
Abstract
Objective
Tailored digital health programs can promote positive health-related lifestyle changes and have been shown to be (cost) effective in trials. However, such programs are used suboptimally. New approaches are needed to optimise the use of these programs. This paper illustrates the potential of recommender systems to support and enhance computer-tailored digital health interventions. The aim is threefold, to explore: (1) how recommender systems provide health recommendations, (2) to what extent recommender systems incorporate theoretical models and (3) how the use of recommender systems may enhance the usage of computer-tailored interventions.
Methods
A scoping review was conducted, using MEDLINE and ScienceDirect, to identify health recommender systems reported in studies between January 2007 and December 2017. Information was subsequently extracted to understand the potential benefits of recommender systems for computer-tailored digital health programs. Titles and abstracts of 1184 studies were screened for the full-text screening, in which two reviewers independently selected articles and systematically extracted data using a predefined extraction form.
Results
A total of 26 articles were included for data extraction. General characteristics were reported, with eight studies reporting hybrid filtering. A description of how each recommender system provides a recommendation is described; the majority of recommender systems used messages as recommendation. We identified the potential effects of recommender systems on efficiency, effectiveness, trustworthiness and enjoyment of the digital health program.
Conclusions
Incorporating a collaborative method with demographic filtering as a second step to knowledge-based filtering could potentially add value to traditional tailoring with regard to enhancing the user experience. This study illustrates how recommender systems, especially hybrid programs, may have the potential to bring tailored digital health forward.
Introduction
Digital health is an umbrella term for the usage of digital technology to support health, 1 and it can be employed to promote positive health-related lifestyle changes. 2 With digital health, the opportunity arises to use computer tailoring to deliver personalised interventions to users via the internet, motivating users to adopt health behaviours without face-to-face counselling. 3 Computer-tailored interventions gather individual information and create a personally tailored intervention based on the behaviour and motivational characteristics of the participant. Using individual data, via theoretically based questionnaires, a computer program sends tailored feedback to the participant. These interventions have the opportunity to function via the internet (often web based), which provides great social and economic advantages 4 (e.g. greater reach, and low costs per smoker,5,6 in the case of support for smoking cessation). Computer-tailored digital health interventions have been shown to be both effective and cost effective in motivating individuals to adopt healthy behaviours such as smoking cessation, 7 weight loss and nutrition interventions.8,9
However, all these opportunities are tempered by the problem that these interventions are used suboptimally. This is reflected by high dropout rates (in randomised trials) 10 and the fact that users do not use the intervention as recommended, or correctly.9,11 More specifically, once the target group has accessed the website of the intervention, they spend a limited amount of time on it and the utilisation rates are low.8,12 Consequently, tailored interventions, although having great potential to effectively motivate people to adopt a healthy lifestyle, may suffer from low usage rates. Practically, as these interventions are underused, they will not motivate a large number of potential participants to change their lifestyle behaviours. 13 Engaging the user, or enhancing the quality of the user experience, and usage of the program is paramount for a digital health intervention to be effective.4,14 This could be achieved by the program itself, via its contents and delivery modes.4,14 Accordingly, it is important to understand how to foster engagement; we need to understand the user experience of digital health programs to address issues such as the low use of intervention features, few logins, and poor retention rates.14–16
One promising approach to fostering the user experience of tailored digital health programs is the use of recommender systems (RSs). 12 These machine-based learning and information retrieval systems have the potential to predict items that will be relevant (e.g. a health message) for individuals. 17 In the last decade, RSs have gained popularity and have been applied in several domains (e.g. e-commerce, social media and advertising), but so far their application in the health domain has been limited. A recent scoping review provided a multidisciplinary overview of the applications of RSs in the health domain, detailing the trends regarding domain application, study methodology, the reporting of behavioural change theories and technical aspects (e.g. interface used). 18 This overview indicates that the use of RSs in changing health behaviour is in its infancy (with only several papers on health-directed RSs and a complete lack of reporting on the theoretical factors and behavioural change techniques used). Nevertheless, the papers do suggest that RSs have the potential to recommend tailored digital health interventions, optimising the message – tailoring it – by selecting the messages most relevant to the user (based on user data). Indeed, one of the potential advantages of the RS is to reduce the burden that an individual may experience because of the huge amount of information available on the internet. 17 Several common approaches used in RSs have been noted in the literature, such as content-based and collaborative filtering, as well as a combination of the two methods (these are also known as hybrid RSs). 18 Different recommendation methods result in different sets of recommended items for the end-user, depending on the algorithm used. For example, in comparison with computer-tailored interventions which are not enhanced by the RS, one benefit of an RS that uses collaborative filtering is the ability to keep renewing data and develop along with user preferences. The system uses the digital trail that individuals have left behind to create a suggestion that suits them optimally. This digital trail could be compared with that of other individuals who share similar interests or attributes, based on the assumption that, if a user with similar interests or attributes likes an item, the original user will like it too. This may lead to personalised suggestions for each user, based on the user’s preferences for a particular item and/or similarities with other users. 19 A possible explanation for the limited usage of computer tailoring may be the lack of attention paid to the differences in personal preferences concerning how health information is presented, as individual preferences in information and information processing styles are dynamic and may fluctuate. 20 This suggests the need to review how the various types of RSs provide health recommendations to develop an approach that has the best potential to enhance the usage of tailored digital health interventions.
