
Abstract
Objective
The main objective of this study is to develop an eHealth adoption model based on patients’ perceptions of public value dimensions and empirically apply the model to understand the adoption of a governmental health app by Jordanian patients. The study attempts to contribute to overcoming the narrow focus of contemporary theories such as UTAUT and, ultimately, to designing more effective implementation strategies in order to address the current delays in global eHealth adoption.
Methods
We conducted a quantitative survey of 430 Jordanian patients, utilizing structural equation modeling (SEM) to process the empirical data. Specifically, we applied an SEM two-step approach that involved (a) evaluating the model-data fit through a review of the measurement model(s) and common method bias; and (b) analyzing the structural model.
Results
Our findings confirm that the proposed patients’ value scale is valid and reliable. Its five dimensions (hedonistic motivation, utilitarian motivation, social value, ethical public value, and public trust value) significantly correlate with patients’ public value, and the latter directly affects their use of eHealth apps, with habits mediating this relationship. Among the dimensions, hedonistic motivations tend to be prioritized over utilitarian ones. Ethical and trust values also play an essential role, particularly in how health technology handles patients’ data and upholds their dignity and self-esteem.
Conclusions
This study highlights the holistic nature of eHealth adoption by patients and the crucial role of public values in their use behavior. It provides useful insights for policymakers and developers.
Introduction
In the last decades, significant technological advancements have dramatically impacted several aspects of our professional and personal lives. The present era is distinguished by an unprecedented surge in the digital revolution, which revolves around utilizing technology to significantly augment the reach and efficiency of businesses and governmental entities. The healthcare industry has been particularly affected by this wave of technological innovation, 1 giving rise to electronic health. 2 eHealth technologies are a broad category of innovations that facilitate delivering medical services through web-based or mobile applications. These innovations include various technologies such as mHealth apps, web-based eHealth services, health clouds, intelligent clothing systems, electronic medical record (EMR) applications, and computerized physician/provider order entry (CPOE). 3
The fusion of eHealth and new information technologies like AI, cloud computing, the Internet of Things (IoT), and wearable devices, on the other hand, has been a watershed event in healthcare, highlighting its critical importance in our ever-evolving world. 4 EHealth has become an essential component of the healthcare system due to its ability to handle various challenges in medicine, such as lowering the rate of medical errors and increasing the effectiveness and efficiency of service delivery. For instance, using electronic medical records, in which a patient's medical history is recorded, helps avoid mistakes in their treatment, such as giving them the wrong drug. 5
Despite the numerous advantages that eHealth applications offer, there is a certain degree of reluctance among patients to accept them for medical treatments via eHealth platforms. As emphasized by Bullock and his colleagues, the global adoption of eHealth applications is currently experiencing a delay. 6 Kim and his colleagues have furthered this argument, positing that a low adoption rate may suggest that optimal strategies still need to be identified to implement telemedicine applications effectively. 7
The above does not seem unrelated to the fact that current theories in the field of eHealth interventions (like the Technology Acceptance Model and Unified Theory of Acceptance and Use of Technology) tend to focus heavily on individual factors while neglecting contextual and situational factors. 8 While individual determinants are important, it is equally crucial to address interpersonal, community, and societal-level factors to effectively promote eHealth adoption. Public value, as defined by Meynhardt's approach, provides a balanced viewpoint between individual and social levels in the adoption of eHealth. It emphasizes the relationships between the individual and society, taking into account individual evaluations of basic needs, emotional-motivational states, and personal experiences. 9 When patients collectively adopt and share similar evaluations, a value becomes “objective,” although it remains subject to change and continuous revision in discursive practices and communication. Therefore, this perspective allows for the integration of both micro- and macro-levels of adoption in eHealth initiatives9–11 Along these lines, the recent study by Gerli et al. highlights the importance of public value in evaluating eHealth services in e-government. 12 Another shortcoming of the eHealth literature is the need to incorporate more theoretical perspectives that can accurately depict the interconnected features required for establishing enduring changes. 13 As a result, it is essential to recognize that emerging technologies like eHealth are multifaceted in users’ minds regarding their usage.14,15 To adequately address this complexity from a public value perspective, the aforementioned contribution by Gerli et al. needs to be complemented by further examination to fully comprehend, in healthcare delivery, the intricate relationships between the various dimensions of public value, ensuring that eHealth apps benefit the public while protecting individual users and marginalized groups. 12
At the theoretical level, we integrate elements from the Unified Theory of Acceptance and Use of Technology (UTAUT) with others from the Public Value Theory (PVT) in a patients’ public value model of eHealth adoption. Within Public Value Theory (PVT), we mainly rely on the Meynhardt's psychological framework, which offers a solid theoretical foundation for evaluating eHealth applications from a patient-centric perspective16,17 (unlike Moore and Bozeman, Meynhardt links public value to fundamental human needs18–21). Our model adopts a notion of public value that extend the Meynhardt and Jasinenko's one by adding patient trust values. 22 In the model, the stimuli associated with eHealth features and benefits affect patients’ public value through its several dimensions and ultimately trigger the response of those patients in terms of habit formation and adoption of the eHealth application. The consideration of the habit as a potential mediator in the association between patients’ public value and their adoption of eHealth is also one of the novelties of our model.
At the empirical level, we take the Jordanian healthcare system as a setting and analyze how its patients’ public value dimensions affect adopting the MyHakeem application. Our critical empirical inquiry is, therefore, what factors influence the adoption of eHealth technology among Jordanian patients based on their value model? To further investigate, we have formulated two sub-questions: (a) To what extent does the patients’ value model predict the actual usage of eHealth technology among Jordanian patients? and (b) To what extent do the stimulus factors inherent in an eHealth app influence patients’ public value when using eHealth technology? In order to answer these questions, we conducted a quantitative survey of 430 Jordanian patients and utilized structural equation modeling (SEM) to analyze the empirical data. Specifically, we applied a structural equation modeling two-step approach that involved (a) evaluating the model-data fit through a review of the measurement model(s) and (b) analyzing the structural model, as described by Vehkalahti. 23 The measurement model(s) were reviewed to determine the extent of their fit with the data, which was found to be satisfactory.
The current paper starts by critically reviewing earlier academic studies regarding eHealth adoption and then—to gain insights to overcome their inadequacies—turns to the contextual background of the notion of eHealth public value. The subsequent part summarizes the conceptual model, the generation of hypotheses, and the investigative techniques utilized in this research. After this, the data analysis and the research outcomes are displayed and scrutinized. In conclusion, this study presents the implications and limits of the findings and suggests further research.
