
Abstract
Research on telemedicine adoption often exhibits a fragmented approach, analyzing patients and healthcare professionals separately. This study addresses that gap by jointly assessing the acceptance of telemedicine in Spain, a country characterized by a low conversion rate from intention to use to actual adoption. An extended UTAUT2 model was applied, incorporating contextual variables such as Trust, Personal Innovativeness, Word of Mouth, and Novelty. Based on a cross-sectional quantitative design with 684 participants (203 professionals and 481 patients), the model demonstrated a high explanatory power for usage intention (adjusted R2 = 0.800). The findings confirm that Performance Expectancy, Hedonic Motivation, and Habit are significant predictors for both groups. Likewise, the contextual variables Trust, Personal Innovativeness, and Novelty had a positive and significant impact. In contrast, Effort Expectancy, Social Influence, and Facilitating Conditions were not significant, while Perceived Price Value showed a negative effect. A multi-group analysis revealed that Performance Expectancy and Trust exert a significantly greater influence on usage intention among healthcare professionals. These findings validate the extended model in healthcare contexts with dual user profiles, challenge the universal applicability of certain UTAUT2 constructs in digitally mature environments, and underscore the need for differentiated implementation strategies based on user profile.
1. Introduction
In recent years, the healthcare sector has been undergoing a profound digital transformation. 1 Within this process, telemedicine has emerged as a key component that includes routine practices such as video consultations and secure messaging, as well as more advanced procedures such as telesurgery. It is now regarded as a versatile and adaptable element of the broader eHealth ecosystem.2,3 Empirical studies consistently highlight benefits such as reduced travel and cost, improved operational efficiency, shorter waiting times, and the possibility of remote monitoring. 4
The COVID-19 pandemic represented a turning point, since telemedicine became an essential channel to maintain continuity of care when face-to-face encounters were restricted. Its usefulness was especially evident in sensitive and communication-intensive areas such as oncology, palliative care, and mental health support.5,6 In the post-pandemic period, telemedicine has remained embedded in routine clinical practice and has expanded into additional specialties, including dermatology and specialized palliative care.7,8 This evolution reflects not only a rapid organizational adaptation but also a growing familiarity with mediated communication between patients and healthcare professionals.
Despite these advances, telemedicine is still in an early or uneven phase of implementation in many health systems. 9 Its adoption depends on the balance between perceived benefits and a set of persistent barriers. These include limitations in performing physical examinations at a distance, 10 the need for reliable technological infrastructure and the persistence of digital literacy gaps,11,12 and resistance to organizational and professional change.
From a communication perspective, concerns about emotional distance and reduced warmth in teleconsultations, described in fields such as neuro-oncology and general practice, are particularly relevant because they may hinder trust-building within the patient–physician relationship.13–15 In this sense, trust becomes especially sensitive to continuity with known professionals, technical quality and the absence of unexpected costs. 16 Recent work shows that specific features of online physician-patient communication are closely linked to care quality: patient-centered communication, adequate consultation time and opportunities to express concerns are associated with more accurate diagnoses, clearer prescriptions, higher satisfaction and stronger continuance intention in e-consults and telemedicine visits.17–19
Qualitative studies also indicate that virtual encounters require professionals to develop specific skills of active listening and interpretation of facial expressions and gestures to sustain mutual understanding. 20 At the same time, many clinicians report little or no formal training in telehealth etiquette and learn to manage their online behavior and consultation environment by trial and error, which reinforces the need for explicit guidance on performance, environment and privacy in virtual care. 21 Communication during teleconsultations often lacks clear guidelines and is strongly conditioned by patients’ health literacy and familiarity with digital technologies, which may affect how information is exchanged and understood. 22 Both patients and professionals also face a learning curve when integrating new digital channels into everyday consultation and follow-up routines. 23 For patients, these challenges may hinder access, understanding, communication, and trust during remote encounters, whereas for healthcare professionals they may increase communicative demands, require new digital and relational skills, and complicate the integration of telemedicine into routine care.20–22
An important question for research on communication in healthcare is how telemedicine is perceived on both sides of the screen, because clinicians and patients jointly construct the meaning, value, and legitimacy of remote encounters. However, most empirical work has examined these groups separately, 24 which produces a fragmented view and makes it difficult to systematically compare their expectations and concerns. 25 Although some recent studies have included both patients and professionals,26,27 they have usually focused on specific clinical contexts or have not applied a shared theoretical framework, which limits direct comparison between both groups. As a result, evidence remains limited regarding which determinants of telemedicine acceptance are common to patients and healthcare professionals and which are role-specific.25,28 This gap limits a comprehensive understanding of communication dynamics around telemedicine and restricts the design of implementation strategies that speak simultaneously to patient needs and professional concerns.
The objective of this study is to assess telemedicine acceptance in an integrated manner, considering both patient and healthcare professional perspectives, and to identify common drivers and specific barriers to its use. The analysis is grounded in the UTAUT2 model proposed by Venkatesh et al., which has shown strong explanatory power in user-centric technology contexts. 29 Given the specific features of clinical and communication environments, the model is extended with variables that recent digital health research have highlighted as especially relevant. These include trust in technology and providers, 30 individual willingness to experiment with new digital solutions,31,32 the influence of word of mouth and informal recommendations in online medical consultation, 33 and perceived technological novelty. 34 Previous work has stressed the need to incorporate such contextual factors in order to better capture the complexity of clinical settings. 35 In this study, the extended model is used to compare two groups with clearly differentiated roles and expectations regarding the use of telemedicine, with the aim of informing more nuanced and communication-oriented implementation strategies.
