
Abstract
Background
After discharge home, stroke survivors and their informal caregivers face a significant lack of support and information which accentuates their psychosocial burden. Online resources might provide this support and address psychosocial needs, but existing online stroke programmes mainly target functional rehabilitation. We aimed to map the existing literature on online resources that have been evaluated in stroke rehabilitation and aimed at reducing psychosocial impact in stroke survivors and informal caregivers.
Methods
MEDLINE was searched (2010–2024) to identify studies investigating online resources targeting psychosocial health. Studies were selected and extracted independently by two reviewers. We described the content, use, and psychosocial impact of these interventions using a narrative approach.
Results
Eleven studies were included in the review, reporting 10 online resources (two studies relating to the same resource). Online resources were heterogeneous: eight information/resources websites, one mobile app, and one forum. Five online resources were dedicated to stroke survivors, four to stroke survivors and their informal caregivers, and one to informal caregivers. Two randomized controlled trials reported a significant decrease in depressive symptoms associated with the use of online resources. Stroke survivors and informal caregivers find online resources useful and acceptable to address their psychosocial needs.
Conclusions
Few online stroke resources have been designed and evaluated to support post-stroke psychosocial rehabilitation. Further larger-scale research needs to study the impact of these interventions on psychosocial recovery over time.
Introduction
Stroke is a major health problem all around the world, with an estimated 9.6 million ischaemic strokes and 4.1 million haemorrhagic strokes each year. 1 In 2010, the prevalence of stroke survivors was 33 million and this number should increase to reach 77 million worldwide in 2030 with a notable increase among young people. 2 The prognosis of patients in the acute phase of stroke considerably improved over the past few years. 3 The increasing number of patients surviving a stroke, combined with the increase in the number of stroke cases in young subjects, has led to an increase in the lifetime with sequelae of stroke, a modification of the type of sequelae, and their impact on the lives of survivors of stroke. Stroke survivors and their informal caregivers face complex healthcare-related challenges (e.g. prevention of complications, and conditions underlying stroke) impairing recovery.4,5 Although improvement in the acute management of stroke has resulted in a reduction of physical sequelae, the latter frequently mask the psychosocial and emotional impact on stroke survivors. These are more generally called ‘hidden disability’ (including depression, anxiety, and management of stress or emotions for example), which lead to impaired psychosocial competency as defined by the World Health Organization (WHO) as ‘a person's ability to maintain a state of mental well-being and to demonstrate this in adaptive and positive behavior while interacting with others, his/her culture and environment’. 6 For example, almost a third of stroke survivors suffer from post-stroke depression,7,8 24% suffer from post-stroke anxiety,9,10 32% have difficulties managing emotions on a daily basis. 11 In addition, it is considered that less than a third of stroke survivors have their emotional needs addressed within the traditional healthcare system. 12 These consequences of stroke are difficult to manage on a daily basis for stroke survivors but also their informal caregivers13,14 who are also often experiencing depression and anxiety. This leads to a vicious circle as caregivers who feel distraught are less likely to take care of their stroke survivor relative, 15 which may in return exacerbate the consequences of stroke.5,16,17
A lack of acknowledgement of stroke's psychosocial impact leads stroke survivors and their informal caregivers to face challenges on their own, which increases the burden and is associated with a strong demand for support and information. 18 Online resources might be interesting to address the psychosocial needs of stroke survivors and their informal caregivers throughout their journey. Online resources include various approaches such as forums, peer support, information websites, and web-based programmes, and these can be accessed autonomously by stroke survivors and their informal caregivers or managed by health professionals. In other pathologies, a growing body of evidence has described a range of beneficial effects of the use of online resources, such as reducing depression and loneliness, which community members can experience through their online engagement and the support of a community that has already experienced the same situation.19–22
Existing interventions to improve transitional care following stroke mainly focus on the medical aspects of management and functional rehabilitation.22–25 The use of online resources has widened access to post-stroke functional rehabilitation while maintaining its efficacy. 26 However, few data are available on online resources to improve psychological burden among stroke survivors, and/or informal caregivers. Although the literature on stroke rehabilitation is rich, no synthesized work focusing on the impact of online resources for transitional care dedicated to psychosocial recovery exists.
