
Abstract
Objectives
We live in a digital age and opportunities within healthcare are increasing, ranging from patient portals to wearable devices. Today’s undergraduates are second generation digital natives and are at a critical point of becoming more autonomous in their healthcare interactions. This study aims to understand their experiences of both digital and broader healthcare. This will enable a better understanding of implications for national policy, individual healthcare organisations and further research.
Methods
Undergraduates aged 18–21 participated in individual interviews or focus groups. Inductive thematic analysis was undertaken. Negative member checking and feedback on emerging themes from both participants and experts were used to increase the validity of the study.
Results
Twenty-four undergraduates participated in the study, including a high proportion of international students. Thematic analysis revealed 16 themes. Six key themes explored in this paper are: generation gap; impact on healthcare professionals (HCPs); use of technology to replace or enhance HCP interactions; use of technology to support administration/transactional activities; paper vs electronic; and personally held health and fitness data.
Conclusion
This paper highlights recommendations for the undergraduate cohort and wider populations including better articulation of benefits, making digital options more personalised and interactive, and raising awareness of dangerous ‘obsessive’ behaviour around health and fitness apps. Some of our findings challenge the assumption that this generation will automatically accept digital initiatives, including the importance this cohort continues to place on face-to-face interactions. In response, we offer some suggestions to improve awareness, utilisation and acceptance of digital health.
Introduction
We live in a digital age where we increasingly carry out everyday activities at our convenience online, such as banking and shopping. Interest in how this digital revolution can support healthcare is increasing globally. 1 If the current direction of developments in digital healthcare is to be a success, it needs acceptance and endorsement from the general ‘well’ public to become normalised in society. This area of research is rapidly changing and a new focus on developing areas of online activity has been identified and recommended. 2
Digital health is a broad term. For the purposes of this paper, we conceptualise this as the use of technology to either replace or enhance existing interactions within healthcare. This may include booking appointments online, patient portals, wearable devices, virtual appointments and other self-service platforms.
‘Digital native’ is one of several terms to describe a generation who have different expectations about life and learning, having grown up with access to digital technology. 3 A digital native is typically someone born after 1980, while those born after 1990 are ‘secondary digital natives’ due to their exposure to Web 2.0 while growing up. 4 It is therefore understandable to assume that undergraduates, who fit the secondary digital native profile, will be natural trailblazers and accepting of digital healthcare opportunities.
This research focused on undergraduates at a major London university. As well as being second generation digital natives, these students are also at a critical point of becoming more autonomous in their interactions with healthcare, having been removed from their existing peer groups, notably parents who remain the primary information source for healthcare. 5 This contrasts with younger adolescents who have been more studied.
Research on younger adolescents has found that healthcare needs tend to focus on appearance; mental health; sexual health; alcohol, smoking and drugs.6,7 Studies have found that perceived barriers to primary care include embarrassment, lack of confidentiality, unsympathetic doctors, and being recognised,6,8 reinforced by studies that highlight difficulties in locating confidential services. 7 This increases with particularly sensitive issues. 9 Should these barriers also exist for undergraduates, there may be an opportunity for digital technology to reduce them. This could encourage sensible use of health services earlier 6 and emphasises the importance of testing the assumption that secondary digital natives will accept and utilise digital healthcare.
In England, reflecting global trends, there is an increasing focus on the use of digital systems in healthcare including the Bob Wachter review of IT implementation in the NHS, 10 and preventative approaches are dominant in NHS policy. 11
While earlier digital health models were static and read only, Web 2.0 has created a range of digital interactions that are participatory. This could be quite basic and transactional (such as arranging an appointment or repeat prescription online) or more innovative (such as personally tracked data feeding predictive algorithms). Patients prefer functions that offer convenience, 12 and if patient-facing digital services are successful, they may help to reduce pressure on healthcare systems globally to tackle prevention and long-term condition management more effectively.