2. Theoretical framework
In the field of health informatics, technology acceptance models have been widely used to explain how users decide whether to engage with new tools and channels. The Technology Acceptance Model (TAM) introduced perceived usefulness and perceived ease of use as central drivers of attitudes toward technology. 36 The Unified Theory of Acceptance and Use of Technology (UTAUT) integrated eight prior frameworks into a model with four core determinants of behavior (performance expectancy, effort expectancy, social influence and facilitating conditions) moderated by age, gender, experience and voluntariness of use. 37 UTAUT2 extended this framework to consumer and everyday-use settings by adding hedonic motivation, price value and habit, and is therefore particularly suited to contexts in which individuals, rather than organizations, decide whether or not to adopt a technology. 29
Other models, such as TAM3, Task-Technology Fit, the Health Belief Model and the Technology Readiness Index, have also been applied to health-related technologies.38–41 However, these approaches either focus on specific perceptual mechanisms or emphasize structural fit between tasks and systems. For decisions about using telemedicine as a regular communication channel, UTAUT2 offers a more comprehensive structure that combines instrumental beliefs, affective responses, value, habit and contextual conditions at the individual level, which makes it especially appropriate for simultaneously modeling the adoption decisions of patients and healthcare professionals.
Empirical evidence in digital health supports this choice. Recent studies have used UTAUT2 to examine telemedicine and mHealth adoption, often extending the original constructs with context-specific variables such as digital literacy, perceived threat or trust in technology.35,42–45 In parallel, conceptual work on telehealth has emphasized that acceptance is closely linked to relational and ethical dimensions, including autonomy support through offering choices, providing clear justifications and conveying empathy in digital encounters. 46 Building on this work, the present study applies an extended UTAUT2 model that incorporates trust, personal innovativeness, perceived novelty and word of mouth in a dual-user design that compares patients and healthcare professionals within a shared theoretical framework.
2.1. Conceptual framework, theoretical hypotheses and research model
Based on the extended UTAUT2 framework and recent digital health research, we propose a conceptual model in which performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivation, habit, trust, personal innovativeness, word of mouth, and perceived novelty are specified as exogenous variables for both patients and healthcare professionals. Although price value is conceptually more salient on the patient side, in this study it was examined in both groups in order to assess whether cost-benefit considerations also contribute to telemedicine adoption among healthcare professionals. These variables represent the main contributors to telemedicine adoption examined in this study across patients and healthcare professionals. Behavioral intention (BI) is specified as the main endogenous variable linking these predictors to actual use (USE), which is modeled as the final outcome variable. In addition, facilitating conditions and habit are specified as direct predictors of USE. The model is estimated for patients and healthcare professionals under a shared conceptual framework, allowing direct comparison between both groups.
2.1.1. Performance expectancy
Performance expectancy (PE) refers to the degree to which using telemedicine is perceived to improve clinical outcomes, efficiency or self-management. In UTAUT2 and telemedicine studies, PE consistently emerges as a core predictor of technology acceptance among both patients and professionals.29,45,47 It captures expectations about access, time saving and perceived quality of care in remote encounters. H1. Performance expectancy positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.2. Effort expectancy
Effort expectancy (EE) captures perceived ease of use. UTAUT2 posits that lower perceived effort facilitates technology acceptance, and several studies in telemedicine and eHealth confirm that simple and intuitive interfaces are associated with higher intention to use.29,48,49 H2. Effort expectancy positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.3. Social influence
Social influence (SI) refers to the perceived pressure or encouragement from significant others, such as colleagues, family members or peers, to use a technology. Prior work shows that recommendations from trusted others can promote the adoption of telemedicine, especially in early diffusion stages or in uncertain situations.29,50,51 H3. Social influence positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.4. Facilitating conditions
Facilitating conditions (FC) denote the perceived availability of technical infrastructure, training and organizational support needed for telemedicine. In digital health contexts, FC have been linked to both intention and actual use, since they reduce practical barriers in remote consultations.29,49,52 H4a. Facilitating conditions positively influence the intention to use telemedicine among healthcare professionals and patients. H4b. Facilitating conditions positively influence the actual use of telemedicine among healthcare professionals and patients.
2.1.5. Hedonic motivation
Hedonic motivation (HM) reflects the enjoyment or positive affect experienced when using a technology. UTAUT2 assumes that pleasurable interaction experiences encourage adoption, and empirical studies show that perceiving telemedicine platforms as enjoyable and comfortable increases intention to use them.29,49,53 H5. Hedonic motivation positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.6. Price value
Price value (PV) reflects the perceived trade-off between the benefits of telemedicine and its economic or time costs.
29
In some healthcare settings, higher price value has been associated with greater intention to use telemedicine services, especially when users perceive savings in travel, waiting time or out-of-pocket expenses.42,54 Although this construct is theoretically more salient for patients, cost-benefit considerations may also be relevant for healthcare professionals, for example in relation to time efficiency and workflow optimization. Therefore, in this study Price Value was examined in both groups. H6. Price value positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.7. Habit
Habit (HB) denotes the extent to which telemedicine use has become automatic or routine as a result of prior experience.
