heightened competitiveness poses challenges to the integrity of public welfare and formal online medical consultation. In today's age of self-media and pervasive internet access, people have gradually embraced online medical consultations. However, a myriad of irregularities exist. Moreover, many individuals disseminate scientific information on platforms like TikTok although what they convey may not always align with reality. Their messaging tends to be robustly commercial, thus creating competition for regulated public hospitals. (N8) At present, the promotion of telemedicine is not sufficiently comprehensive, and enhancing telemedicine promotion within hospitals is imperative for foster public understanding and acceptance. (N8)
Analysis of obstacles: social environment obstruction, The obstacles caused by residents’ information literacy, Hospital environment obstacles, Slackening of primary care physicians, limitations of network clinics
Social environment obstruction: the lack of laws and regulations leads to unclear medical dispute resolution, lack of financial support restricts the development of telemedicine
Doctors and nurses alike express apprehension regarding the handling of medical disputes in telemedicine, as there remains a lack of clarity in addressing issues arising from online consultations. For instance, the “home-based healthcare service” necessitates nurses to conduct medical procedures within the patient's home environment, yet no established protocol exists for resolving medical disputes that may arise during these operations. Consequently, the delineation of responsibilities remains unclear. The extent to which doctors can provide guidance in telemedicine is significantly influenced by the breadth and clarity of existing laws and regulations. At present, there remains ambiguity in the formulation of these laws and regulations. (N10) Various complexities are involved in the tasks that nurses perform within patients’ homes, and I am concerned about how we would address medical disputes if they were to occur. (N12)
Lack of financial support restricts the development of telemedicine
The growth of telemedicine has faced various facets of financial constraints, involving investments in equipment and technology, training and deployment of healthcare professionals, as well as platform construction and operation. The shortage of funds in telemedicine is primarily linked to the underdeveloped nature of local economies, particularly in remote mountainous or rural areas where networks, transportation, and other infrastructure may be lacking.
67
Additionally, residents’ limited healthcare expenditure hampers the expansion of telemedicine services. The development of internet healthcare is heavily contingent on the economic status of a region. It's intrinsically tied to a locality's economic level, necessitating government investments if they aspire to cultivate it. (N16) The cost factor remains a significant question mark. Can telemedicine secure inclusion in Medicare, and what would be the reimbursement rate? Given the current charges in Henan Province, which stand at 200 RMB, patients seeking consultations across provincial lines would need to make direct payments to the teleconsultant at the other end. (N9)
The obstacles caused by residents’ information literacy
Several interviewees highlighted that there are still numerous residents with limited education and difficulty in using smartphones, tending to adhere to traditional healthcare models. These factors pose challenges to the widespread acceptance of telemedicine. Transforming residents’ mindsets is a key challenge in the adoption of telemedicine. Moreover, the absence of in-person consultations through mobile phones or computers can make residents anxious, potentially leading to insufficient disclosure of their medical histories or physical conditions to doctors. The question of whether patients accept telemedicine or not is multifaceted; some patients embrace it, whereas others do not. People's willingness to visit hospitals today is linked to their belief that online consultations are unrealistic. Some individuals prefer accepting the reality of physical medical visits and find them more convenient. (N6)
Hospital environment obstacles: low management attention, low management attention, shortage of general practitioners
Internet hospitals represent a nationally endorsed initiative, but there might be administrators who perceive it as lacking the significance necessary for robust support. (N12) I think the hospital management plays an important role in the development of telemedicine. The lack of attention of hospital management is also critical. (N16)
I believe the initial groundwork involves fostering collaboration between hospitals, particularly in this specific field of healthcare. For example, I am from Luoshan City, and I have established a productive partnership with the internet hospital serving Luoshan. My current hospital and the internet hospital in Luoshan engage in collaborative consultations. (N7) The cooperation of telemedicine service in Xinyang is not sufficient for the telemedicine needs of first-, second- and third-level hospital cooperation. For example, tertiary hospitals can undertake a training program for the medical staff of these community hospitals. (N13)
Another drawback is that in certain locations, there exists a shortage of physicians. For instance, if a surgical condition requires examination, a specialist is needed. In such cases, the advantage of having a general practitioner may not be entirely sufficient, as the limited number of doctors may impede in-depth disease analysis. (N7) These doctors at the general hospital are not enough. If we follow the national policy in Henan Province, there will still be a shortage of 9000 general practitioners. Few doctors now register as general practitioners. Telemedicine often requires more general practitioners. (N7)
Medical factors obstacles: low participation of primary care staff, risks to the personal safety of health care providers, slackening of primary care physicians
Many specialists may not have sufficient time to devote to telemedicine. They are often preoccupied with their specialized tasks and may perceive their specialties as more significant. Consequently, they may allocate less attention to telemedicine. (N12) Medical staff engaged in telemedicine services may have less rest time, which may reduce their enthusiasm and initiative in their work. (N1)