While the digital divide may be reducing, as seen in survey data from NHS Choices on online health practices (Jessica Holdstock, personal communication, 2016), if those using digital services fail to see any merit, there is a risk the anticipated benefits of digital health will not be realised. There is a need to understand what the general public want, and this study will examine this area in more detail from a global undergraduate’s perspective. This is a cohort who should be comfortable with and embrace the use of digital technology for healthcare. There is an opportunity to learn from the experiences and expectations of a group we assume are happy to ‘go digital’.
Thus, this study aims to:
explore the experiences and expectations of both digital and overall healthcare by undergraduates to understand the context in which health services are operating; understand what can be learnt from second generation digital natives that can influence the direction of national policy and future research; enable individual healthcare providers to consider what specific digital initiatives they could target at undergraduates to reduce perceived barriers to healthcare.
Aims a and b provided an insight into opportunities for the wider population; however, this was not a primary intention of the research.
Method
Design
This study used focus groups and 1:1 interviews to collect qualitative data, allowing an understanding of phenomena and lived experience to be created.
13
While focus groups consisting of friends were preferred due to the benefits of undertaking research with a group of peers,
2
they were also undertaken with groups of strangers alongside individual interviews given recruitment time constraints. Focus groups remained small (up to 4), which is appropriate for small studies,
14
while ensuring that the researcher could support participants and effectively transcribe verbatim. Each session explored the following:
participants’ previous experiences with healthcare, both generally and digitally; ranking exercise on different mechanisms (digital and non-digital) to interact with healthcare; experiences of collecting, using and sharing personally held health-related data.
Sample
Participants were aged 18–21 and were studying at University College London (UCL), the largest university in London. Snowball sampling was attempted to increase study participation, and this proved successful in constructing focus groups. Twenty-six participants were recruited and invited to attend either focus groups or interviews between March and July 2016. One participant cancelled on the day of the interview, and a second participant was excluded post interview having exceeded the upper age limit by 5 years. The study aimed to recruit a minimum of 20 participants, based on the method of Fugard & Potts 15 .
Recruitment
Students were approached through posters displayed on student noticeboards, invitations via departmental academic administrators, and advertising in UCL’s internal student newsletter. Attempts were made to advertise via social media, but this only led to some interest from other researchers, and no participants made contact this way.
Participants who contacted the researcher were emailed a copy of the information and consent sheet and asked if they were happy to participate in a focus group or interview. Those who consented were booked into a convenient time slot. All participants received a text reminder the day before their booked slot. Participants were reimbursed £10 for their time.
Setting
The research took place on the UCL Bloomsbury campus, the main university campus. Private rooms were booked ensuring privacy and furniture was laid out to avoid items such as tables acting as a barrier. Ninety minutes were allocated per session to allow time either side of the interview for paperwork and questions.
Procedure
Participants completed a ranking exercise as part of the focus groups and 1:1 interviews. They were asked to rank their preferred communication method for booking a GP appointment, receiving an appointment reminder, a GP consultation and receiving test results. Options included the use of post, emails, SMS, telephone, portals, video and in person.
The interactive exercise increased the validity of this study, enabling participants to focus on key issues despite being ‘offline’. 2 As this study asked participants to think about past experiences and what they might do in a given situation, it is difficult to know if they would actually do what they said they would do. This stimulation allowed participants to consider their options more thoughtfully.
Member checking, expert review and negative case analysis were also undertaken to increase rigour. 13 The researcher ensured all members in focus groups had the opportunity to contribute to prevent results from being skewed by dominant individuals, while remaining neutral throughout to reduce bias and not lead the participants to affirm emerging themes.2,16
Full transcripts were regularly reviewed to ensure reliability.
Supporting materials
An example schedule of questions can be found in the Appendix.
Piloting
Equipment, such as recording devices and laptops, were checked. Materials were reviewed by fellow researchers and adapted accordingly. A small pilot was undertaken using both a focus group and 1:1 interview approach. Those participating in the pilot were asked to give feedback on how they found the questions and whether they had felt pressured to answer in a particular way. Pilot participants advised they had felt open to give their views without feeling pressured. Pilot participants also flagged any questions where they struggled with the meaning.