29
Studies of mHealth and telemedicine show that users who have successfully integrated these tools into their daily routines are more likely to maintain and expand their use over time, both in terms of intention and actual behavior.43,44,47 H7a. Habit positively influences the intention to use telemedicine among healthcare professionals and patients. H7b. Habit positively influences the actual use of telemedicine among healthcare professionals and patients.
2.1.8. Trust
Trust refers to the perception that telemedicine systems and healthcare professionals are reliable, secure and act in the patient’s best interest.
55
In digital health, trust in technology and in providers is a central determinant of acceptance, particularly when personal data and high-stakes clinical decisions are involved.30,35,42,56 Recent evidence also shows that trust increases when patients receive telemedicine from a familiar professional, experience good technical quality and do not face unexpected additional costs.
16
Higher levels of trust tend to reduce perceived risk and increase willingness to engage in remote care. H8. Trust positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.9. Personal innovativeness
Personal innovativeness (PI) is a dispositional tendency to try out new technologies and experiment with novel digital solutions.
31
In the context of telemedicine and mHealth, more innovative patients and professionals display a higher propensity to adopt and continue using digital health tools, especially when they perceive them as useful and aligned with their needs.32,57,58 H9. Personal innovativeness positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.10. Word of mouth
Word of mouth (WOM) refers to informal communication and recommendations about services between individuals.
59
In telemedicine, positive experiences shared by other patients or professionals, both offline and through digital channels, can reduce uncertainty and shape intentions to try or continue using remote consultations.33,60 H10. Word of mouth positively influences the intention to use telemedicine among healthcare professionals and patients.
2.1.11. Novelty
Novelty (NOV) captures the extent to which telemedicine is perceived as new and different from traditional care. From an epistemic motivation perspective, novel stimuli can trigger curiosity and exploratory behavior.
61
Although novelty on its own does not guarantee sustained use, studies in digital health suggest that perceiving a service as innovative can enhance satisfaction and openness to experimenting with new modes of care when clear benefits are communicated.34,62 H11. Perceived novelty positively influences the intention to use telemedicine.
2.1.12. Behavioral intention
Finally, in line with UTAUT and a large body of technology adoption research, behavioral intention is expected to be the main proximal predictor of actual telemedicine use in both groups.37,63,64 H12. Behavioral intention positively influences the actual use of telemedicine.
Figure 1 presents the conceptual framework and research model tested in this study, including the exogenous variables, behavioral intention, and actual telemedicine use. Conceptual framework and research model.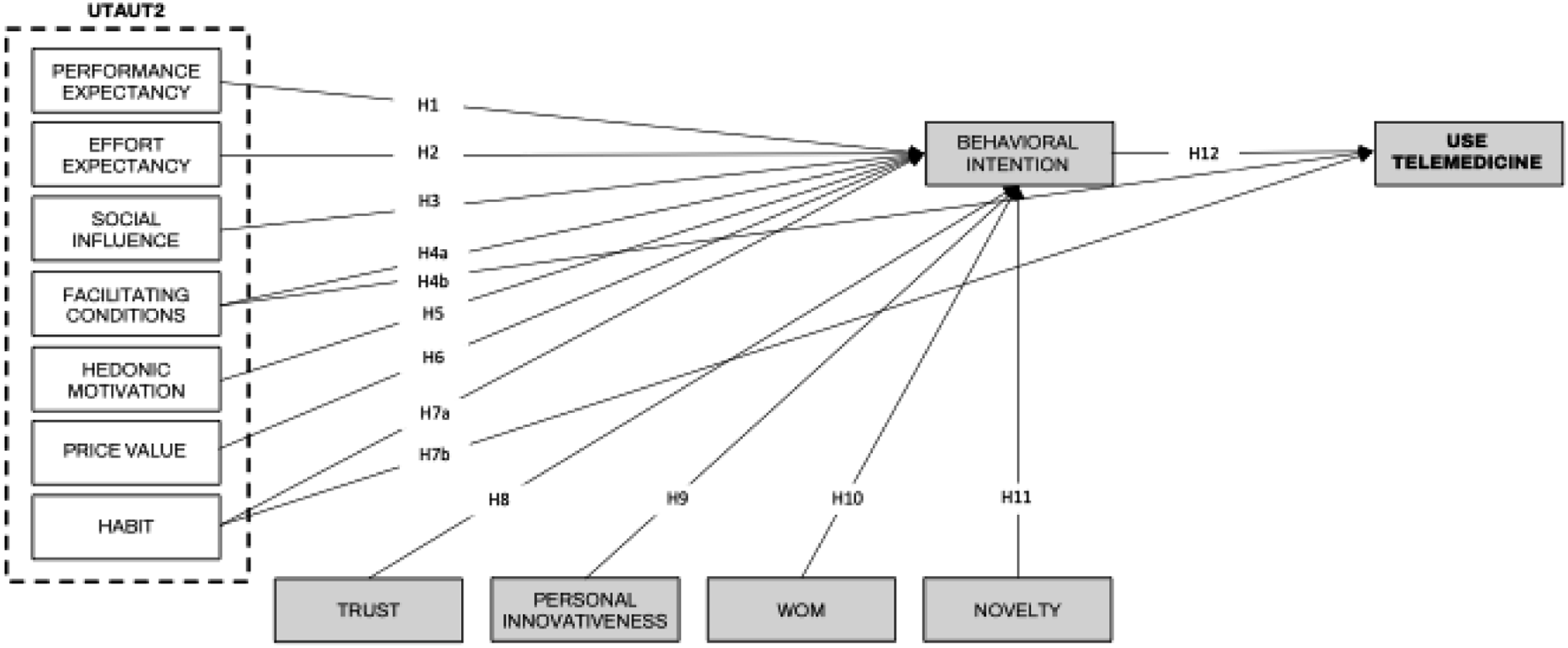
3. Methodology
3.1. Study design and context
This study adopts a cross-sectional quantitative approach based on the use of structured surveys, with the aim of analyzing the factors influencing telemedicine adoption in Spain. The research focuses on two key stakeholder groups: healthcare professionals and patients, in order to capture a comprehensive view of the phenomenon from both perspectives. The reporting of this cross-sectional study was guided by the STROBE statement for observational research.