RSs seem to have the potential to aid computer-tailored interventions by enhancing the user experience. However, to the best of our knowledge, the potential of RSs to aid computer tailoring and via which mechanisms has never been reported. Since RSs’ recommendations for computer-tailored interventions are based on the user’s digital movements and profile, they can be highly personalised, and are most likely to be useful. These features may enhance the user’s experience and in turn lead to higher usage of health interventions, that is, e-loyalty, which can potentially address one of the key health system challenges, the lack of service utilisation. 1
This study uses the user experience model to illustrate via what mechanisms RSs could enhance the user experience and usage of computer tailoring.
21
This model stipulates the underlying mechanism to the use of web-based interventions, which has been validated in three interventions in previous studies.
21
Prior research has provided some support for associations within the model, and demonstrates the importance of the model constructs regarding e-loyalty. The user
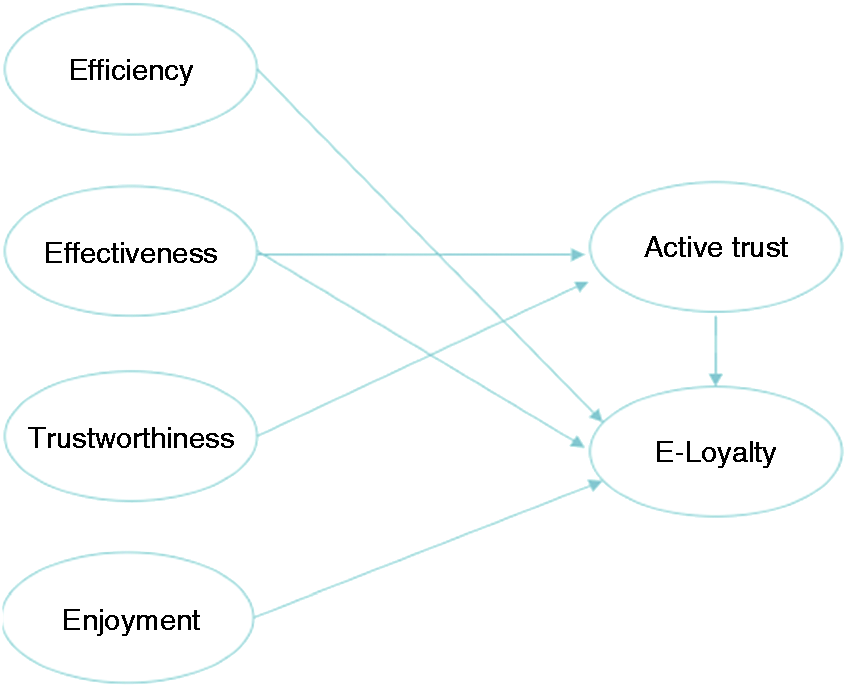
User-experience model (Crutzen et al., 2011). 21
RSs are thus able to track the interactions of the individual with the system and enhance the personal relevance of the recommendations sent to the user. Yet, to the best of our knowledge, literature on RSs and literature on computer tailoring make minimal effort to show that RSs can be linked to tailoring. Whilst a recent scoping review provided an overview regarding trends in health-directed recommender systems, 18 the potential of RS to add value to computer tailoring was not detailed. This study maps current health-directed RSs and their features to constructs of a theoretical model that may explain the underlying mechanism by which RSs potentially may add value to computer tailoring regarding the user experience and the usage of tailored digital health. A next step, therefore, is to identify the potential of RSs with regard to tailored digital health interventions, such as computer-tailored programs, and understand via what mechanisms they could enhance program usage. This may improve e-loyalty and also maximise the health benefits of these programs for the users. For this purpose, the aim is threefold, to explore: (1) how RSs provide health recommendations, (2) to what extent RSs incorporate theoretical models and (3) how the use of RSs may enhance the usage of computer-tailored interventions.
Methods
Literature search
A scoping review was conducted. This method is advantageous when the current literature of the target area is not extensive enough for a full systematic review. 23 The scoping review has a broadly defined research question and researchers can develop the inclusion and exclusion criteria during data extraction, select any study types and chart the available data accordingly. 23 This study adopted the methodology and framework of Arksey and O'Malley, 24 which includes five phases of a scoping review: (1) identify the research question, (2) identify relevant studies, (3) study selection, (4) charting the data and (5) collecting, summarising and reporting results.
This study explores RSs with the purpose of providing health recommendations to patients. The literature search was conducted using MEDLINE (via PubMed) and ScienceDirect to identify all English- or Dutch-language studies available in print or online between January 2007 and December 2017. As our focus was on exploring the potential of RSs by mapping features to the user experience of tailored digital health, rather than a systematic overview of health-directed RSs, we used two common databases for health promotion research. The time frame of 10 years was chosen because of the recent development of RSs, particularly health-directed RSs. 18 The search strategy was based on an earlier scoping review by Hors-Fraile et al. 18 on health RSs. The free text terms were discussed within the research group, leading to the use of the following search terms: (‘Recommender system’ OR ‘recommender systems’ OR ‘recommendation systems’) AND (‘health’ OR ‘healthcare’ OR ‘patient’ OR ‘patients’). When available, the keywords were explored throughout the entire text. In addition, the bibliographies of studies identified in the literature search were searched manually (forward and backward) for additional articles.