Most of the individuals providing home-based health care services are nurses, and the primary concern revolves around safety. Although the system includes a key alarm feature, it primarily activates after an incident has occurred, and even then, the police response may not be immediate. Therefore, there remains a risk of danger. (N13) Healthcare workers to the patients’ home, healthcare workers are also a safety risk. We also need to consider the safety of health workers. (N3)
While every third- and fourth-tier city has its own development potential, the major concern is that excessive reliance on Internet consultations may result in complacency among doctors in these cities. They may start feeling that they are merely needed for basic illnesses and may not be motivated to engage in ongoing learning and professional development. (N1) Telemedicine services may make the work of doctors in some grass-roots hospitals slack off. Therefore, in the development of telemedicine services, it is necessary to strengthen the management of primary care physicians. (N2)
Limitations of network clinics: no traceability of e-prescription, inability to do physical examination, insufficient network facilities
Regardless, I always give them a quick check afterward. Sometimes, when I send an e-prescription, I am unsure whether the patient has retrieved it or not. It lacks a traceability feature. (N5) I've written a prescription on my phone twice before, and I don't know if it worked. This could be a problem with the procedures, which could be improved a little bit. (N8)
For instance, when specialists require access to test results, the inability to receive these results promptly can lead to decreased efficiency. Additionally, certain hospitals may not acknowledge the results of physical examinations conducted at other medical facilities. (N7) In this kind of online consultation, I cannot ask him to conduct a physical examination, which is not very convenient. (N4)
One drawback worth noting is the delay in receiving immediate SMS alerts following patient consultations. After entering the client, there can be a delay of more than ten minutes before the patients’ information can be accessed. (N4) Network facilities in rural areas are insufficient. Telemedicine may have problems such as network delay if implemented in rural areas. Therefore, we must strengthen the network facilities in rural areas. (N13)
Discussion
This study focused on examining the existing landscape of telemedicine services in Xinyang City. This was accomplished by conducting in-depth interviews with 16 medical professionals and administrators associated with a tertiary A level hospital located in the same city. Although telemedicine services have undeniably brought advantages to residents, healthcare institutions, and healthcare providers, there are still notable challenges stemming from social and hospital environments, resident demographics, limitations intrinsic to healthcare providers, and issues concerning network diagnosis and treatment.
Telemedicine offers significant advantages to residents, hospitals, and healthcare professionals. First, for residents, telemedicine delivers enhanced accessibility and cost-effectiveness in healthcare services while granting access to superior-quality medical resources. This aligns with previous findings.68–71 Telemedicine not only aids residents in their rehabilitation, but also plays a pivotal role in health management. For instance, the establishment of electronic health records for individuals from birth streamlines early health interventions and aids in uncovering the root causes of diseases. Second, at the hospital level, telemedicine can catalyze the hospital informatization process, fostering high-quality development. Telemedicine encourages patients with common and frequent ailments to initially seek care at primary healthcare institutions and facilitates efficient referrals. This promotes the evolution of hierarchical diagnosis and treatment, enabling the efficient flow of high-quality medical resources. Finally, the integration of telemedicine with hierarchical diagnosis and treatment alleviates the burden on the healthcare system. Remote sharing of medical cases among healthcare professionals and hospitals contributes to the continuous enrichment of knowledge and enhances the skills of doctors and nurses. 27
In the contemporary landscape, several impediments persist in the advancement of telemedicine in Xinyang City. Within the social sphere, interviewees identified notable shortcomings, including the absence of requisite laws and regulations, 72 inadequate policy support and financial investments, and mounting competition within the market. First, the realm of medical practice remains susceptible to medical disputes, rendering the distributions of responsibilities a complex endeavor.49,73 In the absence of a standardized framework, the quality of online consultations exhibits significant disparities, thereby posing a challenge to residents in identifying dependable online medical consultation services. To a certain extent, this predicament hinders the growth of online medical consultation services, especially in public hospitals. Consequently, the development of robust telemedicine-related legislation, regulations, and standardized protocols has emerged as a pivotal imperative. Furthermore, the provision of comprehensive policy support and financial resources augment the motivation of medical professionals engaged in telemedicine services, facilitating advancements in telemedicine technology and equipment. Finally, establishing equitable pricing structures for telemedicine services coupled with their inclusion in medical insurance reimbursement schemes has the potential to alleviate the financial burden borne by patients. This measure is particularly advantageous for individuals grappling with financial constraints, ultimately bolstering the acceptance of telemedicine among a wider spectrum of patients. There are also many other factors to consider when setting these criteria, such as the cost of offline consultation and local economic development. Progress in telemedicine necessitates judicious allocation of various policy resources to catalyze development.
