
Abstract
Objectives
This study aims to investigate the impact of digital engagement on urban-rural disparities in depressive symptoms among Chinese women.
Methods
Using a dataset from the China Family Panel Studies (CFPS) wave 2020, this study analyzes the impact of digital engagement on the urban-rural disparity in women's depressive symptoms using multiple linear regression and recentered influence function (RIF) models. Furthermore, the extent to which digital engagement affects the urban-rural disparity in women's depressive symptoms was calculated using the RIF decomposition method.
Results
Analysis showed that rural women had significantly higher levels of depressive symptoms compared to urban women; digital engagement significantly reduced women's depressive symptoms levels and mitigated the urban-rural disparity for women with moderate to high levels of depressive symptoms, and the mitigating effect was stronger for the highly depressed sample, but still widened the urban-rural disparity in women's depressive symptoms overall. In addition, the results of the RIF decomposition showed that digital engagement explained 28.28% of the urban-rural disparity in women's depressive symptoms.
Conclusion
There is a significant disparity in depressive symptoms levels between urban and rural women in China. Digital engagement reduces women's depressive symptoms, but it also widens the depressive symptoms disparity between urban and rural women overall. Digital engagement is potentially positive for reducing women's depressive symptoms.
Introduction
Depression has become a major mental illness worldwide, jeopardizing the physical and mental health of human beings.1–4 The prevalence of depressive symptoms in women has increased dramatically in the last decade. 5 Major depressive disorder is more prevalent in women compared to men, 6 and women are twice as likely as men to be diagnosed with depressive symptoms.7–9 This gap widens as men and women enter adulthood and experience inequalities, 10 and there are also significant cross-national differences. 11 In China, there are differences in the prevalence of depressive symptoms among menopausal women across different regions, 12 which is related to the urbanization process and the level of modernization and development. 13 Digitalization is another important symbol of modern social life, and there are also a series of causal relationships between the use of digital technologies, such as the Internet, smartphones, and social media, and psychiatric disorders such as depression.14–16 Especially during the COVID-19 outbreak, emotional coping was positively associated with depression, 17 and depression was more severe in pregnant and postpartum women compared to the general population. 18 Are there urban-rural disparities in women's depressive symptoms? Does digital engagement affect women's depressive symptoms, and if so, does it mitigate or exacerbate urban-rural disparities in women's depressive symptoms? This is an important topic in relation to human rights 19 and health inequalities, 20 but no study has yet explored this.
Rural–urban disparities in women's depressive symptoms
There is a more complex issue of urban-rural disparities in women's depressive symptoms. A study of the United Kingdom and Ireland showed that there was a more pronounced urban-rural disparity in the prevalence of depressive symptoms among women than among men, 21 and that depressive symptoms increased more rapidly with age in rural women than in rural men. 22 Studies on China have shown that rural residents have significantly higher depressive symptoms than urban residents, 23 and that women among rural students are at higher risk of experiencing depression. 24 Especially in low- and middle-income countries, women with low education, widows, divorced and unemployed women are at higher risk of depression, 25 and urban-rural disparities in depressive symptoms are concentrated in the group of unpartnered women. 26 However, it has also been found that rural residence reduces the risk of major depressive disorder and is more protective for young women than young men. 27 In addition, Romans et al. showed that the prevalence of depressive symptoms is typically higher in urban areas than in rural areas, 28 which is mainly due to impaired mental health caused by increased population density and traffic noise associated with urbanization, 29 and country-specific differences. 30 As reducing mental health disparities between urban and rural areas has received much attention in scientific and policy debates,31–33 further identification of urban-rural disparities in women's depressive symptoms is needed.