Data from the pilot study was not used for the main study. The interview schedule and scenarios evolved slightly as a result to ensure questions were being asked clearly and enabled the aims and objectives of this study to be achieved.
Ethical issues
Ethics approval (ID: 8337/001) and data protection approval (ID: Z6364106/2016/01/89) were secured from UCL. The researcher reminded participants they did not need to volunteer any medical information they did not wish to disclose, and further information on conditions was not probed. No participants became upset or distressed during interviews; however, should this have happened they would have been referred to the UCL Support Services and the session terminated.
Participants were all issued with an information and consent form prior to participation. Participants were also given the opportunity to ask questions in person before the interview or focus group began. Personal data were only available to the direct research team for reimbursement purposes and sharing emerging results. Participants were advised that short quotes might be used to illustrate key points but that participants would remain unidentifiable. Personal data were stored on an encrypted device with the Dictaphone containing voice recordings kept securely locked away. All transcripts were anonymised. The research was compliant with the UK Data Protection Act.
Thematic analysis
Thematic analysis was used to analyse the data, 14 and the researcher opted for an analytical framework approach. This systematic method and useful structure for the data supported answering research questions while also ensuring individual views were both connected across participants and maintained within their own contexts. 17 Based on existing published guidance,14,17,18 the first author undertook the following steps: data familiarisation, generation of initial codes, development of early analytical framework, application of analytical framework, building of thematic map and definition of names, all data charted into framework matrix, interpretation of data and write up of scholarly report.
The development of the frame commenced during data collection, ensuring interview schedules could be iteratively adapted as necessary to test new emerging themes and to manage time constraints. The second author, an experienced researcher, validated emerging codes to support determining themes. 14 To develop the coding frame, an inductive approach was used. Advantages include reducing bias that pre-defined frameworks may bring 18 alongside allowing for the unexpected. 17 The inductive approach also allowed the specific research questions to evolve throughout the coding process. 14
Public, patient, clinician and expert involvement
Preliminary results were shared with both participants and experts for feedback. Transcripts were then revisited where discrepancies had been identified, to finalise the coding frame and update the discussion. Feedback was received from 6/24 participants and 2/12 approached experts after being given 9 working days to respond.
Results
Participants
Demographics of participants.

Participants were not asked about their general health, and none were known to be affected by any severe disease. One participant described their experience of living with a manageable long-term condition, and some described ongoing mental health issues. All other participants discussed short-term health issues such as stomach aches or colds.
While demographics are useful for overall context, to avoid making participants identifiable, we do not specify how many participants of which sort did or did not agree with something. Rather than representing a wider population, these data are designed to capture diversity around phenomena. 17
Coding framework
Framework of themes and codes.

Ranking activity results
Median scores.

Contextual themes
Some themes were cross cutting and contextual, supporting the whole framework. These are presented first while key themes are presented in the next section.
Barriers to technology in healthcare
Various barriers to technology in healthcare were perceived by the participants: this included the implications of running out of mobile data or losing signal and the associated cost or interruption to service, as well as issues around security and ease of use, particularly with regard to passwords, set up and multiple log-ins.
Choice
Closely linked to convenience (below), choice was also frequently mentioned. The type and severity/urgency of the health condition were often a big influence on how participants would want to interact with healthcare (digitally or otherwise). A desire to have options was articulated. Another key sub-theme within choice was the ability to ask questions and request further information as part of a two-way conversation, where this was warranted depending on the health condition itself.
Communication methods
Digital communication methods were preferred for more transactional activities; however face to face was preferred by an overwhelming majority when it came to a GP consultation. The participants generally did not seem to trust postal services, which were seen as slow and unreliable. While telephone calls were also not favoured (or used as a communication method in general for this cohort), they were recognised as useful for asking questions.
Convenience
All participants spoke about the importance of convenience to them when making their decisions, taking into consideration factors such as cost, time, balancing other commitments, having to queue, and hours that suited them. Participants spoke of busy lifestyles and a desire to carry out transactions whenever and wherever they wanted to.