Factors in hospitals and the broader healthcare system can also impede the advancement of telemedicine. Hospital-related barriers predominantly include inadequate telemedicine promotion, limited managerial attention, deficient collaboration, and a scarcity of general practitioners. First, interviewees observed that many residents remain unaware of telemedicine services, with publicity efforts primarily relying on public channels and individual healthcare professionals, rendering these efforts insufficient. Second, hospital administrators had varying perspectives on telemedicine. While most administrators recognized the promising prospects of telemedicine, others failed to fully understand its potential advantages. This finding aligns with prior research emphasizing the pivotal role of leadership attention in shaping telemedicine development. 74 Third, the absence of collaborative ventures with other hospitals and shortage of general practitioners in Xinyang City's telemedicine ecosystem may have restricted residents’ access to medical resources. To overcome these obstacles, the training of medical personnel engaged in telemedicine services should be increased. Hospitals must fortify their alliances with other medical institutions to enable knowledge sharing and efficient utilization of medical resources. Ultimately, this will facilitate the sustained efficacy of telemedicine and foster the synergistic development of public hospitals at every tier within Xinyang City. Regarding healthcare personnel, certain primary healthcare providers in Xinyang City have yet to embrace the concept of forming medical alliances with higher-level hospitals and participate in telemedicine initiatives. Knowledge and attitudes play pivotal roles in healthcare workers’ acceptance of telemedicine. 75 Therefore, hospital leaders and publicity departments should intensify their efforts in disseminating and elucidating telemedicine policies, while alleviating the workload burden on healthcare staff. A more reasonable workload would enable doctors to deliver thoughtful diagnoses, engage in comprehensive patient interactions, and exhibit a positive attitude, which are all instrumental in delivering superior telemedicine services.76,77
Residents play a pivotal role in telemedicine, and their individual attributes can serve as either catalysts or impediments to the development of telemedicine. First, residents of Xinyang City often exhibit low levels of education, 32 have difficulty in navigating cell phones, and encounter challenges in articulating their medical conditions to healthcare providers. Second, residents are accustomed to traditional in-person medical consultations and harbor skepticism towards online alternatives because they find them less familiar and comfortable. These factors contribute to the lower acceptance of telemedicine services in the region, in contrast to previous studies that highlight the widespread acceptance of telemedicine among the general population. 78 Residents with limited cognitive capabilities may encounter difficulties in utilizing telemedicine platforms, leading to a reduced adoption rate. 79 Furthermore, some patients struggle to convey their medical condition comprehensively to physicians during online consultations, possibly because of heightened anxiety. To address these challenges, hospital departments should intensify their efforts to raise awareness and understanding of telemedicine among residents, thereby facilitating gradual acceptance. Healthcare professionals should enhance their communication skills to acquire a more comprehensive understanding of the patient's medical history and condition. Moreover, telemedicine service systems can be equipped with mechanisms for collecting and documenting relevant patient information, thereby furnishing healthcare providers with a more robust foundation for diagnosis and treatment decisions.
Web-based healthcare systems have certain limitations. First, all respondents unanimously acknowledged that one of the primary drawbacks of online consultation is the inability to conduct physical examinations, which serve as a critical foundation for the physician's diagnosis. Future innovations should address this constraint. Second, due to social and geographical factors, patients in specific regions lack access to networks and communication devices that are prerequisites for telemedicine, 67 resulting in disparities in telemedicine accessibility and usage. Finally, the respondents highlighted the issue of nontraceable e-prescriptions. Hence, network infrastructure fortification and enhanced telemedicine applications are required to effectively mitigate these limitations.