Spain was selected as the context of analysis due to its low conversion rate from intention to use to actual adoption of telemedicine services, in comparison to countries such as the United States or Germany. 45 This gap is partly attributed to the absence of specific regulatory frameworks, which creates legal uncertainty among healthcare professionals. 65 Additionally, structural barriers such as the digital divide, sociocultural resistance, and cognitive limitations identified among certain patient profiles further justify the need for empirical studies adapted to the national context.65,66
3.2. Data collection instrument and validation
The data collection instrument consisted of a structured questionnaire comprising 45 items measured using a 7-point Likert scale, where 1 indicates “strongly disagree” and 7 indicates “strongly agree.” The items were adapted from previously validated scales in technology adoption studies, ensuring content validity and conceptual coherence, as recommended by Pillet et al. and Dwivedi et al.67,68 In addition, five sociodemographic questions were included, along with an initial screening question to determine whether the respondent was a healthcare professional or a patient, and one additional question to assess prior use of telemedicine services. The full questionnaire is provided as Supplementary Material.
To ensure the validity of the instrument, a two-stage validation process was conducted, following the recommendations of Rincón et al. 69 First, the questionnaire was reviewed by two experts in digital health and two methodological experts, who offered suggestions related to theoretical adequacy and semantic clarity. Second, the questionnaire was evaluated by three senior researchers with experience in technology adoption studies within the healthcare domain. This review allowed for refinement of the wording of several items and adjustments to certain terms to improve their clarity within the Spanish context.
Following this, a pilot test was carried out with a small sample of participants (n = 30), comprising both healthcare professionals and patients. This phase helped to identify potential ambiguities in question formulation and led to minor adjustments to ensure correct interpretation of the questionnaire. A brief introductory section was also included, providing clear definitions and concrete examples of telemedicine services such as video consultations, remote monitoring platforms, or digital delivery of medical reports. This was done to ensure a consistent understanding of the construct across all respondents, following the recommendations of Maldonado-Canca et al. 70
3.3. Procedure and sampling
Sample profile.

Inclusion criteria required that participants be adults and belong to one of the two target groups: (1) practicing healthcare professionals, or (2) patients. Incomplete questionnaires and those with inconsistent responses were excluded from the analysis. 72
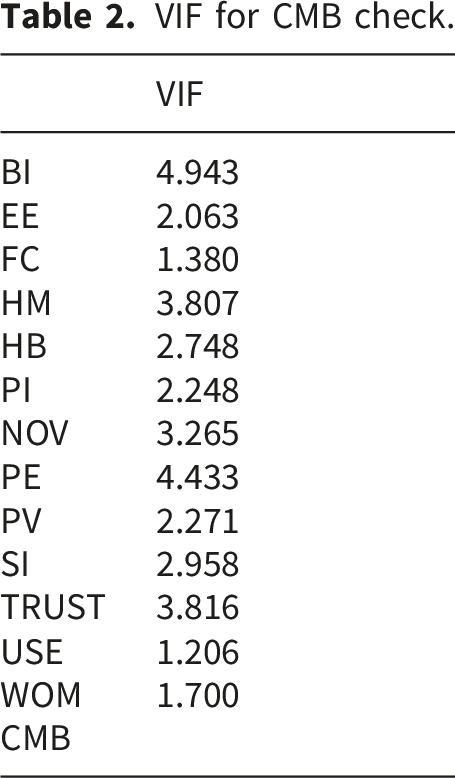
VIF for CMB check.
An a priori power analysis was conducted using G*Power 3.1. 74 Following a conservative criterion, the calculation was based on the largest number of predictors pointing to an endogenous construct in the model (11 predictors for Behavioral Intention in the patient group), a medium effect size (f2 = 0.15), a significance level of α = 0.05, and a statistical power of 0.95. The analysis indicated a minimum required sample size of 178 observations. Both the full sample (n = 684) and the smaller subgroup of healthcare professionals (n = 203) exceeded this threshold, supporting the adequacy of the sample for the overall model estimation and for the multigroup comparisons.