Study selection
The titles and abstracts of 1184 articles were screened by one author. The eligibility criteria were: (1) description of a health-directed RS, (2) online intervention and (3) the study had to be in Dutch or English. Studies referring to the same content in different papers were considered duplicates. The title and abstract screening led to 42 articles for full-text screening. Two authors independently reviewed the full text of these 42 articles. Consensus on study inclusion was reached via discussion.
Data extraction and analysis
For each study included, two authors independently extracted data using a predefined extraction form that included items for understanding how RSs provide health recommendations, to what extent RSs incorporate theoretical grounding and how RSs may enhance the user experience of digital health programs. Any disagreements were resolved by consensus. A pilot study was performed by the two reviewers over three studies, which led to minor adjustments in the extraction form.
The extracted data included three categories: general RSs characteristics, provision of health recommendations and user experience. General RSs characteristics included: first author, year of publication, country of the study, target population, original research (yes, no), RS approach (content-based, collaborative, hybrid, other), type of intervention, inclusion of a theoretical model (yes, no) and type of interface (i.e. web, mobile, other). Content-based filtering is an approach used to recommend items that are similar to items the user has liked in the past. 25 The collaborative approach requires the users to express their preferences by rating items. 25 Hybrid refers to the use of a combination of content-based and collaborative techniques. 26 ‘Other’ refers to RSs that do not fall into the three above-mentioned categories. The provision of health recommendations incorporates feedback used by the system to provide recommendations (i.e. metadata, explicit feedback, implicit feedback, other) and type (of recommendation) (i.e. messages, videos, doctors, other) and includes a description of how the system provides health recommendations. Metadata are the human or computer-assisted content coding provided to an item; these keywords are then matched to the preferences of the user. 18 For instance, when an item is connected to several keywords (metadata), and to a user-created baseline profile to indicate who they are and what type of items they prefer, the filtering system then calculates which metadata and user preferences match best. 27 When recommendations are based on other similar users, the system could ask users to rate the recommended items (explicit feedback) 28 to learn how to best match recommendations to users, while the use of implicit feedback means that user feedback is extracted from user behaviour. 19 User experience included the potential impact of RSs on efficiency, effectiveness, trustworthiness, enjoyment, active trust and e-loyalty. Extracted data are presented in tables and summarised in the text.
Results
The search led to 1184 retrieved articles, of which 42 met the inclusion criteria after the title and abstract were screened. After the full-text screening, 26 articles were included in this study for data extraction.
General RS characteristics
Various approaches of RSs were used in the interventions; these are shown in Table 1. One article (4% of the total) reported an RS using content-based filtering. Five articles (19%) reported collaborative filtering. Eight articles (31%) reported a hybrid approach that involved both content-based and collaborative filtering. Seven articles (27%) used other approaches that do not belong to the above-mentioned filtering methods, including multimodal hybrid reasoning; the fuzzy integer nonlinear programming-ordered weighted average approach (FINLP-OWA), the knowledge and content-based approach, unsupervised ranking aggregation, episode mining, ensemble-learning models and case-based) (detailed in the original articles). Last, five articles (19%) did not report the specific approach used. The majority of the interventions focus on generic health promotion (n = 12, 46%); they provide health education and promote healthy behaviour. Six studies (23%) focused on the prevention of diseases, such as nutritional and weight loss interventions. Seven studies (27%) focused on the relief of disease or pain, such as relieving lower back pain. One article (4%) focused on predicting the side effects of drugs.
General recommender system characteristics.

USA: United States of America.
aUsed with hubs and authority approach.
bUses rule-, case-, and preference-based filtering
cUses item- and user-based filtering.
dUses content-based and collaborative filtering.
eFuzzy integer nonlinear programming-ordered weighted average approach.
fTag-based matrix factorisation.
gGeneric public health.
hDrug side effect.
iElderly.
jCaregivers of chronic patients.
kAdolescents and young adults.
lMirror.
mFitness clubs, doctors, email.
nSocial cognitive theory.
oTranstheoretical model.
pTheory of reasoned action.
In most studies, the target population was patients (n = 12, 46%), while five articles (19%) targeted the general public, two articles (8%) targeted healthy adults, and three articles (12%) targeted another population, such as the elderly or young adolescents; in four articles (15%) the target population was not stated. The interface used for 14 articles (53%) is the web, for eight articles (31%) mobile phones, two articles (8%) used other interfaces, such as doctors and email, and for two articles (8%) the interface used was not reported. Thirteen of the studies (50%) originated in Europe, five studies (19%) in the United States, and five studies (19%) in Asia. Two studies (8%) did not report the country of origin, and one study (4%) originated in Australia and Asia. Regarding the inclusion of original research, 18 articles (69%) were identified as original research, while three articles (12%) were not and five articles (19%) were classified as other. Only three (12%) of the included studies mentioned the inclusion of theoretical models, while 19 articles (73%) did not; in four articles (15%) this was not applicable as the article was either a review or a theoretical paper that discussed the application of a type of RS.
Health recommendations
A description of how the system provides health recommendations, the feedback method used (explicit or implicit) and the type of recommendation provided is detailed in Table 2. All 26 articles (100%) provided a description of how health recommendations were given. Fifteen articles (58%) did not specify the type of feedback their RS gathered to provide recommendations and were indicated as NR. Of the remaining 11 articles (42%), some RSs used more than one type of collected feedback. Nine articles (47%) mentioned the use of metadata, six articles (32%) reported explicit feedback (feedback supplied directly by the user) and four articles (21%) reported implicit feedback. Regarding the type of recommendations, the majority of RSs recommended messages (n = 15, 57%), while three studies (19%) reported medical providers as recommendations; these were doctors, clinics and hospitals. Recommendations defined as ‘other’ (n = 6, 19%) included recipes, alternative coping strategies and sharing information regarding peers who have the same disease diagnosis; two studies (8%) did not report the type of recommendation.