The objective of this scoping review was to map the literature on online resources that have been evaluated in stroke rehabilitation and aimed at reducing psychosocial impact in stroke survivors and informal caregivers.
Methods
We conducted a scoping review because our concept required a synthesis of a wide range of research studies and approaches due to the wide perimeter of psychosocial impact and the various types of online resources. 27 The review followed the five-step scoping framework proposed by Arksey and O’Malley, 28 refined by Levac et al., 29 and is reported according to the PRISMA reporting guideline for Scoping Reviews (PRISMA-ScR) 30 (Supplemental File 1). The protocol of the review was registered on Open Science Framework. 31
Research questions
The research questions were as follows: (1) What are the online resources available on stroke psychosocial rehabilitation that have been evaluated? (2) What is known about the impact of online resources on stroke psychosocial rehabilitation? To answer these questions, we looked at the impact of online resources on psychosocial outcomes for stroke survivors and caregivers such as quality of life; depression; stress and anxiety; social participation; as well as other hidden disabilities (e.g. fatigue). We also considered outcomes relating to rehospitalization; impact on health services, and stroke recurrence. (3) What are the acceptability, adherence, and perceived usefulness of these interventions? (4) What is the place of peer support in these resources, between stroke survivors and between caregivers? (5) How online resources were developed and were final users involved in the development process?
Eligibility criteria
The eligibility criteria were designed according to the population, intervention, comparator, and outcomes (PICO) framework, and are presented in Table 1. To be included in the review, studies had also to be written in English or French language. Quantitative, qualitative, or mixed-method studies, pilot or feasibility studies, and observational or interventional designs were included to explore different perspectives on online psychosocial rehabilitation resources.
Description of the inclusion and exclusion criteria according to the population, intervention, comparator, and outcomes (PICO) framework.

Search strategy
The MEDLINE database was searched using PubMed for records published from 2010 to January 2024 to broadly capture studies focusing on post-stroke rehabilitation improvement through online resources. The queries used to search the database have been validated by our institution's librarian (Supplemental File 2). To search for additional literature that may not have been captured by the database search, we conducted an ascendancy search of the bibliographic references of included studies.
All records were extracted by MD and RG to Rayyan QCRI. 32 Duplicates were then removed. A first screening of the records on title and abstract following inclusion/exclusion criteria was conducted, independently, by MD and RG, who also conducted the second screening of the reports on full texts. The studies were then included after discussion and agreement between the reviewers and members of the scientific advisory board (AT, PMP, and JH). All data from the included studies were then extracted by MD, RG, AT, and JH in a standardized table (Supplemental File 3).
Outcome measures and data extraction
From each included study, the following outcomes were extracted:
Description of the online resources according to TIDieR
33
guidelines. Impact of online resources on psychosocial outcomes of stroke survivors or informal caregivers, such as quality of life, depression, stress and anxiety, social participation as well as other hidden disabilities (e.g. fatigue), using validated scales or non-validated self-reported or qualitative measures. Outcomes relating to stroke care pathways were also extracted. The acceptability and adherence of stroke survivors or informal caregivers to the interventions, using questionnaires, indicators, or qualitative approaches. The inclusion of a peer support component in the online resources, and the type (direct peer-to-peer discussion, peer testimonies). The development process of the online resources, notably the involvement of end-users in the design and conceptual underpinnings of the resources.
Synthesis of results
Data were summarized using a narrative synthesis approach as we anticipated a substantial heterogeneity in study designs, interventions, and outcomes reported in the included studies. We summarized the type and content of online resources and the outcomes of the use of these online resources. Then, results were discussed to identify which intervention may be the most effective in improving stroke survivors’ post-stroke psychosocial recovery.
Results
The database search yielded 1941 records of which 1595 remained after removing duplicates. A total of 1535 records were excluded after reading the title and abstract, and 51 reports were excluded after full-text review. After this initial selection phase, nine studies were included, and an ascendency search of the bibliographic references of the articles reporting these studies identified two additional studies. Overall 11 studies were included in the scoping review, (Figure 1).