Healthcare experiences
All participants were able to relate to previous healthcare experiences of either themselves or a family member. Most personal experiences were related to short-term isolated illnesses. This was a generally well cohort.
Healthcare expectations
While participants tended to talk about negative experiences more than positive ones, many were aware of the problems facing the NHS in England such as not enough doctors and limited flexibility. Participants generally spoke about not wanting to go to the GP unnecessarily. International students sometimes referred to the culture back home where it was not routine to go to a doctor unless you were very sick.
Expectations of HCPs
Some participants spoke about trying home remedies or searching for information because they did not feel they would be able to see a doctor quickly enough, but they still valued the opinion of a healthcare professional just in case.
Information sharing within healthcare
Some participants identified that information sharing within the NHS between individual organisations was not currently the norm, either through personal experiences or through placement work in a healthcare setting.
Motivations to use new technology
Some participants spoke about needing to know there would be benefits to using a new technology such as it being more convenient or offering reassurance to them. Participants also spoke of peer usage and competitiveness as being two reasons why they might take up a new technology.
Key themes
Use of technology to support administration/transactional activities
Participants favoured digital technology to support booking appointments and receiving appointment reminders, especially if they could carry out the activities at their own convenience on personal devices. The use of technology to support test results was a bit more complex. While digital technology was favoured, a combination of notifications and then the ability to download results from a portal seemed to be preferred. This offered the convenience of being able to retrieve results at a convenient time as soon as they were ready, rather than wasting time chasing up their results. Participants raised concerns however as to how rich the information would be and how they could ask questions. Participants were positive but stressed the importance of public facing systems needing to be slick, reliable and to contain the right level of information or facilitate reliable signposting.
Use of technology to replace/enhance HCP interactions
Participants were overwhelmingly opposed to the idea of using technology to replace their face-to-face interactions. Video conferencing was unpopular due to the feeling that they would not be appropriately assessed or that the doctor might be distracted by other things during the virtual consultation. Participants were potentially open to virtual consultations for a longer term ongoing problem, but few had experience of such a condition. Concerns were also raised with internet connectivity and mobile data allowances as a challenge. Virtual consultations were most popular when considered as an option for international students to communicate with their family doctors back home.
Paper vs electronic
Despite being second generation digital natives, this group still tended to see paper as being more official or real, while a couple of participants referred to both physical and electronic formats as being equally ‘permanent’. Concerns were often raised such as information getting lost in cyberspace, difficulty annotating, systems crashing and just generally preferring paper. One participant questioned the legitimacy of receiving something online compared with knowing it had come from their doctor. However, many of the group also indicated they were simply not used to getting information in a more digital format and therefore it may require a change in mind-set. Participants generally appeared open-minded about how they could receive their information in the future.
Generation gap
Many participants identified that they were part of a new generation who were more digitally enabled and therefore more receptive to change. Some raised concerns about how older generations would accept increasing use of technology, especially if they did not have family around to help them. This re-enforced the importance of choice, in that it was felt that older generations should be able to continue booking their appointments over the phone if they wish to do so. They did however recognise that age was not necessarily a hindrance and there were benefits to the use of technology to help with a variety of things including applications to support medication reminders. A large concern was data security and trusting of online information by older generations in their families, concerns in fact shared by many of the participants who highlighted a preference for paper. Several referred to the refusal of such family members to join online banking for that very reason. Another concern was around the use of passwords and log-ins, with several participants pointing out that they too struggled to keep up with this alongside older generations.
Personally held health and fitness data
Participants had mixed experiences of personally held health and fitness data. Many had tried various apps but had found either the novelty had worn off or it was too much effort to keep up to date with inputting data. With regard to fitness or calorie tracking, participants recognised the advantage as being able to reach a goal, either through a specific fitness task (such as running a marathon) or weight loss. The majority of participants however raised concerns about the obsessiveness and dangers of such apps, either through personal experience or behaviours of their peers. Some participants mentioned apps beyond fitness, such as tracking menstrual cycles or sleep. One participant suggested that they would find it useful to have the ability to test their own blood and check for any deficiencies.