3.4. Data analysis
Data were analyzed using partial least squares structural equation modeling (PLS-SEM) in SmartPLS 4.1.1.4. PLS-SEM was considered appropriate because the study aimed to explain and predict Behavioral Intention and actual Use in a model comprising multiple latent constructs, simultaneous structural relationships, and multigroup comparisons between two theoretically relevant user groups. 75
The analysis followed a two-step procedure. First, the measurement model was assessed in terms of indicator reliability, internal consistency reliability (Cronbach’s alpha, rho_A, and composite reliability), convergent validity (average variance extracted), and discriminant validity using the HTMT criterion.76–79 Second, the structural model was assessed through collinearity diagnostics, bootstrapped path coefficients, coefficients of determination (R2), predictive relevance (Q2), and model fit (SRMR), following current PLS-SEM reporting recommendations.75,80
As a post hoc diagnostic for common method bias and collinearity, full collinearity VIF values were examined; all values were below the threshold of 5, indicating no evidence of problematic collinearity.75,81,82 Table 2 reports the corresponding VIF values.
To examine differences between patients and healthcare professionals, the model was estimated separately for each subgroup and group differences in path coefficients were evaluated using the permutation-based multigroup analysis procedure in SmartPLS. Given the unequal group sizes, the comparison relied on group-specific parameter estimates rather than direct comparisons of raw group means, and both groups exceeded the minimum sample requirement for model estimation.
Before comparing the structural paths across groups, measurement invariance of composites was assessed using the MICOM procedure. As compositional invariance was established, partial measurement invariance was confirmed, which is sufficient for comparing group-specific path coefficients. 77
3.5. Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki and the General Data Protection Regulation (GDPR). All participants provided informed consent prior to completing the questionnaire. Confidentiality and anonymity of responses were guaranteed, and all data were handled responsibly and exclusively for scientific purposes. 83
In accordance with the applicable national requirements for anonymous, voluntary survey research involving adult participants and no intervention, formal review by an Institutional Ethics Committee was not required for this study. Accordingly, no ethics approval number was available.
4. Results
4.1. Measurement model evaluation
Factor loadings, composite reliability and convergent validity.

Discriminant validity was examined using the HTMT criterion. All HTMT values were below 0.90, confirming satisfactory discriminant validity among constructs. 85 The full HTMT matrix is reported in Table A1 of the Appendix.
4.2. Structural model evaluation
Variance inflation factor (VIF).

Path coefficients and significance.
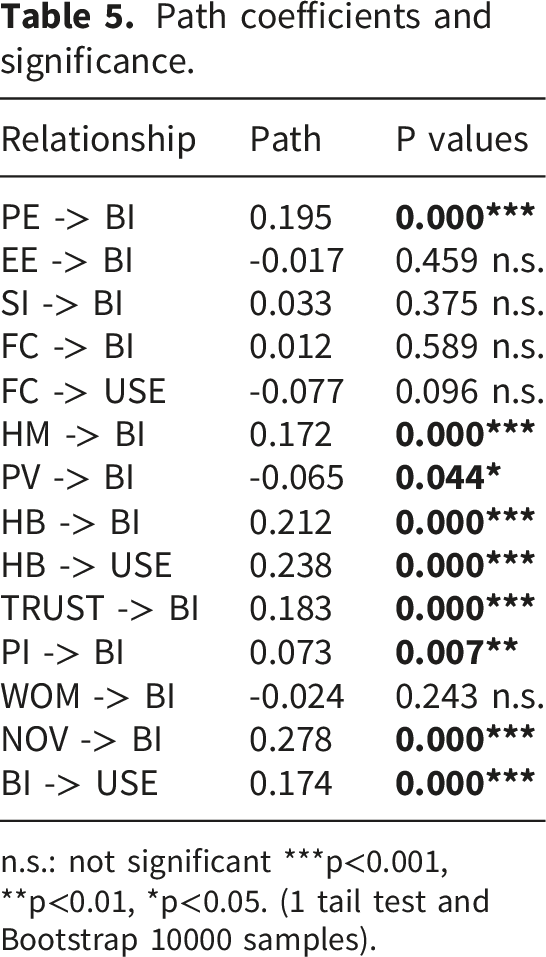
n.s.: not significant ***p<0.001, **p<0.01, *p<0.05. (1 tail test and Bootstrap 10000 samples).
Novelty and Habit exhibited the largest standardized effects on intention, followed by Performance Expectancy and Trust. In contrast, Effort Expectancy, Social Influence, Facilitating Conditions and Word of Mouth did not show significant effects on Behavioral Intention. Regarding actual Use, both Behavioral Intention and Habit had small but significant positive effects, whereas Facilitating Conditions did not reach significance.
Coefficient of determination.

Predictive relevance (Q2).

Model fit (SRMR and complementary indices).

4.3. Practical relevance and differential impact of the model
To identify implementation priorities, an Importance-Performance Map Analysis was conducted for Behavioral Intention. Trust, Habit and Hedonic Motivation combined relatively high importance with only moderate performance, which suggests clear room for improvement if the goal is to strengthen intention to use telemedicine. Novelty and Personal Innovativeness also showed meaningful importance but lower performance, pointing to opportunities for communication strategies that highlight the innovative but still manageable nature of telemedicine services. In contrast, Performance Expectancy and Facilitating Conditions exhibited high performance but lower relative importance in the IPMA, and both Price Value and Word of Mouth showed low importance and performance, indicating a marginal role in this context. The detailed IPMA results are presented in Figure 2. IPMA analysis.
Before conducting the multigroup analysis, Step 2 of the MICOM procedure supported compositional invariance across all constructs, indicating partial measurement invariance and justifying the subsequent multigroup comparison.