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 flow diagram for new systematic scoping reviews.
Most studies (10/11) provided a full description of the study setting and the outcomes. Five included studies were conducted in the US. A total of 10 online resources were reported by the 11 included studies, one study being a responder analysis of another included study. 34 Four online resources were dedicated to stroke survivors and their informal caregivers, five targeted solely stroke survivors, and one solely informal caregivers. In all studies, the participants were living at home before the stroke and had no great difficulties communicating no serious cognitive impairment, and an internet connection. The intervention was over a period of 30 days to 18 months. Ten out of the 11 studies were randomized controlled trials (RCTs), including one pilot RCT, and one was a qualitative study (Table 2).
Characteristics of included studies.

Note: CES-D: Centre for Epidemiological Studies Depression scale; CVD: cardiovascular diseases; EQ-5D-3L: EuroQol-5-Dimensions-3-Levels; HSSUI: Health and Service Utilization Inventory; IP: Interprofessional; MBE-GF: Maslach Burnout Inventory—General Form; MISTT: MIchigan Stroke Transitions Trials; PAM: Patient Activation Measure; PROMIS: Patient-Reported Outcomes Measurement Information System; RCT: randomized controlled trial; SE: self-efficacy; TAU: treatment as usual; TCSI: transition care stroke intervention; VAS: visual analog scale; VMSCC: Virtual Multidisciplinary Stroke Care Clinic.
Description of the online resources
Among the online resources, eight were information/resources websites, one was an information mobile app, and one was a forum. The exact nature of the online resources was very heterogeneous.
Six online resources combined access to a website and additional support from a professional: the Michigan Stroke Transition Trial (MISTT) (Strong et al. 34 and Reeves et al. 35 ) combined access to the MISTT website with home visit and telephone-based case management; the RESCUE website (Lelaurin et al. 36 ), was combined with a nurse follow-up; the STROKE-CARD (Willeit et al. 37 ) combined access to an educational website with remote monitoring and an appointment with a multidisciplinary team; the TEMpEST website (Demir Avci and Gözüm 38 ) combined access to a website with nurses and coordinator follow-up and home visits; the Virtual Multidisciplinary Stroke Care Clinic (VMSCC) (Lo et al. 39 ) combined a website with video-based consultation and telephone calls with a nurse; and the Transitional Care Stroke Intervention (TCSI) (Markle-Reid et al. 40 ) combined access to the My Stroke Recovery Journey website with a coordinator and interprofessional team follow-up. Two studies used only a website without additional professional support: the Caring∼Web© (Pierce et al. 41 ) website and the resource evaluated by Smith et al. 42
One study evaluated a structured stroke rehabilitation program provided through a mobile app named SHEMA to improve knowledge about stroke and quality of life. 43 One study evaluated an online moderated discussion forum open to stroke patients and informal caregivers aimed to facilitate communication between these, and to share information about any aspects of stroke; the forum was hosted by a stroke survivors association and not moderated by professionals. 44
All these programmes, except the forum, made available to participants written or video information/educational resources on stroke (risk factors, complications, management, medications, and glossary). Additional functions were questions/chat/email discussions with professionals37,39,41,42 or stroke survivors/caregivers,37,43 peer testimonials, 35 and links to additional resources (professionals, social and community services, patient associations or stroke support groups).35,36,41 Websites dedicated to stroke survivors included specific information dedicated to caregivers.35,36 Three websites specified that content included empowerment tools designed to improve self-management and problem-solving skills36,39,40 and one website provided information about home care 38 (Table 3).
Description of the interventions according to the TIDieR guidelines.