Digital engagement and women's depressive symptoms
Existing research on the relationship between digital engagement and depressive symptoms in women remains inconsistent. It is still inconclusive whether digital engagement exacerbates or alleviates women's depressive symptoms. On the one hand, several studies have found that higher levels of digital engagement are strongly associated with the severity of depressive symptoms in both young and adult women.34,35 Heavy use of digital media, the Internet, and daily social media use has a significant negative impact on the mental health of female adolescents.36–39 Furthermore, digital engagement such as using social media positively affects depressive symptoms, 40 individuals who frequently use social media experience more severe depressive symptoms than light users. 41 On the other hand, several other studies have shown that digital engagement is not associated with depressive symptoms. 42 Even during the COVID-19 pandemic, there was no basis for the claim that digital technology was directly harmful to mental health. 43 In addition, higher digital engagement was associated with lower levels of depressive symptoms in older adults, and the effect of digital engagement on depressive symptoms was heterogeneous for older women aged 60–70 years and rural residents. 44 Overall, whether digital engagement exacerbates women's depressive symptoms or alleviates it, then, is a question worth examining.
Urban-rural disparities in digital engagement and women's depressive symptoms
Mental health inequality has long existed between urban and rural residents in China,45,46 which is mainly manifested by the fact that the mental health of urban residents is significantly better than that of rural residents. 47 The urban-rural disparity in women's depressive symptoms is a typical manifestation of mental health inequality, so what is the effect of digital engagement on the urban-rural disparity in women's depressive symptoms? It has been argued that digital engagement can reduce mental health inequalities between urban and rural residents, 48 and is a way to alleviate health disparities between urban and rural areas through online health communities. 49 The inference is that digital engagement can mitigate urban-rural disparities in women's depressive symptoms.
However, it has also been argued that digital engagement may also exacerbate urban-rural disparities in women's depressive symptoms. While the internet is an easily accessible source of health information, it can also create inequalities in access to health information, that relying exclusively or heavily on electronic technology to disseminate health information may increase the likelihood of further perpetuating health disparities, 50 and that the existence of the digital divide puts the vast majority of those with lower levels of education, socioeconomic status, and internet skills at a disadvantaged. 51 Particularly in some developing countries, digital engagement opportunities for women are challenged 52 and they are unable to fully enjoy the benefits of engagement, 53 meaning that digital engagement may also exacerbate urban-rural disparities in women's depressive symptoms.
Based on the above, this study proposes three research questions. (1) Whether there is a significant disparity in depressive symptoms levels between urban and rural women. (2) Whether digital engagement associated with women's depressive symptoms, and whether this relationship is consistent among urban and rural women. (3) Whether digital engagement mitigates or exacerbates disparities in depressive symptoms between urban and rural women, and what the impact effects are.
Methods
Data and participants
The study's data comes from the China Family Panel Studies (CFPS) 2020 wave, a nationwide, large-scale, multidisciplinary social tracking survey program implemented by Peking University. The CFPS program is a nationwide, large-scale, multidisciplinary social tracking survey that focuses on a wide range of research topics, including economic and non-economic well-being, economic activity, educational attainment, family relationships and household dynamics, population migration, health, etc. The CFPS program conducted initial and follow-up test surveys in Beijing, Shanghai, and Guangdong in 2008–2009, and formal interviews in 2010, with a total of seven waves of official surveys to date. In 2010, the survey was formally launched. Up to now, seven waves of official surveys have been conducted in 2010, 2012, 2014, 2016, 2018, 2020, and 2022 (database not updated). The CFPS sample covers 25 provinces/municipalities/autonomous regions in mainland China, with a target sample size of 16,000 households, including all household members in the sample households.
We selected the study participants based on gender and age. Specifically, all adult females older than 20 years of age (inclusive) constituted the sample for this study. Since only the 2020 dataset measures digital engagement, the CFPS 2020 wave data was selected for this study, which was conducted in the context of COVID-19 pandemic. A total of 10,640 adult women respondents aged 20 years and older were screened in the CFPS 2020 wave dataset, with an urban sample consisting of 5551 (52.17%) and a rural sample consisting of 5089 (47.83%).