Participants advised they generally did not share their health or fitness data with their peers. The use of ‘social filters’ was frequently mentioned whereby if they did share information they would only share positive things. Most participants were open to sharing these data with an HCP should they be asked or if it supported some of their symptoms; however, it was unlikely they would volunteer the information to their HCP automatically.
Impact on HCPs
Some participants recognised the impact digital technology may have on HCPs. This was largely seen as beneficial; however, concerns were raised about doctors becoming overwhelmed with email traffic. The group generally felt that the impact on HCPs would be positive.
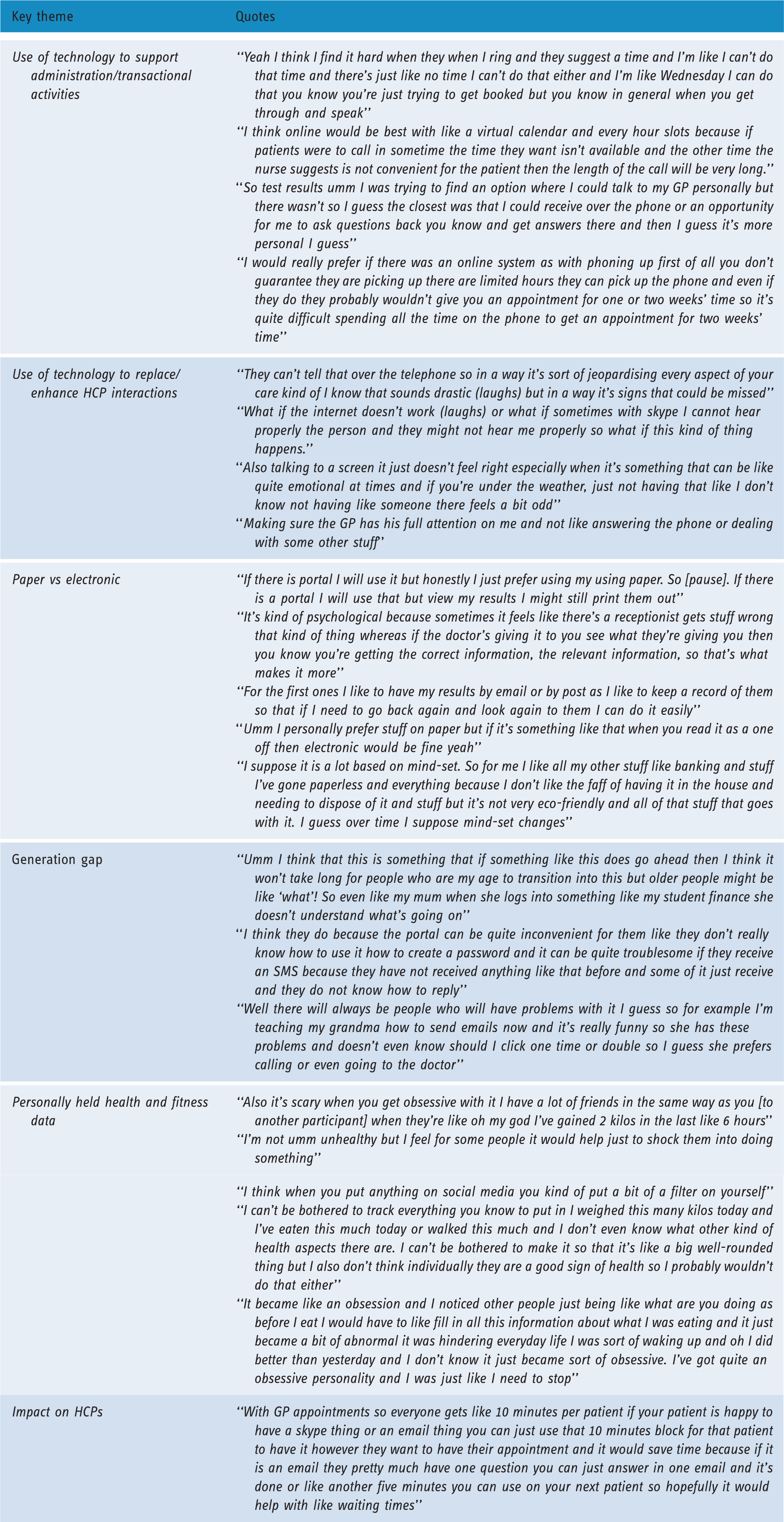
Key theme quotations.