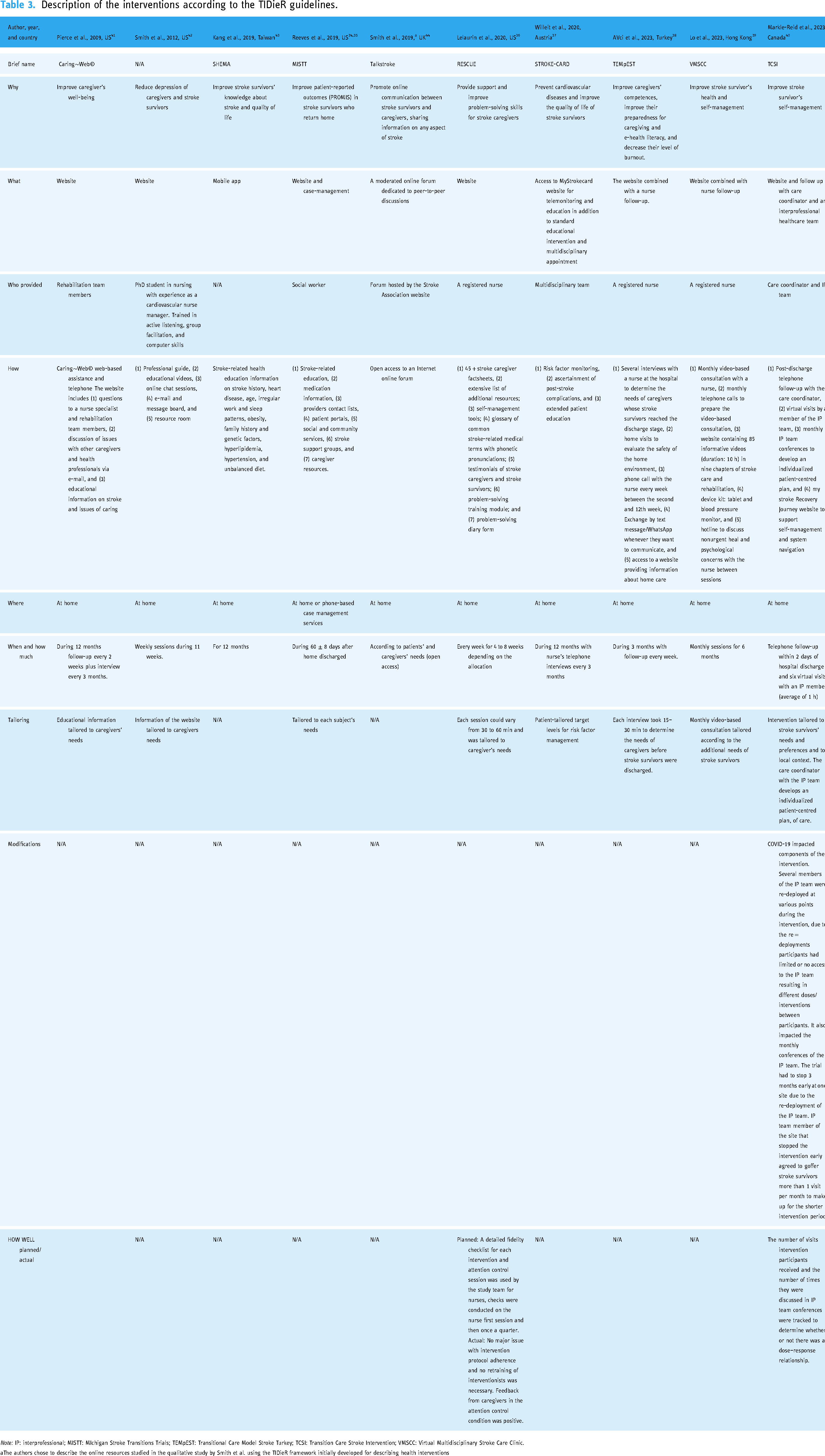
Note: IP: interprofessional; MISTT: MIchigan Stroke Transitions Trials; TEMpEST: Transitional Care Model Stroke Turkey; TCSI: Transition Care Stroke Intervention; VMSCC: Virtual Multidisciplinary Stroke Care Clinic.