Research significance and suggestions for future development
Medical institutions in Xinyang City started constructing Internet hospitals in July 2018. At this stage, 10 county hospitals, 154 township health centers, 25 community service centers, 98 community service stations, and 2490 village clinics have been completed, and a total of 2531 free distribution points have been fully covered. Relying on the National Telemedicine Center to establish a telemedicine information system, the telemedicine system has been connected to 23 medical institutions and three 120 emergency vehicles. The Internet hospital has been online for 683 days, and 657 doctors with more than three years of independent clinical work experience have been online in the Internet hospital. At present, the Internet hospital has 51 online departments, including general medicine, internal medicine, surgery, obstetrics and gynecology, pediatrics, psychiatry, and traditional Chinese medicine, with more than 30,000 online consultations and 1200 electronic prescriptions.
From the perspective of the medical staff and administrators of a public grade-three hospital in Xinyang City, this study discusses the current development status of telemedicine services in Xinyang City, focusing on analyzing the advantages and obstacles of telemedicine. Although telemedicine has been operational, it is still in its initial stage, and there are problems, mainly in the following aspects: First, regional information sharing and mutual recognition in the medical community need to be improved; Second, the problem of “digital divide” among special groups still exists. Third, the entire lifecycle of digitally intelligent medical services is yet to be established.
From the perspective of the medical staff and administrators of a public grade-three hospital in Xinyang City, this study discusses the current development status of telemedicine services in Xinyang City, focusing on analyzing the advantages and obstacles of telemedicine. Although telemedicine has been operational, it is still in its initial stage, and there are problems, mainly in the following aspects: First, regional information sharing and mutual recognition in the medical community need to be improved; Second, the problem of “digital divide” among special groups still exists. Third, the entire lifecycle of digitally intelligent medical services is yet to be established.
Recommendation 2: A social and working environment for the use of digitally intelligent medical services should be created with commensurate effort. In building a social and work environment for the use of digitally intelligent healthcare services, the key goal is to create an ecosystem that integrates technology and healthcare so that digital tools can be more smoothly embedded at all levels of healthcare services. Interdisciplinary collaboration is required, including the joint efforts of information technology professionals, healthcare practitioners, and policymakers. At the social level, digital literacy education should be strengthened and the public's cognition of log-intelligent medical care should be improved, to encourage patients to actively participate in digital medical services. In the workplace, healthcare professionals must be trained for proficiency in the use of digital tools, and healthcare organizations must invest in efficient and secure information systems to ensure the privacy and security of patient data. We will build a medical service ecosystem that supports innovation, intelligence, and efficiency through joint efforts, thereby providing patients with a more personalized and convenient medical experience.
At the same time, there is a certain herd mentality in the use of intelligent medical services by doctors, nurses, and patients, which is influenced by multiple social levels, such as hospital management. First, the publicity and guidance of log-intelligent medical services can be strengthened through multiple channels of hospital management and relevant government departments to create a relaxed public opinion environment for the use of digitally intelligent medical services. Second, the supporting medical equipment should be customized and supplemented according to the working environment of doctors and nurses when using digitally intelligent medical services to speed up the operational efficiency of the entire digital medical service system. Finally, hospital management should ensure that doctors and nurses undergo the corresponding training and learning of the digitally intelligent medical service system, formulating its training system and training plan. Doctors and nurses with a strong sense of responsibility, high enthusiasm for digital intelligent medical service modes, and abundant spare time should be targeted for early digital intelligent medical service training so that they can become the backbone of the department's digital intelligent medical service mode to drive and assist the ensuing training personnel.
Third, a multiparty incentive mechanism should be established for the use of digitally intelligent medical services. At this stage, digital intelligent medical services may also pose risks such as information leakage, loss, and unreliability. Medical institutions in Xinyang City still lack relevant norms for Internet-based medical care, and the corresponding regulatory policies and systems are imperfect. However, the development of digital intelligent medical services involves certain uncertainties. Therefore, the high-quality development of digital intelligent medical services in Xinyang medical institutions requires improvements in relevant laws, regulations, and institutional guarantees. Only by cooperating with medical institutions and social capital can government departments win the trust of doctors, nurses, patients, and remaining sectors of society. Medical institutions in Xinyang City can establish reasonable incentive mechanisms for the promotion and application of digitally intelligent medical services to attract social resources to participate in the construction of digital intelligent medical service projects. For example, a certain proportion of funds can be invested for the construction of digital medical services without requiring dividends for operating profits in project promotion and operation stages. Alternatively, credit guarantee can be provided to digital intelligence medical service companies, to reduce the risks and operating costs faced by software companies of these services and promote the development of software companies and industry at large. The incentive would mean that Xinyang medical institutions would be able to explore the reform of the salary incentive system for medical care. Based on background usage records of digital intelligence medical services, the time spent by doctors and nurses using digital intelligence medical services and the time and situation of log-intelligence medical services used by patients under management can be included in the performance appraisal system of doctors and nurses to improve their participation in the log-intelligence medical service model.