Information searching
Two final themes emerged around information searching. Participants had varied reasons to search for information online. They seemed to have high critical awareness when it came to using online sources and treated them with caution depending on factors such as source, branding and extreme opinions.
Feedback from participants and researchers
Preliminary themes were shared with both experts and the original participants of the study for feedback to increase validity of the coding frame. Participants also confirmed they did not feel led and had been able to express their own opinions. Ambiguity over some of the terms used was flagged, for example virtual consultations could be segregated into video calls, webchats and the use of WhatsApp.
Discussion
The aims of this research will each be explored in turn.
Aim 1: Explore the experiences and expectations of both digital and overall healthcare by undergraduates to understand the context in which health services are operating
Recruiting via a university allowed a range of international views to be captured, representative of a modern, global society and with participants each bringing experiences of different cultural expectations and healthcare systems. Provision of healthcare to undergraduates must recognise and cater for a variety of expectations.
Participants could easily reflect on general experiences of healthcare; however, they were not always able to speak about experiences of digital healthcare. Although they could easily articulate the use of digital technology in other areas (e.g. banking), they struggled to do the same for healthcare and indeed many participants were unaware of what was already possible (an example being the use of the Summary Care Record in the UK to identify drug allergies). They had generally not experienced the same frustrations as more frequent healthcare users, such as complications of data sharing between providers, although some expressed dissatisfaction with the GP registration process, which they considered cumbersome.
Aim 2: Understand what can be learnt from second generation digital natives that can influence the direction of national policy and future research
Many of the viewpoints expressed aligned with literature on digital natives 3 . They are a cohort with a perceived busy and stressful lifestyle, often trying to balance lectures, part-time jobs and a busy social life. Services must be convenient, reliable and slick, otherwise they will not be adopted. Choice between options is also necessary, depending on severity of the condition, as well as opportunities to seek clarification instantly where necessary. This becomes very subjective and it is questionable whether many current healthcare models can cope with supporting such demands in their current configurations.
There were however some surprising findings in our results that challenge assumptions often made that digital natives will be automatically accepting of digital healthcare. Firstly, participants’ resistance to using virtual means to interact with healthcare professionals: the value of face to face interaction was more important than saving time and cost on travel, for example. Secondly, we note their perception of how paper documents can seem more real and important.
Finally, health and fitness tracking were not met with great enthusiasm. While the quantified self-movement is growing, 19 including the quantification of physical activity 20 and sleep, 21 the success of such apps and devices remains quite limited. 21 The attitudes of our participants mirror previous research in which tracking tended to be useful only if it was being used for action, goals or sense-making. 22 Previous research on wearables to support healthcare have suggested younger generations are more likely to be comfortable using such devices due to their more open attitudes. 19 However, the participants’ experiences in this study were short lived and they were seen as too much hassle. This is unsurprising when other studies have found even patients with long-term conditions may see the tracking of data as ‘work’. 22 Overall, this cohort therefore did not feel the value outweighed the effort required of them.
It would be wrong to assume this cohort will be completely accepting of digital healthcare. That they appear to have more faith in face-to-face appointments and paper documents flies in the face of much national policy. However, we note that, in the UK context, there is considerable ongoing work promoting the sharing of relevant and useful healthcare information. It is likely this cohort have not experienced much of that as yet. Further, nearly all experiences the participants discussed were isolated episodes of ill health. The management of chronic long-term conditions is radically different.