The authors chose to describe the online resources studied in the qualitative study by Smith et al. using the TIDieR framework initially developed for describing health interventions
Development of the online resources
Of the studies included in this review, six provided information about how they developed the online resource. Among them, four included stroke survivors and/or informal caregivers’ perspectives in their development35,39,40,42 mainly through focus groups or scientific committees involving health professionals and patients,35,39,42 and one involving the patient's partner in research. 40 Three described structured pilot and usability tests.38,41,42,45
Seven studies explicitly based their intervention on an existing framework, none had the same framework and none was specific to online interventions. Three frameworks targeted care practices or organizations: the Chronic Care Model (MISTT Trial), 46 the Friedmann's Framework of systemic organization Caring∼Web© website) 47 and the Transitional Care Model (TEMpEST). 48 Two targeted behaviour change: the Self-efficacy theory of behavioural change from Bandura (VMSCC), 49 and Lorig and Holdman's self-management theory (TCSI). 50 One was specific to stress management the stress process model (Smith et al.), 42 and one of the caregiving the prepared family caregiver model (RESCUE). 51 Finally, one was a framework for the complex intervention development process, the medical research framework for the development of complex intervention. 52 The other studies did not mention the theoretical underpinning of their intervention.
Needs assessment
Five studies described how the intervention adapted to stroke survivors’ needs. These all concerned interventions combining website with health professional follow-up. Need assessment was conducted at discharge (TEMpEST 38 and TCSI 40 ), at discharge and three months (MISTT 35 ), solely at three months (STROKE-CARD 37 ), or monthly during the intervention (VMSCC 39 ). The needs assessment was either done by the professional in charge of the follow-up (MISTT 35 , VMSCC, 39 and TEMpEST 38 ), by a multidisciplinary team assessment (STROKE-CARD 37 ), or both the health professional in charge of the follow-up in collaboration with a multidisciplinary team (TCSI 40 ). The other studies did not mention conducting a needs assessment during the intervention.
Impact of online resources on depressive symptoms
A total of eight studies investigated depression as an outcome (five for stroke survivors and three for informal caregivers). Regarding the impact on depression for stroke survivors, two interventions (an educational website with remote monitoring 37 and an information website combined with monthly follow-up with a nurse 39 ) significantly reduced anxiety or depressive symptoms for stroke survivors (P < 0.001 and P = 0.008, respectively), while the three other did not.36,40,41 Another study found that increased mastery and social support gained using a website were significantly correlated with reduced depression of stroke survivors (respectively r = −0.49: P < 0.005, and r = −0.37; P < 0.05) at one month. 42 In addition, the qualitative study reported by Smith et al. 44 characterized the process of emotional adjustment after stroke and the role of the online forum in this process. The authors found that participating in an online stroke community as a stroke survivor could be beneficial for the progression of positive emotional adjustment. Regarding the impact on depression for informal caregivers, one study 42 reported fewer depressive symptoms (P < 0.01) among informal caregivers who used the website than those who did not and reported that reduced depression of informal caregivers was correlated with increased mastery at one month (r = −0.030; P < 0.05). Furthermore, informal caregivers who had access to a website combined with nurse follow-up presented significantly lower scores in burnout (P = 0.001) 38 ; (Table 4).
Descriptive summary of findings from included studies.

Note: CES-D: Centre for Epidemiological Studies Depression scale; CVD: cardiovascular diseases; EQ-5D-3L: EuroQol-5-Dimensions-3-Levels; HSSUI: Health and Service Utilization Inventory; MBE-GF: Maslach Burnout Inventory—General Form; MID: minimally important difference MISTT: MIchigan Stroke Transitions Trials; PAM: patient activation measure; PROMIS: Patient-Reported Outcomes Measurement Information System; RCT: randomized controlled trial; SE: Self-efficacy; TAU: treatment as usual; T1: measure 1 at baseline in Smith et al. study; T2: measure post-test in smith el study; T3: measure at one-month follow-up in Smith et al. study; VAS: visual analog scale.
Impact of online resources on other psychosocial outcomes
Quality of life
A total of four studies investigated quality of life as an outcome. Only one study using an educational website with remote monitoring significantly improved patient-related health quality of life (P < 0.001) at 12 months 37 (Table 4). However, the MISTT,34,35 the SHEMA app, 43 and the TCSI 40 did not lead to a significant improvement in quality of life.