Limitations
The limitations of this study are summarized as follows: First, the interviewees primarily consisted of medical staff and administrators from tertiary hospitals, which represents a limited sample source. Future research should consider gathering the perceptions of various groups on telemedicine to attain a more comprehensive perspective. Second, this study relied on qualitative research as the sole methodology. In future studies, it would be beneficial to incorporate a variety of research methods to gain a deeper understanding of telemedicine development.
Conclusions
This study primarily focused on the current state of telemedicine service development in Xinyang City, along with corresponding strategies to address the challenges encountered. Although telemedicine services in Xinyang City have made healthcare more accessible to patients, improved operational efficiency, facilitated resource sharing, and enhanced hospital capabilities and healthcare worker competencies, there are still several obstacles that hamper its development. These challenges include the absence of telemedicine-related legislation and regulations, limited policies and financial support, inadequate attention from hospital management, insufficient and ineffective publicity efforts, lack of collaboration, limited acceptance of telemedicine by residents, low engagement of primary healthcare personnel, inability to conduct remote physical examinations, and shortcomings in telemedicine software technology. To foster the sustainable and effective growth of telemedicine services in Xinyang City, the current challenges must be addressed, and potential future issues should be anticipated. This can only be achieved through ongoing enhancements of hospital infrastructure, public awareness, and regulatory frameworks.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241277670 - Supplemental material for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City
Supplemental material, sj-docx-1-dhj-10.1177_20552076241277670 for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City by Peng Qingjie, Huang Wanyu, Yang Jingying, Yang Ming, Wang Linlin, Mao Qiyue, Wang Fan and Pan Minghao in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241277670 - Supplemental material for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City
Supplemental material, sj-docx-2-dhj-10.1177_20552076241277670 for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City by Peng Qingjie, Huang Wanyu, Yang Jingying, Yang Ming, Wang Linlin, Mao Qiyue, Wang Fan and Pan Minghao in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241277670 - Supplemental material for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City
Supplemental material, sj-docx-3-dhj-10.1177_20552076241277670 for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City by Peng Qingjie, Huang Wanyu, Yang Jingying, Yang Ming, Wang Linlin, Mao Qiyue, Wang Fan and Pan Minghao in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076241277670 - Supplemental material for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City
Supplemental material, sj-docx-4-dhj-10.1177_20552076241277670 for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City by Peng Qingjie, Huang Wanyu, Yang Jingying, Yang Ming, Wang Linlin, Mao Qiyue, Wang Fan and Pan Minghao in DIGITAL HEALTH
Supplemental Material
sj-jpg-5-dhj-10.1177_20552076241277670 - Supplemental material for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City
Supplemental material, sj-jpg-5-dhj-10.1177_20552076241277670 for How to promote telemedicine in underdeveloped cities in central China? Qualitative interviews with medical personnel in tertiary A-level hospital of Xinyang City by Peng Qingjie, Huang Wanyu, Yang Jingying, Yang Ming, Wang Linlin, Mao Qiyue, Wang Fan and Pan Minghao in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank the interviewees for their participation in the survey.
Availability of data and materials
Our data were collected for the research group and are not publicly available. The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Consent for publication
Not applicable in the declarations section.
Contributorship
Peng Qingjie and Huang Wanyu undertook the analyses and wrote the first drafts manuscript. Yang Jingying, Yang Ming and Wang Linlin conducted these face-to-face interviews. Pan Minghao, Wang Fan and Mao Qiyue critically reviewed the manuscript. All authors read and approved the finial manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study conforms to the principles outlined in the Declaration of Helsinki and has been approved by the Ethics Committee of Xinyang Normal University (Study ID: XFEC-2023-21). Written informed consent was obtained from all the participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Humanities and Social Sciences Project of Henan Provincial Department of Education (2023-ZZJH-057), the Soft Science Project of Xinyang (No.20230043) and the Xinyang Normal University Student Scientific Research Fund Project (No. 2023-DXS-134).
Guarantor
MP is this manuscript's guarantor.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.