Measures
Depressive symptoms
These were measured using the simplified CES-D 8-item scale, and it has been measured since 2018 using the simplified CES-D 8-item self-report scale that has been accepted in several studies.15,54 The CES-D 8-item measures the frequency of a variety of feelings or behaviors that have occurred in the past week for the respondent, and consists of six positive entries and two negative entries, with specific entries were (a) I feel depressed, (b) I find it hard to do anything, (c) I do not sleep well, (d) I feel pleasant, (e) I feel lonely, (f) I live happily, (g) I feel sad and upset, and (h) I feel that I cannot go on with my life. Frequency was measured in coding using a four-point scale, that is, hardly ever (less than a day) was coded as 1, some of the time (1–2 days) was coded as 2, often (3–4 days) was coded as 3, and most of the time it was coded as 4. Scores on the eight measurement items were summarized to obtain a composite index ranging from 8 to 32, with higher values indicating higher levels of depressive symptoms. In this study, the Cronbach's alpha for CES-D-8 was 0.773.
Digital engagement
Existing studies have not yet developed a measurement scale for digital engagement. Damant et al. defined digital engagement as the respondents’ adoption of information and communication technologies (ICT) such as the Internet, cell phones, and computers, as evidenced by the use of Internet networks, cell phones, smartphones, computers, and tablets. 55 Layte et al. used five digital behaviors in their study to measure the respondents’ digital engagement. These digital behaviors include “sharing photos and videos,” “messaging friends or family,” “school/college work,” “watching clips/videos,” and “downloading and listening to music.” 34 Based on this, this study measured digital engagement using eight binary measures (yes/no) of digital engagement behaviors(in the original questionnaire it was multicategorical, but these digital use behaviors were not measured uniformly in CFPS2020, and we coded them dichotomously), which are: “accessing the Internet on a computer,” “accessing the Internet on a mobile device,” “using WeChat,” “posting on social media,” “playing online games,” “shopping online,” “watching short videos,” and “online learning.” Respondents with these digital engagement behaviors were coded as 1, otherwise coded as 0. The scores of the eight digital engagement behaviors were then aggregated to obtain a digital engagement index ranging from 0 to 8 scores, with larger values indicating a higher degree of digital engagement.
Control variables
The control variables in this study were selected from four aspects: demographic characteristics, economic status, health status, and residential characteristics. (a) Demographic characteristics (age, marital status, years of education): age and years of education were self-reported continuous data from respondents; marital status included married and unmarried (single, divorced, and widowed). (b) Economic status (insurance, annual personal income): insurance is categorized into having at least one insurance and none; annual personal income is self-reported continuous data. (c) Self-assessed health status (body mass index, BMI): self-assessed health status is a five-point Likert scale; BMI is calculated based on respondents’ self-reported height and weight. (d) Residence characteristics (residence, residence region): residence was categorized into two groups: urban and rural; residence region included five groups: northeast China, western China, central China, and eastern China.
Statistical analysis
This study first examined whether there is a significant difference in depressive symptoms levels between urban and rural women and whether other characteristics are specifically significant between urban and rural areas using the T-test and χ2 test (Table 1). Then, OLS models were constructed to test the effect of digital engagement on women's depressive symptoms in the overall sample, urban sample, and rural sample, respectively (Table 2), and endogeneity analysis was conducted. In the following study, the effect of digital engagement on urban-rural depressive symptoms disparity among women was analyzed using the RIF (recentered influence function) model.
Descriptive statistics of all variables (N = 10,640).

Note: ***p < 0.001, *p < 0.05.
Regression results of digital engagement affect women's depressive symptoms.

Note: Robust standard errors in parentheses; ***p < 0.001, **p < 0.01, *p < 0.05.
The RIF model was used to analyze the effect of digital engagement on the urban-rural depressive symptoms disparity among women. It is used to measure the effect of a small change in a sample on a statistic, and the RIF regression and RIF decomposition model are mainly used to explore the components of distributional inequality and intergenerational disparities. Papers by Firpo et al. 56 and Rios-Avila 57 provide a detailed study of the rationale and implementation of the RIF model. In this study, the RIF model helps to examine how digital engagement affects the depressive symptoms disparity among women, and how it affects the depressive symptoms disparity between urban and rural women. Through further decomposition, it was calculated to what extent the variables affect the depressive symptoms disparity between urban and rural women. Specifically, the effect of digital engagement on the depressive symptoms disparity between urban and rural women was tested using RIF regression (Table 3), and finally, the extent to which digital engagement affects the depressive symptoms disparity between urban and rural women was measured using the RIF decomposition model (Table 4).