Provision of health recommendations.
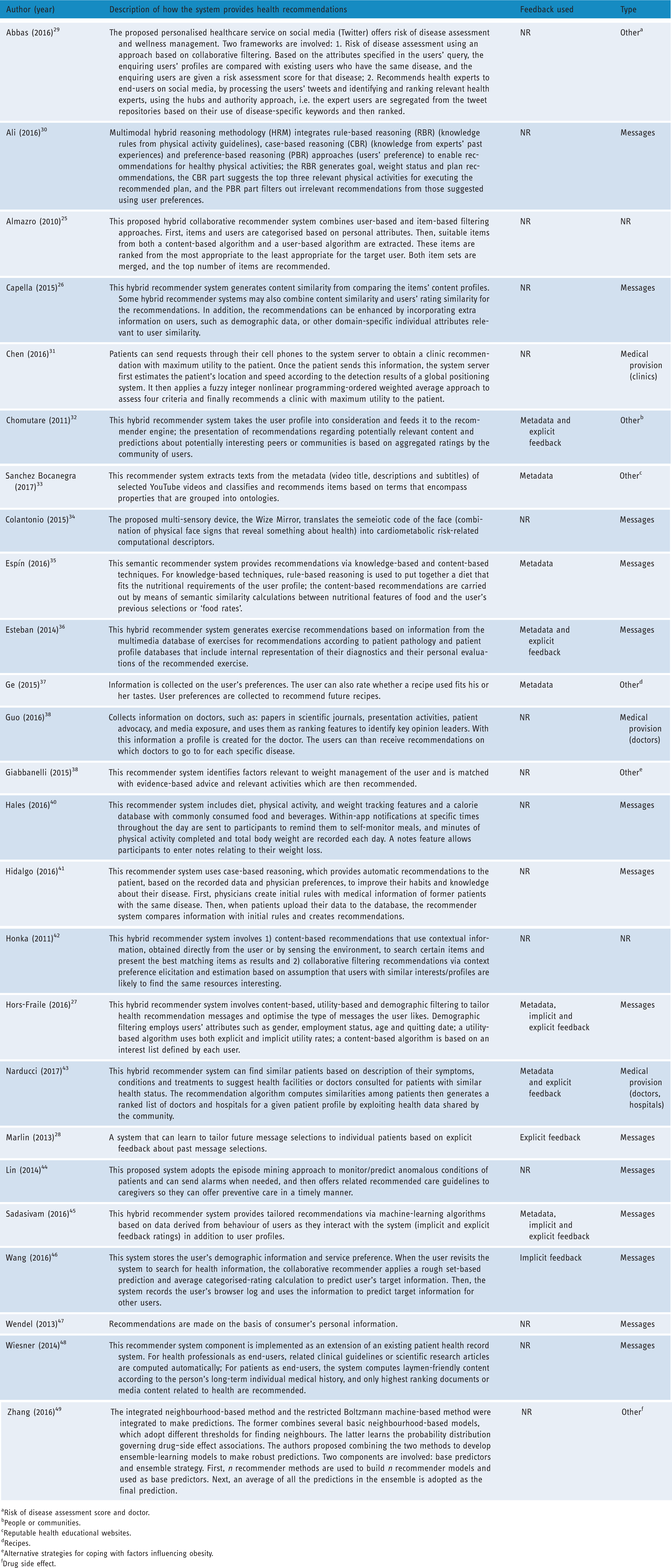
aRisk of disease assessment score and doctor.
bPeople or communities.
cReputable health educational websites.
dRecipes.
eAlternative strategies for coping with factors influencing obesity.
fDrug side effect.
Provision of health recommendations and how the user experience may be enhanced
The potential effect of RSs on the user experience was extracted from the studies, using the constructs of the user-experience model: efficiency, effectiveness, trustworthiness, enjoyment and active trust. Table 3 depicts for each study whether there is a potential effect on each construct of user experience. No potential effects were identified for active trust.
Potential effect of the recommender system on user experience.

The potential effects on efficiency, effectiveness, trustworthiness and enjoyment are detailed as follows. We have mapped the features of different types of RSs onto the constructs of the user-experience model to provide an understanding of how these features uniquely enhance the user experience and may ultimately lead to e-loyalty, or usage. The potential advantages of different types of RSs in relation to each construct are presented below.