Empowerment and self-management
Five studies reported outcomes on users’ empowerment. Among these, three, all relating to an intervention combining access to a website and professional follow-up, found significant improvement in stroke-survivors’ empowerment and self-management skills. The MISTT intervention significantly improved stroke survivors’ activation, as measured by the Patient Activation Measure (PAM), both over time (P = 0.042), and compared to case-management alone (P = 0.016) and treatment as usual (TAU) (P = 0.07).34,35 The VMSCC 39 intervention reported a significantly greater self-efficacy (P = 0.042) and a greater social participation (P = 0.026) than TAU at 6 months. In addition, the TCSI 40 reported a significant difference in stroke survivors' self-management in the intervention group compared to TAU. The SHEMA mobile app 43 significantly improved stroke knowledge in a pre–post analysis (P = 0.002), but so it was in the control group (P = 0.001). The educational website with remote monitoring by Willeit et al. 37 did not report results on stroke survivors' empowerment although they mentioned it in the aims of the intervention.
Physical health and healthcare consumption
Results converge towards an improvement in the physical health of stroke survivors. Use of the information websites combined with case management or with remote monitoring significantly decreased the modified Rankin Scale (mRS) compared to control34,35,37 and improved self-reported physical function (reported by the MISTT as measured by the PROMIS Global-10 (P < 0.001) 35 and the TCSI as measured by the Physical functioning dimension of the SF-12 (P = 0.005) 40 ). The website with remote monitoring also reduced the cumulative incidence of cardiovascular disease (P = 0.007) at 12 months. 37 Moreover, the TCSI intervention did not lead to reduced risk of hospital readmission 40 while the Caring∼Web© website dedicated to informal caregivers showed a significant reduction in the use of health services (emergency department and hospital re-admission) for their stroke survivor relative 3 months after stroke (P = 0.001). 41
Adherence, acceptability, and perceived usefulness of the intervention
Four of the 11 included studies investigated adherence to their intervention, results were very heterogeneous according to the type of intervention. While it is difficult to combine these adherence assessments, these suggest better adherence and more regular use of online resources by caregivers than stroke survivors. Indeed, Pierce et al. 41 reported that informal caregivers regularly used the Caring∼Web© with a mean of 1–2 h per week, 102 messages to nurses, as well as 2148 messages in the non-structured peer-to-peer email discussions during the 12 months of the study. On the opposite, Reeves et al. 35 reported that 11% of stroke survivors declined training on how to use the website, 61% received training but never accessed the website, and only 28% accessed the website (consulting a mean of 25 pages over a mean 3.3 days). Adherence to a structured program reported by Smith et al. 42 seems high with only 3/32 survivor/caregiver dyads (9.4%) who completed fewer than 10 sessions of the 11 weekly sessions planned in the intervention. Smith et al. 44 reported that there were 69 participants on the online forum; among these, 39 were stroke survivors, 29 were informal caregivers, and one was a healthcare professional, who published a total of 124 posts.
Three studies analysed the perceived usefulness and satisfaction of online resources. Results concerned only informal caregivers’ perceptions. By analysing nurses’ interviews with informal caregivers, Pierce et al. 41 found that the intervention (online resources combined with nurse follow-up) was an outlet for stress for caregivers. It helped them to be more positive in their caregiving role and adopt the stroke survivor's point of view. Web users were satisfied with the content of the intervention. In the study reported by Smith et al., 42 informal caregivers perceived a significant benefit for stroke survivors in the intervention arm (P < 0.03). Lelaurin et al. 36 reported that informal caregivers gave positive feedback, particularly regarding sessions with nurses, factsheets, and resources, but mentioned that similar information was already transmitted to them at the time of the stroke.