Results of digital engagement affect urban-rural disparities in women's depressive symptoms.

Note: Robust standard errors in parentheses; ***p < 0.001, **p < 0.01, *p < 0.05.
RIF decomposition results for urban-rural women's depressive symptoms disparities.
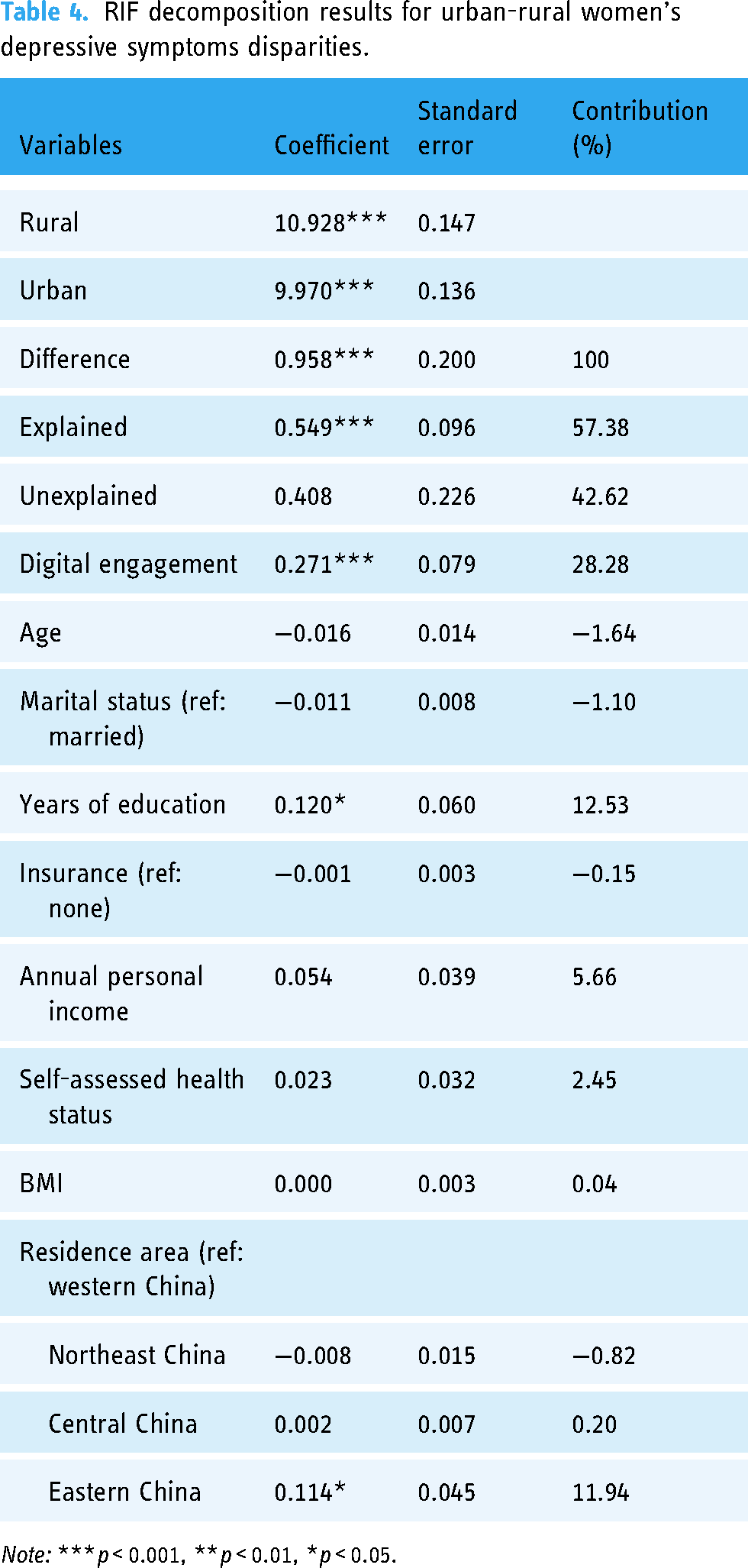
Note: ***p < 0.001, **p < 0.01, *p < 0.05.