Literature review
Ehealth technology acceptance models and their inadequacies
Several theories have been proposed to evaluate how effectively potential customers accept technology-driven platforms, including the Technology Acceptance Model (TAM), the Theory of Reasoned Action (TRA), the Theory of Planned Behavior (TPB), and the Diffusion of Innovation Theory. 24 In addition, the Unified Theory of Acceptance and Use of Technology (UTAUT) model, which synthesizes the critical components of eight prominent models, 25 has been widely used to explain technology adoption and its implications in various fields, 26 especially in eHealth applications. 27 The Unified Theory of Acceptance and Use of Technology model is the most frequently used framework for examining eHealth adoption,13,28 particularly in developing countries. 29
In this context, Arfi et al. present a review of research works that implemented the UTAUT theoretical frameworks for analyzing technology adoption in the healthcare and eHealth domains. 30 The study revealed that researchers had explored various factors influencing behavioral intention in healthcare, besides the original Unified Theory of Acceptance and Use of Technology variables such as performance expectancy, social influence, effort expectancy, and facilitating conditions. 30 Additionally, Kalayou's study demonstrated that the TAM can be effectively used to assess behavioral intention to use eHealth for the sustainable adoption of eHealth technologies. 31
In contrast, understanding why people adopt an information system can be explained by the user's personality traits rather than the technology itself. 32 One important factor in technology acceptance is self-efficacy, including computer self-efficacy. 33 Additionally, a high level of facilitating conditions can support technology adoption.31,34 Other researchers have studied how personal innovativeness and behavioral intention (BI) are related35,36 and how psychological factors can predict behavioral intention.37–39 Furthermore, challenges related to the adoption of digital technology in healthcare, such as perceived security, privacy threats, and information security, have been investigated by researchers like Arfi et al. 30
However, the Technology Acceptance Model and Unified Theory of Acceptance and Use of Technology have faced criticism for oversimplifying and focusing solely on individual adopters’ perceptions and intentions to adopt technology. 40 Critics argue that these models lack robust heuristic value, have limited descriptive and predictive capabilities, and lack practical value. 41 Furthermore, they have diverted researchers’ attention from other important research topics, creating the illusion of progress in knowledge accumulation.41,42 Several researchers have sought to expand these models to adapt to the constantly evolving information technology landscape, leading to theoretical confusion and uncertainty.43,44 Additionally, these models have been criticized for the gap between intention and behavior, which has been acknowledged, and the empirical support for the relationship between intention and behavior has not always been consistent in previous literature. 45 In the context of eHealth technology, a limitation of these models is that they assume a single user is associated with a particular set of eHealth requirements, neglecting the diversity of users and tasks involved in healthcare delivery. 46 Consequently, adoption models are needed to reconcile the needs and perceptions of multiple users.40,46 Based on the flaws found in the models of technology adoption (particularly eHealth) discussed previously, Syamsudin et al. note that UTAUT's model extensions are needed to apply the theory in non-commercial settings, such as public eHealth. 47
As stated in the Introduction, patients’ reluctance towards eHealth Care and the current delay in its global adoption may have to do with the lack of optimal implementation strategies, and this shortcoming seems to be partly attributable to the current theories’ focus on individual readiness to accept health technologies. It is, therefore, necessary to strengthen the presence of theoretical perspectives in the eHealth literature that grasp the complex interplay of connections and structures involved in implementing sustainable change. In light of this increasingly recognized complexity of eHealth implementation, it is recommended that forthcoming research endeavors focus on obtaining models that accommodate eHealth apps’ multidimensional, active, and interdependent nature. 13
Public value theory and its potential usefulness in explaining ehealth adoption
To overcome the Unified Theory of Acceptance and Use of Technology inadequacies, we took insights from the public value literature, which is highly significant in the continued development of research in public administration. 48 Two main traditions of thought can be distinguished in this literature. 49 The first and oldest comes from the field of administrative ethics, and has to do with the values that express the normativity inherent in public administration (“public values”). Works such as those of Frederickson or Van Wart are good exponents of this tradition, whose most outstanding current figure is perhaps Barry Bozeman. Without renouncing the markedly conceptual and normative nature of such discourse on public values, this author promotes a renewed perspective that seeks to build bridges between the theoretical and empirical planes.50,51 At the former plane, Bryson et al. suggest that in any society, there are commonly held values that determine the entitlements and privileges that citizens should have, as well as their responsibilities toward society, government, and each other. 52 These values also shape the fundamental ideas that should guide governments and policies. Bozeman's research is considered normative because he examines situations where society, market processes, or government fall short of delivering the ideal types of public value. 53
The second tradition of thought identified by Jorgensen and Rutgers is that of public value management, which was born in 1995 with the publication of the book “Creating Public Value” by Mark H. Moore.49,54 He defines “public value” as a framework that enables public managers to align their perception of value with the allocation of public resources, while also enhancing their understanding of what their “publics” value and how interacting with these. 54 Unlike Bozeman's research and the subsequent literature it influenced, the contribution of Mark H. Moore centers on taking action. 53 Moore has a keen interest in public management. In its first form, the notion of public value was analogous to shareholder value in public management. The concern is in the decline in the value of government and public managers in today’s epoch of economic individualism and market dominance. He seeks persuasive rhetoric and a systematic approach to finding, advocating for, and achieving public good. In his early work, his perspective on public value generation is narrower compared to the subsequent literature, which tends to be less manager-centric and more aware of the problematic nature of the relationship between managerial empowerment and democratic concerns. 52
Working from this second tradition, Meynhardt adopts its vision of public value as arisen from an evaluative judgment on what is or is not valuable to society. 17 However, he relocates such judgment between the individual needs and his/her perceptions of value for the public, which are shaped by the dynamics of the individual's relationships with other people as well as the object under evaluation. 55 On the one hand, individuals’ basic needs structure their public value evaluation. 17 On the other hand, their perceived value for the public is functionally important to fulfilling their needs. 56 The latter are organized into four categories, which are translated into four public value measurements: moral-ethical, hedonistic-aesthetical, utilitarian-instrumental, and political-social. 17 Meynhardt’s connection between fundamental human wants and the societal value generated renders his Public Value Theory a valuable study tool for assessing the interplay between individual experiences at the micro level and broader social consequences at the macro level. 9 Moreover, such connection contributes to making the theoretical construct more subjective and less prescriptive, as public value becomes determined by subjective assessments of fundamental needs and experiences via emotional-motivational moods and activities. 57
The public value theory presents a useful framework for comprehending the adoption of eHealth by emphasizing the collective benefits and societal goals of eHealth initiatives. 58 In contrast to individual theories such as the Unified Theory of Acceptance and Use of Technology, which focus on personal factors influencing adoption, 59 public value theory considers the broader context, including the social, organizational, and public dimensions that influence the effectiveness of eHealth solutions. 12
One of the key strengths of public value theory is its ability to encompass the multifaceted nature of value creation in public services. 60 In the context of eHealth, this includes not only improving individual health outcomes but also enhancing community health, reducing healthcare disparities, and increasing access to healthcare services. By focusing on these collective benefits, public value theory provides a comprehensive perspective for evaluating the impact of eHealth initiatives on public health. 12
Moreover, public value theory emphasizes the importance of social fairness, trust, and legitimacy in the adoption of new technologies. 61 For eHealth initiatives to gain widespread acceptance, they must be perceived as trustworthy and legitimate by the public. 62 Public value theory offers insights into how to establish and maintain this trust, emphasizing transparency, accountability, and responsiveness in the development and deployment of eHealth solutions. 63
As evaluative framework, public value has been utilized in examining eHealth services, which are government services that utilize information technology to provide healthcare information and services to people. 12 In Bend's study, the public value of eHealth applications was evaluated by considering their effectiveness in achieving intended objectives and the confidence established between individuals and healthcare practitioners. 64 In a comprehensive study, Svejvig et al. analyzed the impact of eHealth on patients’ and workers’ perceptions of healthcare service quality. 65 Gerli et al. suggest that privacy, security, accountability, and public value are essential when assessing eHealth services. 12 In 2016, Scott et al. conducted a study on the public value-based construct with a specific focus on assessing the success of e-government information systems. They discovered that this construct comprises nine factors: Expense, Time, Comfort, Personalization, Communication, Ease of Information Retrieval, Trust, Well-Informedness, and Participation in Decision-Making. These factors help clarify a significant part of the public's perception of e-government success. 66
Building on the previous contributions, Gerli et al. performed a study on the acceptance of eHealth and analyzed its public value aspects using three conceptual frameworks: Jørgensen & Bozeman, Twizeyimana & Andersson, and Scott et al.12,66–68 They combined the values of the public administration-citizen relationship with three key dimensions identified by Twizeyimana and Andersson and used the outcomes and indicators from Scott et al. and Twizeyimana and Andersson, to measure e-government services.66–68 Their study showed how various indicators, each representing a distinct aspect of public value, contribute to enhancing public value through strengthening governance, public services, or societal well-being. Their methodology categorized public value components into three groups: programs distributed through digital devices, acquisition and utilization of personal data, and adherence to open-source principles. The study concluded that the public value theory is a robust theoretical model for analyzing e-services, emphasizing the intricate connections between various elements of public value in healthcare provision.
Theoretical framework and hypothesis development
Integrating UTAUT and public value theory in a patients’ value model
In the last section, we argued that EHealth Technology Acceptance Models suffer from substantial limitations and that Public Value Theory (PVT) can be useful in explaining eHealth adoption. We now integrate elements of UTAUT with others from PVT in a patients’ public value model. We first briefly establish the rationale for this integration and then formulate the model, whose constituent constructs are addressed in successive subsections.