Multigroup analysis.

5. Discussion
This study contributes to research on telemedicine adoption by modeling, within a single extended UTAUT2 framework, how patients and healthcare professionals in Spain form intentions to use telemedicine. The dual perspective remains relatively uncommon in the literature, where users and clinicians are often examined separately. 25 The model achieved high explanatory power for Behavioral Intention and acceptable explanatory power for actual Use, which indicates that a combined set of functional, experiential and dispositional factors can account for a substantial share of variance in telemedicine acceptance in a public healthcare context.
Functional expectations about what telemedicine can achieve emerged as an important part of this picture. In line with prior digital health work, Performance Expectancy was a robust positive predictor of Behavioral Intention, and Behavioral Intention itself was associated with actual Use.45,53 This reinforces the core assumption of UTAUT that perceived improvements in care, convenience or efficiency, once translated into a stable intention, are likely to be reflected in behavior.37,63,64 This result also suggests that respondents evaluate telemedicine primarily in terms of concrete care and access benefits, which is consistent with earlier evidence highlighting reduced travel and cost, shorter waiting times, improved efficiency, and remote monitoring as salient perceived advantages of telemedicine. 4
Beyond functional gains, the results highlight a cluster of experiential and communication-related variables as central drivers of intention. Hedonic Motivation and Habit were both positively associated with intention to use telemedicine, and Habit also predicted actual Use, consistent with studies that link enjoyable experiences and routinized use to stronger engagement with digital health services.42,44,45 Trust also emerged as a key predictor, which echoes evidence that confidence in platforms, professionals and data handling is decisive in sensitive clinical interactions.30,32,56 Taken together, these findings suggest that telemedicine adoption depends not only on perceived utility, but also on whether remote encounters are experienced as communicatively effective, familiar, and trustworthy. This interpretation is in line with earlier research showing that patient-centered communication, adequate consultation time, and opportunities to express concerns are associated with higher satisfaction and continuance intention, whereas emotional distance may hinder trust-building in teleconsultations.13–15,17–19 Personal Innovativeness contributed positively, suggesting that users who are more willing to experiment with new technologies are particularly receptive to telemedicine offers, in line with earlier work on technology-related traits.31,32 Finally, Novelty showed a positive association with intention, which supports the idea that seeing telemedicine as a modern, innovative option can motivate initial trial, even if novelty effects may weaken over time.34,61
By contrast, several structural or classical UTAUT2 predictors showed limited influence in this sample. Effort Expectancy, Social Influence and Facilitating Conditions were not significant, despite having been associated with telemedicine acceptance in other settings.43,48,51 This pattern is consistent with more recent findings in digitally mature populations, where ease of use and access to infrastructure are taken for granted and thus become weaker differentiators of intention. 50 Rather than indicating that these factors are irrelevant, the results suggest that they may operate as background conditions: once a basic threshold of infrastructure, digital literacy, and familiarity has been reached, they may no longer be decisive in explaining variation in intention.11,12 Qualitative analyses of telemedicine consultations similarly show that, once a basic threshold of digital and health literacy is reached, patients and clinicians are more concerned with conversational flow, rapport and mutual understanding than with purely technical ease-of-use. 22 This reading is also compatible with evidence that clinicians often learn teleconsultation practices by trial and error, which may shift attention from basic operability to interaction management and communication quality.20,21 From a communication perspective, this suggests that messages focused exclusively on simplicity or technical support may have limited incremental impact once basic usability thresholds are met.
Two findings deserve particular attention. First, Price Value displayed a small but significant negative association with intention. In a public healthcare system where core services are expected to be free, respondents may interpret questions about price mainly as a signal of potential out-of-pocket costs. This would explain why higher salience of price considerations is associated with lower willingness to use telemedicine, and is consistent with evidence that patients express greater confidence when teleconsultations do not entail additional charges beyond usual care, 16 as well as with the regulatory uncertainty and pricing concerns reported for digital health in Spain.43,65 Second, Word of Mouth did not significantly predict intention, despite its relevance in online health and eWOM research. 60 This suggests that in institutionalized care settings, informal recommendations may be less influential than formal communication by providers and health authorities, especially when issues of clinical safety and data protection are salient.
The importance–performance analysis reinforces these interpretations. Trust, Habit and Hedonic Motivation combined high importance with only moderate performance levels, which identifies them as priority levers for interventions that aim to strengthen telemedicine uptake. Personal Innovativeness and Novelty also showed meaningful importance and lower performance, pointing to opportunities for communication campaigns that frame telemedicine as an innovative yet manageable option. In contrast, Performance Expectancy and Facilitating Conditions displayed relatively high performance but lower incremental importance, and both Price Value and Word of Mouth appeared as low-importance, low-performance constructs, suggesting that cost-focused arguments and informal peer advocacy may have limited leverage in this context.