Results
Descriptive statistics of all variables
Table 1 shows the overall profile of the study sample, which consisted of a total sample of 10,640 females, of which the rural sample (5089, 47.83%) was slightly less than the urban sample (5551, 52.17%). The depressive symptoms score of the overall sample was 13.95 ± 4.14, where the results of the T-test and χ2 test showed that the rural sample (14.39 ± 4.30) had higher depressive symptoms than the urban sample (13.56 ± 3.95) (10.37, p < 0.001). This suggests that there is a disparity in women's depressive symptoms between urban and rural areas within Chinese women, that rural women are more depressed than urban women, and that there is depressive symptoms inequality between urban and rural women. 90.48% were in marital status, and the average number of years of education was 5.14 years. In terms of other variables, Table 1 also shows that there are statistically significant differences between urban and rural women in the variables of marital status (5.51, p < 0.05) and residence region (303.76, p < 0.001). However, no significant differences were found in other characteristic variables.
Regression analysis results of digital engagement affect women's depressive symptoms
Table 2 shows the results of multiple linear regressions of digital engagement affecting depressive symptoms in women, including the overall sample, rural and urban sample. The regression results show that, after controlling for other variables, digital engagement is negatively associated with female depressive symptoms in the overall sample (−0.141, p < 0.001), rural sample (−0.135, p < 0.001), and urban sample (−0.137, p < 0.001), respectively. It suggests that digital engagement can significantly alleviate female depressive symptoms, both in rural and urban women. To exclude the influence of confounding factors, this study conducted an endogeneity analysis during model testing, which showed that all explanatory variables in the model were exogenous, that is there were no endogenous variables. Moreover, the control variables were statistically significant in the overall sample, rural sample, and urban sample.
The effect of digital engagement on urban-rural women's depressive symptoms disparities
Table 3 shows the results of the RIF regressions, including the effect of digital engagement at different quantiles of the urban-rural women's depressive symptoms disparity. Regarding the urban-rural disparity in female depressive symptoms, Table 3 reports the coefficients of digital engagement at the 10th, 50th, and 90th quantiles, and the results show that the effect of digital engagement at the 10th quantile on the urban-rural disparity in women's depressive symptoms was not statistically significant (−0.027, p > 0.05). However, at the 50th quantile (−0.174, p < 0.001), and 90th quantile (−0.250, p < 0.001), digital engagement was specifically statistically significant on the urban-rural female depressive symptoms disparity. It was able to significantly mitigate the depressive symptoms disparity between urban and rural women, and the strength of this mitigation effect was greater at the 90th than at the 50th, suggesting that the mitigation effect was stronger for the sample of highly depressed women.
RIF decomposition results of digital engagement on urban-rural women's depressive symptoms disparities
Table 4 reports the results of decomposing the depressive symptoms disparity between urban and rural women into characteristic effects using the RIF decomposition. The RIF decomposition results show that characteristic variables such as digital engagement explained 57.83% of the depressive symptoms disparity between urban and rural women. Specifically, digital engagement exacerbated the depressive symptoms disparity between urban and rural women (0.271, p < 0.001) with a contribution of 28.28%. In addition to this, years of education (0.120, p < 0.05) and whether they live in the eastern region (0.114, p < 0.05) are two important factors that exacerbate the depressive symptoms disparity between urban and rural women, and their contribution proportions to exacerbate the depressive symptoms disparity between urban and rural women are 12.53% and 11.94%, respectively. Besides, the effects of other variables on depressive symptoms disparity between urban and rural women were not statistically significant.