Leaving aside moderating variables such as age, gender, etc., UTAUT models are basically structured in three layers: a set of factors that foster or inhibit technology adoption, a synthetic psychological construct reflecting these factors, and a behavioral variable of technology adoption. Our model conceptualizes and operationalizes the technology adoption variable in UTAUT terms, and maintains this three-layer structure but introduces three fundamental changes. First, from the set of factors in the first layer of the UTAUT models, we retain only those relevant to our purpose (understanding the adoption of a government health app) and subsume them into a more comprehensive set that is mostly drawn from public value theory. Second, the habit factor of the UTAUT 2 models is not subsumed in such a comprehensive set but plays a mediating role in our model. Third, the synthetic psychological construct that bridges the factors with technology adoption is not, in our model, a mediator variable (behavioral intention) but a second-order construct (patients’ public value).
Regarding the former, the original UTAUT identified four factors: performance expectancy, effort expectancy, social influence, and facilitating conditions. 25 UTAUT 2 added to them hedonic motivation, price value, and habit. 69 In our model, performance expectancy and effort expectancy are subsumed into the construct of utilitarian motivation (common to technology adoption research and Public Value Theory), whereas hedonic motivation appears as hedonistic motivation and social influence becomes a component of the social value dimension. To these three Meynhardt and Jasinenko's dimensions, they add a fourth of ethical public value that is also hosted by our model. 17 And, aiming for even greater comprehensiveness, we extended Meynhardt and Jasinenko's framework with the incorporation of Epstein's “trust” construct.22,70 Moreover, given our focus on a free government application, it would not make sense to include price value as a factor either. What is included, instead, is habit, but as a mediating variable, as we pointed out in the previous paragraph. In the following subsections, the rationale behind each of the factors included in the model is discussed in more detail.
Regarding the substitution of behavioral intention for patients’ public value as a synthesis construct or second-order latent variable, this is justified for two fundamental reasons. Firstly, the suitability of Public Value Theory as a comprehensive umbrella for the set of factors considered as first-order latent variables. Secondly, many researchers have highlighted the limited impact of behavioral intention on behavior, known as the behavior-intention gap.71–74 Figure 1 displays the model that we adopt to examine the relationships between patients’ public value, their habits, and their utilization of eHealth applications. Furthermore, it is vital to consider Appendix A in the online supplemental materials in this context.
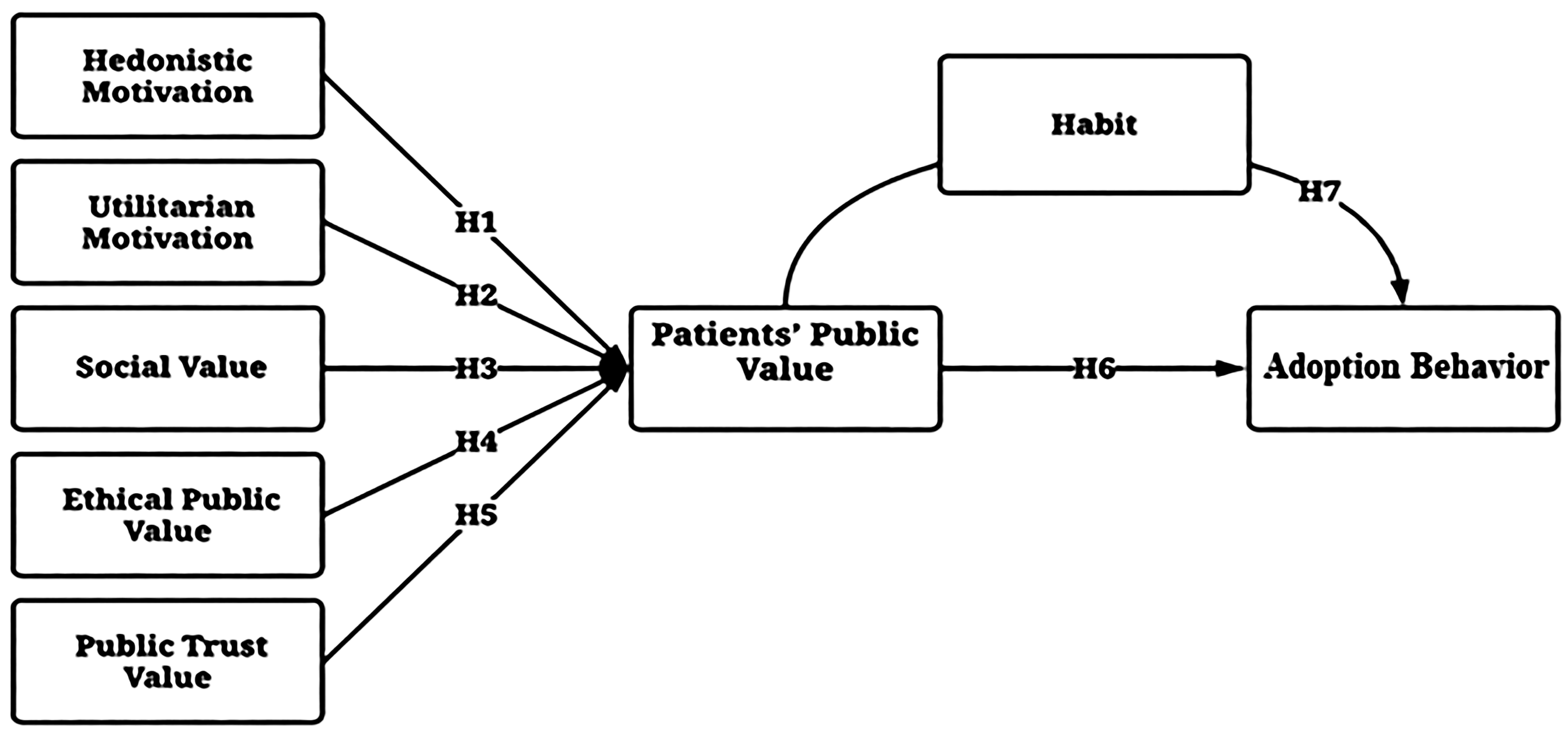
The study model “patients’ value model” (PVM).
Hedonistic motivation
As per classical Freudian theory, the pursuit of pleasure and avoidance of pain, known as the pleasure principle, was considered the most fundamental need. However, this view was updated with the introduction of the death instinct. The cognitive-experiential self-theory (CEST) recently added a new basic need to their perspective on fundamental needs. This new need is to behave by the hedonic principle, which means seeking positive emotions and avoiding negative ones. 22 According to Meynhardt and Jasinenko, hedonistic motivation is the value placed on pleasure and the desire to create positive experiences. In IS research, hedonic motivation refers to an individual's intrinsic motivation to obtain pleasure from using technology. 75 It is commonly measured as perceived enjoyment. 76 Consequently, it stems from the profoundly ingrained evolutionary desire to minimize pain and increase pleasure to survive.
In the context of eHealth, hedonic motivation is essential to eHealth consumers, and it could even be a sufficient reason for adoption. 75 Additionally, hedonic value is non-instrumental but experiential and affective. Customers experience hedonic value when utilizing (IS) is valued for its own sake, apart from its utilitarian value. Empirical research on information systems has demonstrated that users’ perception of hedonic value is essential in the context of IS use, particularly in eHealth.77,78 In addition, Talukder et al. discovered that hedonic motivation was the driving force behind users’ positive perceptions of healthcare IT and services. 79
In light of this context, the present study aligns with Meynhardt's perspective on the values and needs of individuals. In the words of Meynhardt, evaluation is inherently intertwined with basic human needs. Needs refer to the perceived insufficiencies or deficiencies in an individual's psychological state, wherein an apparent disparity exists between the current and desired states. 11 These disparities subsequently generate a motivational response, prompting the individual to engage in actions to address and fulfill these needs. Needs play a crucial role as actual or hypothetical standards for assessment; they serve as the essence of the “ought.”