Efficiency
Efficiency refers to the user’s easy search of and access to the information provided. 21 All the RSs demonstrated in the extracted articles show potential to enhance efficiency by filtering out the information that does not fit the user’s profile and attributes, and providing only a limited amount of recommendations, thus minimising information overload for the users. For example, Sancez Bocanegra and colleagues 33 proposed a content-based approach that matched users to health educational websites based on the metadata descriptions of the selected health videos that the user watched. Content-based filtering has also been used in combination with knowledge-based filtering to provide refined nutritional information for the elderly in two algorithm steps; the first step was via knowledge-based recommendation to identify nutritional requirements through the user’s profile, or other knowledge about the user (e.g. demographics, environmental factors, culture, religion) and the next step was, via content-based recommendation, to personalise the diet obtained, by means of semantic similarity calculations between the nutritional features of food and the user’s past ratings of the recommended food. The combination of several reasoning techniques is also evident in the multimodal hybrid reasoning methodology developed by Ali and colleagues. 30 This RS involved rule-based reasoning (using knowledge rules from physical activity guidelines), case-based reasoning (knowledge from health experts’ successful cases from the past) and preference-based reasoning approaches (user’s preference) to provide tailored recommendations for healthy physical activities. Hidalgo et al 41 used case-based reasoning to provide medical information to diabetic patients based on patient data and physician preferences from the medical information; thus only the most relevant information was recommended. Another technique for increasing efficiency is collaborative filtering;25,28,29,46 this makes recommendations based on user-user similarities, such as similarities in user demographics (e.g. Abbas et al., 2016 29 ) and history of ratings of recommended items (e.g. Marlin et al., 2013 28 ), and results in useful recommendations. Moreover, tag-based matrix factorisation is type of collaborative filtering that has been applied to gather information both on a user’s ratings and tags of the preferred attributes of food to provide refined recommendations of recipes. 37
Several extracted articles outlined a hybrid RS that combined content- based and collaborative filtering techniques; a hybrid system has the potential to enhance efficiency, as only the top-ranked most applicable items as well as similar items that are matched on metadata of items preferred in the past are recommended to the target user.19,26,27,32,36,42,43,45 For example, in the study by Esteban and colleagues, 36 the RS incorporated information from databases of exercise recommendations and patient pathology, as well as users’ ratings on the recommended exercises they completed, and was thus able to generate a limited but tailored number of exercises for the prevention of lower back pain problems. Similarly, in the study by Narducci et al., 43 the hybrid RS recommended only the top-ranked physicians and health facilities for a patient by integrating information from his or her personal health record and ratings of health facilities or doctors consulted by other patients with a similar health status. This technique has also been demonstrated in RSs that support smoking cessation.19,27,45
Other approaches of RSs that increase efficiency by providing refined recommendations for maximum utility by the users include: a) FINLP-OWA, 31 which integrates a variety of information sources; b) an unsupervised ranking aggregation approach that takes multiple recommendation criteria into consideration 38 ; c) an episode-mining approach that predicts/monitors abnormal conditions of patients by extracting information from personal medical records 44 and d) ensemble-learning models that work with the average over several prediction models to make a robust prediction about drug side effects. 49
Effectiveness
Effectiveness refers to the quality and the relevance of the information recommended to the users. 21 In general, the different types of approaches used in RSs have the potential for effectiveness by providing only relevant recommendations for each user. For example, Sanchez Bocanegra and colleagues 33 used content-based filtering to enrich health information with additional content that has metadata that were matched with that of the health videos that the user watched, thus providing relevant information that the user might be interested in. In an RS that provides nutritional information for the elderly, the recommendation was further personalised when content-based filtering was used as a subsequent step after knowledge-based filtering; that is, after identifying nutritional requirements through the ontological user profile, recommendations were then made based on the user’s preferred food. 35 RSs that use collaborative filtering take into account feedback information collected from a community of users, thus enhancing the effectiveness or relevance of the recommendation. One type of collaborative filtering, known as user-based filtering, suggests an item to a user based on the co-ratings assigned to that item by other users who are ‘similar’ in taste. 26 For example, Abbas and colleagues 29 proposed a user-based technique for suggesting a risk assessment score that compares key attributes that affect the presence of a disease between the enquiring patients and those of other patients with the same disease, such as age, gender, ethnicity, weight, height, family disease history and other commonly observed predictors for the disease. As such, the risk assessment score is highly relevant to the condition of patient, as a variety of aspects related to disease susceptibility are considered according to the profiles of other similar patients. In some articles, user-based collaborative filtering techniques adopted users’ item ratings to achieve a higher predictive accuracy, as in research conducted by Guo and colleagues, 38 in which users’ implicit ratings (browser logs) were used to make predictions about the enquiring user’s preferred and relevant health information, and research by Marlin et al., 28 in which the most relevant smoking-cessation support messages were provided based on users’ explicit ratings of their preferences regarding the motivational value of the messages. Moreover, Almazro and colleagues 25 proposed a hybrid collaborative RS combining both user-based and item-based approaches. The latter approach can predict items that are most similar to the ones that have received ratings from the target user, based on the patterns of co-ratings provided by other users. As indicated by the authors, this RS that employs both item-based and user-based filtering may have the advantage in suggesting the most accurate items to users.