Discussion
The urban-rural disparity in women's depressive symptoms is a manifestation of mental health access inequality among women. While previous studies have focused on perspectives such as income inequality58,59 and differences in socioeconomic status60,61 among depressed patients, this study focuses on urban-rural disparities in women's depressive symptoms.
It confirmed the existence of significant urban-rural disparities in depressive symptoms among Chinese women, with rural women having significantly higher levels of depressive symptoms (14.39) than urban women (13.56). This is mainly due to the significant disparity between urban and rural areas in China. Some studies have indicated that the urban-rural disparity is a structural factor that contributes to social inequality in China. 62 In terms of mental health, unequal resource allocation and social participation between urban and rural China are potential factors contributing to the different trajectories of depressive symptoms between urban and rural areas, 63 with rural residents having significantly higher depressive symptoms than their urban counterparts,23,64 and rural older adults having higher levels of depressive symptoms than their urban counterparts.60,65,66 For Chinese rural women, unemployment, poorer health or economic status, and lower social support were positively associated with depressive symptoms. 67 This suggests that the urban-rural dichotomous social structure of Chinese society not only reflects the pattern of economic development in China, but also contributes to inequalities in the development of the nation's mental health.
In fact, there are also national differences in urban-rural disparities in depressive symptoms. 30 For example, the prevalence of depressive symptoms among rural residents in the United States is lower than that among urban residents. 13 However, rural women in the United States have a significantly higher risk of perinatal depressive symptoms than urban women. 68 In contrast, there is no urban-rural disparity in depressive symptoms among older Canadians. 69 In low-income and developing countries, women's depressive symptoms is associated with conditions such as limited economic and educational opportunities, economic hardship, lack of autonomy, forced marriage, domestic violence, and inadequate family support. 70 This implies that there are broader socioeconomic factors behind the issue of urban-rural disparities in women's depressive symptoms.
Digital engagement reduces depressive symptoms among women overall, as well as among urban and rural women, which is consistent with previous research findings. 44 Access to more health information on the Internet through digital engagement,71,72 opportunities for social engagement, social activities, and recreation, 73 and supportive online interactions on social media can reduce depressive symptoms. 74 However, this is inconsistent with the findings of several studies,34,35,37–39 which concluded that high levels of digital engagement negatively impact women's mental health and can exacerbate depressive symptoms in women. It can be inferred that there is a high degree of heterogeneity in the relationship between digital engagement and depressive symptoms, 40 with various modes of digital engagement having distinct effects on depressive symptoms. People may experience depressive symptoms when they engage excessively on social networks, 75 as constant social comparison and invasion of privacy can lead to negative emotions. 76 Therefore, when reducing depressive symptoms in women through digital engagement approaches, attention needs to be paid to the differences between different digital engagement approaches and their effects on action.
Digital engagement significantly mitigates urban-rural disparities for women with moderate and high levels of depressive symptoms, and the mitigating effect of digital engagement is stronger the higher the level of depressive symptoms, but not for women with low levels of depressive symptoms. This suggests that the “digital dividend” effect is greater than the “digital divide” effect for urban-rural disparities between women with moderate and high levels of depressive symptoms. This finding is consistent with previous findings on health inequality among Chinese residents that digital engagement can help reduce mental health inequality among urban and rural residents. 47 As people with deep health deprivation, the effect of the Internet on mitigating health inequality became stronger as well, and had stronger marginal effects in rural and women's groups. 48
The reason for this is that women with moderate and high levels of depressive symptoms overcame the effects of their disadvantaged position in the “digital divide” and became more proactive in accessing health information and engaging in more online activities through digital engagement. Similarly, a study on urban-rural disparities in the impact of the Internet on depressive symptoms among older adults showed that the mechanisms by which Internet use affected depressive symptoms differed between urban and rural older adults, with rural older adults benefiting more. 77 This suggests that vulnerable groups, such as the rural elderly and rural women feel the “digital dividend” effect more. However, the “digital divide” is still an important obstacle for women in developing countries, and their opportunities for digital engagement are still limited. 52 The Internet can help users access a wide range of health information, but those who are more educated, younger, of higher socioeconomic status, and more Internet-savvy are able to access more health information, leading to unequal access to health information. 50 This implies that while digital engagement narrows urban-rural disparities among women with moderate and high levels of depressive symptoms, there is still a need to focus on social factors such as the availability of women's digital engagement, as well as individual factors such as their ability to engage digitally.