Consequently, the assessment of individuals’ values is shaped by the satisfaction of their fundamental needs, whether explicitly or implicitly. If patients find that using an eHealth application contributes to their subjective need fulfillment, they will likely view it favorably. However, if their needs are unmet, they may experience psychological discomfort, which can affect their values and lead to a negative assessment of the application.16,17,55
In light of the context mentioned above, when patients perceive that the eHealth application effectively satisfies their hedonistic needs and elicits positive emotions, it increases the likelihood of fostering a positive hedonistic motivation, subsequently enhancing the public value of patients. Conversely, if the eHealth app is unable to satisfy individuals’ hedonistic needs, it can result in psychological distress and a pessimistic assessment. Consequently, this diminishes hedonistic motivation and undermines patients’ perceptions of the value of eHealth applications. As a result, the study proposed:
Utilitarian motivation
The concept of utilitarian value in information systems pertains to the degree of effectiveness and efficiency that users perceive when utilizing such systems.80,81 In the same way that, the desire for pleasure, joy, and enjoyment generates hedonistic consumption, the desire to solve problems and meet needs and wants stimulates utilitarian consumption. Even though, in most circumstances, both hedonistic and utilitarian incentives influence consumption decisions, either hedonistic or utilitarian motivation has been proven to dominate the decision-making process. 82
In addition, Motivation Theory suggests that hedonistic and utilitarian motivations influence individuals’ behaviors, including their engagement with eHealth.13,83,84 The utilitarian-instrumental dimension is crucial in creating public value, as it represents a collectively shared value associated with efficiency and the effective generation of benefits. This dimension is based on the need for control and coherence in one's conceptual framework, which focuses on people's ability to comprehend, anticipate, and handle their environment. 17 In the provision of services, the instrumental-utilitarian profile is driven by two fundamental questions: “Is it useful?” and “Is it profitable?”. 56
Utilitarian services, conversely, are more logical and functional, satisfying consumers’ essential consuming demands. 82 As outcome-oriented characteristics, it considers the usefulness, quality, performance, and predictability of the participation process, which can enhance the primary service outcome. 85 The utilitarian advantages of eHealth services, particularly the system's ability to store and access health records, can inspire individuals to cultivate favorable attitudes and confidence in eHealth.78,86
Furthermore, the research on utilitarian motivations in eHealth adoption, particularly through the perspectives of the Technology Acceptance Model (TAM) and the Unified Theory of Acceptance and Use of Technology (UTAUT), indicates a strong emphasis on factors such as perceived usefulness (PU) and performance expectancy (PE).87,88 Studies have demonstrated that performance expectancy significantly influences behavioral intention in various contexts, including the adoption of health information technologies.89,90 However, the specific reasons for adopting eHealth tools often go beyond perceived usefulness and performance expectancy, centering more on the practical and immediate health benefits perceived by the patients. 91
The eHealth app, driven by utilitarian motivation, has the potential to generate public value for patients by providing reliable and effective services to address societal health concerns. In Jordan, where almost 24% of individuals aged 40 to 69 face a 10-year cardiovascular disease (CVD) risk exceeding 30% or already have cardiovascular disease, and 18% of the population experiences depression, with only 6.5% undergoing therapy, 92 the application of ICTs in healthcare can significantly improve patient-centeredness and care integration, crucial elements in multimorbidity care. Recognized as a catalyst for innovation in health and social care systems, eHealth offers numerous benefits for those with chronic conditions. It enhances the overall quality of life for patients and their family caregivers, optimizes resource utilization, and indirectly improves care appropriateness for Jordanian society, as widely acknowledged in the literature. 93
The current debate takes us back to the psychological concept of utilitarian motivation proposed by Meynhardt & Jasinenko.
17
The idea is grounded in humans’ fundamental need for control and coherence within his/her conceptual systems. Specifically, it relates to the patient's capacity to understand, expect, and exert influence over their environment. Consequently, this process contributes to establishing a patient's public value about the utilization and acceptance of the eHealth app. Therefore, the study posits
Social value
Adopting technology is not just about utility but also social value. It connects users with their social group and helps them express their personality, social image, and social class membership. 83 In today's society, consumption is no longer just about traditional goods and production accessories; it has become a form of self-expression and identity. By adopting the same technology as their superiors and aspirational groups, individuals can maintain their existing status order. 94 Furthermore, technology services can enhance social relationships and provide social value, especially when publicly or socially recommended, making it easy for consumers to derive social value from technology content. 95 Thus, many technology adoption theories, such as UTAUT, integrate social value within their models through the construct of social influence.25,69
The rise of digital health platforms and online health communities (OHCs) has significantly boosted patient engagement in healthcare. Healthcare providers face equal opportunities and threats from patient-driven service innovation. Recent literature underscores the importance of patient and stakeholder participation in creating value in healthcare services. 96 Users on health platforms contribute financially, ethically, epistemicly, and in other forms of value through interactions and platform engagement, including assisting other patients and sharing health information. User ratings, social connections, patient feedback tracking, and user profiling are methods for generating social value from health technologies.97,98 Chamakiotis et al. explored how online health communities create social value in post-conflict areas, identifying three categories of non-economic social value: cognitive, professional, and epistemic. Social value is fostered through philanthropic, moral, and reciprocal activities, offering new ways to engage with digital health. 98
From a public value approach, the emphasis is put on the contributions to what individuals perceive as “society” and its overall well-being, relying heavily on images and relationships that significantly influence organizations. Echoing Epictetus’ second-century philosophy, “People are not disturbed by things, but by the view they take of them.” 56 Meynhardt adds that the social dimension of public value embodies “a collectively shared value associated with social interactions and what it means to create positive group relations.” Individuals strive to maintain healthy relationships, social identity, and group participation in alignment with the fundamental need for social belonging. 17 The construction of public value hinges on conceptualizing the broader public and signifies mental representations of society. This understanding characterizes the “public” as the collectively shared assessment of the social collective. From this perspective, the public is not merely a social aggregate but a state of mind shaped by organizations and their activities, grounded in contemporary psychological theories of basic human needs. While public value denotes the value generated from a societal standpoint by contributing to what people perceive as “society” and its well-being, human needs address the essential psychological class underlying all judgments. 99
In summary, patients seek to create social value by using eHealth apps to nurture relationships, social identity, and group participation, aligning with their basic need for social belonging and reflecting on their public value. Consequently, the study hypothesized that
Ethical public value
Ethics lie at the heart of the values that guide healthcare delivery. 100 Like Justice, Privacy,101,102 and Human Dignity. 103 The identification and protection of ethics in eHealth services from the standpoint of service users is essential. 104 The ethical considerations surrounding health information have been a long-standing issue. However, with the integration of technology in healthcare, a plethora of novel ethical concerns have emerged that require attention. Health data storage and dissemination are no longer under individuals’ direct control, which poses several challenges that must be resolved for eHealth to thrive in the future. 105
In contrast, as eHealth advances, it brings exciting opportunities and essential concerns. While ethical concerns should not hinder innovation, we must carefully consider potential scenarios that allow us to progress in medicine and as a society. 106 To this end, experts have suggested that the evaluation of eHealth services should encompass both the concept of public value and social justice while also prioritizing privacy, security, and accountability. 12 Public value refers to the moral and sociocultural standards that individuals uphold as just and right, and these values can inform personal and external normative commitments that guide behavior.44,107 Ultimately, social and public values hold ethical significance and should be considered when developing and implementing eHealth services.
In other words, a social value is anything that says we should act in a manner consistent with that value. Values are moral ideals that should be adhered to if possible. There are numerous such values, and they may frequently be in conflict. For instance, the common value that available health and social care resources should be used to have the greatest potential impact on population health may conflict with the value that these resources should be geographically distributed equitably. Some say that achieving as much equality as feasible in the distribution of health in the population is a more essential social aim than achieving equality in the distribution of resources. However, this may entail an unequal distribution of resources to ensure that those who are the least healthy but are nonetheless able to benefit from health and social care receive a proportionally bigger part. Therefore, we must consider why equality and inequality are important. 108
In this context, The UK's Citizen Council has emphasized the importance of allowing people to make their own decisions and respecting their personal values, cultural beliefs, and religious practices. However, it acknowledged that occasionally, it may be necessary to limit individual choice for the benefit of the entire population. Although the National Institute for Health and Care Excellence (NICE) agrees that respect for autonomy and individual choice is crucial for the National Health Service (NHS) and its users, this should not result in recommendations suggesting interventions that are neither clinically nor economically beneficial. 109
In eHealth literature, Gerli et al. have identified a possible conflict between the protection of personal privacy and the public benefits that can be obtained through the collection of personal data, particularly in the context of contact-tracing apps (CTAs) used during the COVID-19 pandemic.