The multigroup analysis adds nuance by showing that patients and healthcare professionals do not weigh all factors equally. Performance Expectancy had a stronger effect on Behavioral Intention among patients, whereas Trust was more influential among clinicians. This is consistent with prior work that highlights perceived usefulness as a central driver for patients and system reliability, clinical responsibility and medico-legal clarity as central concerns for professionals.25,30 This difference suggests that patients approach telemedicine more in terms of concrete access and care benefits, whereas professionals assess it more through the lens of reliability, responsibility, and integration into clinical practice. This interpretation fits earlier literature showing that, for patients, telemedicine may affect access, understanding, communication, and trust, while for professionals it often entails additional communicative, relational, and organizational demands.11,20–22 Qualitative studies of clinicians similarly emphasize that consolidating telemedicine requires specific communication and diagnostic-reasoning skills, integration of digital tools into everyday practice and institutional communication efforts that foster patient trust and cultural change. 20 For communication practice in healthcare settings, these results underscore the need for differentiated communication strategies: messages directed at patients may focus on concrete benefits such as convenience, access and continuity of care, while communications targeting professionals should prioritize guarantees about data security, quality of care and alignment with existing clinical workflows. Overall, the findings support the value of a dual-sided, communication-oriented lens for understanding telemedicine adoption and for adapting general acceptance models to the specific realities of public healthcare systems.
5.1. Theoretical implications
The findings of this study contribute to the theoretical understanding of technology adoption in digital health, within a framework where telemedicine adoption is understood as part of the configuration of new, mediated channels of clinical communication between patients and healthcare professionals. More specifically, the extended model contributes theoretically by showing that UTAUT2 can be adapted to telemedicine in a way that captures not only functional expectations, but also relational and dispositional dimensions of remote care. In addition, applying the model simultaneously to patients and healthcare professionals makes it possible to identify both common drivers and role-specific differences within a shared analytical structure. The inclusion of context-specific variables such as Trust, Personal Innovativeness and Novelty, all of which showed substantial explanatory power for usage intention, reinforces arguments in favor of adapting acceptance frameworks to sector-specific conditions.35,42 These additional constructs, not present in the original formulation, extend the conceptual scope of UTAUT2 in clinical environments.
The prominence of Trust and Personal Innovativeness reflects the particular characteristics of healthcare settings, where perceived reliability and individual readiness to adopt new tools are central to adoption decisions.30,32 Novelty adds a cognitive and affective layer linked to technological curiosity that has been little explored in classical acceptance models. At the same time, the results suggest that not all added constructs contribute equally to the explanatory power of the model. Trust, Personal Innovativeness and Novelty strengthened the explanation of Behavioral Intention, whereas Word of Mouth did not show a significant effect. This indicates that extending UTAUT2 is particularly useful when the added constructs capture mechanisms that are salient in institutionalized clinical settings. Taken together, these extensions contribute to a model with high explanatory power for Behavioral Intention and good predictive capacity, which supports its theoretical relevance in dual-user clinical contexts.
At the same time, the non-significant effects of Effort Expectancy, Social Influence and Facilitating Conditions challenge the presumed universality of UTAUT2. In environments where digital health has become institutionalized, these constructs may lose explanatory strength, while affective, experiential and value-driven variables become more salient.48,50 These null results may therefore point to boundary conditions for the model. Once basic operability, access, and familiarity are no longer major obstacles, intention may depend less on technical ease or social prompting and more on relational confidence, prior habituation, and the perceived meaningfulness of the telemedicine experience. This pattern suggests that the technological maturity of a context is itself a boundary condition for acceptance models and should be taken into account in future theoretical refinements.
The negative association between Price Value and intention, together with the non-significant role of Word of Mouth, also nuances the transferability of consumer-oriented constructs to public healthcare systems. In highly regulated and institutionalized settings, economic and social influence variables may operate differently, with structural, psychological and ethical considerations playing a more central role than classic cost-benefit or peer-pressure mechanisms.54,65 In this context, Price Value may be interpreted less as value for money and more as a cue of possible out-of-pocket costs, whereas Word of Mouth may be less decisive when telemedicine is embedded in formal care pathways and institutional communication structures. From the perspective of online medical consultation, this result adds nuance to bibliometric evidence that highlights word of mouth, social media and anxiety as emerging themes in digital consultation research, 33 suggesting that informal recommendation dynamics may be less decisive when telemedicine is embedded in institutional care pathways.
In addition, our focus on acceptance and proximal use outcomes can be linked to broader pathway models that examine how clinician–patient communication shapes health outcomes. Recent work on online physician–patient communication shows that specific interactional features shape perceived diagnostic and, through it, both psychological and physical quality of life. 86 This suggests that future theoretical developments could integrate adoption models such as extended UTAUT2 with communication pathway frameworks, connecting upstream determinants of intention and use with downstream constructs such as perceived diagnostic and health-related quality of life in telemedicine encounters.
Finally, the multigroup analysis provides empirical support for incorporating a segmented perspective into adoption models. Differences in the weight of core predictors between patients and professionals justify differentiated theoretical treatments of user groups and align with calls for role-specific modeling in multi-user contexts. 24 The results therefore suggest that a shared model can hold across groups while the salience of specific predictors differs by role. Overall, the study confirms the robustness of several established constructs while proposing refinements that point towards a more flexible UTAUT2, sensitive to psychological variables, stakeholder roles and the digital maturity of healthcare systems.
5.2. Practical implications
The results offer several practical guidelines for designing and communicating telemedicine services in public healthcare systems. The importance–performance analysis indicates that Trust, Habit and Hedonic Motivation are priority levers. From a communication and design perspective, this points to the need for platforms that not only work reliably but also convey warmth and clarity in mediated encounters. Features such as stable audio and video, clear identification of professionals, simple and respectful language, and interfaces that support turn-taking and eye contact as far as possible can help patients experience remote consultations as legitimate clinical visits rather than as purely technical interactions.