Furthermore, the RSs that utilise different approaches such as combining content-based and collaborative filtering,19,26,27,32,36,42,43,45 combining rule-, case-, and preference-based reasoning, 30 and combining knowledge-based and content-based filtering 35 may optimise recommendation accuracy by integrating different sources of information.25,26,43 For instance, a hybrid (content-based and collaborative) RS for patients with lower back pain problems provided exercise recommendations that were appropriate for the patients by making predictions based on a community of users’ explicit ratings of the recommended exercises. 36 A similar approach has been employed in RSs that sent relevant messages for smoking cessation,19,27,45 recommended peers and communities to support diabetic patients 32 and recommended physicians and health facilities that have been consulted by other patients with similar health status. 43
Other filtering methods that enhance the relevance and accuracy of the recommendation include a) the FINLP-OWA approach that made recommendations of clinics by taking into consideration four patient concerns: no-waiting, the shortest path to a clinic, preference for a clinic and preference for a doctor, which are highly relevant when seeking health care; 31 b) the unsupervised ranking aggregation approach, which integrated multiple sources of medical-related data to enhance the relevance of the recommendations; 38 c) the episode mining approach, which provided real-time guidelines for care that were relevant to patients’ current condition 44 and d) the ensemble-learning models that utilised a diversity of base predictors to enhance the accuracy of the recommendations. 49
Enjoyment
Enjoyment refers to the user’s positive affective perceptions about the recommended items. 21 RSs that provide recommendations based on a user’s preference may enhance their affective perception, as the users are invited to provide feedback on or rate the items that have been recommended to them. The information on the user feedback is used to shape future recommendations so they may be more adapted to user needs or interests; this has the potential to promote positive affective experience with the system, i.e. enjoyment of use. In a content-based RS that recommends recipes, the user was given the option to rate whether the recipe fits his or her taste, so future recommendations are matched with the metadata of the recipe(s) that the user liked in the past. 37 RSs that use collaborative filtering or combine the collaborative filtering method with another (in cases of hybrid RSs) can potentially enhance the user’s enjoyment by taking into consideration similarity with their explicit or implicit ratings of a recommended item. For example, RSs that used collaborative filtering to send smoking cessation support messages invited users to provide ratings of four different aspects of the messages: influence, emotional response, relevance and preference. 28 Similarly, in several hybrid (content-based and collaborative filtering) RSs, users were requested to rate recommended content that could enhance the self-management of diabetes, including vital health information about diabetes and information about relevant supportive peers and doctors, 32 other users were asked to rate recommendations for exercises to combat lower back problems 36 and others to rate smoking-cessation support messages, based on their preferences.19,27,45 Using algorithms, the ratings collected by the collaborative filtering method can be fed back to the RSs, and the user profiles can be updated, which may enhance the affective experience of users, as the recommendations they receive will fit their preferences.
Trustworthiness
Trustworthiness is the believability of the provided information on the part of the users and refers to both cognitive and affective perceptions: It is based on a cognitive process (e.g. rational reasons) and an emotional base (e.g. a strong positive affect for the trustee). 21 More specifically, three articles suggested an approach used in RSs that may potentially enhance trustworthiness, that is, knowing that other people like himself or herself who are also users of the system have benefited from the intervention. The social norm of usage may create a rational cognitive foundation that the system is trustworthy because of other users’ engagement, and foster a sense of trust in the system. In a content-based RS that targeted social support for weight loss, one of the features was that messages could be sent from frequent app users to re-engage infrequent app users who were matched via the system. In addition, a newsfeed was developed for users to view the progress of other users’ weight loss, with the ability to send others encouragement for achieving these goals. 40 The encouragement from similar peers and seeing others’ progress may enhance the believability of the information provided by the system. In a hybrid (content-based and collaborative) RS that suggested other diabetic patients similar to the target user to promote interaction with among peers, the recommendation was inspired by the ‘Patients-Like-Me’ concept, so users could recognise other users of the system who were similar to themselves, to feel supported. 32 In another hybrid (content-based and collaborative) RS that recommended physicians and health facilities, users were able to find the most similar patients, see how their disease was treated by professionals, and receive suggestions for the treatment of their own disease. 43 These articles suggest that interactions with other users, as well as having others’ information, can improve the understanding of one’s own health condition, and may increase the believability of the recommendations received, because of peer norm influence, along with enhancing users’ perception of the trustworthiness of the RSs.
Discussion
This study illustrates the potential for using RSs in supporting and enhancing computer-tailored digital health interventions. More specifically, we built on the results of a previous scoping review 18 that contributed to the various types of recommender systems and the feedback types, by offering understanding of the underlying mechanisms that enhance the usage of computer-tailored digital health programs.
First, we explored how RSs provide health recommendations, by extracting the general RS characteristics and detailing how the (proposed) RS in each study provided health recommendations. The majority reported original research and originated in Europe. Most of the identified health-directed RSs were hybrid types, mostly combining content-based filtering with collaborative filtering. In line with a previous scoping review on health-directed RSs, most of these interventions focus on generic health promotion, followed by disease relief and prevention. 18 The majority of the RS programs used the web as interface, followed by the mobile platform, targeting mostly patients and the general public. This seems consistent with the common delivery modes and targeted users of tailored digital health programs, such as the Dutch tailored intervention for physical activity. 50 As the previous scoping review on health-directed RSs showed, the theoretical grounding of the programs was scarcely reported. 18 However, we found that three studies did include theoretical theories for designing the system and messages; these were social cognitive theory, 51 the transtheoretical model 52 and the theory of reasoned action. 53 For instance, the transtheoretical model, which states that behaviour change occurs in five phases (i.e. pre-contemplation, contemplation, preparation, action and maintenance), was integrated in a hybrid RS. 27 Based on a survey assessing the phase that a user is in, the frequency of the delivered messages was selected. 27 This illustrates that the integration of behavioural change theories in RSs can have further merits.
Second, the provision of the health recommendations was detailed. In line with the previous scoping review on the health-directed RS, messages were the most used type of item for making recommendations. Yet, the details of how these messages were drafted, and to what extent they were based on theories or behavioural change techniques, is underreported.18,29 It is therefore recommended that future studies report on the design of messages to understand the underlying mechanism regarding why specific RSs are or are not effective in eliciting behaviour change. Regarding the feedback method used by the RS, most studies used metadata and explicit feedback.