12
However, ethical public value is grounded in the fundamental human need for self-worth and dignity. Therefore, the assessment carried out by patients regarding the impact of certain eHealth services on their self-worth and positive self-regard can be considered an ethical public value. This dimension encompasses how an eHealth application interacts with patients, particularly in promoting and improving patients’ sense of self-worth and dignity. The MyHakeem application should demonstrate ethical behavior that promotes the ethical aspect of the patient's public value. Additionally, it must exhibit morally acceptable conduct, at a minimum.
17
The following hypothesis was thus put forth
Public trust value
Trust plays a crucial role in promoting social, economic, and democratic advancement, as emphasized by multiple studies. 110 Establishing trust in government is essential for creating public value, as it provides legitimacy to government acts and underscores the importance of a robust relationship between citizens and the government. 111 In healthcare, patients’ trust in doctors is vital for delivering public value and impacting health outcomes and satisfaction. 64
Despite efforts, defining trust remains challenging. 112 For instance, the health literature alone offers 49 definitions. Some definitions, like Rousseau, Sitkin, Burt, and Cramer's, are valuable within eHealth adoption. They describe trust as “a psychological state consisting of the intention to accept vulnerability based on positive expectations of the intentions or behavior of another under conditions of risk and interdependence.” 113
In the public value sphere, though, trust has a broader meaning; it is the third most important source of public value.114,115 An organization (the government) and its activities (the eHealth initiative) are perceived as trusted and legitimate by the public and critical stakeholders to varying degrees. 114 It lies at the core of the relationship between citizens and the government. It is essential regarding services that influence life and liberty, such as health. However, it is also essential for many other services. A lack of trust eliminates public value, even if formal service and outcome goals are accomplished in certain instances. 115 Consequently, trust generates public value. 116
Trust is crucial to modern eHealth technologies. 117 It is widely acknowledged that cultivating trust in eHealth services is vital for ensuring the successful implementation of technology. 30 Patients place great importance on trust when discussing health-related Internet information (HRII) with healthcare professionals (HCPs), which encourages their participation. 100 Therefore, eHealth must instill trust in citizens, assuring them that their data is being processed accurately, is up-to-date and of high quality, and that security risks are being addressed. In essence, eHealth must inspire confidence in citizens to use it. 104 Despite this, research into the nature and extent of public trust in healthcare systems is rare. 118
An alternative perspective posits that trust possesses intrinsic value rather than serving solely as a means to an end. 119 Trust is widely recognized as a core value and a belief in the higher-order or more generalized schema of personhood, such as that the self is worthy and people are generally trustworthy.22,70 Trust is commonly understood to encompass both affective and cognitive aspects. Furthermore, trust is essential to foster meaning and see patterns, such as the dichotomy between trust and distrust. 120
Therefore, as an integral component of patients’ public value, the trust value dimension influences their willingness to make meaning and perceive patterns within the eHealth system. Trust engenders a positive and receptive mindset that enhances patients’ overall experience, utilization, and understanding of the system. By valuing trust, patients are more likely to embrace the system, interpret information, and identify meaningful patterns, contributing to a more fruitful engagement with the eHealth system. Consequently, the study hypothesized that
Patients’ public value and adoption behavior
To understand why people do what they do and feel what they feel, we need to know what's important to them and what they need and don't need. A central concept concerned with “importance” and “needing” is value. 121 Values can be understood as abstract representations of desired outcomes that are organized hierarchically based on their importance to an individual. Additionally, values are motivational constructs encompassing individuals’ beliefs regarding desirable goals applicable across various contexts and times. 122
Another vital perspective highlights the relationship between subject and object as the source of value. 123 Value emerges from the interaction between a subject who evaluates and an object that is evaluated. Values are subjective and relational, depending on the presence of a valuing subject and the nature of their relationship with the object. The evaluation of this relationship is influenced by individual needs, which act as motivating factors initiating the evaluation process. Needs, being evaluative, generate motivation to take action by serving as reference points for determining what individuals should strive for or aim to achieve.11,17
Epstein's cognitive-experiential self-theory (CEST) integrates different perspectives by recognizing four basic needs: positive self-evaluation, maximizing pleasure and avoiding pain, gaining control and coherence over one's conceptual system, and positive relationships.22,70 These needs are connected to values, with people implicitly valuing experiences that meet their needs. Meynhardt and Jasinenko used these basic needs as a foundation to develop a public value scale, defining public value by the relationship between society and individuals, determined by evaluations of basic needs and realized through emotional-motivational states and personal experiences. 17
In the healthcare domain, particularly eHealth, public value is crucial in understanding eHealth adoption. The current study introduces the concept of patients’ public value, rooted in the values proposed by Epstein, Grawe, Meynhardt, and Jasinenko.17,22,124 Patients’ public value can be understood as the value experienced by patients in their relationship with the eHealth system. This value is subjective, influenced by patients’ evaluations related to their basic needs, and is activated through emotional and motivational states, shaped and sustained by meaningful experiences. 125
The public value of patients comprises several dimensions: hedonistic motivation, utilitarian motivation, social value, ethical value, and trust value. These dimensions are derived from Meynhardt's and Epstein's studies, emphasizing that value is not solely determined by the objective features of the eHealth system but by patients’ subjective evaluations, needs, and emotions.17,22,55,70 When patients collectively share these values, they become public, creating a shared narrative that influences the adoption of eHealth applications.
17
Thus,
Mediator role of habit
The role of habits in shaping behavior is recognized as pivotal, particularly in health psychology, where “habit” denotes behavior prompted automatically by learned cue-behavior correlations. Gardner's definition characterizes habit as a process where a stimulus generates an impulse toward action based on learned associations. 126 Once formed, habits persist regardless of motivational fluctuations, triggering behavior in response to cues even during deliberate goal pursuit. 127 Habit theory posits that automatic habits diminish the impact of intention on behavior, suggesting their potential use for sustaining positive behavior over time. 128 Empirical evidence supports habit's effects on action, with moderate-to-strong habit-behavior correlations. 126 In health and eHealth, habit is defined as a neurologic pattern initiated by repetition and cued responses, influencing health and eHealth usage. Three antecedents define healthy habit formation: a constant cue context, repeated cue encounters, and the learning of stimulus-response links. 129 The outcome of a health habit affects both health 129 and eHealth adoption. 130
When analyzing the adoption and utilization of technology, specifically through the lens of the Unified Theory of Acceptance and Use of Technology, Venkatesh et al. have posed inquiries regarding the primary role of behavioral intention as the primary indicator of technology usage. 69 They have introduced a new theoretical factor, habit, as an essential additional predictor of technology usage. 69 They found that habit has both direct and indirect effects on technology adoption. 69 Additionally, in their literature review, Tamilmani et al. suggested that the habit construct should be included in research on consumer-driven established technologies, given that the role of habit in maintaining the use of technology tends to become more crucial when such use has to be motivated intrinsically. 131
Given the prevalence of technology adoption, particularly in mHealth and eHealth contexts, patients may integrate eHealth services into their daily routines, leading to habitual behavior. When a behavior becomes a habit, it occurs automatically and without conscious thought.
83
In light of the preceding discussion, the following hypothesis has been proposed
Material and method
Initially, the study obtained ethical approval from the “Scientific Research Ethics Committees” of the Jordanian Ministry of Health, granted under reference number MBA/ethics committee/4779 on 23/3/2023. In this study, we used a questionnaire adapted from previous studies,17,83,132–136 detailed in Appendix A in the online supplemental materials (Copyright: Elsevier Inc. 2020, Elsevier Inc. 2019, Elsevier Inc. 2021, Taylor & Francis 2020, and Creative Commons Attribution 4.0 International License). All scales used in our study had been previously validated and demonstrated reliability in studies conducted by Al-Azzam et al., Ashraf et al., Halder et al., Hossain et al., Meng et al., Meynhardt and Jasinenko, and Miller and Simmering17,83,132–136. In addition, participants provided their informed consent to participate in the study, as indicated in the first section of the questionnaire (refer to Appendix B in the online supplemental materials). The survey was accurately translated into Arabic to cater to the language needs of the intended audience and included patient consent, demographic information, and 28 items to evaluate the various aspects of the research model (refer to Appendix B in the online supplemental materials). The questionnaire's formulation was guided by public value theory and acceptance technology literature, as outlined in Appendix A in the online supplemental materials.