Training is equally relevant. For healthcare professionals, communication skills in remote settings should be explicitly addressed, including how to open and close teleconsultations, how to check understanding, how to manage silence and technical problems, and how to express empathy through a screen. For patients, brief, accessible guidance before the consultation; for example, short messages or infographics on how to prepare, what to expect and how confidentiality is protected, can reduce uncertainty and support habit formation around telemedicine use.
The dual-user design and the multigroup analysis highlight the need to segment communication strategies. For patients, messages should emphasize concrete benefits such as convenience, continuity of care and faster access, directly linked to Performance Expectancy. For healthcare professionals, communication should focus on guarantees about data security, clinical quality and medico-legal clarity, strengthening Trust in systems and institutions. Aligning institutional campaigns, onboarding materials and in-consultation scripts with these differentiated priorities can make adoption efforts more responsive to the concerns of each group.
The negative association between Price Value and intention suggests that cost-related messages require particular care in public healthcare systems where services are generally expected to be free at the point of use. Communication around telemedicine should therefore clarify when services are covered under public provision and avoid ambiguous references to additional fees that might inadvertently trigger cost concerns and lower willingness to use remote care.
Finally, although Effort Expectancy and Facilitating Conditions did not emerge as significant predictors in the overall model, they may still be relevant for specific groups such as older adults or people with low digital literacy. Ensuring that telemedicine services are easy to access, providing simple technical support channels and integrating basic digital skills training into patient education can help prevent these factors from becoming hidden barriers. In combination, these measures can strengthen the communicative quality of telemedicine encounters and support more equitable adoption across user profiles.
5.3. Limitations and future research directions
This study has several limitations that should be considered when interpreting the findings. The cross-sectional, self-report design does not allow causal inferences and captures telemedicine perceptions at a single point in time. Although the model explains a substantial share of variance in Behavioral Intention, the explained variance for actual Use is more modest, which suggests that additional factors, such as organizational routines, clinical severity or visit type, may shape the translation from intention to behavior.
The analysis is also limited to the Spanish public healthcare context, characterized by expectations of free access at the point of care and by a specific regulatory and cultural environment for digital health. Caution is therefore needed when generalizing the results to other countries, private systems or mixed financing models. Comparative studies across health systems and professional cultures would help distinguish between context-specific patterns and more general determinants of telemedicine acceptance.
Finally, the study relies on structured questionnaires and does not incorporate direct observation of consultations or other forms of interactional data. Future research could adopt mixed-method designs that combine surveys with interviews, focus groups or analysis of recorded teleconsultations, in order to capture communication practices, relational quality and perceived safety in greater depth. Longitudinal and experimental studies would also be valuable to track how habits develop over time, to test the effects of specific interface or message designs, and to examine additional constructs such as perceived risk, privacy concerns or communication competence among both patients and professionals.
6. Conclusions
This study shows that telemedicine acceptance in Spain is shaped not only by functional expectations, but also by experiential and relational factors. Within the extended UTAUT2 framework, Performance Expectancy, Hedonic Motivation, Habit, Trust, Personal Innovativeness, and Novelty emerged as relevant drivers of Behavioral Intention, while Habit and Behavioral Intention were positively associated with actual Use. By contrast, Effort Expectancy, Social Influence, and Facilitating Conditions did not show significant effects, suggesting that in public and digitally mature healthcare contexts these factors may operate more as enabling conditions than as active determinants of intention.
The study also highlights the value of analyzing telemedicine from a dual perspective. Patients placed greater weight on Performance Expectancy, whereas healthcare professionals were more strongly influenced by Trust. This indicates that telemedicine implementation should not rely on uniform communication or adoption strategies. Interventions aimed at patients may be more effective when they emphasize access, convenience, and continuity of care, whereas strategies targeting professionals should prioritize reliability, data security, and alignment with clinical practice.
Overall, the findings suggest that successful telemedicine adoption depends not only on technical availability, but also on whether remote care is perceived as credible, understandable, and communicatively effective. Future research should test this model in other health systems and examine more directly how adoption processes relate to communication quality and downstream care outcomes.
Supplemental material
Supplemental material - Both sides of the screen: A dual-sided model of telemedicine adoption through extended UTAUT2
Supplemental material for Both sides of the screen: A dual-sided model of telemedicine adoption through extended UTAUT2 by Mario Sierra-Martín, Luis-Alfonso Maldonado-Canca, Pilar Alarcón-Urbistondo, and Juan-Pedro Cabrera-Sánchez in Digital Health.
Footnotes
ORCID iDs
Ethical considerations
The study adhered to all applicable ethical standards involving human participants. All necessary ethical and consent declarations have been fulfilled.
Consent to participate
All participants were informed about the purpose of the study and provided informed consent prior to participation.
Author contributions
The authors have contributed equally to all parts of the article.
Funding
This research received a grant from Plan Propio del Vicerrectorado de Investigación of the University of Málaga.
Declaration of conflicting interests
The authors have no conflicts of interest to declare that are relevant to this article. The authors ensure that there's no financial/personal interest or belief that could affect the objectivity. To prevent ambiguity, authors state explicitly that there is no potential competing interests.
Data Availability Statement
All data will be available on demand.
Supplemental material
Supplemental material for this article is available online.