Peer support in online resources
Four of the studied online resources included peer exchanges: one was exclusively based on peer-to-peer sharing and support (online forum 44 ), the others included components such as referencing of local and online stroke peer support groups (MISTT trial 35 ), peer-testimonials (Rescue website 36 ) and discussion by e-mail between caregivers (Caring∼web© 42 ). Only the qualitative study reported by Smith et al. 44 explicitly investigated the effect of peer support and peer-to-peer experience sharing in the online forum; the authors concluded that the sharing of experience between peers was decisive in post-stroke emotional trajectory adjustment. However, the use of forums to share experiences between stroke survivors needs to be cautious or supervised as it can have both a positive and negative effect on the stroke survivor's emotional trajectory. Indeed, this trajectory can oscillate over time between improvement and deterioration, and the effect of the forum can vary according to the stroke survivor's condition. The sharing of experiences seems promising to provide emotional support and contribute to the normalization processes. 44 Participants of the online stroke community felt comfort and gratitude in being able to discuss with their peers.
Discussion
This scoping review included eleven studies investigating online resources dedicated to post-stroke psychosocial recovery.35–37,41–44 Of these, six combined the online resource with support from a health professional,35–37 eight provided information via the online resource (seven websites and one mobile App), and one was a discussion forum.35–37,41–44 Four quantitative studies37–39,42 found an improvement in psychosocial aspects, particularly depression, two in stroke survivors and two in informal caregivers through the use of online resources; reduction in psychosocial burden was mediated by increased mastery/social support. 42 Furthermore, online resources decreased informal caregivers’ stress and helped them better understand the stroke survivors for whom they cared for.41,42 It was also found that participating in an online forum could improve post-stroke emotional trajectory, however, the course of the emotional adjustment of stroke survivors was not stable over time as it varied between a positive and a negative emotional trajectory. This phenomenon could be triggered by various stages of the patient's journey, such as reaching the end of physiotherapy or starting antidepressant treatment, for example. 44 In addition, online resources combined with professional support improved the overall health of stroke survivors, but it was not possible to discriminate between the use of online resources alone compared and online resources combined with professional support.34–37,39,40 Furthermore, when reported, the online resources were useful41,42 and acceptable for stroke survivors and their caregivers,36,41 however adherence and use seem better among caregivers than stroke survivors themselves.
The level of evidence on the impact of online resources on depression and anxiety among stroke survivors remains poor and is supported by only two studies, one that combined an education website with remote monitoring and an additional appointment with a multidisciplinary team of stroke professionals 37 and another that combined an information website with monthly follow-up with a nurse. 39 It is therefore not possible to differentiate the impact of the two components of the intervention on the participants. Moreover, adherence to the programmes was very heterogeneous, and only one study investigated the fidelity of the intervention, 36 which is the comparison between the intervention planned in the protocol and the intervention implemented. 53 If this parameter had been reported in all studies, this would have allowed a comparison as to how the intervention evolved in terms of adherence, participant responsiveness, and involvement, and better identify the functioning of the different interventions. This, in addition to the lack of theoretical underpinning of some of the interventions, prevented us from understanding the mechanisms of action of the interventions, and how they might support stroke survivors. A lack of qualitative evaluation also limited the depth of the interpretation of the effect of using online resources.
Among the studies included in the present scoping review, the trial reported by Strong et al. 34 and Reeves et al., 35 which associated case management and a website, improved stroke survivors' activation and physical health. 35 The consequences of a stroke can leave the stroke survivor more dependent on his/her family which impacts social participation and can cause post-stroke depression. 54 Since improving functional aspects tends to improve the mood, 26 and Smith et al. 42 found that depression was correlated with mastery and social support, 42 we hypothesized that the effect of online resources on depression might also indirectly be driven by functional improvement, mastery, and autonomy gained by using the online resource. It is also of note that four studies investigated quality of life but none of them concluded that using online resources improved this. Moreover, only five studies conducted a baseline needs assessment, making it impossible to study the impact of online resources on the change of post-stroke needs over time and on long-term needs. Further research needs to be conducted on the impact of online resources in post-stroke psychosocial rehabilitation and should focus on the development of long-term interventions.
Three of the studies included were dedicated exclusively to caregivers.36,41,42 Results were promising regarding the positive impact of using the website on post-stroke depression and, the physical and mental health of informal caregivers.36,41,42 Moreover, a study reported an impact on informal caregivers, however, it is, again, not possible to differentiate whether this result is due to the use of the online resource or to the follow-up by the nurse. 38 These results suggest that using online resources to obtain information or receive social support could help to manage the psychological burden of informal caregivers. It would therefore be interesting to study these findings in greater depth since available results were from studies with a low level of evidence.36,42,44 Furthermore, knowing that the mental health of stroke survivors is linked to the mental health of informal caregivers,14,18,54 it could be hypothesized that using online resources to act on informal caregivers' mental health could have an indirect impact on stroke survivors.