Study design and data collection procedures
This study utilized a quantitative cross-sectional design to evaluate the adoption of the MyHakeem application among patients in governmental hospitals in Jordan. The study focused on patients who had either downloaded the MyHakeem mobile app or used its web-based version. MyHakeem application is a web-based platform and mobile app that allows patients to conveniently access and view their pre-booked medical appointments, as well as vital medical information such as active and pending medications, recent immunizations, pending and complete laboratory tests, allergies, vital signs, and demographic data. These data are securely stored on the user's electronic health record, which is registered within the healthcare institution that implements the Hakeem program. Furthermore, this application also provides a hassle-free way for patients to have their monthly medications delivered to them, especially if they are unable to physically go to the hospital. 137
To carry out the research, the study team selected three major governmental hospitals in the Jordanian Capital Governorate (Amman), including Prince Hamza Hospital with 471 available beds, Al Basheer Hospital, the largest public hospital in Jordan with 1090 available beds, and Al Totangi Hospital with 151 available beds, all of which had implemented the Hakeem program. 138 The patient affairs department of these hospitals assisted the research team in randomly selecting 478 patients who completed a questionnaire administered via a Google Forms link between April 19th and July 5th, 2023.
In structural equation modeling, it is recommended to have at least 400 participants for a valid sample size. 139 Before analyzing the data, cleaning procedures were carried out, which involved identifying and handling missing data, detecting outliers, examining sample size, testing multivariate normality, and conducting Bartlett's and the Kaiser, Meyer, Olkin (KMO) tests. 140 A total of 478 questionnaires were distributed, resulting in a 97.3% response rate with 465 completed forms returned and no missing values observed. However, there were 26 outlier values and nine response biases, which accounted for 7.5% of the sample (see Appendix E). Ultimately, the final sample consisted of 430 participants, sufficient for SEM. An exploratory factor analysis was then conducted to consolidate the dimensions associated with each construct (refer to tables in Appendix F in the online supplemental materials for more information)
Sample characteristics
Table 1 presents an analysis of the demographic data from the sample, including gender, age, education level, frequency of product usage, doctor visits, and overall health status. The sample included 430 individuals, with 51.4% male and 48.6% female. The largest percentage of participants fell within the age range of 41–50 years (45.1%), followed by 31–40 years (38.6%),≥50 years (8.8%), and 18–30 years (7.4%). The majority of participants held a bachelor's degree (47.9%), followed by postgraduate (41.6%) and high school (10.5%). In terms of the MyHakeem app's usage, 12.8% reported using it only once, 40.9% used it 2–3 times, and 46.3% used it three times or more. Regarding doctor visits in the last three months, 54.7% reported visiting a doctor, while 45.3% did not. Regarding health status in the last three months, 51.6% reported being sick, while 48.4% reported not being sick.
Demographic data.

Statistical analysis
Initially, the factorability of the 28 items in the patients’ value scale was assessed using IBM-SPSS v26. Upon examination, it was found that all 28 items had a satisfactory correlation with at least one other item. The Kaiser–Meyer–Olkin measure of sampling adequacy was calculated to be 0.863, which is higher than the recommended value of 0.6. 131 Additionally, Bartlett's test of sphericity was significant χ2(378) = 4398.971, p < .001, indicating that the correlation structure is appropriate for factor analysis.140,141 Furthermore, all diagonals of the anti-image correlation matrix were greater than 0.5, and all communalities were greater than 0.30 (refer to Appendix F in the online supplemental materials), which further supports the notion that each item shares some variance with other items.140,141 Based on these overall indicators, it was concluded that the 28 items were sufficient for exploratory factor analysis.
Next, exploratory factor analysis was applied to all 28 items of the instrument, using a cut-off point of 0.40 and Kaiser's criterion of eigenvalues greater than 1 (refer to Appendix F in the online supplemental materials).142,143 This analysis yielded an eight-factor solution (including marker variable) that accounted for 79.86% of the variance, which was deemed the best fit for the data.142,143 The eight-factor solution was favored due to its alignment with the theoretical framework and the “leveling off” of eigenvalues on the scree plot after the eighth factor.
The following two-step approach of structural equation modeling, as proposed by Hair and his colleagues, was implemented using AMOS 26. 140 The first step involved assessing the measurement model, which showed that all goodness-of-fit indices for the model constructs met the recommended thresholds as evidenced by χ2 (244) = 387.272, chi-squared degree of freedom ratio (χ2/df) = 1.587, comparative fitness index (CFI) = 0.961, standardize root mean square residual (SRMR) = 0.051, and root mean square error of approximation RMSEA = 0.052, and p = .336.144,145 The second step involved analyzing the structural model, and the findings are discussed in the model's results section.
Descriptive statistics for the seven constructs were presented in Table 2 during the confirmatory factor analysis (CFA) stage. The skewness and kurtosis were within a tolerable range for assuming a normal distribution, and the highest mean was for the hedonistic motivation of 3.06. 140 Also, the CFA was performed to evaluate the constructs’ reliability and validity (refer to Tables 2 and 3), and all factor loadings exceeded the 0.50 level (0.729–0.939).140,141 The constructs’ reliability was evaluated using Cronbach’s alpha and McDonald's Omega coefficient, and the data showed internal reliability greater than the recommended threshold of 0.70. 146
Confirmatory factor analysis and descriptive statistics.

Note: HB: Habit; UM: Utilitarian motivation; PTV: Public Trust Value; SV: Social value; HM: Hedonistic motivation; EPV: Ethical public value; UB: Adoption behavior. α = Cronbach's Alpha coefficient; ω = McDonald's Omega coefficient.
Discriminant, convergent validity and composite reliability for the first order of confirmatory factor analysis (CFA).

Note: HB: Habit; UM: Utilitarian motivation; PTV: Public Trust Value; SV: Social value; HM: Hedonistic motivation; EPV: Ethical public value; AB: Adoption behavior; Composite Reliability = (CR) > 0.70, Average Variance Extracted = AVE > 0.50, Maximum Shared Variance = AVE > MSV and McDonald Construct Reliability = MaxR(H) > 0.7. The square root of the AVE is displayed as diagonal boldface values.
Despite self-administered questionnaires being widely used in research, many studies fail to report common method bias. 147 To address this issue, our research employed an advanced technique called the external marker variable approach, which is more precise than the common latent factor method. 136 This approach involves incorporating an additional latent feature, the blue marker, into the survey method due to its common role in biasing results of experimental and survey studies.135,148 Data analysis revealed that there was no bias in the questionnaire responses. This was demonstrated by the non-significant difference between the unconstrained and constrained models, as shown in Table 4.
Model Fit Indices and Model Comparisons for confirmatory factor analysis CA Models with Marker Variable.
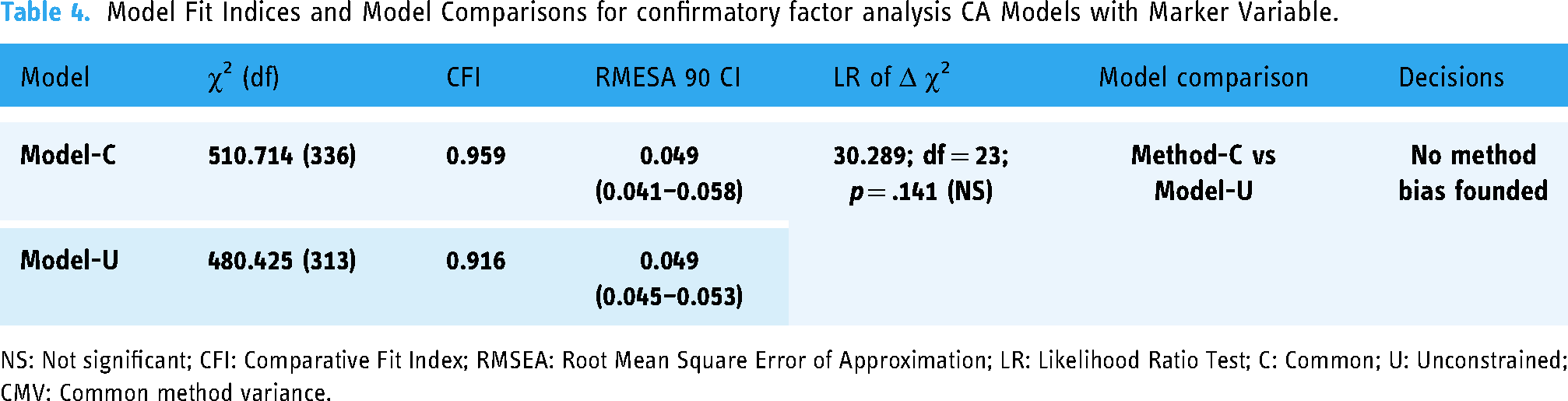
NS: Not significant; CFI: Comparative Fit Index; RMSEA: Root Mean Square Error of Approximation; LR: Likelihood Ratio Test; C: Common; U: Unconstrained; CMV: Common method variance.