Third, this study explored how RSs may potentially link to the constructs of the user experience. 21 While all approaches potentially have advantages for providing relevant recommendations and preventing information overload, i.e. effectiveness and efficiency, respectively, we found that knowledge-based filtering may be more appropriate in the context of tailored digital health programs. Knowledge-based filtering works by predicting items based on explicit knowledge about users (e.g. via questionnaires), and is therefore able to predict items that are relevant and/or tailored to the user’s interest, 35 thus enhancing the efficiency and effectiveness of the recommendation. This approach has been applied as an initial step in RSs to rule out all information that doesn’t match user’s ‘preferences’. 35 However it differs from content-based filtering, as the latter is useful for capturing the nuances in objective features of items themselves, i.e. matching the metadata of one’s preferred item to that of the recommended item. 26 This is not appropriate for digital health programs if the aim is to provide personalised information, as opposed to information that has similarities in metafeatures.
We found that for some RSs that use user-based collaborative filtering, users are able to explicitly rate the items that have been recommended to them previously, and the aggregated ratings by the community of users with similar profiles or attributes are machine-calculated to predict top-ranked items for the target user. This suggests that demographic filtering can be applied in a user-based collaborative RS to incorporate extra information on user similarity to enhance the relevance of the recommendations. It is also possible to incorporate the behavioural similarity of user-system interaction between users (implicit feedback) to predict what will be preferred in the future for the target use.26,38 Collaborative filtering methods not only enhance the ease of retrieving user’s information, but also enhance users’ enjoyment, as their preferences are considered through implicit and explicit ratings. Moreover, several studies have shown relevance in the items recommended using collaborative filtering. For example, Marlin et al. 28 found that more users have positive opinions about smoking-cessation support messages if the recommendations are based on users’ past ratings. Similarly, in a collaborative RS that collects implicit feedback (from users’ browser logs) to predict for the information provided to other users, users reported positively in the domains of satisfaction, expectation-confirmation, perceived trust, perceived usefulness, and perceived value of the system. 38 One distinct feature of collaborative filtering is that as new data about the users are collected, the RS is able to adjust recommendations adapted to real-time user feedback and thus remain relevant and engaging. 19
Taken together, we propose a hybrid RS that uses a knowledge-based method as the first step, and a user-user collaborative method using demographic filtering in the second step to provide health recommendations in computer-tailored digital health interventions. This may have the potential to enhance user experience via efficiency, effectiveness, trustworthiness and enjoyment. In terms of efficiency, both knowledge-based and collaborative filtering methods are able to provide convenient access to recommendations for the users as the recommendations are filtered and prioritised, opposing information overload. The use of both filtering methods are further able to refine the recommendations based on user profiles, preferences and the ratings of other similar users, and thus assist users when they search for reliable information. Moreover, different recommendation methods can be fused to achieve better relevance of the recommendations, 26 i.e. effectiveness. By incorporating the collaborative filtering component, recommendations are adapted to the explicit and/or implicit ratings of other users, along with information gathered from the user profiles. 45 As such, the hybrid RS, using knowledge-based and collaborative filtering, is able to identify relevant items that suit the user’s profile as one basis for predicting future choices, and, drawing from comparison with other similar users, incorporate individual variation in what items matter more and for whom. 26 This may enhance the relevance of the recommendations as information from a variety of sources is used to make a robust prediction. Furthermore, expressing preferences by rating recommended items (one of the features of collaborative filtering) may enhance the user’s affective experiences or enjoyment, as their autonomy is respected and the recommendations are adapted to their interests. Last, a user’s preference may change over time; therefore up-to-date recommendations are essential for the effectiveness of information delivered. Incorporating collaborative filtering has the advantage of adapting to multiple users who are similar to the target user; moreover, as more data become available over time, this type of RS generally improves in performance. 26 The collaborative component of the hybrid RS is able to strengthen future predictions as more user feedback is gathered into the system. 25
According to the user experience model, 21 efficiency (ease of use), effectiveness (relevance) and enjoyment are determinants of e-loyalty, or active usage of a digital health program. In addition, several articles note that a feature of their RS enables users to compare their information with other users to promote interaction for motivation and support purposes.32,40 This element may be incorporated in our proposed hybrid RS to enhance the perceived trustworthiness of the system, or the believability of the information, as users can see similar users who are also utilising the system, thus a peer norm. It has been proposed that perception both of effectiveness and trustworthiness are related to users’ behaviours in acting on the information provided (active trust), and that this is the mechanism that leads to e-loyalty. 21 RSs may thus potentially influence the usage of digital health programs via enhancing the efficiency, effectiveness, enjoyment and trustworthiness of the intervention.