Among the different interventions included in the scoping review, five proposed a ‘peer-support’ component (referral to a stroke support group, 35 testimonials, 36 or discussions/chat sessions with peers41,42,44), however, only one of them specifically detailed this aspect in the evaluation. 44 Peer support decreases post-stroke depression but the mechanism behind this effect needs to be further investigated. 55 Smith et al. 44 reported that discussing with peers may trigger the transition in the recovery trajectory, and according to when stroke survivors have access to peer support, this may have a negative or positive impact on their psychological feelings, 44 which is supported by that reported by Alaszewski et al. 56 Considering that social support is associated with a decrease in post-stroke depression, 54 these results suggest that sharing experiences might have a positive impact on the depressive syndrome of survivors. Online peer support has to be further investigated since, although it was part of five interventions, this specific component was not separately evaluated, and, it is reported that online peer support is less effective than face-to-face interventions. 55
Limitations
Despite the large number of studies identified only a few were included. Moreover, among these, and despite the majority being randomized control trials, most of them were not sufficiently powerful to draw any conclusion and generalize results. In addition, due to the narrative nature of this review, we did not control for risks of bias. Furthermore, there was no qualitative assessment of the online resources, and the potential effect of online resources on the empowerment of stroke survivors and their informal caregivers as well as on peer support was not evaluated, although the latter are known to impact mental health in other chronic diseases.20,21,57,58
Conclusion
The use of online resources for stroke survivors and their informal caregivers may be a suitable way to decrease post-stroke depression and anxiety especially when combined with a nurse or case-management follow-up. However, most studies had a very limited sample size, and the interventions as well as the results were heterogeneous. The data from this scoping review suggest that future studies of online resources should study with greater depth how the online resource responds to the needs of participants, the adherence, and mechanisms of actions over the long term.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241240895 - Supplemental material for What are the available online resources targeting psychosocial burden among stroke survivors and their informal caregivers: A scoping review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241240895 for What are the available online resources targeting psychosocial burden among stroke survivors and their informal caregivers: A scoping review by Marion Delvallée, Romain Garreau, Anne Termoz, Pierre-Marie Ploteau, Laurent Derex, Anne-Marie Schott and Julie Haesebaert in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241240895 - Supplemental material for What are the available online resources targeting psychosocial burden among stroke survivors and their informal caregivers: A scoping review
Supplemental material, sj-docx-2-dhj-10.1177_20552076241240895 for What are the available online resources targeting psychosocial burden among stroke survivors and their informal caregivers: A scoping review by Marion Delvallée, Romain Garreau, Anne Termoz, Pierre-Marie Ploteau, Laurent Derex, Anne-Marie Schott and Julie Haesebaert in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241240895 - Supplemental material for What are the available online resources targeting psychosocial burden among stroke survivors and their informal caregivers: A scoping review
Supplemental material, sj-docx-3-dhj-10.1177_20552076241240895 for What are the available online resources targeting psychosocial burden among stroke survivors and their informal caregivers: A scoping review by Marion Delvallée, Romain Garreau, Anne Termoz, Pierre-Marie Ploteau, Laurent Derex, Anne-Marie Schott and Julie Haesebaert in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgements
The authors would like to thank the librarian of our institution, Mrs Florence Bouriot for her help in validating their search equations and Mr Philip Robinson for his help in scientific writing and English revision.
Contributorship
MD, RG, and JH conceptualized the original draft of the manuscript. RG, JH, and MD designed the research equation. PMP, AT, and JH participated in study selection, appraisal, and data extraction. AT, AMS, and LD critically reviewed and revised the manuscript and made appropriate edits or changes.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and patient consent
This research is not subject to ethical approval since the research did not have participants (humans or animals).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Non applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.