The second order confirmatory measurement model & reliability and validity
The current study developed a second-order reflective measurement model for patients’ public value by drawing on Meynhardt's concept of public value and the concept of trust value. This model was formulated by Brown's guidelines. 149 The three-step process involved in this study includes, firstly, constructing a first-order confirmatory factor analysis (CFA) solution that is both well-fitting and conceptually sound, which has been achieved in the preceding section of this article. Secondly, analyzing the correlations among the factors in the first-order solution, which are presented in Tables 3 and 5, the results indicate that the correlation coefficients between the five components of patients’ public value surpass their correlations with other constructs, with moderate to high correlations ranging from 0.453 to 0. 0.619. 150 Lastly, the second-order factor model fits with data, as evidenced by the following fit indices: χ2 (231) = 375.521, χ2/df = 1.626, CFI = 0.961, SRMR =0.048, RMSEA = 0.054, and p = .245. 144 As shown in Appendix D in the online supplemental materials, patients’ public value is comprised of five first-order dimensions: public trust value, social value, hedonistic motivation, utilitarian motivation, and ethical public value. Additionally, an assessment of the instrument's validity and reliability was conducted, as indicated in Tables 3, 5 and 6.
Discriminant, convergent validity and composite reliability for 2nd order of confirmatory factor analysis (CFA).

Note: Patients Public Value (PPV); Adoption behavior (AB); Habit (HB); Composite Reliability = (CR) > 0.70, Average Variance Extracted = AVE > 0.50, Maximum Shared Variance = AVE > MSV and McDonald Construct Reliability = MaxR(H) > 0.7. ***p < .001. The square root of the AVE is displayed as diagonal boldface values.
Heterotrait-Monotrait ratio (HTMT) correlation analysis result.

The composite reliability (CR) and average variance extracted (AVE) were used to evaluate the convergent validity of the first and second orders of confirmatory factor analysis, as recommended by Hair et al. 140 A model's convergent validity is established when composite reliability values exceed 0.70, AVE values surpass 0.50 and the AVE values exceed both the average shared variance (ASV) and their corresponding maximum shared variance (MSV). Our study found that all composite reliability values exceeded 0.70 and all AVE values were above 0.50, which confirms the model's convergent validity,140,153 as shown in Table 3. Discriminant validity was determined using two different methods: the approach proposed by Fornell and Larcker 154 and the heterotrait-monotrait ratio of correlations (HTMT) as suggested by Henseler et al. 151 According to Fornell and Larcker's method, discriminant validity is confirmed if the square roots of the AVE values, which are displayed along the diagonal axis in Table 3, are greater than the corresponding inter-construct correlation coefficients. Our study found that the smallest square root of AVE was 0.811, which exceeded the highest correlation coefficient value of 0.619. This confirms the discriminant validity of our model. Additionally, all HTMT values, as presented in Table 6, were below the threshold of 0.90, which further supports the discriminant validity of the measures, by Henseler et al.'s 151 guidelines. As a result, our research model achieved both convergent and discriminant validity. Therefore, it can be concluded that the measurement items used in this study demonstrate suitable construct validity.
Model's results
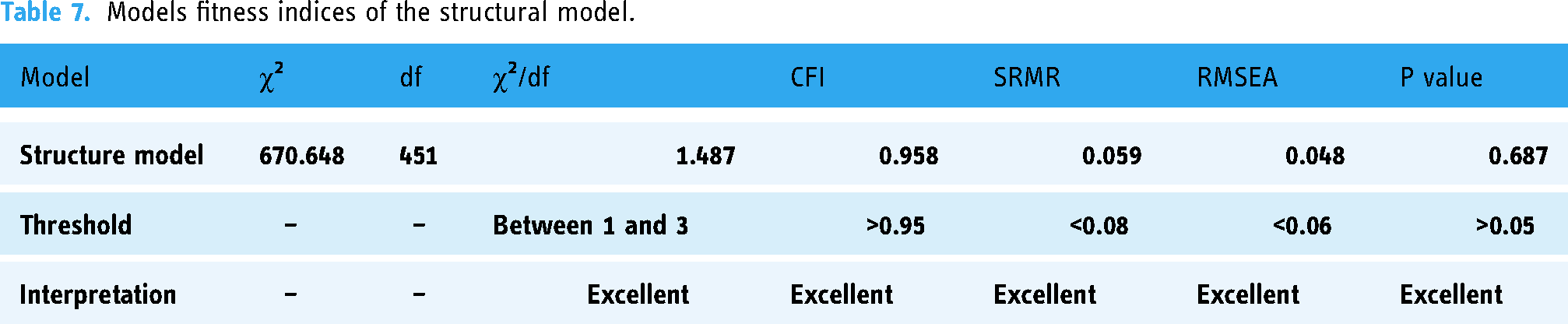
In this study, the final step of Structural Equation Modeling (SEM) involved transforming the measurement model into a structural model, as suggested by Hair et al. 140 Results showed that the model fit was satisfactory according to the criteria established by Crawford & Kelder and Gaskin and Lim.144,152 Specifically, the chi-square (χ2) value was 387.272, χ2/df was 1.587, the Comparative Fit Index (CFI) was 0.961, the Standardized Root Mean Square Residual (SRMR) was 0.051, the Root Mean Square Error of Approximation (RMSEA) was 0.052, and the P value was 0.336. As depicted in Figure 2 and Table 7, no further modifications or improvements were needed.

Structural model.
Models fitness indices of the structural model.
The hypotheses H1 (β = 0.802, p < .001), H2 (β = 0.699, p < .001), H3 (β = 0.716, p < .001), H4 (β = 0.732, p < .001), and H5 (β = 0.690, p < .001) were supported as patients’ public value was significantly influenced by hedonistic motivation, utilitarian motivation, social value, ethical public value, and public trust value, respectively. Similarly, H6 (β = 0.233, p = .003) was supported as patients’ public value reported a significant impact on adoption behavior towards eHealth apps (see Table 8). The structural model also explained a 34% variance in the adoption of eHealth apps (Figure 2).
Hypotheses testing.

Note. *p < .05; ***p < .001.
Subsequently, the researchers examined the indirect relationships between the public value of patients and their utilization of eHealth applications. According to the data in Table 9, the results indicate a significant indirect impact of patients’ public value on adopting eHealth apps. Usage habits mediate this effect, hence confirming hypothesis H7 (β = 0.205, p < .001).
Results of the bootstrapping method for mediation.

Note. IV = Independent variable; M = Mediator DV = Dependent variable. ***p < .001.