In conclusion, our scoping review suggests that supporting traditional tailoring with an RS mechanism may have added value in light of enhancing the user experience. In traditional (computer-) tailored digital health, users are asked to provide information via questionnaires (e.g. rating on a Likert scale to what extent the user agrees with specific statements). Based on these responses, or a calculated score of multiple items, the tailored program provides a personalised message. In addition, traditional programs have often been personalised and adapted to the user’s demographics (e.g. providing information to pregnant women about the consequences of smoking for the unborn child20,54). This mechanism closely links to the filtering method based on explicit knowledge about the users, i.e. knowledge-based filtering, which can be performed by collecting personal information, such as preferences and demographics provided by the user via a questionnaire. Like traditional tailored digital health, knowledge-based filtering is able to discard irrelevant messages based on the information gathered as user data. 35 As such, the recommendations are personalised and only the set of information that fits the user’s profile is provided to the user. It has been argued that this personalisation in tailoring leads to enhanced relevance as perceived by the user, in turn promoting user engagement and information processing. 20 Yet, although shown to be effective, these tailored programs are still suboptimally used. 10 Thus, an RS that relies solely on knowledge-based filtering may not add value to tailored digital health because it doesn’t have additional features that may potentially enhance the determinants to e-loyalty. Nevertheless, it is likely that the hybrid RS, incorporating a collaborative approach with demographic filtering techniques as a second step to knowledge-based filtering, may have the potential to enhance the user experience in terms of efficiency, effectiveness and enjoyment. For instance, adding user-based collaborative filtering to the program, based on the ratings of the filtered messages (i.e. items tailored to the user’s responses) by users who are similar in demographic character, the program could predict and provide calculated top-ranked items (based on user similarity and ratings for each message) for the target user. For instance, from 50 potential health messages, 30 messages are filtered out by knowledge-based filtering (based on a questionnaire assessing demographics and motivational beliefs regarding behavioural change). Instead of presenting the 30 remaining personalised messages, the user-based collaborative filtering allows the system to rank the top messages based on user ratings and provide the user with the top 10 most important messages. The use of the demographic-filtering technique can identify users who have a similar demographic profile; this may be important for health interventions because of potential cross-cultural variations. In sum, our proposed hybrid RS using layered filtering that has knowledge-based and collaborative filtering, in subsequent steps, could potentially enhance the efficiency (e.g. by reducing the information burden), effectiveness (e.g. the most relevant messages are presented) and enjoyment (e.g. the remaining messages are most preferred, according to their explicit ratings). When the system allows users to observe the ratings of other users, such a hybrid RS may also enhance the perceived trustworthiness of the messages. This feature, however, should be applied with sensitivity, because of the confidentiality of the user’s information. This study illustrates how RSs may have the potential to bring (computer-) tailored digital health forward by enhancing the user experience of such programs.
Although our study was able to identify the strength of a hybrid RS and its potential application in digital health interventions, it is not without limitations. First, only two databases were used to conduct a scoping review, to analyse journal articles regarding RSs; this may have somewhat limited the search. Future studies could incorporate other databases as well as grey literature to maximise the inclusion of potentially informative literature. Second, we applied the user experience model in different types of RSs to understand their potential to enhance e-loyalty in digital health interventions. 21 We found that not all the studies explicitly outlined the methods of feedback used in the RS. For example, some articles on RSs using collaborative filtering did not report explicit feedback gathered from the users, yet it is possible that explicit feedback was used, as it is often an essential feature of the collaborative filtering technique that we suggest may enhance user’s enjoyment, as their preferences are taken into consideration. Therefore, the information on the method of feedback that was not reported in the identified articles could not be analysed with regard to the user experience constructs. Third, not all articles stated the specific approach that they used in their RS to provide health recommendations; owing to this lack of reporting, we were unable to delineate the type of these RS. Fourth, the current user experience model has not been extensively validated, and longitudinal studies are needed to show that e-loyalty predicts actual usage and change of health behaviours.
Last, while we described different techniques used by RSs to increase efficiency, effectiveness, enjoyment and trustworthiness, most of the studies did not explicitly assess and evaluate the effects of the RS they were describing on these user experience constructs in their target population because they did not use a specific theory with regard to user experience. Therefore, the results of our study on how features of RSs are linked to user experiences need to be validated in future studies, and the current results in our study should be interpreted with caution. Future research on RSs and their applications for enhancing e-loyalty can profit from including empirical assessments of user experience constructs, as the objectives of RS techniques do not necessarily result in the intended effects.
Conclusions
Tailored digital health programs have been found to be suboptimally used because of limited user engagement and experience; this is reflected in the lack of (correct) usage, and high dropout rates. Although the application of RSs remains limited in the health sector, it may have the potential to enhance the usage of tailored digital health interventions. In particular, hybrid RSs that combine knowledge-based and collaborative filtering techniques could potentially lead to improved e-loyalty in traditional computer-tailored interventions by enhancing users’ perceptions of efficiency, effectiveness, enjoyment and trustworthiness. A hybrid RS has the unique advantage of further refining recommended items based on user similarity, and is able to adapt to users’ preferences in real time. It may also be important to incorporate behavioural change theories in computer-tailored interventions using hybrid RSs to optimise the benefits of such interventions for health promotion.
Footnotes
Acknowledgements
We are indebted to Rixt Zijlstra for her valuable feedback on the first draft of the manuscript, and to Santiago Hors-Fraile for his input regarding the RS approaches.
Conflicts of interest
None declared.
Contributorship
K.L.C. and D.D. designed and planned the study. D.D. screened titles and abstracts, and D.D. and X.S. independently screened full texts and extracted data. K.L.C., D.D. and X.S. produced the first draft of the manuscript. Different versions of the manuscript were reviewed and conceptualised by all co-authors. All authors have read and approved the final manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Guarantor
K.L.C.
Peer review
This manuscript was reviewed by two reviewers, the authors have elected for these individuals to remain anonymous.