Several studies have flagged issues with technical, logistical and regulatory challenges around new models of care for GP consultations. This includes email, 23 virtual online consultations 24 and text messaging. 25 The overall consensus was that some mechanisms may work for particular patients or patient groups. For this group, activities that can be carried out through existing university portals may prove most successful, compared with new initiatives that may be perceived as risky or hard work.
Although the participants have been more dismissive of using technology than expected, they appeared open-minded and recognised mind-set changes were required, similar to how people have accepted online banking, for example. The issues raised were not unique to this age group, including concerns around cyber security and a reluctance to move away from paper.
Likewise, it could be argued they were more likely to recognise dangers around obsessiveness with data tracking. These dangers are already evident in the literature: with non-medical devices communicating assumptions on what is healthy, 21 unhealthy obsessions with data such as ‘chronorexia’, an unhealthy obsession with ‘healthy sleeping’, 21 and the risk of wrongly assuming a device is completely accurate. 20
Finally, participants indicated they would probably not share their own data with an HCP, which either indicates a lack of faith in data rigour or a fear in challenging the patient–doctor relationship. This mirrors previous studies where few patients considered their data as something useful to an HCP. 22 Other issues include that the number of false positives may impact on healthcare professionals’ workload unnecessarily 21 and a current lack of engagement by providers, due to a variety of reasons including a lack of usable export mechanisms. 20 Such data tracking may therefore reinforce bad activities or behaviours without the ability to obtain a HCP’s expert opinion on the data.
Aim 3: Enable individual healthcare providers to consider what specific digital initiatives they could target at undergraduates to reduce perceived barriers to healthcare
A key barrier to healthcare for this cohort was getting a GP appointment. Participants lacked patience and would instead attend as a walk in; if they were sick, they wanted to be seen immediately and this appeared to be more important during stressful times such as examination periods. Thus, while the technology may support administrative functions, it is unlikely to support their underlying goal of seeing the GP quicker if the same appointments are offered. The opportunity to see a doctor quicker through virtual means is less relevant given the preference for face-to-face consultations.
Participants often spoke of visiting their GP with conditions that could be treated through self-care and over-the-counter medications. Despite showing high levels of scrutiny towards online information, they continued to feel the need for a GP to rule out anything more sinister. This presents a second barrier whereby participants struggled to make sense of the overwhelming amount of information available to them and potentially led to avoidable appointments being made. There is an opportunity to target undergraduates with more communication direct from the GP practice so they feel the information is relevant to them, such as assistance with processes like registration or health campaigns. This could include better signposting to trustworthy information sources.
Several participants raised the point that some initiatives such as video calls or portals may be more useful in managing a long-term condition; they just could not relate them to their personal experiences. There are opportunities within many healthcare organisations to explore what this means for their patients.
Limitations
Although this study was able to address the aims laid out, a number of limitations are recognised. Given constraints, pragmatic mitigation actions were undertaken where possible.
Digital natives
While this paper did not set out to prove or disprove the concept of a digital native, the researcher may have recruited those keener on digital technology than the average undergraduate. This is because the majority of participants were recruited via email or electronic newsletter and the advert asked for people who undertake other digital transactions such as online banking to get their attention. It may have excluded undergraduates less keen on using digital in general.
Validity
Many activities discussed were things participants had no experience of, such as booking appointments online. It is therefore difficult to know if what participants say they will do is what they would actually do. This limitation was identified at the start of the project and the ranking exercised was used as a mitigation, aimed to give participants some headspace to consider their options against one another. The use of participant and expert feedback also mitigated the impact of this.
Ranking exercise choices
While useful to focus participants, some of the choices that had been grouped in the activity were interpreted differently by participants. It is also unclear if participants felt they could offer alternative options despite being invited to.
Interviewer bias
The researcher introducing themselves as working for the NHS may have led to participants being more positive, trying to please the researcher.