Discussion
The current study validated a five-dimensional scale for evaluating patients’ adoption of eHealth applications based on their public value. The scale includes the four dimensions of Meynhardt and Jasinenko (hedonistic motivation, utilitarian motivation, social value, and ethical public value) as well as the added dimension of public trust value. 17 This additional dimension has a significant correlation with patients’ public value (Figure 2), which is in line with psychological theories that emphasize the importance of trust in interpersonal relationships. 155 Empirical research has also shown that trust is crucial in eHealth systems and public value theory. Several studies, including those by Callinan et al., Chohan and Hu, De Leebeeck, Lindenfalka, and Vimarlunda, and Tur-Sinai et al., have found that trust is the most significant factor in generating digital public value and is closely linked to eHealth services.156–160
The study findings also confirm that patients prioritize hedonistic motivations when using eHealth applications. This contrasts with previous studies by Griesser et al. and Rahman et al., who argued that hedonistic motivation is typically not a factor in eHealth technology usage.161,162 Griesser et al. added that prior experience is the basis for hedonistic and utilitarian values, while the health category is more closely related to utilitarian values than to hedonistic values. 161 However, in the adoption of eHealth applications, hedonistic motivations can indeed be prioritized over utilitarian motivations. This is especially true since many eHealth technologies include features that foster emotional connections, such as personalized health insights, gamification elements, and motivational messages. These elements appeal to hedonic values by creating positive emotional experiences and fostering a sense of fulfillment and engagement with one's health journey. Many empirical studies, including Alam et al., Han and Zo, Ferreira-Brito et al., and Soni et al., support this claim, indicating that hedonic motives often lead to eHealth adoption, even in contexts traditionally associated with utilitarian values like health.163–166 Additionally, Tamilmani et al. conducted a meta-analysis revealing that 58% (53/91) of the included UTAUT2-related empirical studies involved hedonic motivation as a factor, with 81% (43/53) of the studies finding a positive relationship between hedonic motivation and technology adoption.167,168 This trend is evident in the eHealth field as well.167,169
Furthermore, the research emphasizes the significant influence of social value on the public perception of patients, underscoring the importance of positive relationships, social inclusion, and the fundamental human need for social interaction in shaping the public value of patients. This aligns with the findings of Meynhardt and Jasinenko, as well as prior empirical studies in eHealth, which have demonstrated the role of social value in the adoption of eHealth apps to enhance patients’ standing within their communities.17,170 Additionally, Chamakiotis et al. emphasize the ability of online health communities to provide social value by facilitating connections among individuals dedicated to improving healthcare collectively. These platforms enable the exchange of knowledge, support, resource sharing, collaboration, and empowerment of patients to collectively create social value. 98
In line with Meynhardt and Jasinenko's claim about the connection between ethical value, personhood, and the fundamental essence of humanity, the study's results affirm that ethical value is a key factor in shaping the public value of patients. 17 The ethical value in eHealth revolves around how health technology handles patients’ data and upholds their dignity and self-esteem.104,171,172 The results of Lin-Hi et al.'s study also assert that patients are more likely to embrace eHealth apps if they believe that the technology does not endanger the ethical foundations of their society and is consistent with their ethical values. 173
Moreover, the study's results prove that patients’ public values have a significant impact on their behavior when it comes to accepting and adopting eHealth applications. This impact is supported by neuroscientific research, which often begins by examining the neurochemical dopamine and the ventral tegmental area (VTA), both of which play a crucial role in how the brain processes and evaluates reward-related behavior.174,175 A recent review of neuroscientific literature on the relationship between values and behavior has provided evidence of a more direct connection. 176 Additionally, neuroimaging research by Brosch et al. has shown that individuals with strong self-transcendence values tend to consider the long-term consequences of their actions more heavily when making decisions. 177 Furthermore, empirical studies by Yuen et al. and Liu et al. have found that fulfilling psychological needs and creating value are vital factors in determining behavior. The perceived value of telehealth also directly and indirectly influences patients’ adoption, which aligns with the findings of the current study.178,179
However, habit is a crucial link between values and behavior, mediating around 20.5% of this relationship. In other words, regular use of the features of an eHealth app acts as a mediator, linking patients’ values with its usage. This finding is consistent with Wood et al. and Balleine and Dezfouli, who found that a positive user experience, reliable features, and an intuitive interface contribute to habit formation, reinforcing the relationship between values and behavior.180,181 By promoting positive habits that align with one's core values, the app becomes integral to patients’ daily routines.182,183
Theoretical and practical implications
Our study has significant theoretical implications. It encourages the evaluation of technology adoption in the relatively novel context of patient adoption of eHealth and broadens the understanding of public value in that context. It corroborates that the public value model of patients significantly influences their utilization and acceptance of eHealth apps and, by incorporating patients’ trust value into the existing dimensions of hedonistic motivation, utilitarian motivation, social value, and ethical value, it emphasizes the importance of trust as a foundational factor. In so doing, it calls for acknowledging the multidimensionality of public value and the role of trust in influencing individuals’ adoption of technology. Its findings also highlight the importance of several aspects, including ethical and social values, in shaping patients’ public values regarding eHealth adoption. On the other hand, the heavy impact of patients’ values on their behavior reinforces the findings of neuroimaging research regarding value-behavior relationships. Also, knowing how habits are formed will contribute to a better understanding of how to bridge the gap between abstract values and behavior.
At a practical level, the study provides valuable insights for creating patient-centric eHealth interventions and policies. By considering patients’ values, healthcare professionals may be better able to design interventions tailored to each patient's unique needs and preferences. In line with the confirmed significance of eHealth applications being perceived as valuable and aligned with patients’ utilitarian needs, developers and healthcare organizations should prioritize the development of eHealth apps that offer tangible advantages, such as enhanced accessibility to healthcare information and improved health outcomes. However, a more holistic understanding of patients’ perspectives and adoption factors may guide eHealth interventions’ design, implementation, and promotion more fully aligned with patients’ values, preferences, and trust. In addition, this holistic model can guide the development of targeted strategies to address specific factors and improve patients’ experiences, such as addressing privacy concerns, empowering patients, promoting social support and health justice, and ensuring ethical standards are met. The model also paves the way to foster sustained engagement and adoption through user experience and interface design. In the end, aligning eHealth initiatives with patients’ values can contribute to the development of positive habits, which in turn can lead to improved health outcomes.
Limitations and future research
Although this research has made significant contributions to the current academic literature and has practical applications, it is essential to acknowledge its limitations when interpreting the findings. First of all, the study examined an eHealth app that is still in the process of development and found that it needed to contain all the services and features that patients needed. This resulted in the absence of an identification of the actual influence of certain variables on patient values. Second, our empirical application is situated within the framework of Jordan's emerging economy, characterized by distinct health and digital infrastructure compared to more developed countries. Hence, this calls for caution when extrapolating these empirical results to developed countries. Last, our model did not incorporate the factors associated with eHealth technology infrastructure.
This study offers promising directions for future research to explore the intricate interplay between patients’ values and their adoption of eHealth technology. Investigating how various variables may moderate or mediate the relationship between patients’ values and eHealth technology adoption is essential. Conducting longitudinal studies can provide valuable information on eHealth programs’ long-term effectiveness and viability. Additionally, incorporating public value theory into technology adoption models, particularly in the context of eHealth and Healthcare 4.0, can ensure that these models align with the latest technological advancements.
Conclusion
This study introduces a five-dimensional scale that assesses patients’ adoption of eHealth applications based on their public value. The scale includes five dimensions that significantly correlate with patients’ public value: hedonistic motivation, utilitarian motivation, social value, ethical public value, and public trust value. Patients in developing countries tend to prioritize hedonistic motivations when using eHealth applications, while social and utilitarian values significantly create patients’ public value. Ethical and trust values also play an essential role in creating public value, particularly in how health technology handles patients’ data and upholds their dignity and self-esteem. This study highlights the crucial role of public values in patients’ adoption of eHealth apps.
It is essential to recognize the complexity of patients’ public values and their impact on technology adoption. To foster patient-centric eHealth interventions and policies, healthcare providers must develop interventions customized to each patient's specific needs and preferences. Developers and healthcare organizations should prioritize the creation of eHealth apps that provide tangible benefits, including greater access to healthcare information and improved health outcomes.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241272567 - Supplemental material for A public value-based model to understand patients’ adoption of eHealth: Theoretical underpinnings and empirical application
Supplemental material, sj-docx-1-dhj-10.1177_20552076241272567 for A public value-based model to understand patients’ adoption of eHealth: Theoretical underpinnings and empirical application by Mohammad Alhur, José Caamaño-Alegre and Francisco Reyes-Santias in DIGITAL HEALTH
Footnotes
Acknowledgements
We are grateful to the services provided by Grammarly for helping us polish our writing.
Author contributions
The study was conceived by José, Francisco, and Mohammad, who conducted literature research. Mohammad was responsible for collecting and analyzing the data. José, Francisco, and Mohammad drafted and critically reviewed the manuscript. Finally, José and Francisco approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study obtained ethical approval from the “Scientific Research Ethics Committees” of the Jordanian Ministry of Health, granted under reference number (MBA/ethics committee/4779) on 23/3/2023.
Funding
This research has been funded with support from the USC's ECOAGRASOC research group.
Guarantor
Mohammad Alhur
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.