It is worth noting that digital engagement actually exacerbates the urban-rural disparity in overall women's depressive symptoms, with a contribution of 28.28%. This result has both macro-social and micro-individual causes. At the macro level, China's dual urban-rural structure has economic, medical, and educational resources that are primarily skewed toward cities, urban areas have better data infrastructure than rural areas, and the gap in data infrastructure quality between urban and rural areas persists and is widening, 78 which can result in differences in the availability and likelihood of digital engagement between urban and rural women, thus exacerbating urban-rural disparities in women's depressive symptoms. These structural factors at the societal level may contribute to rural women's lack of access to digital resources or limit their digital exposure, thereby exacerbating urban-rural disparities in women's depressive symptoms.
At the micro level, although digital technologies can provide support to meet people's mental health needs, the digital divide may exclude some people with weaker digital engagement, thus exacerbating social inequality. 51 One study noted that there is a digital divide between urban and rural residents, but rural residents are less likely to use the Internet compared to urban residents, and women tend to use the Internet less frequently. 79 Exclusion is due to a lack of knowledge, skills, and financial resources, not due to a lack of willingness. 80 Thus, digital participation exacerbates the urban-rural disparity in women's depressive symptoms due to a combination of macro-social and micro-individual factors. In addition, educational attainment was the second largest contributing factor in exacerbating the urban-rural disparity in women's depressive symptoms. This enriches previous research that education is an important factor in explaining inequalities in the prevalence of depressive symptoms among older women 81 and that higher education significantly exacerbates inequalities in people's health, both in urban and rural populations. 82 Finally, the fact that whether one lives in the eastern region contributes more to urban-rural disparities in women's depressive symptoms than in the central and western regions further suggests that there are more complex factors, such as socioeconomic development, underlying the issue of urban-rural disparities in women's depressive symptoms.
There are also limitations to this study. On the one hand, this study uses cross-sectional data, which does not allow causal inference and does not reveal causality and explore mechanisms of influence. On the other hand, China's cultural background and urban-rural dual economic structure may affect the cross-country generalizability of this study. In addition, the effect of COVID-19 could not be ruled out in this study, but due to data restrictions, variables related to COVID-19 were not controlled for; and measurement of digital engagement lacks normative and scientific validity, and there are no usable scales.
Conclusions
This study focuses for the first time on the link between digital engagement and urban-rural disparities in women's depressive symptoms. The findings not only enrich the research on the digital divide and mental health inequality, but also extend the research on feminist psychology and provide insights into digital psychotherapy, which can help to bridge the urban-rural women's mental health gap by enhancing the depth and breadth of rural women's digital engagement. In addition, it also provides new perspectives for promoting women's health equality.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076241239246 - Supplemental material for Association between digital engagement and urban-rural disparities in Chinese women's depressive symptoms: A national-level cross-sectional study
Supplemental material, sj-doc-1-dhj-10.1177_20552076241239246 for Association between digital engagement and urban-rural disparities in Chinese women's depressive symptoms: A national-level cross-sectional study by Xiaochen Wang and Yangyang Wang in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to acknowledge the Institute of Social Science Survey (ISSS) of Peking University for the approval to use the wave 2020 of CFPS dataset. They express their sincere gratitude to all subjects who participated in the survey.
Contributors
X.W. did writing the original draft and data curation. Y.W. did framework and model analyses and data curation, and also writing the original draft. Two authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Biomedical Ethics Committee of Peking University (IRB00001052-14010). All participants gave written informed consent in accordance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
YW.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.