Sample bias
The majority of participants in this study were female (20/24) and international students (17/24); 13/17 had moved to the UK for undergraduate studies and 4/17 had completed secondary education in the UK prior to undergraduate studies. This may have led to a sample bias.
Implications
This was a modest study conducted at one site. Results are largely concordant with the existing literature, but a larger evidence base is needed before firm recommendations can be made, and we must exercise caution before making assumptions around digital natives. If further work replicates these findings, however, we suggest the following recommendations:
Transactional basic ‘self-service’ activities should continue to be developed, with the benefits better articulated to patients so they are aware of and can take advantage of their options. Patient-facing digital health should be compatible with smartphones and involve simple yet secure sign-up processes. Health economies (both globally and locally) should be cautious not to invest in ‘solutions’ that will not be used by patients; the target patient group should be considered carefully when making such decisions. Healthcare providers and universities should collaborate to consider how existing student portals can be best utilised. Digitisation will work best with undergraduates when they can access additional content or resources when desired: a patient receiving test results electronically, for example, must be signposted to further information or a mechanism to ask questions and obtain answers within a sensible timeframe. Campaigns and information should be delivered to this cohort in a format that is useful for them. Studies have shown the benefit of using social media to target such groups, and universities should consider more effective campaigns relating to healthcare.
26
Healthcare systems should undertake further work with second generation digital natives to help break down barriers in digital healthcare. This group can provide a valuable bridge across generations given their greater experience of digital services generally. Considering healthcare beyond undergraduates, our findings support the view that increased regulation is required to protect both patients and HCPs when using more innovative methods to communicate. In addition, healthcare providers need to carefully consider to whom they offer such services. Patients not wanting to communicate electronically with their HCPs have been evident in other studies,
27
and we must ensure, as new initiatives are rolled out, they are what patients want. Further research is recommended given many participants highlighted a trend around obsessiveness with personal health and data tracking, to understand whether such applications are increasing eating disorders or other anxieties around ‘the quantified self’. This is evident throughout undergraduates and their peer groups. Universities should be aware of this and be prepared to educate their students of the potential dangers.
Conclusion
This paper highlights an opportunity for healthcare systems globally to reach out more effectively to undergraduates. More collaborative work needs to be done to understand why they are not convinced of the benefits and to break down barriers to use. This study highlights how implementing technology alone is not the default answer if the advantages are not obvious, even to our digital natives. If we fail to do this, we risk switching on more digital solutions that fail to deliver benefits to patients, clinicians or healthcare systems.
Footnotes
Acknowledgements
We would like to thank the following for their assistance and guidance throughout this research: Chris Howroyd, Katie Benjamin, Matt Stibbs and Pippa Bark-Williams. We would like to thank the following colleagues of the main author (AC) who gave their support during the time this research project ran: Lisa Alderton, Lois Lere and Nicola Costin-Davis. We would also like to thank the following family members of the main author (AC) for their support and encouragement throughout the study period: Robert Cowey, Alice Cowey, Ian Greensmith, Smita Greensmith and Anthony Greensmith.
Contributorship
AC led all parts of this research project. HP contributed in the following areas: design of the study, gaining ethical approval, reviewing and editing the manuscript, approved final version of the manuscript.
Data sharing
Permissions do not exist to allow the sharing of the raw qualitative data.
Declaration of conflicting interests
AC was an employee of NHS England at the time the original research was carried out. HP is an employee of UCL. He has received consultancy fees from Crystallise and The HELP Trust, and funding from myownteam and Shift.ms.
Ethical approval
Approval was secured from the UCL Research Ethics Committee (ID: 8337/001) as was UCL Data Protection approval (ID: Z6364106/2016/01/89).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The research led to receipt of a £1,000 dissertation prize from Cerner, awarded after completion of the research. Cerner had no input into the writing or submission of the paper.
Guarantor
HP.
Peer review
This manuscript was reviewed by Francesco Pinciroli, Politecnico Milano, Italy, and one other individual who has chosen to remain anonymous.